Non-High-Density Lipoprotein Cholesterol and Progression of Chronic Kidney Disease: Results from the KNOW-CKD Study

 , , , , , and
on behalf of the Korean Cohort Study for Outcomes in Patients with Chronic Kidney Disease (KNOW-CKD) Investigators
, , , , , and
on behalf of the Korean Cohort Study for Outcomes in Patients with Chronic Kidney Disease (KNOW-CKD) Investigators
Abstract
1. Introduction
2. Materials and Methods
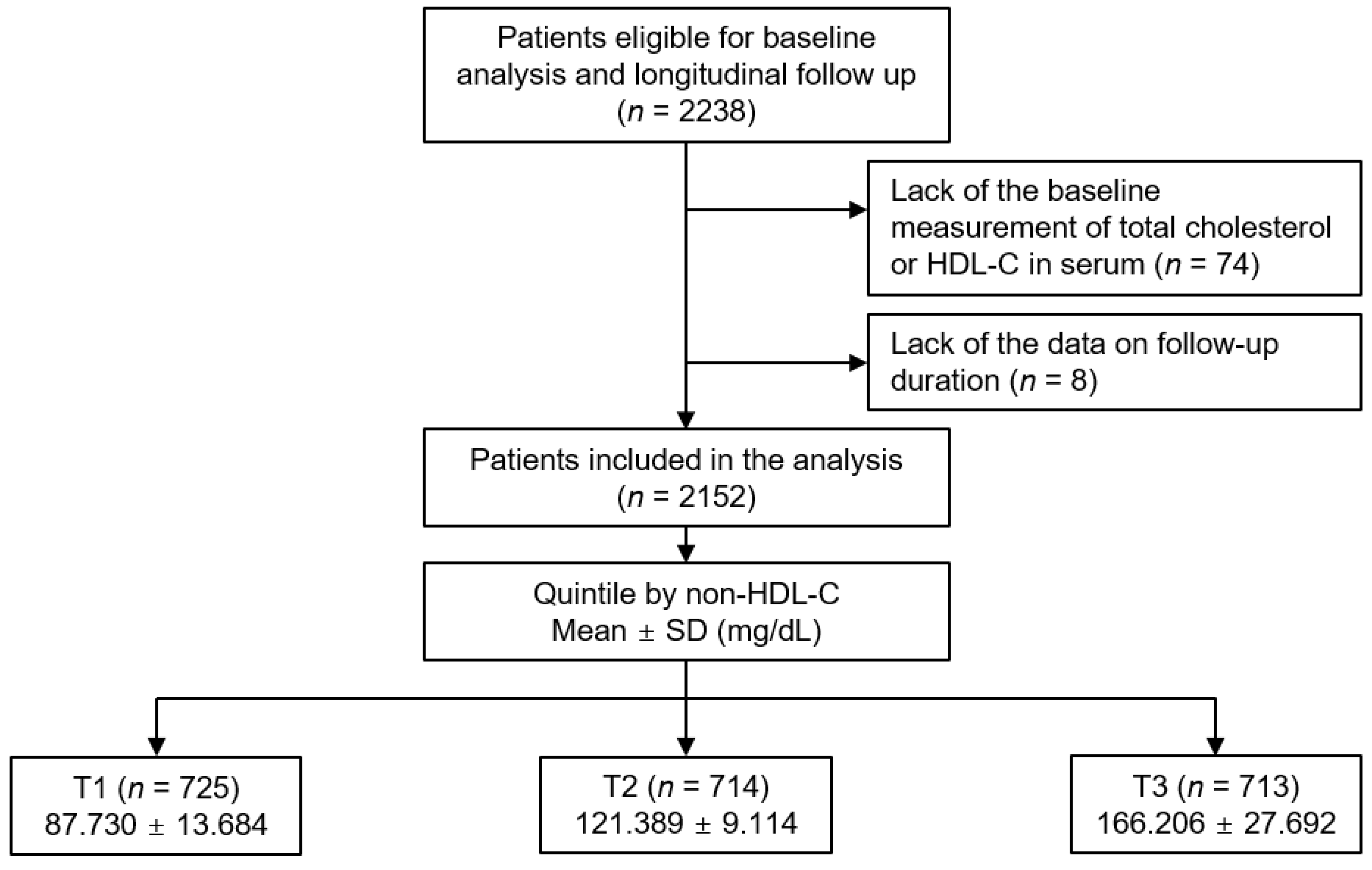
2.1. Study Design
2.2. Data Collection from Participants
2.3. Exposure and Study Outcome
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
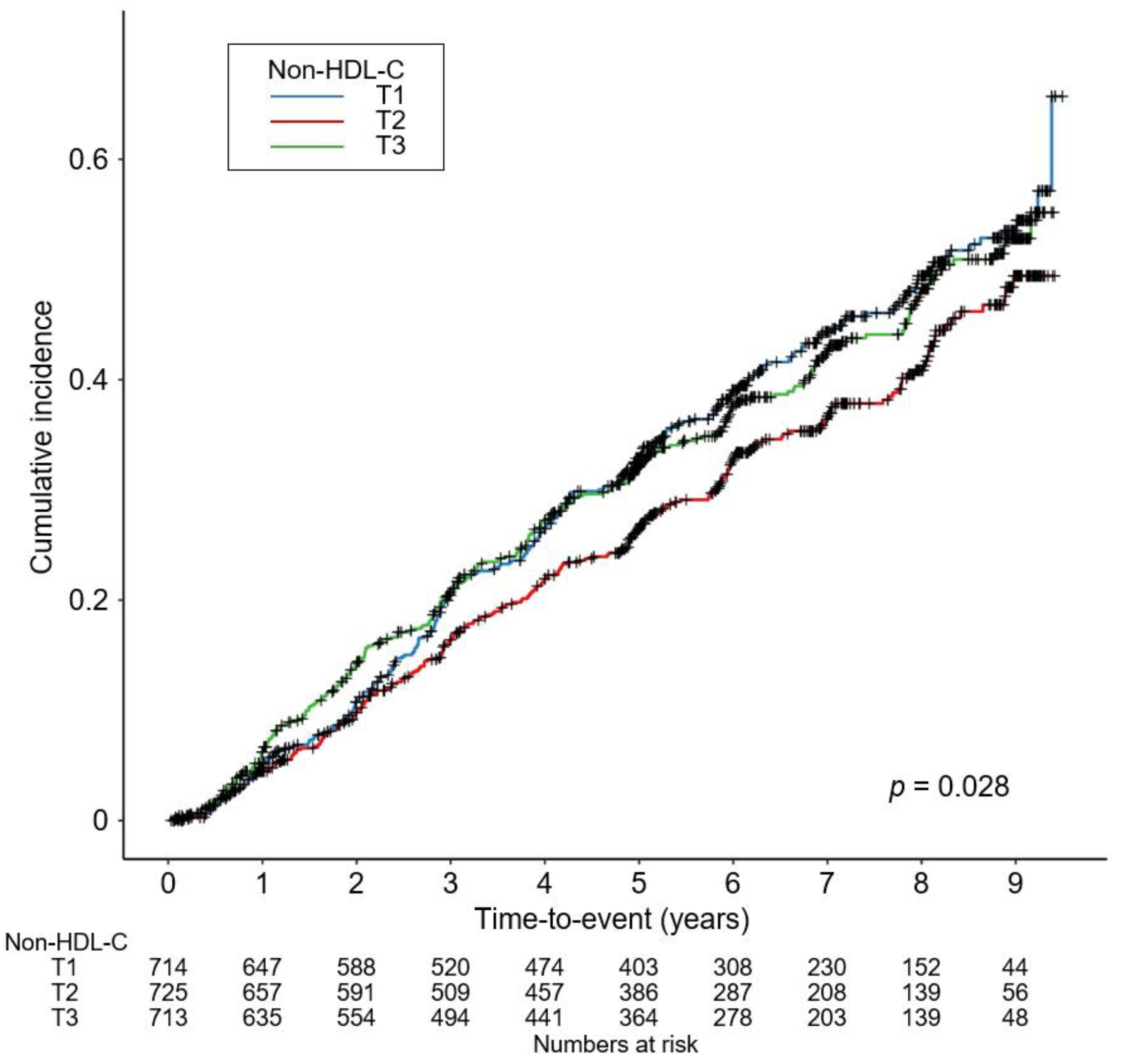
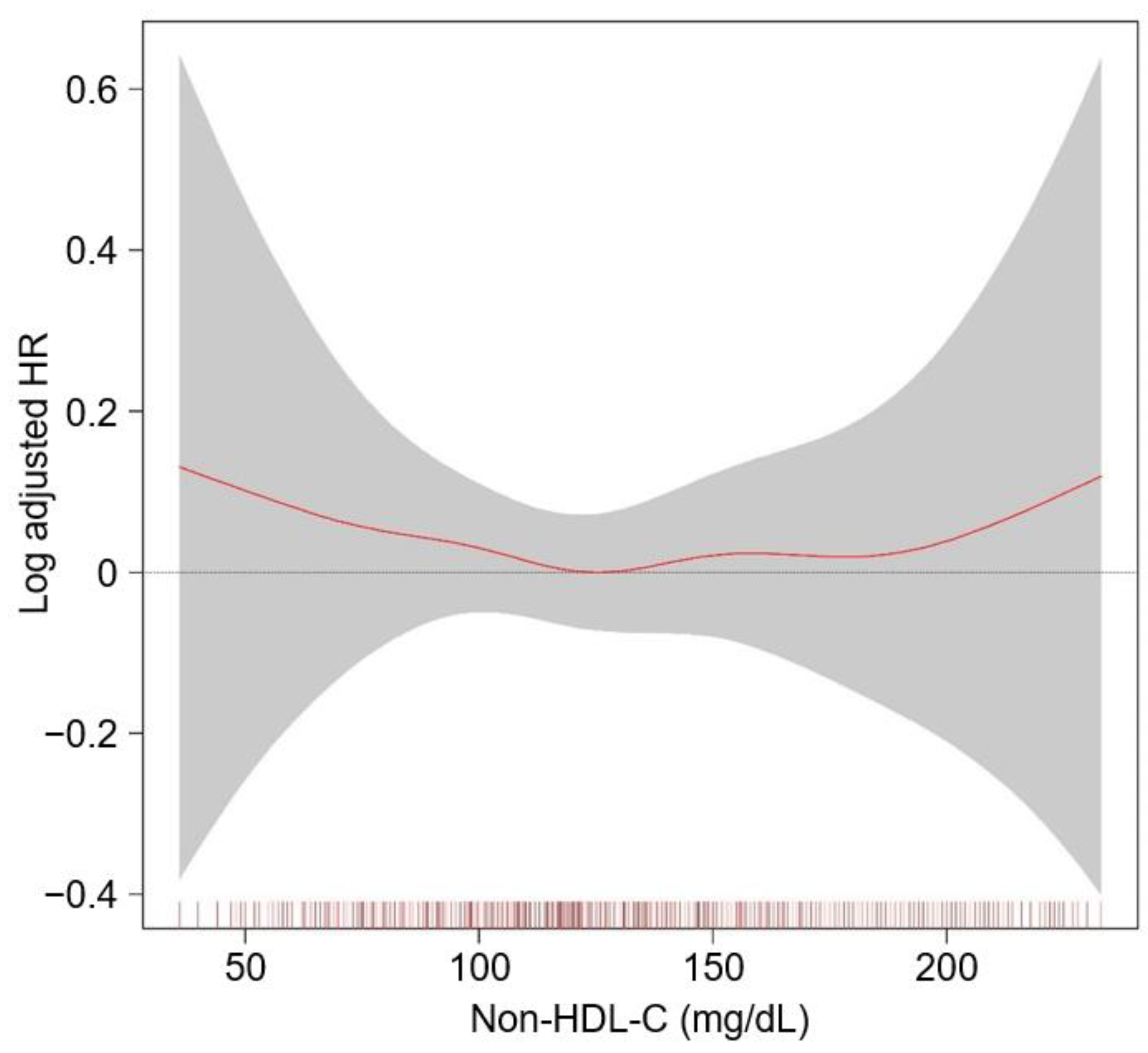
3.2. Association of nHDL with Renal Outcomes in Patients with Non-Dialysis CKD
3.3. Sensitivity Analyses
3.4. Subgroup Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsuruya, K.; Yoshida, H.; Nagata, M.; Kitazono, T.; Iseki, K.; Iseki, C.; Fujimoto, S.; Konta, T.; Moriyama, T.; Yamagata, K.; et al. Impact of the Triglycerides to High-Density Lipoprotein Cholesterol Ratio on the Incidence and Progression of CKD: A Longitudinal Study in a Large Japanese Population. Am. J. Kidney Dis. 2015, 66, 972–983. [Google Scholar] [CrossRef]
- Kochan, Z.; Szupryczynska, N.; Malgorzewicz, S.; Karbowska, J. Dietary Lipids and Dyslipidemia in Chronic Kidney Disease. Nutrients 2021, 13, 3138. [Google Scholar] [CrossRef]
- Tsuruya, K.; Yoshida, H.; Nagata, M.; Kitazono, T.; Iseki, K.; Iseki, C.; Fujimoto, S.; Konta, T.; Moriyama, T.; Yamagata, K.; et al. Association of Hypertriglyceridemia With the Incidence and Progression of Chronic Kidney Disease and Modification of the Association by Daily Alcohol Consumption. J. Ren. Nutr. Off. J. Counc. Ren. Nutr. Natl. Kidney Found. 2017, 27, 381–394. [Google Scholar] [CrossRef]
- Wanner, C.; Tonelli, M. KDIGO Clinical Practice Guideline for Lipid Management in CKD: Summary of recommendation statements and clinical approach to the patient. Kidney Int. 2014, 85, 1303–1309. [Google Scholar] [CrossRef]
- Toth, P.P.; Philip, S.; Hull, M.; Granowitz, C. Association of Elevated Triglycerides With Increased Cardiovascular Risk and Direct Costs in Statin-Treated Patients. Mayo Clin. Proc. 2019, 94, 1670–1680. [Google Scholar] [CrossRef]
- Nelson, A.J.; Navar, A.M.; Mulder, H.; Wojdyla, D.; Philip, S.; Granowitz, C.; Peterson, E.D.; Pagidipati, N.J. Association Between Triglycerides and Residual Cardiovascular Risk in Patients With Type 2 Diabetes Mellitus and Established Cardiovascular Disease (From the Bypass Angioplasty Revascularization Investigation 2 Diabetes [BARI 2D] Trial). Am. J. Cardiol. 2020, 132, 36–43. [Google Scholar] [CrossRef]
- Li, Y.H.; Tseng, W.K.; Yin, W.H.; Lin, F.J.; Wu, Y.W.; Hsieh, I.C.; Lin, T.H.; Sheu, W.H.; Yeh, H.I.; Chen, J.W.; et al. Prognostic effect of high-density lipoprotein cholesterol level in patients with atherosclerotic cardiovascular disease under statin treatment. Sci. Rep. 2020, 10, 21835. [Google Scholar] [CrossRef]
- Sonmez, A.; Yilmaz, M.I.; Saglam, M.; Unal, H.U.; Gok, M.; Cetinkaya, H.; Karaman, M.; Haymana, C.; Eyileten, T.; Oguz, Y.; et al. The role of plasma triglyceride/high-density lipoprotein cholesterol ratio to predict cardiovascular outcomes in chronic kidney disease. Lipids Health Dis. 2015, 14, 29. [Google Scholar] [CrossRef]
- Kim, J.Y.; Park, J.T.; Kim, H.W.; Chang, T.I.; Kang, E.W.; Ahn, C.; Oh, K.H.; Lee, J.; Chung, W.; Kim, Y.S.; et al. Inflammation Alters Relationship Between High-Density Lipoprotein Cholesterol and Cardiovascular Risk in Patients With Chronic Kidney Disease: Results From KNOW-CKD. J. Am. Heart Assoc. 2021, 10, e021731. [Google Scholar] [CrossRef]
- Kang, H.T.; Kim, J.K.; Kim, J.Y.; Linton, J.A.; Yoon, J.H.; Koh, S.B. Independent association of TG/HDL-C with urinary albumin excretion in normotensive subjects in a rural Korean population. Clin. Chim. Acta Int. J. Clin. Chem. 2012, 413, 319–324. [Google Scholar] [CrossRef]
- Kang, H.T.; Shim, J.Y.; Lee, Y.J.; Lee, J.E.; Linton, J.A.; Kim, J.K.; Lee, H.R. Association between the ratio of triglycerides to high-density lipoprotein cholesterol and chronic kidney disease in Korean adults: The 2005 Korean National Health and Nutrition Examination Survey. Kidney Blood Press. Res. 2011, 34, 173–179. [Google Scholar] [CrossRef]
- Kim, J.Y.; Kang, H.T.; Lee, H.R.; Lee, Y.J.; Shim, J.Y. Comparison of lipid-related ratios for prediction of chronic kidney disease stage 3 or more in Korean adults. J. Korean Med. Sci. 2012, 27, 1524–1529. [Google Scholar] [CrossRef]
- Tsuruya, K.; Yoshida, H.; Nagata, M.; Kitazono, T.; Hirakata, H.; Iseki, K.; Moriyama, T.; Yamagata, K.; Yoshida, H.; Fujimoto, S.; et al. Association of the triglycerides to high-density lipoprotein cholesterol ratio with the risk of chronic kidney disease: Analysis in a large Japanese population. Atherosclerosis 2014, 233, 260–267. [Google Scholar] [CrossRef]
- Nam, K.H.; Chang, T.I.; Joo, Y.S.; Kim, J.; Lee, S.; Lee, C.; Yun, H.R.; Park, J.T.; Yoo, T.H.; Sung, S.A.; et al. Association Between Serum High-Density Lipoprotein Cholesterol Levels and Progression of Chronic Kidney Disease: Results From the KNOW-CKD. J. Am. Heart Assoc. 2019, 8, e011162. [Google Scholar] [CrossRef]
- Schaeffner, E.S.; Kurth, T.; Curhan, G.C.; Glynn, R.J.; Rexrode, K.M.; Baigent, C.; Buring, J.E.; Gaziano, J.M. Cholesterol and the risk of renal dysfunction in apparently healthy men. J. Am. Soc. Nephrol. 2003, 14, 2084–2091. [Google Scholar] [CrossRef]
- Muntner, P.; Coresh, J.; Smith, J.C.; Eckfeldt, J.; Klag, M.J. Plasma lipids and risk of developing renal dysfunction: The atherosclerosis risk in communities study. Kidney Int. 2000, 58, 293–301. [Google Scholar] [CrossRef]
- Fox, C.S.; Larson, M.G.; Leip, E.P.; Culleton, B.; Wilson, P.W.; Levy, D. Predictors of new-onset kidney disease in a community-based population. JAMA 2004, 291, 844–850. [Google Scholar] [CrossRef]
- Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP). Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef]
- Su, X.; Kong, Y.; Peng, D. Evidence for changing lipid management strategy to focus on non-high density lipoprotein cholesterol. Lipids Health Dis. 2019, 18, 134. [Google Scholar] [CrossRef]
- Suh, S.H.; Oh, T.R.; Choi, H.S.; Kim, C.S.; Bae, E.H.; Ma, S.K.; Oh, K.-H.; Han, S.H.; Kim, S.W. Non-High-Density Lipoprotein Cholesterol and Cardiovascular Outcomes in Chronic Kidney Disease: Results from KNOW-CKD Study. Nutrients 2022, 14, 3792. [Google Scholar] [CrossRef]
- Oh, K.H.; Park, S.K.; Park, H.C.; Chin, H.J.; Chae, D.W.; Choi, K.H.; Han, S.H.; Yoo, T.H.; Lee, K.; Kim, Y.S.; et al. KNOW-CKD (KoreaN cohort study for Outcome in patients With Chronic Kidney Disease): Design and methods. BMC Nephrol. 2014, 15, 80. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Eckardt, K.U.; Tsukamoto, Y.; Levin, A.; Coresh, J.; Rossert, J.; De Zeeuw, D.; Hostetter, T.H.; Lameire, N.; Eknoyan, G. Definition and classification of chronic kidney disease: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2005, 67, 2089–2100. [Google Scholar] [CrossRef]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for chamber quantification: A report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar] [CrossRef] [PubMed]
- Moorhead, J.F.; Chan, M.K.; El-Nahas, M.; Varghese, Z. Lipid nephrotoxicity in chronic progressive glomerular and tubulo-interstitial disease. Lancet 1982, 2, 1309–1311. [Google Scholar] [CrossRef]
- Gröne, H.J.; Walli, A.; Gröne, E.; Niedmann, P.; Thiery, J.; Seidel, D.; Helmchen, U. Induction of glomerulosclerosis by dietary lipids. A functional and morphologic study in the rat. Lab. Investig. A J. Tech. Methods Pathol. 1989, 60, 433–446. [Google Scholar]
- Joles, J.A.; van Goor, H.; van der Horst, M.L.; van Tol, A.; Elema, J.D.; Koomans, H.A. High lipid levels in very low density lipoprotein and intermediate density lipoprotein may cause proteinuria and glomerulosclerosis in aging female analbuminemic rats. Lab. Investig. A J. Tech. Methods Pathol. 1995, 73, 912–921. [Google Scholar]
- Liu, Y.; Coresh, J.; Eustace, J.A.; Longenecker, J.C.; Jaar, B.; Fink, N.E.; Tracy, R.P.; Powe, N.R.; Klag, M.J. Association between cholesterol level and mortality in dialysis patients: Role of inflammation and malnutrition. JAMA 2004, 291, 451–459. [Google Scholar] [CrossRef]
- Lu, Y.; Nyunt, M.S.Z.; Gao, Q.; Gwee, X.; Chua, D.Q.; Yap, K.B.; Pan, F.; Ng, T.P. Malnutrition Risk and Kidney Function and Decline in Community-Dwelling Older Adults. J. Ren. Nutr. 2022, 32, 560–568. [Google Scholar] [CrossRef]
- Gluba-Brzozka, A.; Franczyk, B.; Rysz, J. Cholesterol Disturbances and the Role of Proper Nutrition in CKD Patients. Nutrients 2019, 11, 2820. [Google Scholar] [CrossRef]
- Vaziri, N.D.; Navab, M.; Fogelman, A.M. HDL metabolism and activity in chronic kidney disease. Nat. Rev. Nephrol. 2010, 6, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Yancey, P.G.; Ikizler, T.A.; Jerome, W.G.; Kaseda, R.; Cox, B.; Bian, A.; Shintani, A.; Fogo, A.B.; Linton, M.F.; et al. Dysfunctional high-density lipoprotein in patients on chronic hemodialysis. J. Am. Coll. Cardiol. 2012, 60, 2372–2379. [Google Scholar] [CrossRef] [PubMed]
- Moradi, H.; Vaziri, N.D.; Kashyap, M.L.; Said, H.M.; Kalantar-Zadeh, K. Role of HDL dysfunction in end-stage renal disease: A double-edged sword. J. Ren. Nutr. 2013, 23, 203–206. [Google Scholar] [CrossRef] [PubMed]
- Baigent, C.; Landray, M.J.; Reith, C.; Emberson, J.; Wheeler, D.C.; Tomson, C.; Wanner, C.; Krane, V.; Cass, A.; Craig, J.; et al. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): A randomised placebo-controlled trial. Lancet 2011, 377, 2181–2192. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| nHDL Level | p Value | |||
|---|---|---|---|---|
| T1 | T2 | T3 | ||
| Follow-up duration (year) | 6.334 ± 2.493 | 6.320 ± 2.533 | 6.234 ± 2.538 | 0.720 |
| Age (year) | 55.098 ± 12.452 | 53.478 ± 11.897 | 52.620 ± 12.314 | 0.001 |
| Male | 465 (64.1) | 434 (60.8) | 422 (59.2) | 0.144 |
| Age-adjusted CCI | 0.001 | |||
| 0–3 | 330 (45.5) | 398 (55.7) | 394 (55.3) | |
| 4–5 | 232 (32.0) | 193 (27.0) | 207 (29.0) | |
| 6–7 | 132 (18.2) | 105 (14.7) | 97 (13.6) | |
| ≥8 | 31 (4.3) | 18 (2.5) | 15 (2.1) | |
| Primary cause of CKD | 0.117 | |||
| DM | 215 (29.7) | 155 (21.7) | 175 (24.6) | |
| HTN | 139 (19.2) | 137 (19.2) | 150 (21.1) | |
| GN | 211 (29.1) | 247 (34.6) | 227 (31.9) | |
| TID | 4 (0.6) | 5 (0.7) | 4 (0.6) | |
| PKD | 107 (14.8) | 119 (16.7) | 114 (16.0) | |
| Others | 49 (6.8) | 51 (7.1) | 42 (5.9) | |
| Smoking history | 0.151 | |||
| Non-smoker | 361 (49.8) | 395 (55.3) | 392 (55.1) | |
| Ex-smoker | 118 (16.3) | 108 (15.1) | 115 (16.2) | |
| Current smoker | 246 (33.9) | 211 (29.6) | 204 (28.7) | |
| Medication | ||||
| ACEIs/ARBs | 214 (29.5) | 197 (27.6) | 219 (30.7) | 0.425 |
| Diuretic use | 237 (32.7) | 210 (29.4) | 239 (33.5) | 0.212 |
| Anti-HTN drugs ≥ 3 | 214 (29.5) | 197 (27.6) | 219 (30.7) | 0.425 |
| Statins | 509 (70.2) | 343 (48.0) | 266 (37.3) | <0.001 |
| BMI (kg/m2) | 24.140 ± 3.277 | 24.583 ± 3.206 | 25.100 ± 3.681 | <0.001 |
| Waist circumference (cm) | 86.518 ± 9.543 | 87.410 ± 9.470 | 88.659 ± 10.089 | <0.001 |
| SBP (mmHg) | 125.552 ± 15.070 | 128.585 ± 16.716 | 129.361 ± 16.530 | <0.001 |
| DBP (mmHg) | 74.724 ± 10.425 | 77.742 ± 10.952 | 78.303 ± 11.567 | <0.001 |
| Laboratory findings | ||||
| Hemoglobin (g/dL) | 12.520 ± 2.019 | 12.970 ± 2.000 | 13.031 ± 2.010 | <0.001 |
| Albumin (g/dL) | 4.188 ± 0.353 | 4.205 ± 0.371 | 4.132 ± 0.530 | 0.010 |
| Total cholesterol (mg/dL) | 138.422 ± 21.093 | 169.807 ± 16.377 | 214.798 ± 30.740 | <0.001 |
| HDL-C (mg/dL) | 50.692 ± 17.316 | 48.418 ± 14.229 | 48.592 ± 14.407 | 0.013 |
| LDL-C (mg/dL) | 68.828 ± 15.342 | 94.705 ± 16.829 | 127.746 ± 27.669 | <0.001 |
| TG (mg/dL) | 117.327 ± 58.870 | 152.076 ± 77.792 | 204.278 ± 125.992 | <0.001 |
| Fasting glucose (mg/dL) | 107.427 ± 33.661 | 110.925 ± 41.189 | 115.025 ± 44.121 | 0.001 |
| hs-CRP (mg/dL) | 0.500 (0.200, 1.400) | 0.600 (0.210, 1.700) | 0.800 (0.300, 1.900) | 0.449 |
| Spot urine ACR (mg/g) | 331.017 (80.954, 891.067) | 312.364 (63.343, 950.315) | 426.526 (91.296, 1489.556) | <0.001 |
| Creatinine (mg/dL) | 1.925 ± 1.220 | 1.768 ± 1.133 | 1.767 ± 1.103 | 0.015 |
| eGFR (mL/min/1.73 m2) | 47.145 ± 28.686 | 52.215 ± 30.834 | 51.965 ± 30.823 | 0.001 |
| CKD stages | 0.111 | |||
| Stage 1 | 93 (12.8) | 130 (18.2) | 125 (17.5) | |
| Stage 2 | 132 (18.2) | 135 (18.9) | 140 (19.6) | |
| Stage 3a | 114 (15.7) | 117 (16.4) | 122 (17.1) | |
| Stage 3b | 161 (22.2) | 149 (20.9) | 143 (20.1) | |
| Stage 4 | 169 (23.3) | 146 (20.4) | 141 (19.8) | |
| Stage 5 | 56 (7.7) | 37 (5.2) | 42 (5.9) |
| NHDL | Events, n (%) | Model 1 | Model 2 | Model 3 | Model 4 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| HR (95% CIs) | p Value | HR (95% CIs) | p Value | HR (95% CIs) | p Value | HR (95% CIs) | p Value | |||
| Composite renal event | T1 | 295 (40.7) | 1.302 (1.084, 1.564) | 0.005 | 1.224 (1.033, 1.452) | 0.020 | 1.178 (0.982, 1.414) | 0.077 | 1.309 (1.074, 1.595) | 0.008 |
| T2 | 243 (34.0) | Reference | Reference | Reference | Reference | |||||
| T3 | 278 (39.0) | 1.207 (1.000, 1.456) | 0.050 | 1.213 (1.021, 1.440) | 0.028 | 1.216 (1.015, 1.457) | 0.033 | 1.272 (1.040, 1.556) | 0.019 | |
| NHDL | Events, n (%) | Model 1 | Model 2 | Model 3 | Model 4 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| HR (95% CIs) | p Value | HR (95% CIs) | p Value | HR (95% CIs) | p Value | HR (95% CIs) | p Value | |||
| Decline of renal function | T1 | 198 (27.3) | 1.162 (0.932, 1.448) | 0.182 | 1.144 (0.933, 1.403) | 0.197 | 1.055 (0.846, 1.316) | 0.634 | 1.110 (0.882, 1.398) | 0.373 |
| T2 | 174 (24.4) | Reference | Reference | Reference | Reference | |||||
| T3 | 197 (27.6) | 1.148 (0.917, 1.436) | 0.228 | 1.193 (0.973, 1.463) | 0.089 | 1.209 (0.976, 1.498) | 0.082 | 1.002 (0.791, 1.271) | 0.984 | |
| Initiation of RRT | T1 | 226 (31.2) | 1.293 (1.047, 1.597) | 0.017 | 1.207 (0.993, 1.468) | 0.058 | 1.139 (0.924, 1.404) | 0.224 | 1.151 (0.915, 1.449) | 0.231 |
| T2 | 184 (25.8) | Reference | Reference | Reference | Reference | |||||
| T3 | 214 (30.0) | 1.247 (1.005, 1.546) | 0.045 | 1.228 (1.008, 1.495) | 0.041 | 1.224 (0.995, 1.506) | 0.056 | 1.281 (1.014, 1.619) | 0.038 | |
| NHDL | Model 1 | Model 2 | Model 3 | Model 4 | |||||
|---|---|---|---|---|---|---|---|---|---|
| HR (95% CIs) | p value | HR (95% CIs) | p value | HR (95% CIs) | p value | HR (95% CIs) | p value | ||
| Composite renal event | T1 | 1.240 (1.047, 1.467) | 0.013 | 1.224 (1.033, 1.451) | 0.019 | 1.178 (0.976, 1.432) | 0.088 | 1.309 (1.051, 1.630) | 0.016 |
| T2 | Reference | Reference | Reference | Reference | |||||
| T3 | 1.209 (1.018, 1.437) | 0.031 | 1.213 (1.021, 1.441) | 0.028 | 1.216 (1.010, 1.464) | 0.039 | 1.273 (1.013, 1.598) | 0.038 | |
| Decline renal function | T1 | 1.139 (0.930, 1.395) | 0.207 | 1.144 (0.933, 1.402) | 0.196 | 1.055 (0.843, 1.321) | 0.640 | 1.111 (0.883, 1.396) | 0.369 |
| T2 | Reference | Reference | Reference | Reference | |||||
| T3 | 1.195 (0.974, 1.466) | 0.087 | 1.193 (0.973, 1.464) | 0.090 | 1.209 (0.972, 1.504) | 0.088 | 1.002 (0.780, 1.288) | 0.985 | |
| Initiation of RRT | T1 | 1.236 (1.018, 1.501) | 0.032 | 1.207 (0.993, 1.468) | 0.059 | 1.139 (0.915, 1.417) | 0.243 | 1.151 (0.887, 1.484) | 0.290 |
| T2 | Reference | Reference | Reference | Reference | |||||
| T3 | 1.219 (1.001, 1.485) | 0.049 | 1.228 (1.008, 1.495) | 0.041 | 1.224 (0.991, 1.513) | 0.061 | 1.282 (0.977, 1.683) | 0.073 | |
| NHDL | Events, n (%) | Unadjusted HR (95% CIs) | p for Interaction | Adjusted HR (95% CIs) | p for Interaction | |
|---|---|---|---|---|---|---|
| Age < 60 years | T1 | 173 (40.7) | 1.255 (1.011, 1.556) | 0.720 | 1.256 (0.972, 1.624) | 0.157 |
| T2 | 159 (33.3) | Reference | Reference | |||
| T3 | 188 (39.0) | 1.270 (1.028, 1.569) | 1.320 (1.024, 1.701) | |||
| Age ≥ 60 years | T1 | 122 (40.7) | 1.168 (0.885, 1.543) | 1.396 (1.010, 1.929) | ||
| T2 | 84 (35.6) | Reference | Reference | |||
| T3 | 90 (39.0) | 1.087 (0.807, 1.464) | 1.1685, 0.817, 1.670) | |||
| Male | T1 | 174 (37.4) | 1.084 (0.872, 1.348) | 0.153 | 1.047 (0.807, 1.359) | 0.007 |
| T2 | 151 (34.8) | Reference | Reference | |||
| T3 | 162 (38.4) | 1.145 (0.917, 1.430) | 1.453 (1.114, 1.895) | |||
| Female | T1 | 121 (46.5) | 1.528 (1.165, 2.004) | 1.506 (1.086, 2.088) | ||
| T2 | 92 (32.9) | Reference | Reference | |||
| T3 | 116 (39.9) | 1.315 (1.000, 1.729) | 0.993 (0.710, 1.388) | |||
| BMI < 23 kg/m2 | T1 | 111 (41.4) | 1.252 (0.936, 1.675) | 0.898 | 0.794 (0.558, 1.129) | 0.035 |
| T2 | 77 (34.7) | Reference | Reference | |||
| T3 | 82 (39.6) | 1.289 (0.944, 1.760) | 0.980 (0.673, 1.425) | |||
| BMI ≥ 23 kg/m2 | T1 | 183 (40.6) | 1.233 (0.999, 1.522) | 1.562 (1.217, 2.005) | ||
| T2 | 164 (33.7) | Reference | Reference | |||
| T3 | 196 (39.0) | 1.186 (0.963, 1.459) | 1.433 (1.120, 1.835) | |||
| eGFR ≥ 45 mL/min/1.73 m2 | T1 | 51 (16.2) | 1.036 (0.707, 1.520) | 0.585 | 0.994 (0.651, 1.518) | 0.011 |
| T2 | 54 (14.8) | Reference | Reference | |||
| T3 | 60 (16.6) | 1.094 (0.757, 1.580) | 0.736 (0.478, 1.133) | |||
| eGFR < 45 mL/min/1.73 m2 | T1 | 244 (59.5) | 1.183 (0.978, 1.431) | 1.313 (1.046, 1.648) | ||
| T2 | 189 (54.2) | Reference | Reference | |||
| T3 | 218 (62.1) | 1.353 (1.113, 1.644) | 1.426 (1.131, 1.797) | |||
| Spot urine ACR < 300 mg/g | T1 | 88 (26.4) | 1.486 (1.073, 2.057) | 0.173 | 1.400 (0.951, 2.059) | 0.800 |
| T2 | 62 (18.4) | Reference | Reference | |||
| T3 | 57 (19.6) | 1.031 (0.720, 1.478) | 1.229 (0.824, 1.833) | |||
| Spot urine ACR ≥ 300 mg/g | T1 | 202 (55.5) | 1.157 (0.945, 1.416) | 1.259 (0.993, 1.593) | ||
| T2 | 176 (49.9) | Reference | Reference | |||
| T3 | 213 (53.4) | 1.161 (0.951, 1.418) | 1.290 (1.015, 1.639) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suh, S.H.; Oh, T.R.; Choi, H.S.; Kim, C.S.; Bae, E.H.; Ma, S.K.; Oh, K.-H.; Hyun, Y.Y.; Sung, S.; Kim, S.W., on behalf of the Korean Cohort Study for Outcomes in Patients with Chronic Kidney Disease (KNOW-CKD) Investigators. Non-High-Density Lipoprotein Cholesterol and Progression of Chronic Kidney Disease: Results from the KNOW-CKD Study. Nutrients 2022, 14, 4704. https://doi.org/10.3390/nu14214704
Suh SH, Oh TR, Choi HS, Kim CS, Bae EH, Ma SK, Oh K-H, Hyun YY, Sung S, Kim SW on behalf of the Korean Cohort Study for Outcomes in Patients with Chronic Kidney Disease (KNOW-CKD) Investigators. Non-High-Density Lipoprotein Cholesterol and Progression of Chronic Kidney Disease: Results from the KNOW-CKD Study. Nutrients. 2022; 14(21):4704. https://doi.org/10.3390/nu14214704
Chicago/Turabian StyleSuh, Sang Heon, Tae Ryom Oh, Hong Sang Choi, Chang Seong Kim, Eun Hui Bae, Seong Kwon Ma, Kook-Hwan Oh, Young Youl Hyun, Suah Sung, and Soo Wan Kim on behalf of the Korean Cohort Study for Outcomes in Patients with Chronic Kidney Disease (KNOW-CKD) Investigators. 2022. "Non-High-Density Lipoprotein Cholesterol and Progression of Chronic Kidney Disease: Results from the KNOW-CKD Study" Nutrients 14, no. 21: 4704. https://doi.org/10.3390/nu14214704
APA StyleSuh, S. H., Oh, T. R., Choi, H. S., Kim, C. S., Bae, E. H., Ma, S. K., Oh, K.-H., Hyun, Y. Y., Sung, S., & Kim, S. W., on behalf of the Korean Cohort Study for Outcomes in Patients with Chronic Kidney Disease (KNOW-CKD) Investigators. (2022). Non-High-Density Lipoprotein Cholesterol and Progression of Chronic Kidney Disease: Results from the KNOW-CKD Study. Nutrients, 14(21), 4704. https://doi.org/10.3390/nu14214704