
Positive Additive and Multiplicative Interactions among Clustered Components of Metabolic Syndrome with Type 2 Diabetes Mellitus among Brazilian Adolescent Students

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Anthropometric and Blood Pressure Measurements
2.3. Biochemical Assays
2.4. Metabolic Syndrome Definition
2.5. Outcome Definition
2.6. Statistical Analysis
3. Results
3.1. Description of the Study Population
3.2. Comparing Observed and Expected Joint Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, L.L.; Lawrence, J.; Davis, C.; Liese, A.D.; Pettitt, D.J.; Pihoker, C.; Dabelea, D.; Hamman, R.; Waitzfelder, B.; Kahn, H.; et al. Prevalence of overweight and obesity in youth with diabetes in USA: The SEARCH for Diabetes in Youth study. Pediatr. Diabetes 2010, 11, 4–11. Available online: https://pubmed-ncbi-nlm-nih-gov.proxy1.library.jhu.edu/19473302/ (accessed on 22 October 2021). [CrossRef]
- Savic Hitt, T.A.; Katz, L.E.L. Pediatric Type 2 Diabetes: Not a Mini Version of Adult Type 2 Diabetes. Endocrinol. Metab. Clin. N. Am. 2020, 49, 679–693. Available online: https://pubmed.ncbi.nlm.nih.gov/33153674/ (accessed on 16 December 2021). [CrossRef]
- Dart, A.B.; Martens, P.J.; Rigatto, C.; Brownell, M.D.; Dean, H.J.; Sellers, E.A. Earlier Onset of Complications in Youth With Type 2 Diabetes. Diabetes Care 2014, 37, 436–443. Available online: http://care.diabetesjournals.org/lookup/ (accessed on 27 December 2021). [CrossRef]
- Tfayli, H.; Arslanian, S. Pathophysiology of type 2 diabetes mellitus in youth: The evolving chameleon. Arq. Bras. Endocrinol. Metabol. 2009, 53, 165. [Google Scholar] [CrossRef]
- Reinehr, T. Clinical presentation of type 2 diabetes mellitus in children and adolescents. Int. J. Obes. 2005, 29, S105–S110. Available online: https://www.nature.com/articles/0803065/ (accessed on 22 October 2021). [CrossRef]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.; James, W.P.T.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the international diabetes federation task force on epidemiology and prevention; National heart, lung, and blood institute; American heart association; World heart federation; International atherosclerosis society; And international association for the study of obesity. Circulation 2009, 120, 1640–1645. Available online: http://circ.ahajournals.org/ (accessed on 4 April 2021).
- Reisinger, C.; Nkeh-Chungag, B.N.; Fredriksen, P.M.; Goswami, N. The prevalence of pediatric metabolic syndrome—A critical look on the discrepancies between definitions and its clinical importance. Int. J. Obes. 2021, 45, 12–24. [Google Scholar] [CrossRef]
- Alberti, K.G.M.M.; Zimmet, P.; Shaw, J. Metabolic syndrome—A new world-wide definition. A consensus statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. Available online: https://pubmed.ncbi.nlm.nih.gov/16681555/ (accessed on 27 December 2020). [CrossRef]
- Huang, P.L. A comprehensive definition for metabolic syndrome. Company of Biologists; DMM Dis. Model. Mech. 2009, 2, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Bentham, J.; Di Cesare, M.; Bilano, V.; Bixby, H.; Zhou, B.; Stevens, G.A.; Ezzati, M.; Riley, L.M.; Taddei, C.; Hajifathalian, K.; et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. Available online: https://pubmed.ncbi.nlm.nih.gov/29029897/ (accessed on 28 February 2021).
- Miller, J.M.; Kaylor, M.B.; Johannsson, M.; Bay, C.; Churilla, J.R. Prevalence of metabolic syndrome and individual criterion in US adolescents: 2001–2010 national health and nutrition examination survey. Mary Ann Liebert Inc. Metab. Syndr. Relat. Disord. 2014, 12, 527–532. Available online: https://pubmed.ncbi.nlm.nih.gov/25247821/ (accessed on 5 April 2021). [CrossRef]
- Ramírez-Vélez, R.; Anzola, A.; Martinez-Torres, J.; Vivas, A.; Tordecilla-Sanders, A.; Prieto-Benavides, D.; Izquierdo, M.; Correa-Bautista, J.E.; Garcia-Hermoso, A. Metabolic Syndrome and Associated Factors in a Population-Based Sample of Schoolchildren in Colombia: The FUPRECOL Study. Metab. Syndr. Relat. Disord. 2016, 14, 455–462. Available online: https://pubmed.ncbi.nlm.nih.gov/27508490/ (accessed on 28 December 2020). [CrossRef]
- Asghari, G.; Eftekharzadeh, A.; Hosseinpanah, F.; Ghareh, S.; Mirmiran, P.; Azizi, F. Instability of different adolescent metabolic syndrome definitions tracked into early adulthood metabolic syndrome: Tehran Lipid and Glucose Study (TLGS). Pediatr. Diabetes 2017, 18, 59–66. Available online: https://onlinelibrary-wiley-com.proxy1.library.jhu.edu/doi/full/10.1111/pedi.12349/ (accessed on 20 October 2021). [CrossRef]
- Ford, E.S.; Li, C. Defining the Metabolic Syndrome in Children and Adolescents: Will the Real Definition Please Stand Up? J. Pediatr. 2008, 152, 160–164. Available online: https://pubmed.ncbi.nlm.nih.gov/18206681/ (accessed on 27 December 2020). [CrossRef]
- Cook, S.; Weitzman, M.; Auinger, P.; Nguyen, M.; Dietz, W.H. Prevalence of a metabolic syndrome phenotype in adolescents: Findings from the third National Health and Nutrition Examination Survey, 1988–1994. Arch. Pediatr. Adolesc. Med. 2003, 157, 821–827. Available online: https://pubmed.ncbi.nlm.nih.gov/12912790/ (accessed on 20 October 2021). [CrossRef] [PubMed]
- Ford, E.S.; Ajani, U.A.; Mokdad, A.H. The metabolic syndrome and concentrations of C-reactive protein among U.S. youth. Diabetes Care 2005, 28, 878–881. Available online: https://pubmed.ncbi.nlm.nih.gov/15793189/ (accessed on 20 October 2021). [CrossRef]
- de Ferranti, S.D.; Gauvreau, K.; Ludwig, D.S.; Neufeld, E.J.; Newburger, J.W.; Rifai, N. Prevalence of the metabolic syndrome in American adolescents: Findings from the Third National Health and Nutrition Examination Survey. Circulation 2004, 110, 2494–2497. Available online: https://pubmed.ncbi.nlm.nih.gov/15477412/ (accessed on 20 October 2021). [CrossRef]
- Kahn, R.; Buse, J.; Ferrannini, E.; Stern, M. The metabolic syndrome: Time for a critical appraisal—Joint statement from the American Diabetes Association and the European Association for the Study of Diabetes. American Diabetes Association; Diabetes Care. 2005, 28, 2289–3304. Available online: https://care.diabetesjournals.org/content/28/9/2289/ (accessed on 6 April 2021). [CrossRef]
- Bonora, B.M.; Marescotti, M.; Marcuzzo, G.; Avogaro, A.; Fadini, G.P. Synergistic interactions among metabolic syndrome components and homeostasis model assessment of insulin resistance in a middle-aged general population over time. Metab. Syndr. Relat. Disord. 2015, 13, 171–178. Available online: http://www.liebertpub.com/doi/10.1089/met.2014.0163/ (accessed on 6 April 2021). [CrossRef]
- Vaidya, D.; Szklo, M.; Liu, K.; Schreiner, P.J.; Bertoni, A.G.; Ouyang, P. Defining the metabolic syndrome construct: Multi-Ethnic Study of Atherosclerosis (MESA) cross-sectional analysis. Diabetes Care 2007, 30, 2086–2090. [Google Scholar] [CrossRef][Green Version]
- Fadini, G.P.; Coracina, A.; Inchiostro, S.; Tiengo, A.; Avogaro, A.; de Kreutzenberg, S.V. A stepwise approach to assess the impact of clustering cardiometabolic risk factors on carotid intima-media thickness: The metabolic syndrome no-more-than-additive. Eur. J. Prev. Cardiol. 2008, 15, 190–196. Available online: https://pubmed.ncbi.nlm.nih.gov/18391647/ (accessed on 6 April 2021). [CrossRef] [PubMed]
- Baldassarre, D.; Werba, J.P.; Castelnuovo, S.; Frigerio, B.; Amato, M.; Ravani, A.; Veglia, F.; Sirtori, C.R.; Tremoli, E. The metabolic syndrome predicts carotid intima-media thickness no better than the sum of individual risk factors in a lipid clinic population. Atherosclerosis 2010, 210, 214–219. Available online: https://pubmed.ncbi.nlm.nih.gov/20227694/ (accessed on 6 April 2021). [CrossRef] [PubMed]
- Inchiostro, S.; Fadini, G.P.; de Kreutzenberg, S.V.; Citroni, N.; Avogaro, A. Is the Metabolic Syndrome a Cardiovascular Risk Factor Beyond Its Specific Components? J. Am. Coll. Cardiol. 2007, 49, 2465. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0735109707012041/ (accessed on 6 April 2021). [CrossRef] [PubMed]
- Golden, S.H.; Folsom, A.R.; Coresh, J.; Richey Sharrett, A.; Szklo, M.; Brancati, F. Risk factor groupings related to insulin resistance and their synergistic effects on subclinical atherosclerosis: The Atherosclerosis Risk in Communities Study. Diabetes 2002, 51, 3069–3076. Available online: https://pubmed.ncbi.nlm.nih.gov/12351449/ (accessed on 9 May 2021). [CrossRef] [PubMed]
- Rothman, K.J.; Greenland, S.; Walker, A.M. Concepts of interaction. Am. J. Epidemiol. 1980, 112, 467–470. Available online: https://pubmed.ncbi.nlm.nih.gov/7424895/ (accessed on 29 September 2021). [CrossRef]
- Szklo, M.; Nieto, F.J. Defining and Assessing Heterogeneity of Effects: Interaction. In Epidemiology Beyond The Basics, 4th Ed; Jones & Bartlett Learning: Burlington, MA, USA, 2019. [Google Scholar]
- VanDerWeele, T.J.; Knol, M.J. A tutorial on interaction. Epidemiol. Method 2014, 3, 33–72. Available online: https://www.degruyter.com/document/doi/10.1515/em-2013-0005/html?lang=en/ (accessed on 21 January 2022). [CrossRef]
- Da Silva, T.L.N.; Klein, C.H.; De Moura Souza, A.; Barufaldi, L.A.; De Azevedo Abreu, G.; Kuschnir, M.C.C.; de Vasconcellos, M.T.L.; Bloch, K.V. Response rate in the study of cardiovascular risks in adolescents—ERICA. Rev. Saude Publica 2016, 50, 3s. Available online: http://www.rsp.fsp.usp.br/ (accessed on 28 September 2020). [CrossRef]
- de Vasconcellos, M.T.L.; do Silva, P.L.N.; Szklo, M.; Kuschnir, M.C.C.; Klein, C.H.; de Abreu, G.A.; Barufaldi, L.A.; Bloch, K.V. Sampling design for the Study of Cardiovascular Risks in Adolescents (ERICA). Cad. Saude Publica 2015, 31, 921–930. Available online: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0102-311X2015000500005&lng=en&nrm=iso&tlng=en/ (accessed on 28 September 2020). [CrossRef]
- Bloch, K.V.; Szklo, M.; Kuschnir, M.C.C.; de Abreu, G.A.; Barufaldi, L.A.; Klein, C.H.; de Vasconcelos Maurício, T.L.; da Veiga Glória, V.; Figueiredo, V.C.; Dias, A.; et al. The study of cardiovascular risk in adolescents—ERICA: Rationale, design and sample characteristics of a national survey examining cardiovascular risk factor profile in Brazilian adolescents. BMC Public Health 2015, 15, 94. Available online: http://www.biomedcentral.com/1471-2458/15/94/ (accessed on 28 September 2020).
- Alberti, S.G.; Zimmet, P. The IDF Consensus definition of the Metablic Syndrome in Children and Adolescents. Int. Diabetes Fed. 2007, 24, 2-930229. [Google Scholar]
- Cureau, F.V.; Bloch, K.V.; Henz, A.; Schaan, C.W.; Klein, C.H.; de Oliveira, C.L.; Giannini, D.T.; de Leon, E.B.; Abreu, G.d.; Telo, G.H.; et al. Challenges for conducting blood collection and biochemical analysis in a large multicenter school-based study with adolescents: Lessons from ERICA in Brazil. Cad. Saude Publica 2017, 33, e00122816. Available online: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0102-311X2017000404001&lng=en&tlng=en/ (accessed on 28 September 2020). [CrossRef]
- Telo, G.H.; Cureau, F.V.; Szklo, M.; Bloch, K.V.; Schaan, B.D. Prevalence of type 2 diabetes among adolescents in Brazil: Findings from Study of Cardiovascular Risk in Adolescents (ERICA). Pediatr. Diabetes 2019, 20, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Rothman, K.J. Modern Epidemiology; Little Brown & Co: Boston, MA, USA, 1986; 358p. [Google Scholar]
- Onis MDe Onyango, A.W.; Borghi, E.; Siyam, A.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, J.M.; Divers, J.; Isom, S.; Saydah, S.; Imperatore, G.; Pihoker, C.; Marcovina, S.M.; Mayer-Davis, E.J.; Hamman, R.F.; Dolan, L.; et al. Trends in Prevalence of Type 1 and Type 2 Diabetes in Children and Adolescents in the US, 2001–2017. JAMA 2021, 326, 717. [Google Scholar] [CrossRef] [PubMed]
- Fagot-Campagna, A.; Pettitt, D.J.; Engelgau, M.M.; Ríos Burrows, N.; Geiss, L.S.; Valdez, R.; Beckles, G.L.; Saaddine, J.; Gregg, E.W.; Williamson, D.F.; et al. Type 2 diabetes among North adolescents: An epidemiologic health perspective. J. Pediatr. 2000, 136, 664–672. [Google Scholar] [CrossRef]
- Kahkoska, A.R.; Dabelea, D. Diabetes in Youth: A Global Perspective. Endocrinol. Metab. Clin. N. Am. 2021, 50, 491–512. Available online: https://pubmed.ncbi.nlm.nih.gov/34399958/ (accessed on 20 August 2022). [CrossRef]
- Fazeli Farsani, S.; Van Der Aa, M.P.; Van Der Vorst, M.M.J.; Knibbe, C.A.J.; De Boer, A. Global trends in the incidence and prevalence of type 2 diabetes in children and adolescents: A systematic review and evaluation of methodological approaches. Diabetologia 2013, 56, 1471–1488. Available online: https://pubmed.ncbi.nlm.nih.gov/23677041/ (accessed on 20 August 2022). [CrossRef]
- International Diabetes Federation. International Diabetes Federation. IDF Diabetes Atlas, 10th ed; International Diabetes Federation: Brussels, Belgium, 2021. [Google Scholar]
- Wu, H.; Patterson, C.C.; Zhang, X.; Ghani, R.B.A.; Magliano, D.J.; Boyko, E.J.; Ogle, G.D.; Luk, A.O.Y. Worldwide estimates of incidence of type 2 diabetes in children and adolescents in 2021. Diabetes Res. Clin. Pract. 2022, 185, 109785. [Google Scholar] [CrossRef]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- Szklo, M.; Nieto, F.J. Communicating Results of Epidemiologic Studies. In Epidemiology Beyond The Basics, 4th ed.; Jones & Bartlett Learning: Burlington, MA, USA, 2019. [Google Scholar]
- Rothman, K.J. Six persistent research misconceptions. J. Gen. Intern. Med. 2014, 29, 1060–1064. Available online: https://pubmed.ncbi.nlm.nih.gov/24452418/ (accessed on 6 May 2022). [CrossRef]
- Pollock, B.D.; Chen, W.; Harville, E.W.; Shu, T.; Fonseca, V.; Mauvais-Jarvis, F.; Kelly, T.N.; Bazzano, L.A. Differential sex effects of systolic blood pressure and LDL-C on Type 2 diabetes: Life-course data from the Bogalusa Heart Study. J. Diabetes 2018, 10, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, H.N.; Zhang, Y.L.; Hernandez-Ono, A. Regulation of Plasma Triglycerides in Insulin Resistance and Diabetes. Arch. Med. Res. 2005, 36, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Ryu, K.S.; Ye, H.; Kang, J.; You, N.Y.; Choi, K.S.; Hwangbo, Y.; Lee, J.W.; Cha, H.S. Risk Factors of Undiagnosed Diabetes Mellitus among Korean Adults: A National Cross-Sectional Study Using the KNHANES Data. Public Health 2021, 18, 1195. [Google Scholar] [CrossRef]
- Royston, P.; Altman, D.G.; Sauerbrei, W. Dichotomizing continuous predictors in multiple regression: A bad idea. Stat. Med. 2006, 25, 127–141. Available online: https://pubmed.ncbi.nlm.nih.gov/16217841/ (accessed on 13 December 2021). [CrossRef] [PubMed]
- Janssen, I.; Heymsfield, S.B.; Allison, D.B.; Kotler, D.P.; Ross, R. Body mass index and waist circumference independently contribute to the prediction of nonabdominal, abdominal subcutaneous, and visceral fat. Am. J. Clin. Nutr. 2002, 75, 683–688. Available online: https://pubmed.ncbi.nlm.nih.gov/11916754/ (accessed on 9 June 2021). [CrossRef] [PubMed]
- Rader, D.J. Effect of Insulin Resistance, Dyslipidemia, and Intra-abdominal Adiposity on the Development of Cardiovascular Disease and Diabetes Mellitus. Am. J. Med. 2007, 120 (Suppl. 1), S12–S18. Available online: https://pubmed.ncbi.nlm.nih.gov/17320517/ (accessed on 15 June 2021). [CrossRef] [PubMed]
- Tripathy, D.; Mohanty, P.; Dhindsa, S.; Syed, T.; Ghanim, H.; Aljada, A.; Dandona, P. Elevation of free fatty acids induces inflammation and impairs vascular reactivity in healthy subjects. Diabetes 2003, 52, 2882–2887. Available online: https://pubmed.ncbi.nlm.nih.gov/14633847/ (accessed on 22 October 2021). [CrossRef]
- American Diabetes Association. Screening for Diabetes. Diabetes Care 2002, 25 (Suppl. 1), S21–S24. Available online: http://diabetesjournals.org/care/article-pdf/25/suppl_1/s21/454886/s21.pdf/ (accessed on 20 December 2021). [CrossRef]
- Wallace, A.S.; Wang, D.; Shin, J.I.; Selvin, E. Screening and diagnosis of prediabetes and diabetes in us children and adolescents. Pediatrics 2020, 146, e20200265. [Google Scholar] [CrossRef]
- Savva, S.C.; Tornaritis, M.; Savva, M.E.; Kourides, Y.; Panagi, A.; Silikiotou, N.; Georgiou, C.; Kafatos, A. Waist circumference and waist-to-height ratio are better predictors of cardiovascular disease risk factors in children than body mass index. Int. J. Obes. Relat. Metab. Disord. J. Int. Assoc. Study Obes. 2000, 24, 1453–1458. [Google Scholar] [CrossRef]
- Ma, L.; Cai, L.; Deng, L.; Zhu, Y.; Ma, J.; Jing, J.; Chen, Y. Waist Circumference is Better Than Other Anthropometric Indices for Predicting Cardiovascular Disease Risk Factors in Chinese Children—A Cross-Sectional Study in Guangzhou. J. Atheroscler. Thromb. 2016, 23, 320–329. [Google Scholar] [CrossRef] [PubMed]
- Tavares, L.F.; Fonseca, S.C.; Garcia Rosa, M.L.; Yokoo, E.M. Relationship between ultra-processed foods and metabolic syndrome in adolescents from a Brazilian Family Doctor Program. Public Health Nutr. 2012, 15, 82–87. Available online: https://pubmed.ncbi.nlm.nih.gov/21752314/ (accessed on 1 October 2022). [CrossRef] [PubMed]
- Chan, T.F.; Lin, W.T.; Huang, H.L.; Lee, C.Y.; Wu, P.W.; Chiu, Y.W.; Huang, C.; Tsai, S.; Lin, C.; Lee, C. Consumption of sugar-sweetened beverages is associated with components of the metabolic syndrome in adolescents. Nutrients 2014, 6, 2088–2103. Available online: https://pubmed.ncbi.nlm.nih.gov/24858495/ (accessed on 2 October 2022). [CrossRef] [PubMed]
- Fornari, E.; Maffeis, C. Treatment of Metabolic Syndrome in Children. Front. Endocrinol. 2019, 10, 702. [Google Scholar] [CrossRef]
- DeBoer, M.D. Assessing and Managing the Metabolic Syndrome in Children and Adolescents. Nutrients 2019, 11, 1788. [Google Scholar] [CrossRef]
- Styne, D.M.; Arslanian, S.A.; Connor, E.L.; Farooqi, I.S.; Murad, M.H.; Silverstein, J.H.; Yanovski, J.A. Pediatric Obesity—Assessment, Treatment, and Prevention: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2017, 102, 709–757. [Google Scholar] [CrossRef]
- Morrison, J.A.; Friedman, L.A.; Wang, P.; Glueck, C.J. Metabolic Syndrome in Childhood Predicts Adult Metabolic Syndrome and Type 2 Diabetes Mellitus 25 to 30 Years Later. J. Pediatr. 2008, 152, 201–206. Available online: https://www.sciencedirect.com/science/article/pii/S0022347607008566/ (accessed on 11 September 2022). [CrossRef]
- Magnussen, C.G.; Koskinen, J.; Chen, W.; Thomson, R.; Schmidt, M.D.; Srinivasan, S.R.; Kivimäki, M.; Mattsson, N.; Kähönen, M.; Laitinen, T.; et al. Pediatric metabolic syndrome predicts adulthood metabolic syndrome, subclinical atherosclerosis, and type 2 diabetes mellitus but is no better than body mass index alone: The Bogalusa Heart Study and the Cardiovascular Risk in Young Finns Study. Circulation 2010, 122, 1604–1611. [Google Scholar] [CrossRef]
- Asghari, G.; Hasheminia, M.; Heidari, A.; Mirmiran, P.; Guity, K.; Shahrzad, M.K.; Azizi, F.; Hadaegh, F. Adolescent metabolic syndrome and its components associations with incidence of type 2 diabetes in early adulthood: Tehran lipid and glucose study. Diabetol. Metab. Syndr. 2021, 13, 1. [Google Scholar] [CrossRef]
- Reinehr, T.; Wunsch, R.; Pütter, C.; Scherag, A. Relationship between Carotid Intima-Media Thickness and Metabolic Syndrome in Adolescents. J. Pediatr. 2013, 163, 327–332.e4. [Google Scholar] [CrossRef]
- Mente, A.; Yusuf, S.; Islam, S.; McQueen, M.J.; Tanomsup, S.; Onen, C.L.; Rangarajan, S.; Gerstein, H.C.; Anand, S.S.; INTERHEART Investigators. Metabolic syndrome and risk of acute myocardial infarction a case-control study of 26,903 subjects from 52 countries. J. Am. Coll. Cardiol. 2010, 55, 2390–2398. Available online: https://pubmed.ncbi.nlm.nih.gov/20488312/ (accessed on 16 December 2021). [CrossRef] [PubMed]
- Kuschnir, M.C.C.; Bloch, K.V.; Szklo, M.; Klein, C.H.; Barufaldi, L.A.; Abreu, G.A.; Schaan, B.; da Veiga, G.V.; da Silva, T.L.N.; de Vasconcellos, M.T.L.; et al. ERICA: Prevalence of metabolic syndrome in Brazilian adolescents. Rev. Saude Publica 2016, 50 (Suppl. 1), 11s. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | n | |||
|---|---|---|---|---|
| Continuous | Median | 1ºQ 3ºQ | ||
| Age | 37,815 | 15 | 13 | 16 |
| Categorical | (%) | 95% Confidence intervals | ||
| Female | 22,682 | 50.2 | ||
| Smoking (≥1 cigarette smoked in the last 30 days) | 1406 | 4.2 | 3.8 | 4.7 |
| Alcohol consumption (≥1 drink in the last 30 days) | 7685 | 21.6 | 20.3 | 23.0 |
| Sedentary behavior γ | 14,133 | 40.5 | 38.9 | 42.1 |
| Physical inactivity (≤ 420 min per week) | 24,713 | 62.7 | 61.7 | 63.8 |
| Obesity (%) | 3097 | 9.2 | 8.5 | 10.0 |
| Public Schools | 27,990 | 77.8 | 72.4 | 82.3 |
| Metabolic syndrome * | 861 | 2.6 | 2.3 | 2.9 |
| Components of metabolic syndrome | ||||
| One component | 13,025 | 33.7 | 31.9 | 35.6 |
| Two components | 3390 | 9.5 | 8.5 | 10.6 |
| Three components | 825 | 2.5 | 2.1 | 2.9 |
| Four components | 134 | 0.4 | 0.3 | 0.6 |
| Five components | 9 | 0.1 | 0.0 | 0.2 |
| Metabolic syndrome components | ||||
| Elevated waist circumference *** | 4386 | 12.6 | 11.6 | 13.7 |
| High blood pressure # | 2677 | 8.2 | 7.6 | 8.9 |
| High glucose δ | 1147 | 4.1 | 3.5 | 4.8 |
| High triglycerides λ | 1712 | 4.6 | 4.1 | 5.1 |
| Low HDL-c ** (%) | 13,076 | 32.7 | 30.3 | 35.2 |
| Type 2 Diabetes Mellitus Γ | 1227 | 3.28 | 2.91 | 3.69 |
| Identified by a physician θ | 1126 | 3.05 | 2.69 | 3.46 |
| Undiagnosed diabetes φ | 101 | 0.23 | 0.16 | 0.31 |
| Interaction Measures | |||
|---|---|---|---|
| Elevated WC * and/or High BP # | |||
| Normal HDL-c | Low HDL-c ** | ||
| Normal TG | 1 | PR = 0.83 (0.52, 1.31) | RERI TG * HDL-c = 2.53 (−0.41, 5.46) |
| High TG λ | PR = 1.53 (0.58, 4.04) | PR = 3.88 (1.88, 8.01) | Interaction ratio TG*HDL-c = 3.08 (0.90, 10.55) |
| Low HDL-c ** or High BP # | |||
| Normal WC | Elevated WC * | ||
| Normal TG | 1 | PR = 1.00 (0.53, 1.91) | RERI TG * WC = 2.86 (−2.89, 8.61) |
| High TG λ | PR = 1.89 (0.87, 4.14) | PR = 4.76 (1.42, 15.95) | Interaction ratio TG*WC = 2.51 (0.75, 8.44) |
| High TG λ or High BP # | |||
| Normal HDL-c | Low HDL-c ** | ||
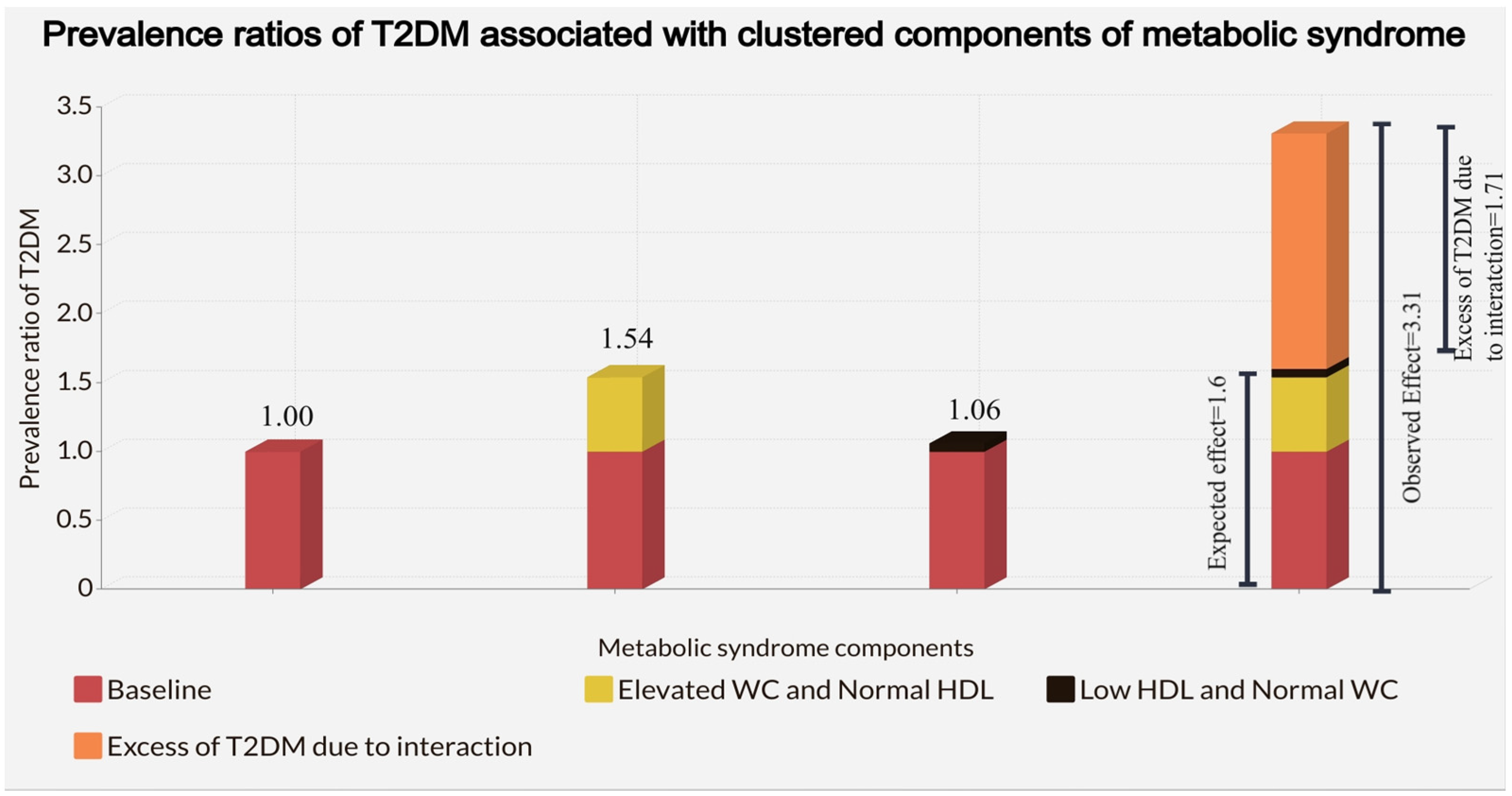
| Normal WC | 1 | PR = 1.06 (0.45, 2.47) | RERI WC * HDL-c = 1.71 (−1.05, 4.46) |
| Elevated WC * | PR = 1.54 (0.63, 3.78) | PR = 3.31 (1.18, 9.25) | Interaction ratio WC*HDL-c = 2.03 (0.59, 7.01) |
| High TG λ or Low HDL-c ** | |||
| Normal BP | High BP # | ||
| Normal WC | 1 | PR = 0.41 (0.22, 0.75) | RERI WC * BP = 0.97 (0.15, 1.79) |
| Elevated WC * | PR = 0.73 (0.36, 1.47) | PR = 1.10 (0.46, 2.68) | Interaction ratio WC * BP = 3.71 (1.42, 9.70) |
| Elevated WC * and/ or Low HDL-c ** | |||
| Normal TG | High TG λ | ||
| Normal BP | 1 | PR = 3.29 (1.58, 6.83) | RERI BP * TG = 0.50 (−4.17, 5.18) |
| High BP # | PR = 1.02 (0.55, 1.89) | PR = 3.81 (1.26, 11.58) | Interaction ratio BP * TG = 1.14 (0.27, 4.80) |
| Elevated WC * and/or High TG λ | |||
| Normal HDL-c | Low HDL-c ** | ||
| Normal BP | 1 | PR = 1.02 (0.63, 1.64) | RERI BP * HDL-c = 0.27 (−0.99, 1.53) |
| High BP # | PR = 0.92 (0.41, 2.01) | PR = 1.21 (0.54, 2.71) | Interaction ratio BP * HDL-c = 1.30 (0.39, 4.35) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deusdará, R.; de Moura Souza, A.; Szklo, M. Positive Additive and Multiplicative Interactions among Clustered Components of Metabolic Syndrome with Type 2 Diabetes Mellitus among Brazilian Adolescent Students. Nutrients 2022, 14, 4640. https://doi.org/10.3390/nu14214640
Deusdará R, de Moura Souza A, Szklo M. Positive Additive and Multiplicative Interactions among Clustered Components of Metabolic Syndrome with Type 2 Diabetes Mellitus among Brazilian Adolescent Students. Nutrients. 2022; 14(21):4640. https://doi.org/10.3390/nu14214640
Chicago/Turabian StyleDeusdará, Rodolfo, Amanda de Moura Souza, and Moyses Szklo. 2022. "Positive Additive and Multiplicative Interactions among Clustered Components of Metabolic Syndrome with Type 2 Diabetes Mellitus among Brazilian Adolescent Students" Nutrients 14, no. 21: 4640. https://doi.org/10.3390/nu14214640
APA StyleDeusdará, R., de Moura Souza, A., & Szklo, M. (2022). Positive Additive and Multiplicative Interactions among Clustered Components of Metabolic Syndrome with Type 2 Diabetes Mellitus among Brazilian Adolescent Students. Nutrients, 14(21), 4640. https://doi.org/10.3390/nu14214640