
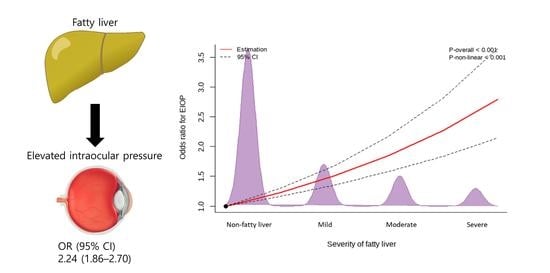
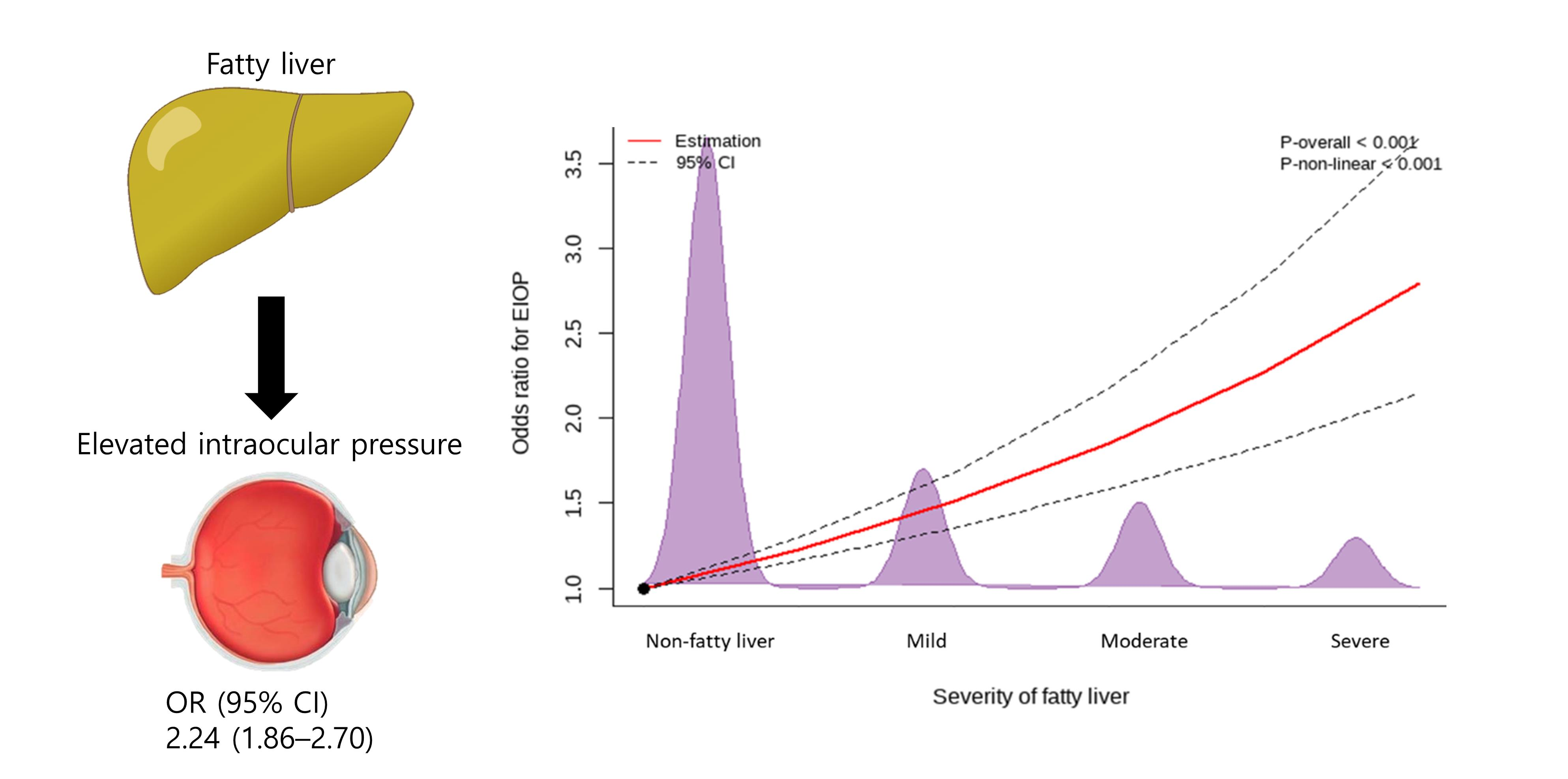
Fatty Liver Is an Independent Risk Factor for Elevated Intraocular Pressure
 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
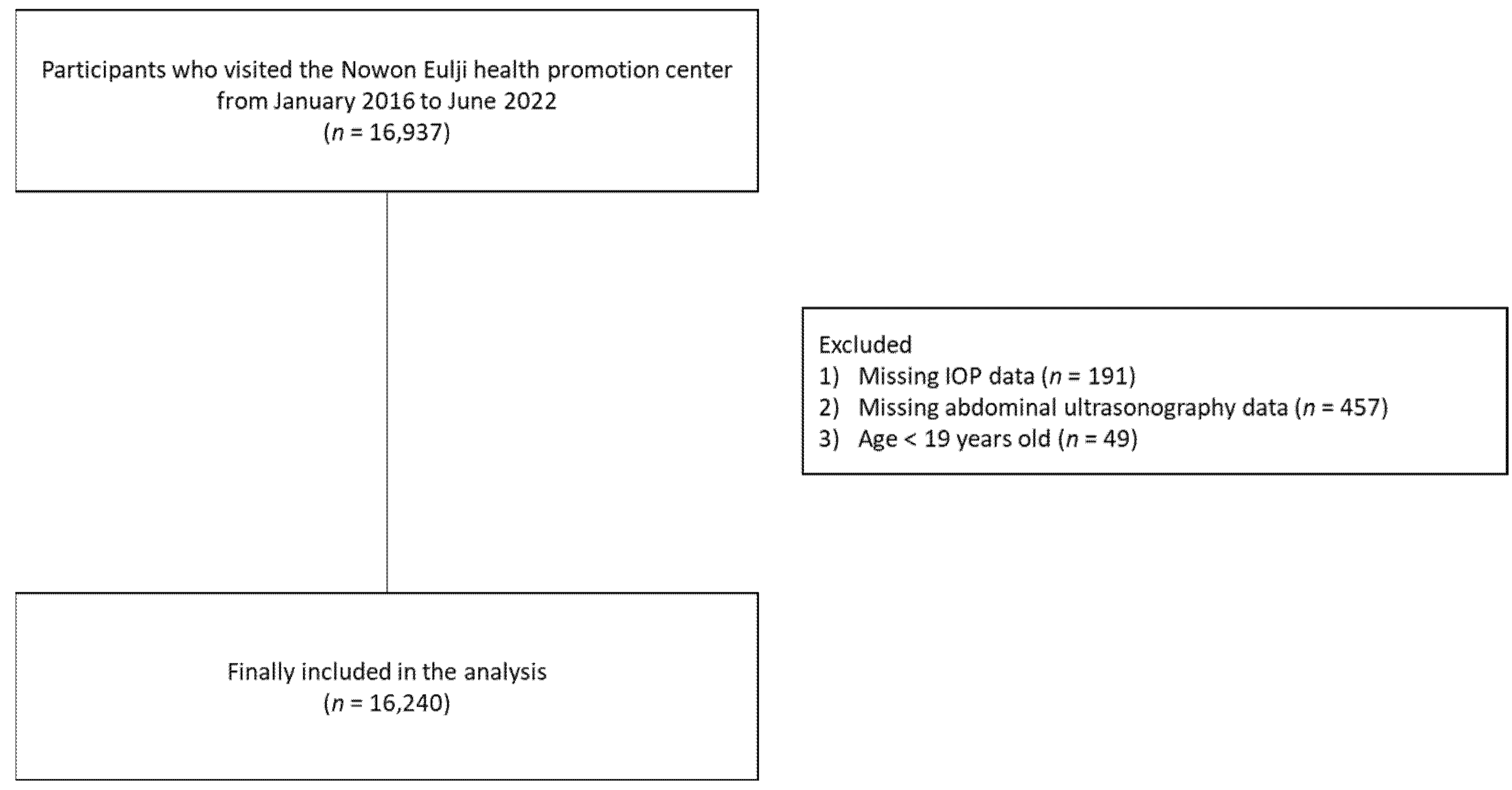
2.1. Study Population
2.2. Assessment of Fatty Liver
2.3. IOP Measurement
2.4. Assessment of Insulin Resistance
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Study Population
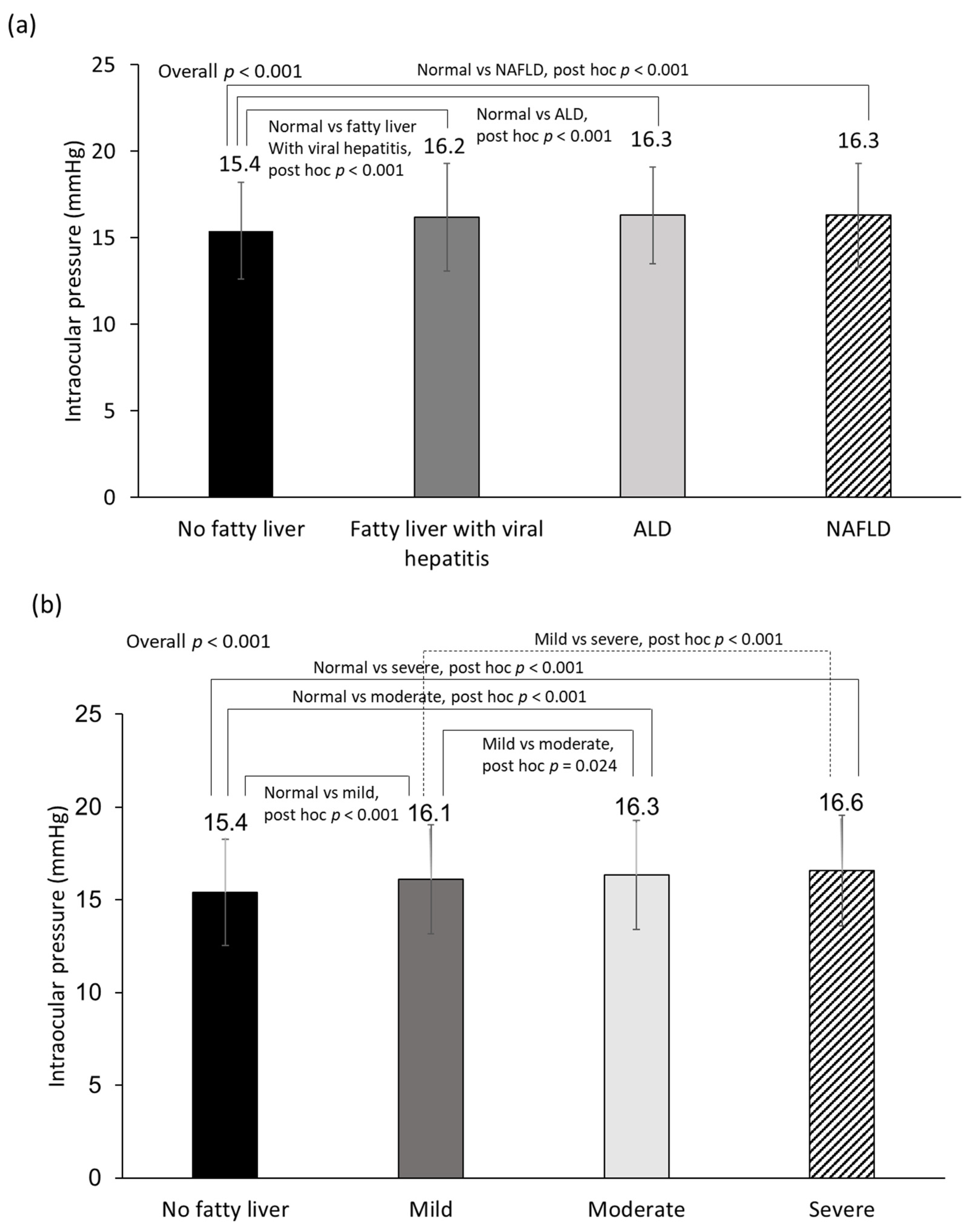
3.2. Relationship between Fatty Liver and EIOP
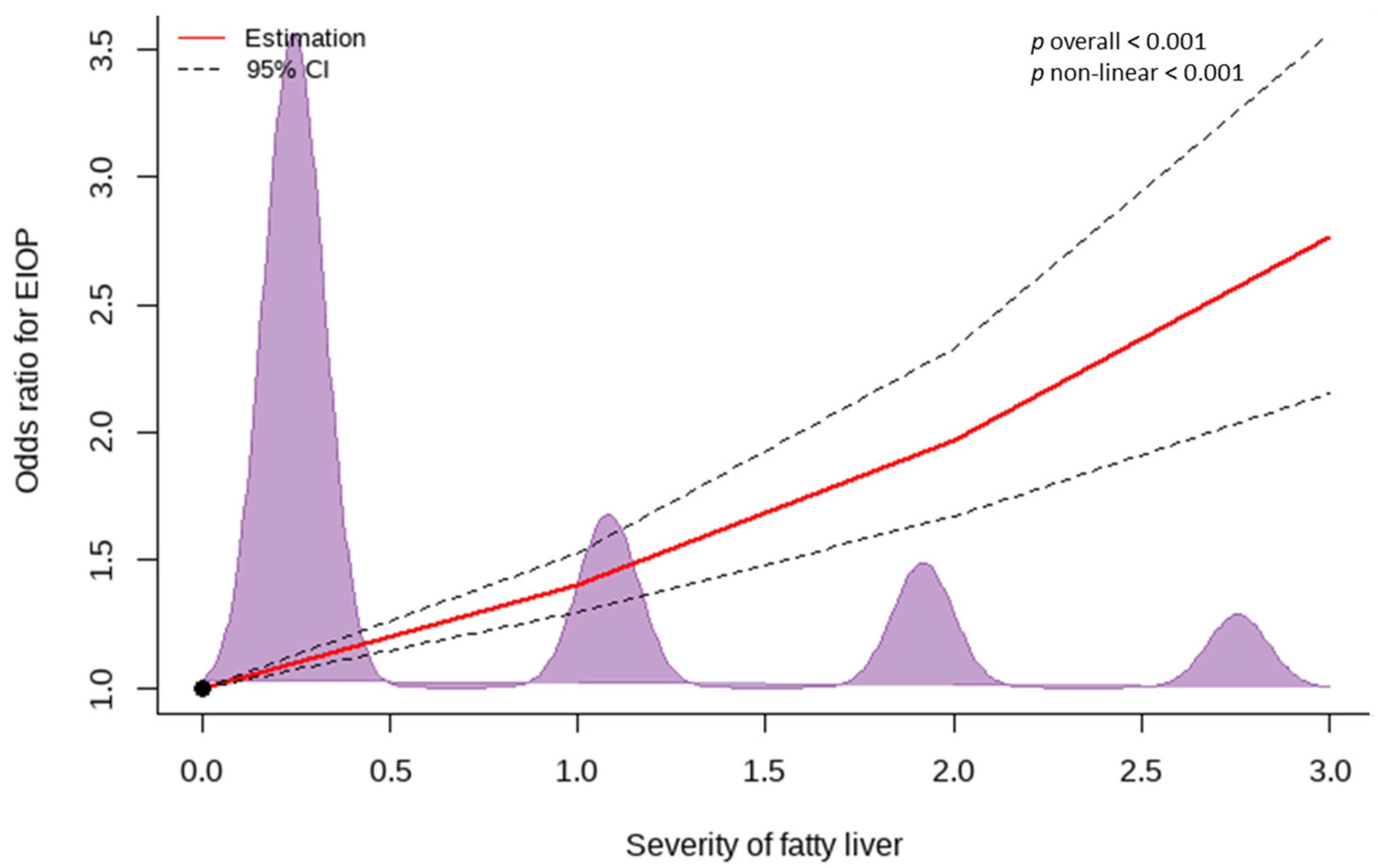
3.3. Dose–Response Relationship between EIOP and the Severity of Fatty Liver
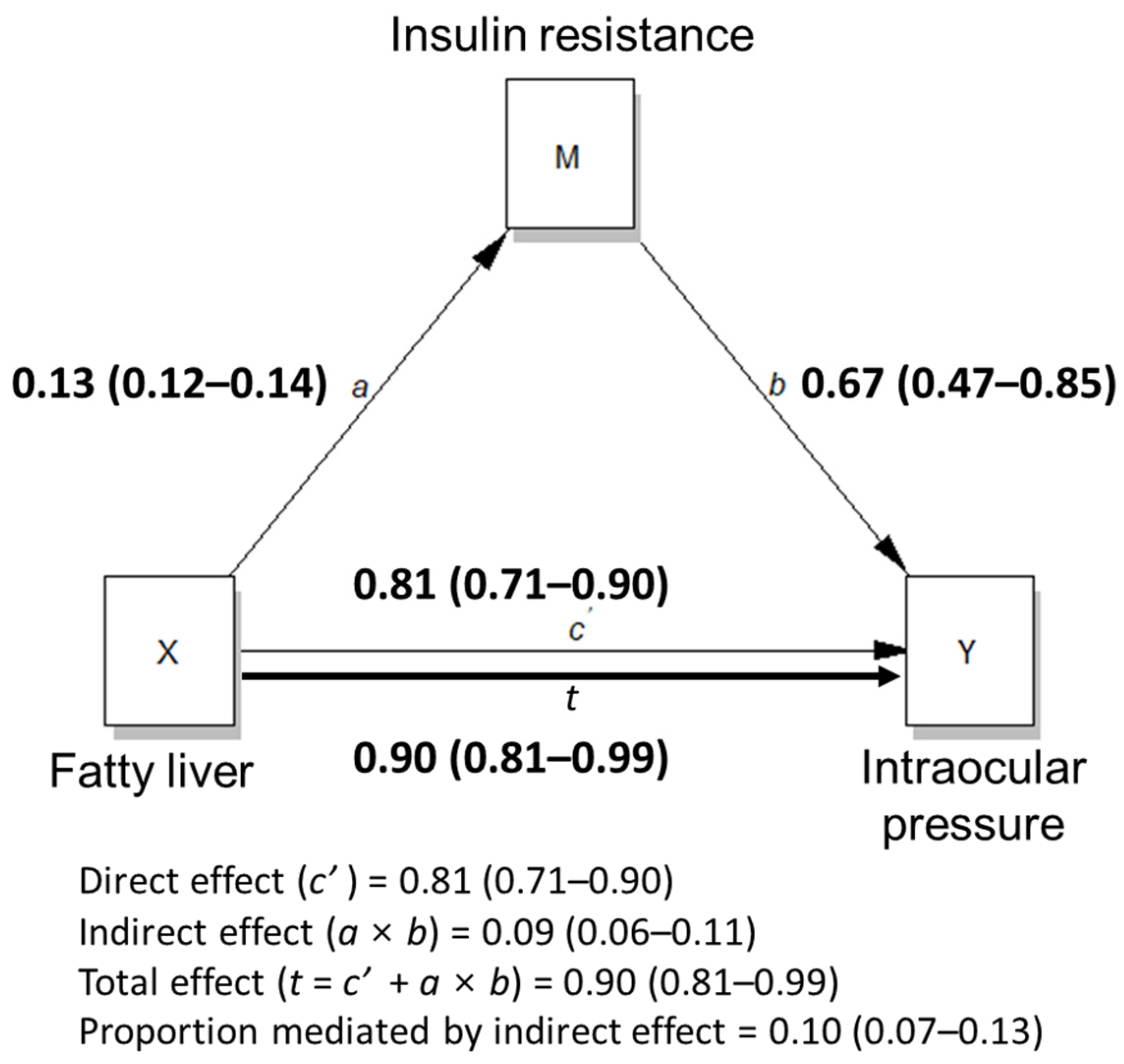
3.4. Insulin Resistance-Mediated Effect of Fatty Liver on IOP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, M.; Zheng, B.; Wang, Q.; Sun, X. Impact of Visual Field Testing on Intraocular Pressure Change Trends in Healthy People and Glaucoma Patients. J. Ophthalmol. 2020, 2020, 7936205. [Google Scholar] [CrossRef] [PubMed]
- Kitazawa, Y.; Horie, T.; Aoki, S.; Suzuki, M.; Nishioka, K. Untreated Ocular Hypertension: A Long-Term Prospective Study. Arch. Ophthalmol. 1977, 95, 1180–1184. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, S.; Hara, K.; Sano, I.; Onoda, K.; Nagai, A.; Yamaguchi, S.; Tanito, M. Systemic factors associated with intraocular pressure among subjects in a health examination program in Japan. PLoS ONE 2020, 15, e0234042. [Google Scholar] [CrossRef] [PubMed]
- Nemesure, B.; Wu, S.-Y.; Hennis, A.; Leske, M.C.; Barbados Eye Studies Group. Factors Related to the 4-Year Risk of High Intraocular Pressure: The Barbados Eye Studies. Arch. Ophthalmol. 2003, 121, 856–862. [Google Scholar] [CrossRef]
- Nakano, T.; Tatemichi, M.; Miura, Y.; Sugita, M.; Kitahara, K. Long-Term Physiologic Changes of Intraocular Pressure: A 10-year longitudinal analysis in young and middle-aged Japanese men. Ophthalmology 2005, 112, 609–616. [Google Scholar] [CrossRef]
- Mori, K.; Ando, F.; Nomura, H.; Sato, Y.; Shimokata, H. Relationship between intraocular pressure and obesity in Japan. Int. J. Epidemiol. 2000, 29, 661–666. [Google Scholar] [CrossRef]
- Le, M.H.; Yeo, Y.H.; Li, X.; Li, J.; Zou, B.; Wu, Y.; Ye, Q.; Huang, D.Q.; Zhao, C.; Zhang, J.; et al. 2019 Global NAFLD Prevalence: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2021. In Press. [Google Scholar] [CrossRef]
- Im, H.J.; Ahn, Y.C.; Wang, J.-H.; Lee, M.M.; Son, C.G. Systematic review on the prevalence of nonalcoholic fatty liver disease in South Korea. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101526. [Google Scholar] [CrossRef]
- Allen, A.M.; Van Houten, H.K.; Sangaralingham, L.R.; Talwalkar, J.A.; McCoy, R.G. Healthcare Cost and Utilization in Nonalcoholic Fatty Liver Disease: Real-World Data from a Large U.S. Claims Database. Hepatology 2018, 68, 2230–2238. [Google Scholar] [CrossRef]
- Dharmalingam, M.; Yamasandhi, P.G. Nonalcoholic Fatty Liver Disease and Type 2 Diabetes Mellitus. Indian J. Endocrinol. Metab. 2018, 22, 421–428. [Google Scholar] [CrossRef]
- Bang, K.B.; Cho, Y.K. Comorbidities and Metabolic Derangement of NAFLD. J. Lifestyle Med. 2015, 5, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Byrne, C.D.; Tilg, H. NAFLD and increased risk of cardiovascular disease: Clinical associations, pathophysiological mechanisms and pharmacological implications. Gut 2020, 69, 1691–1705. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Yu, R.; Xiong, Y.; Du, F.; Zhu, S. A vicious circle between insulin resistance and inflammation in nonalcoholic fatty liver disease. Lipids Health Dis. 2017, 16, 203. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.-J.; Lee, Y.-H.; Cha, B.-S. Causal Relationship of Non-alcoholic Fatty Liver Disease with Obesity and Insulin Resistance. JKD 2014, 15, 76–81. [Google Scholar] [CrossRef][Green Version]
- Carr, R.M.; Correnti, J. Insulin resistance in clinical and experimental alcoholic liver disease. Ann. N. Y. Acad. Sci. 2015, 1353, 1–20. [Google Scholar] [CrossRef]
- Hernaez, R.; Lazo, M.; Bonekamp, S.; Kamel, I.; Brancati, F.L.; Guallar, E.; Clark, J.M. Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: A meta-analysis. Hepatology 2011, 54, 1082–1090. [Google Scholar] [CrossRef]
- Dunn, W.; Angulo, P.; Sanderson, S.; Jamil, L.H.; Stadheim, L.; Rosen, C.; Malinchoc, M.; Kamath, P.S.; Shah, V.H. Utility of a new model to diagnose an alcohol basis for steatohepatitis. Gastroenterology 2006, 131, 1057–1063. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Muniyappa, R.; Lee, S.; Chen, H.; Quon, M.J. Current approaches for assessing insulin sensitivity and resistance in vivo: Advantages, limitations, and appropriate usage. Am. J. Physiol. Endocrinol. Metab. 2008, 294, E15–E26. [Google Scholar] [CrossRef]
- Kwon, Y.J.; Kim, J.H.; Jung, D.H. Association Between Nonalcoholic Fatty Liver Disease and Intraocular Pressure in Korean Adults. J. Glaucoma 2018, 27, 1099–1104. [Google Scholar] [CrossRef]
- Klein, B.E.; Klein, R.; Knudtson, M.D. Intraocular pressure and systemic blood pressure: Longitudinal perspective: The Beaver Dam Eye Study. Br. J. Ophthalmol. 2005, 89, 284–287. [Google Scholar] [CrossRef] [PubMed]
- Reddy, A.; Halenda, K.; Cromer, P.; Chen, L.; Butler, J.; Raed, A.; Bhagatwala, J.; Sponseller, T.; Bollinger, K.; Zhu, H.; et al. The Association of Intraocular Pressure with Obesity and Cardiometabolic Risk in a Young Farmworker Population. J. Glaucoma 2021, 30, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Cho, J.; Kim, M.H.; Guallar, E. The association of blood pressure and primary open-angle glaucoma: A meta-analysis. Am. J. Ophthalmol. 2014, 158, 615–627.e619. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, K.; Yasuda, M.; Ninomiya, T.; Hata, J.; Hashimoto, S.; Yoshitomi, T.; Kiyohara, Y.; Ishibashi, T. Insulin Resistance Is a Risk Factor for Increased Intraocular Pressure: The Hisayama Study. Investig. Ophthalmol. Vis. Sci. 2015, 56, 7983–7987. [Google Scholar] [CrossRef]
- Chun, Y.H.; Han, K.; Park, S.H.; Park, K.M.; Yim, H.W.; Lee, W.C.; Park, Y.G.; Park, Y.M. Insulin resistance is associated with intraocular pressure elevation in a non-obese Korean population. PLoS ONE 2015, 10, e112929. [Google Scholar] [CrossRef]
- Oh, S.W.; Lee, S.; Park, C.; Kim, D.J. Elevated intraocular pressure is associated with insulin resistance and metabolic syndrome. Diabetes Metab. Res. Rev. 2005, 21, 434–440. [Google Scholar] [CrossRef]
- Seddon, J.M.; Schwartz, B.; Flowerdew, G. Case-control study of ocular hypertension. Arch. Ophthalmol. 1983, 101, 891–894. [Google Scholar] [CrossRef]
- Yoshida, M.; Ishikawa, M.; Kokaze, A.; Sekine, Y.; Matsunaga, N.; Uchida, Y.; Takashima, Y. Association of life-style with intraocular pressure in middle-aged and older Japanese residents. Jpn. J. Ophthalmol. 2003, 47, 191–198. [Google Scholar] [CrossRef]
- Song, J.E.; Kim, J.M.; Lee, M.Y.; Jang, H.J.; Park, K.H. Effects of Consumption of Alcohol on Intraocular Pressure: Korea National Health and Nutrition Examination Survey 2010 to 2011. Nutrients 2020, 12, 2420. [Google Scholar] [CrossRef]
- Wang, H.; Mehal, W.; Nagy, L.E.; Rotman, Y. Immunological mechanisms and therapeutic targets of fatty liver diseases. Cell. Mol. Immunol. 2021, 18, 73–91. [Google Scholar] [CrossRef]
- Fatkhullina, A.R.; Peshkova, I.O.; Koltsova, E.K. The Role of Cytokines in the Development of Atherosclerosis. Biochemistry 2016, 81, 1358–1370. [Google Scholar] [CrossRef] [PubMed]
- Flammer, J.; Haefliger, I.O.; Orgül, S.; Resink, T. Vascular dysregulation: A principal risk factor for glaucomatous damage? J. Glaucoma 1999, 8, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.-Y.; Li, J.; Xu, M.; Wang, T.-G.; Sun, W.-W.; Chen, Y.; Bi, Y.-F.; Wang, W.-Q.; Ning, G. Elevated whole blood viscosity is associated with insulin resistance and non-alcoholic fatty liver. Clin. Endocrinol. 2015, 83, 806–811. [Google Scholar] [CrossRef] [PubMed]
- Karadag, R.; Arslanyilmaz, Z.; Aydin, B.; Hepsen, I.F. Effects of body mass index on intraocular pressure and ocular pulse amplitude. Int. J. Ophthalmol. 2012, 5, 605–608. [Google Scholar] [CrossRef]
- Fabbrini, E.; Sullivan, S.; Klein, S. Obesity and nonalcoholic fatty liver disease: Biochemical, metabolic, and clinical implications. Hepatology 2010, 51, 679–689. [Google Scholar] [CrossRef]
- Parekh, A.; Srivastava, S.; Bena, J.; Albini, T.; Nguyen, Q.D.; Goldstein, D.A. Risk Factors Associated with Intraocular Pressure Increase in Patients with Uveitis Treated with the Fluocinolone Acetonide Implant. JAMA Ophthalmol. 2015, 133, 568–573. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Non-Fatty Liver Group | Fatty Liver Group | Total Participants | p * |
|---|---|---|---|---|
| (n = 10,454) | (n = 5786) | (n = 16,240) | ||
| Male sex, n (%) | 4637 (44.4%) | 4229 (73.1%) | 8866 (54.6%) | <0.001 |
| Age, years | 46.1 ± 12.5 | 46.7 ± 12.3 | 46.3 ± 12.4 | 0.002 |
| BMI, kg/m2 | 22.5 ± 2.8 | 26.5 ± 3.3 | 24.0 ± 3.5 | <0.001 |
| WC, cm | 80.5 ± 8.4 | 91.7 ± 9.3 | 84.5 ± 10.2 | <0.001 |
| MBP | 86.6 ± 10.5 | 93.1 ± 10.7 | 88.9 ± 11.0 | <0.001 |
| Smoking status, n (%) | <0.001 | |||
| Never-smoker | 8170 (78.4%) | 3663 (63.5%) | 11833 (73.1%) | |
| Former smoker | 806 (7.7%) | 766 (13.3%) | 1572 (9.7%) | |
| Current smoker | 1449 (13.9%) | 1342 (23.3%) | 2791 (17.2%) | |
| Current drinker, n (%) | 5526 (53.0%) | 3280 (56.8%) | 8806 (54.4%) | <0.001 |
| Regular exerciser, n (%) | 1938 (18.6%) | 1047 (18.1%) | 2985 (18.4%) | 0.495 |
| Hematocrit, % | 42.3 ± 4.0 | 44.4 ± 3.9 | 43.1 ± 4.1 | <0.001 |
| FPG, mg/dL | 87.1 ± 15.7 | 99.2 ± 26.5 | 91.4 ± 21.0 | <0.001 |
| HOMA-IR | 0.8 ± 1.4 | 1.7 ± 1.8 | 1.1 ± 1.6 | <0.001 |
| HbA1c, % | 5.5 ± 0.6 | 5.9 ± 1.0 | 5.6 ± 0.8 | <0.001 |
| Total cholesterol, mg/dL | 190.2 ± 34.3 | 199.3 ± 39.3 | 193.5 ± 36.4 | <0.001 |
| AST, U/L | 24.0 ± 13.7 | 30.5 ± 17.2 | 26.3 ± 15.4 | <0.001 |
| ALT, U/L | 21.5 ± 16.8 | 38.0 ± 28.0 | 27.4 ± 22.9 | <0.001 |
| hsCRP, mg/dL | 0.1 ± 0.3 | 0.2 ± 0.3 | 0.1 ± 0.3 | <0.001 |
| HBV, n (%) | 327 (3.1%) | 121 (2.1%) | 448 (2.8%) | <0.001 |
| HCV, n (%) | 25 (0.2%) | 15 (0.3%) | 40 (0.2%) | 0.934 |
| DM, n (%) | 451 (4.3%) | 935 (16.2%) | 1386 (8.5%) | <0.001 |
| HTN, n (%) | 1491 (14.3%) | 1947 (33.7%) | 3438 (21.2%) | <0.001 |
| Dyslipidemia, n (%) | 2498 (23.9%) | 3225 (55.7%) | 5723 (35.2%) | <0.001 |
| IOP, mmHg | 15.4 ± 2.9 | 16.3 ± 2.9 | 15.7 ± 2.9 | <0.001 |
| EIOP, n (%) | 206 (2.0%) | 249 (4.3%) | 455 (2.8%) | <0.001 |
| EIOP | Unadjusted | Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p * | OR (95% CI) | p * | OR (95% CI) | p * | OR (95% CI) | p * | |
| No fatty liver | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||
| Fatty liver | 2.24 (1.86–2.70) | <0.001 | 1.45 (1.16–1.80) | 0.001 | 1.47 (1.18–1.84) | 0.001 | 1.36 (1.08–1.71) | 0.008 |
| EIOP | Unadjusted | Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p * | OR (95% CI) | p-value | OR (95% CI) | p * | OR (95% CI) | p * | |
| No fatty liver | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | ||||
| Fatty liver with viral hepatitis | 1.90 (0.77–4.69) | 0.164 | 1.10 (0.44–2.75) | 0.846 | 1.07 (0.43–2.71) | 0.879 | 1.01 (0.40–2.54) | 0.991 |
| ALD | 2.55 (1.86–3.50) | <0.001 | 1.63 (1.17–2.27) | 0.004 | 2.02 (1.43–2.85) | <0.001 | 1.80 (1.27–2.56) | 0.001 |
| NAFLD | 2.18 (1.78–2.66) | <0.001 | 1.40 (1.10–1.77) | 0.005 | 1.35 (1.07–1.72) | 0.013 | 1.26 (0.99–1.61) | 0.064 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.-H.; Kwon, Y.-J.; Lee, H.S.; Han, J.H.; Joung, B.; Kim, S.J. Fatty Liver Is an Independent Risk Factor for Elevated Intraocular Pressure. Nutrients 2022, 14, 4455. https://doi.org/10.3390/nu14214455
Lee J-H, Kwon Y-J, Lee HS, Han JH, Joung B, Kim SJ. Fatty Liver Is an Independent Risk Factor for Elevated Intraocular Pressure. Nutrients. 2022; 14(21):4455. https://doi.org/10.3390/nu14214455
Chicago/Turabian StyleLee, Jun-Hyuk, Yu-Jin Kwon, Hye Sun Lee, Jee Hye Han, Boyoung Joung, and Sung Jin Kim. 2022. "Fatty Liver Is an Independent Risk Factor for Elevated Intraocular Pressure" Nutrients 14, no. 21: 4455. https://doi.org/10.3390/nu14214455
APA StyleLee, J.-H., Kwon, Y.-J., Lee, H. S., Han, J. H., Joung, B., & Kim, S. J. (2022). Fatty Liver Is an Independent Risk Factor for Elevated Intraocular Pressure. Nutrients, 14(21), 4455. https://doi.org/10.3390/nu14214455