
Improving the Nutrient Quality of Foods and Beverages Using Product Specific Standards for Nutrients to Limit Will Substantially Reduce Mean Population Intakes of Energy, Sodium, Saturated Fat and Sugars towards WHO Guidelines

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
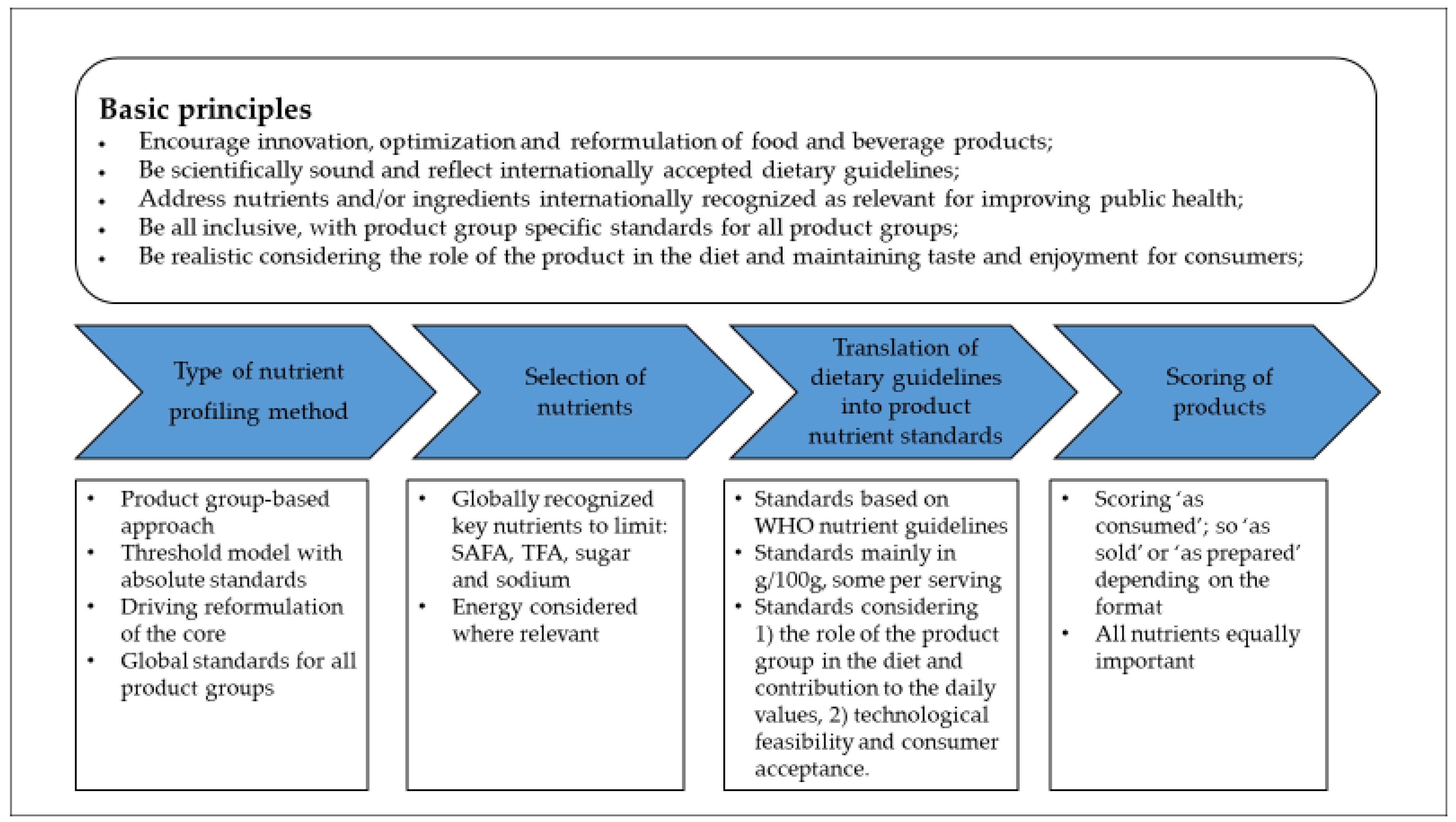
2.1. Standards Development Approach
2.1.1. Basic Principles
2.1.2. Type of Nutrient Profiling Method
2.1.3. Selection of Nutrients
2.1.4. Translation of Dietary Guidelines into Product Nutrient Standards
Energy
Sodium
SAFA
Sugars
Trans Fat
2.1.5. Scoring of Products
2.2. Modelling
2.2.1. Food Consumption and Composition Data
2.2.2. Food Group Alignment
2.2.3. Modelling Scenario’s
- Baseline: Population nutrient intake based on the original survey data
- Reformulation: Population nutrient intake following ‘hypothetical reformulation’ to meet the product group specific nutrient standards defined
2.2.4. Conversion Standards in g/serving to g/100 g
- The standard value for Energy is expressed per serving of each food product.
- The standard for Saturated Fat in the food groups, Emulsion-based Sauces, and Mustards, is expressed as % of total fat.
- The nutrient standards for the food groups Ice cream and Desserts, and Sweet and Savoury Snacks, are per serving.
2.2.5. Data Analysis
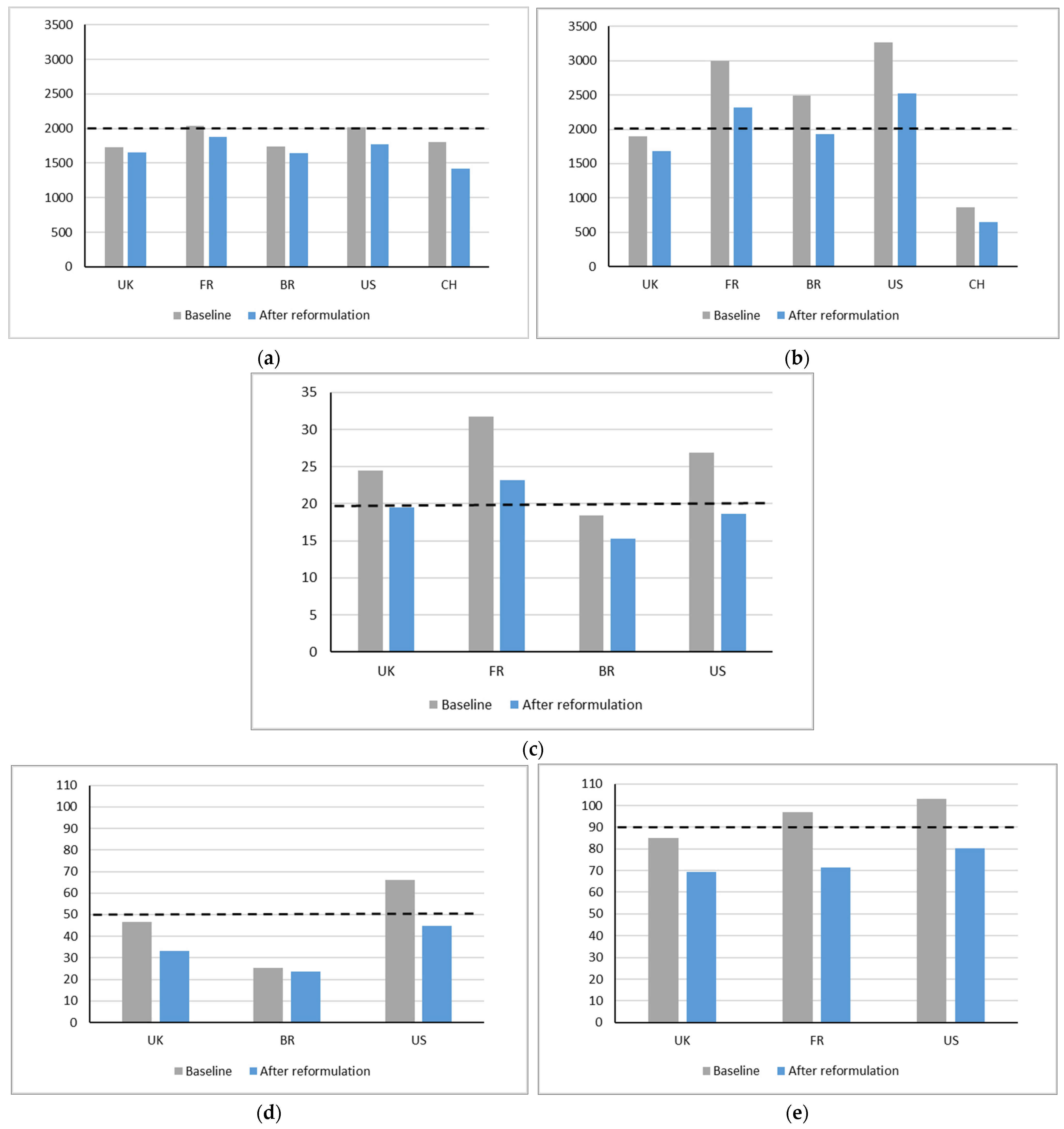
3. Results
3.1. Energy
3.2. Sodium
3.3. SAFA
3.4. Added Sugars
3.5. Total Sugars
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Micha, R.; Shulkin, M.L.; Peñalvo, J.L.; Khatibzadeh, S.; Singh, G.M.; Rao, M.; Fahimi, S.; Powles, J.; Mozaffarian, D. Etiologic Effects and Optimal Intakes of Foods and Nutrients for Risk of Cardiovascular Diseases and Diabetes: Systematic Reviews and Meta-Analyses from the Nutrition and Chronic Diseases Expert Group (Nutricode). PLoS ONE 2017, 12, e0175149. [Google Scholar] [CrossRef]
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Murray, C.J. Health Effects of Dietary Risks in 195 Countries, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef]
- FAO/WHO (Ed.) Diet, Nutrition and the Prevention of Chronic Diseases: Report of a Joint Fao/Who Expert Consultation; WHO: Geneva, Switzerland, 2004. [Google Scholar]
- Global Action Plan for the Prevention and Control of Ncds 2013–2020; WHO: Geneva, Switzerland, 2013.
- Nijman, C.A.J.; Zijp, I.M.; Sierksma, A.; Roodenburg, A.J.C.; Leenen, R.; Van den Kerkhoff, C.; Weststrate, J.A.; Meijer, G.W. A Method to Improve the Nutritional Quality of Foods and Beverages Based on Dietary Recommendations. Eur. J. Clin. Nutr. 2007, 61, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Dotsch-Klerk, M.; Goossens, W.P.M.M.; Meijer, G.W.; van het Hof, K.H. Reducing Salt in Food; Setting Product-Specific Criteria Aiming at a Salt Intake of 5 g Per Day. Eur. J. Clin. Nutr. 2015, 69, 799–804. [Google Scholar] [CrossRef]
- Guideline: Sodium Intake for Adults and Children; WHO: Geneva, Switzerland, 2012.
- Political Declaration of the High-Level Meeting of the General Assembly on the Prevention and Control of Non-Communicable Diseases; UN: New York, NY, USA, 2011.
- Human Energy Requirements. Report of a Joint FAO/WHO/UNU Expert Consultation, Rome, Italy, 17–24 October 2001. In FAO Food and Nutrition Technical Report Series 1; FAO/WHO/UNU: Rome, Italy, 2004. [Google Scholar]
- Guideline: Sugars Intake for Adults and Children; WHO: Geneva, Switzerland, 2015.
- European Parliament, Council of the European Union. Regulation (Eu) No 1169/2011 of the European Parliament and of the Council of 25 October 2011 on the Provision of Food Information to Consumers, Amending Regulations (Ec) No 1924/2006 and (Ec) No 1925/2006 of the European Parliament and of the Council, and Repealing Commission Directive 87/250/Eec, Council Directive 90/496/Eec, Commission Directive 1999/10/Ec, Directive 2000/13/Ec of the European Parliament and of the Council, Commission Directives 2002/67/Ec and 2008/5/Ec and Commission Regulation (Ec) No 608/2004 Text with Eea Relevance. Off. J. Eur. Union L 2011, 304, 18–63. [Google Scholar]
- Popkin, B.M.; Armstrong, L.E.; Bray, G.M.; Caballero, B.; Frei, B.; Willett, W.C. A New Proposed Guidance System for Beverage Consumption in the United States. Am. J. Clin. Nutr. 2006, 83, 529–542. [Google Scholar] [CrossRef] [PubMed]
- Alliance, international Food & Beverage. Reducing Saturated Fats & Eliminating Trans Fats. Available online: https://ifballiance.org/commitments/product-formulation/reducing-saturated-fats-eliminating-trans-fats/ (accessed on 6 September 2022).
- French Republic. Consumption Data and Eating Habits from the Inca3 Study. French Republic. Available online: https://www.data.gouv.fr/fr/datasets/donnees-de-consommations-et-habitudes-alimentaires-de-letude-inca-3/#description (accessed on 6 September 2022).
- Survey of 2017–2018 Family Budgets: Nutritional Assessment Household Availability of Food in Brazil. Rio de Janeiro: 56 P IBGE: Rio de Janeiro. Brazil. 2020. Available online: https://biblioteca.ibge.gov.br/index.php/biblioteca-catalogo?view=detalhes&id=2101742 (accessed on 6 September 2022).
- National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Data 2017–2018. Department of Health and Human Services, Centers for Disease Control and Prevention. Available online: https://wwwn.cdc.gov/nchs/nhanes/ContinuousNhanes/Default.aspx?BeginYear=2017 (accessed on 6 September 2022).
- Popkin, B.M.; Du, S.; Zhai, F.; Zhang, B. Cohort Profile: The China Health and Nutrition Survey—Monitoring and Understanding Socio-Economic and Health Change in China, 1989–2011. Int. J. Epidemiol. 2010, 39, 1435–1440. [Google Scholar] [CrossRef] [PubMed]
- Lai, H.T.; Hutchinson, J.; Evans, C.E.L. Non-Milk Extrinsic Sugars Intake and Food and Nutrient Consumption Patterns among Adolescents in the Uk National Diet and Nutrition Survey, Years 2008–2016. Nutrients 2019, 11, 1621. [Google Scholar] [CrossRef] [PubMed]
- British Nutrition Foundation. Your Balanced Diet—Get Portion Wise. British Nutrition Foundation. Available online: https://www.nutrition.org.uk/putting-it-into-practice/balancing-the-diet/get-portion-wise/ (accessed on 6 September 2022).
- Brazilian Table of Food Composition (Tbca). Version 7.1. University of São Paulo (USP) and Food Research Center (FoRC): São Paulo, Brazil 2020. Available online: http://www.fcf.usp.br/tbca (accessed on 6 September 2022).
- Van Kappel, A.; Amoyel, J.; Slimani, N.; Vozar, B.; Riboli, E. Epic-Soft Picture Book for Estimating Food Portion Sizes; IARC: Lyon, France, 1995. [Google Scholar]
- Code of Federal Regulations. Title 21 Food and Drugs, Part 101 Food Labeling, Section §101.12. Reference Amounts Customarily Consumed Per Eating Occasion. Code of Federal Regulations. Available online: https://www.ecfr.gov/current/title-21/chapter-I/subchapter-B/part-101/subpart-A/section-101.12 (accessed on 6 September 2022).
- China Notifies Draft National Food Safety Standard—General Rules for Nutritional Labeling of Prepacked Foods. United States Department of Agriculture (USDA), Foreign Agricultural Service (FAS): Beijng, China. 2021. Available online: https://www.fas.usda.gov/data/china-china-notifies-revised-draft-national-food-safety-standard-general-rules-nutritional (accessed on 6 September 2022).
- Carrefour. Magasins Et Courses En Ligne (Drive, Livraison À Domicile). Available online: https://www.carrefour.fr/ (accessed on 6 September 2022).
- Supermarché Alimentaire—Supermarchés Match. Available online: https://www.supermarchesmatch.fr/ (accessed on 6 September 2022).
- Dadiet—The Dietary Intake Evaluation Tool. Dazult Limited: Maynooth, Ireland. Available online: https://dadiet.daanalysis.com (accessed on 6 September 2022).
- Global Index 2021. Access to Nutrition Initiative: Utrecht, The Netherlands. 2021. Available online: https://accesstonutrition.org/index/global-index-2021/ (accessed on 6 September 2022).
- Food and Agricultural Benchmark. World Benchmarking Alliance: Amsterdam, The Netherlands. 2021. Available online: https://www.worldbenchmarkingalliance.org/publication/food-agriculture/rankings/ (accessed on 6 September 2022).
- Bingham, S.A. Limitations of the Various Methods for Collecting Dietary Intake Data. Ann. Nutr. Metab. 1991, 35, 117–127. [Google Scholar] [CrossRef]
- Le, T.H.; Disegna, M.; Lloyd, T. National Food Consumption Patterns: Converging Trends and the Implications for Health. EuroChoices 2022. [Google Scholar] [CrossRef]
- Zhang, J.G.; Wang, H.J.; Du, W.W.; Hunag, F.F.; Wang, Z.H.; Zhang, B. Dietary Sodium Intake of Adult Residents in 15 Provinces of China. Food Nutr. China 2022, 28, 75–77. [Google Scholar]
- Ma, H.; Xue, Q.; Wang, X.; Li, X.; Franco, O.H.; Li, Y.; Heianza, H.; Manson, J.E.; Qi, L. Adding Salt to Foods and Hazard of Premature Mortality. Eur. Heart J. 2022, 30, 2878–2888. [Google Scholar] [CrossRef] [PubMed]
- Newson, R.S.; Lion, R.; Crawford, R.J.; Curtis, V.; Elmadfa, I.; Feunekes, G.I.; Hicks, C.; Liere, M.; van Lowe, C.F.; Meijer, G.W.; et al. Behaviour Change for Better Health: Nutrition, Hygiene and Sustainability. BMC Public Health 2013, 13 (Suppl. 1), S1. [Google Scholar] [CrossRef] [PubMed]
- Hyseni, L.; Elliot-Green, A.; Lloyd-Williams, F.; Kypridemos, C.; O’Flaherty, M.; McGill, R.; Orton, L.; Bromley, H.; Cappuccio, F.P.; Capewell, S. Systematic Review of Dietary Salt Reduction Policies: Evidence for an Effectiveness Hierarchy? PLoS ONE 2017, 12, e0177535. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Brinsden, H.C.; MacGregor, G.A. Salt Reduction in the United Kingdom: A Successful Experiment in Public Health. J. Hum. Hypertens. 2014, 28, 345–352. [Google Scholar] [CrossRef]
- Calorie Reduction: The Scope and Ambition for Action; Public Health England (PHE): London, UK, 2018. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/800675/Calories_Evidence_Document.pdf (accessed on 6 September 2022).
- Trieu, K.D.H.; Coyle, D.H.; Afshin, A.; Neal, B.; Marklund, M.; Wu, J.H.Y. The Estimated Health Impact of Sodium Reduction through Food Reformulation in Australia: A Modeling Study. PLoS Med. 2021, 18, e1003806. [Google Scholar] [CrossRef]
- Hooper, L.; Martin, N.; Oluseyi, F.; Jimoh, O.F.; Kirk, C.; Foster, E.; Asmaa, S.; Abdelhamid, S.A. Reduction in Saturated Fat Intake for Cardiovascular Disease. Cochrane Database Syst. Rev. 2015, 6, CD011737. [Google Scholar] [CrossRef] [PubMed]
- Hashem, K.M.; He, F.J.; MacGregor, G.A. Effects of Product Reformulation on Sugar Intake and Health-a Systematic Review and Meta-Analysis. Nutr. Rev. 2019, 77, 181–196. [Google Scholar] [CrossRef] [PubMed]
- Federici, C.; Detzel, P.; Petracca, F.; Dainelli, L.; Fattore, G. The Impact of Food Reformulation on Nutrient Intakes and Health, a Systematic Review of Modelling Studies. BMC Nutr. 2019, 5, 2. [Google Scholar] [CrossRef] [PubMed]
- 10 Years of USLP Unilever. 2021. Available online: https://www.unilever.com/files/92ui5egz/production/4653a3a9cfc705af80ca30583938ca0e4112a919.pdf (accessed on 6 September 2022).
- Reducing Salt, Sugar and Calories Unilever. 2022. Available online: https://www.unilever.com/planet-and-society/positive-nutrition/reducing-salt-sugar-and-calories/ (accessed on 6 September 2022).
- Positive Nutrition—Strategy and Goals Unilever. 2022. Available online: https://www.unilever.com/planet-and-society/positive-nutrition/strategy-and-goals/ (accessed on 6 September 2022).
- Positive Nutrition and Fortfication Unilever. 2022. Available online: https://www.unilever.com/planet-and-society/positive-nutrition/positive-nutrition-and-fortification/ (accessed on 6 September 2022).
- Neufingerl, N.; Eilander, A. Nutrient Intake and Status in Adults Consuming Plant-Based Diets Compared to Meat-Eaters: A Systematic Review. Nutrients 2022, 14, 29. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Nutrient | Daily Value |
|---|---|
| Energy | 2000 kcal/day |
| Sodium | 2000 mg/day (5 g salt/day) |
| SAFA | 10 en% * = 20 g/day |
| Free sugars | 10 en% * = 50 g/day |
| Country | UK | France | Brazil | US | China |
|---|---|---|---|---|---|
| Survey name | UK National Diet and Nutrition Survey (NDNS) | French dietary survey on the general population (INCA3) | Inquérito Nacional de Alimentação (INA) | National Health and Nutrition Examination Survey (NHANES) | China Health and Nutrition Survey (CHNS) |
| Survey period | 2016/2017 and 2018/2019 | 2015 | 2017–2018 | 2017–2018 | 2004–2011 |
| Age range | ≥2 years | 2–79 years | ≥10 years | ≥2 years | ≥2 years |
| Number of participants | 4490 | 3946 | 46,164 | 6177 | 49,464 |
| Dietary assessment method | 4× Estimated diet diary | 3 × Non-consecutive 24-h records (2–14 years) or 24-h recalls (15–79 years) | 2 × 24-h recall | 2 × 24-h recall | 3× Weighted/measured diet diary |
| Food composition table used | Composition of foods integrated dataset (CoFID) | ANSES- CIQUAL table | Brazilian Table of Food Composition (TBCA) | Food and Nutrient Database for Dietary Studies (FNDDS) | 2004 China Food Composition Tables (CFCT) |
| Nutrient data available | Energy, sodium, SAFA, added (NMES) and total sugars | Energy, sodium, SAFA and total sugars | Energy, sodium, SAFA and added sugars | Energy, sodium, SAFA, added and total sugars | Energy and sodium |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dötsch-Klerk, M.; Kovacs, E.M.R.; Hegde, U.; Eilander, A.; Willems, J.I. Improving the Nutrient Quality of Foods and Beverages Using Product Specific Standards for Nutrients to Limit Will Substantially Reduce Mean Population Intakes of Energy, Sodium, Saturated Fat and Sugars towards WHO Guidelines. Nutrients 2022, 14, 4289. https://doi.org/10.3390/nu14204289
Dötsch-Klerk M, Kovacs EMR, Hegde U, Eilander A, Willems JI. Improving the Nutrient Quality of Foods and Beverages Using Product Specific Standards for Nutrients to Limit Will Substantially Reduce Mean Population Intakes of Energy, Sodium, Saturated Fat and Sugars towards WHO Guidelines. Nutrients. 2022; 14(20):4289. https://doi.org/10.3390/nu14204289
Chicago/Turabian StyleDötsch-Klerk, Mariska, Eva M. R. Kovacs, Ujwal Hegde, Ans Eilander, and Julie I. Willems. 2022. "Improving the Nutrient Quality of Foods and Beverages Using Product Specific Standards for Nutrients to Limit Will Substantially Reduce Mean Population Intakes of Energy, Sodium, Saturated Fat and Sugars towards WHO Guidelines" Nutrients 14, no. 20: 4289. https://doi.org/10.3390/nu14204289
APA StyleDötsch-Klerk, M., Kovacs, E. M. R., Hegde, U., Eilander, A., & Willems, J. I. (2022). Improving the Nutrient Quality of Foods and Beverages Using Product Specific Standards for Nutrients to Limit Will Substantially Reduce Mean Population Intakes of Energy, Sodium, Saturated Fat and Sugars towards WHO Guidelines. Nutrients, 14(20), 4289. https://doi.org/10.3390/nu14204289