
Impact of Fruit and Vegetable Protein vs. Milk Protein on Metabolic Control of Children with Phenylketonuria: A Randomized Crossover Controlled Trial
 ,
,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
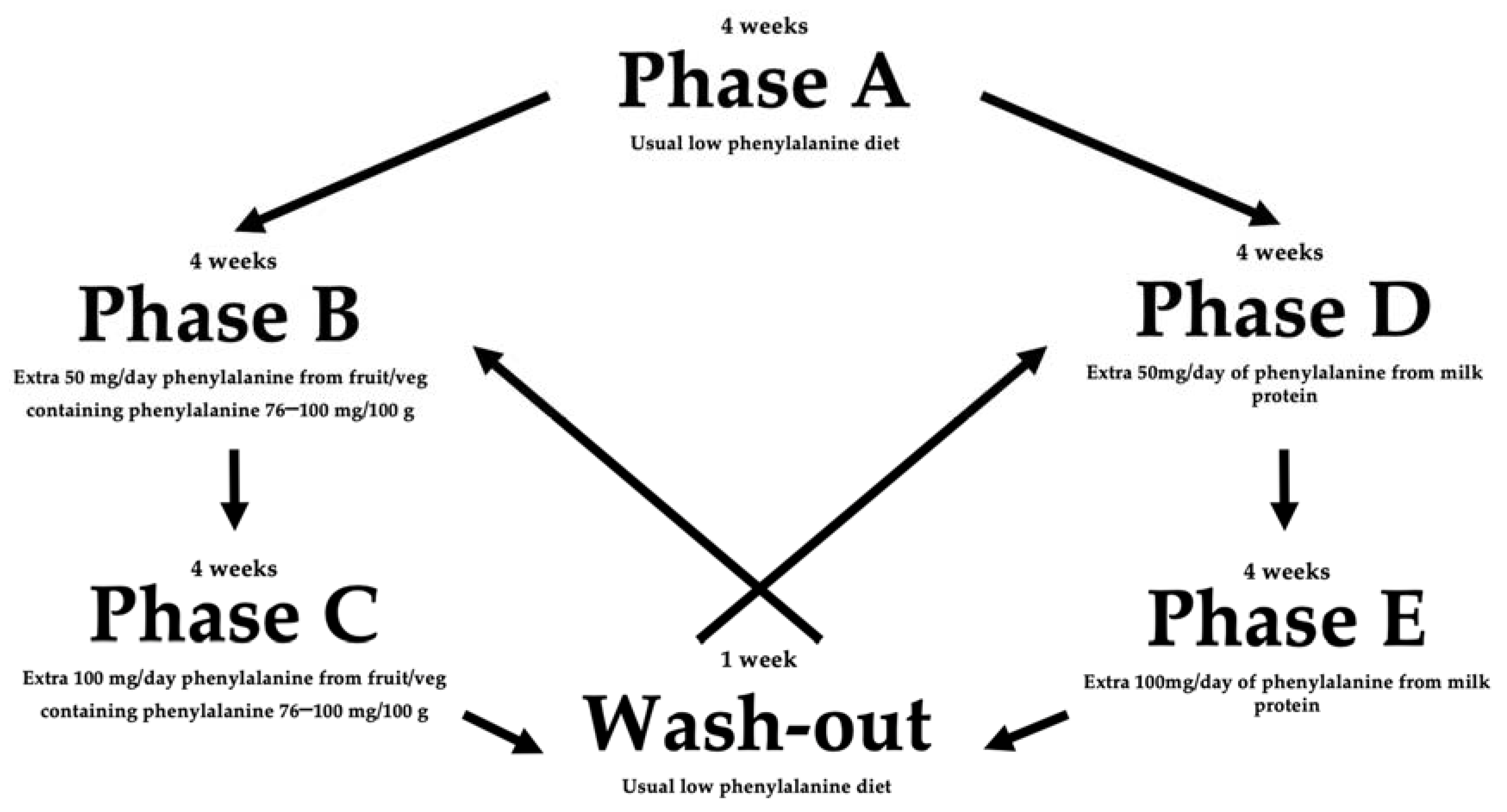
2.2. Study Design
- -
- Phase A: no change to dietary intake.
- -
- Phase B and C: usual diet with an additional 50 mg and 100 mg/day of phenylalanine from fruits and vegetables containing phenylalanine 76–100 mg/100 g, respectively.
- -
- Phase D and E: usual diet with an additional 50 mg and 100 mg/day of phenylalanine from milk protein sources, respectively.
2.3. Data Collection
2.4. Statistical Analysis
2.5. Ethical Aspects
3. Results
3.1. Participants
3.2. Intervention
3.3. Tolerance of Additional Phenylalanine Intake
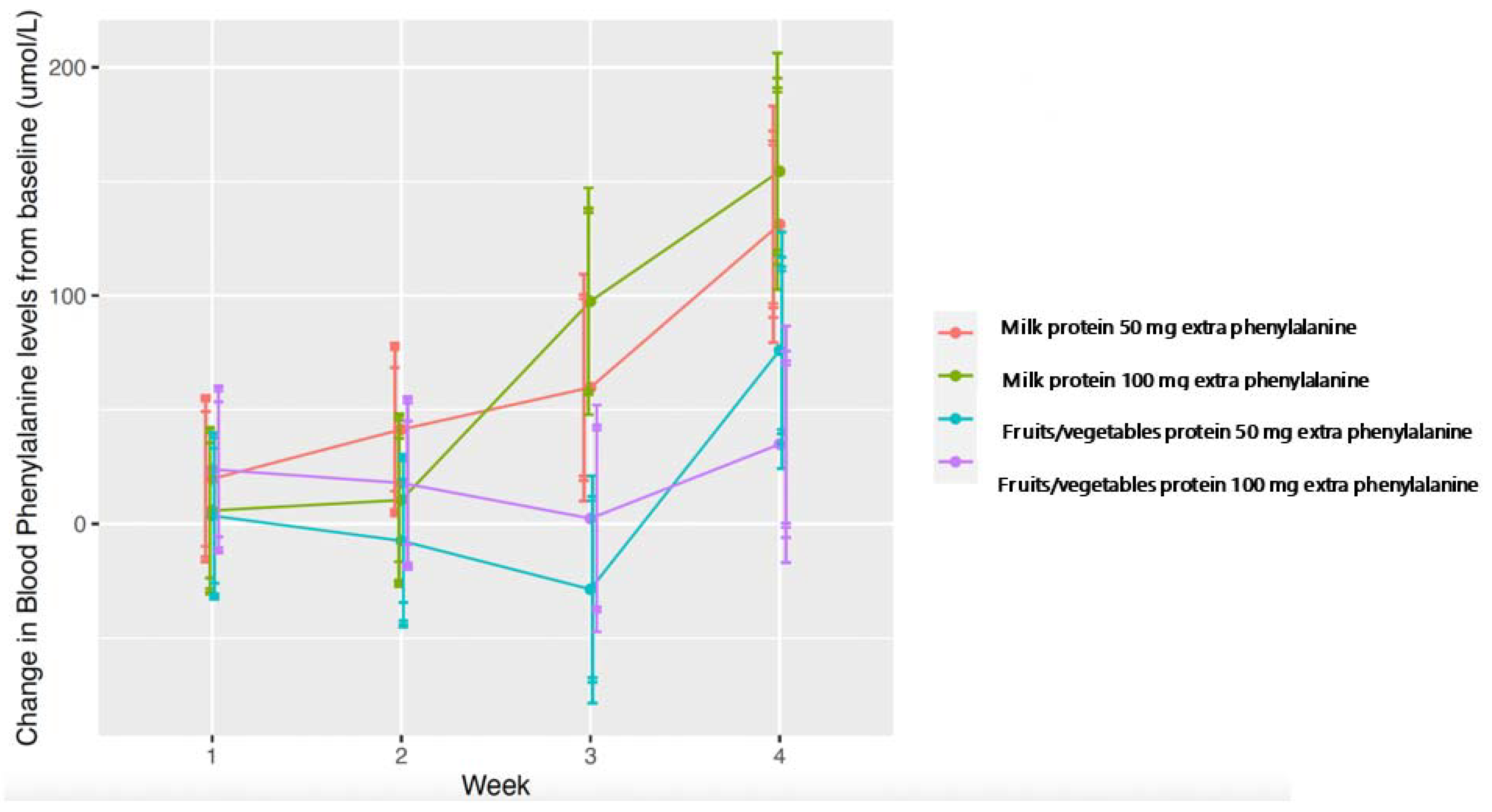
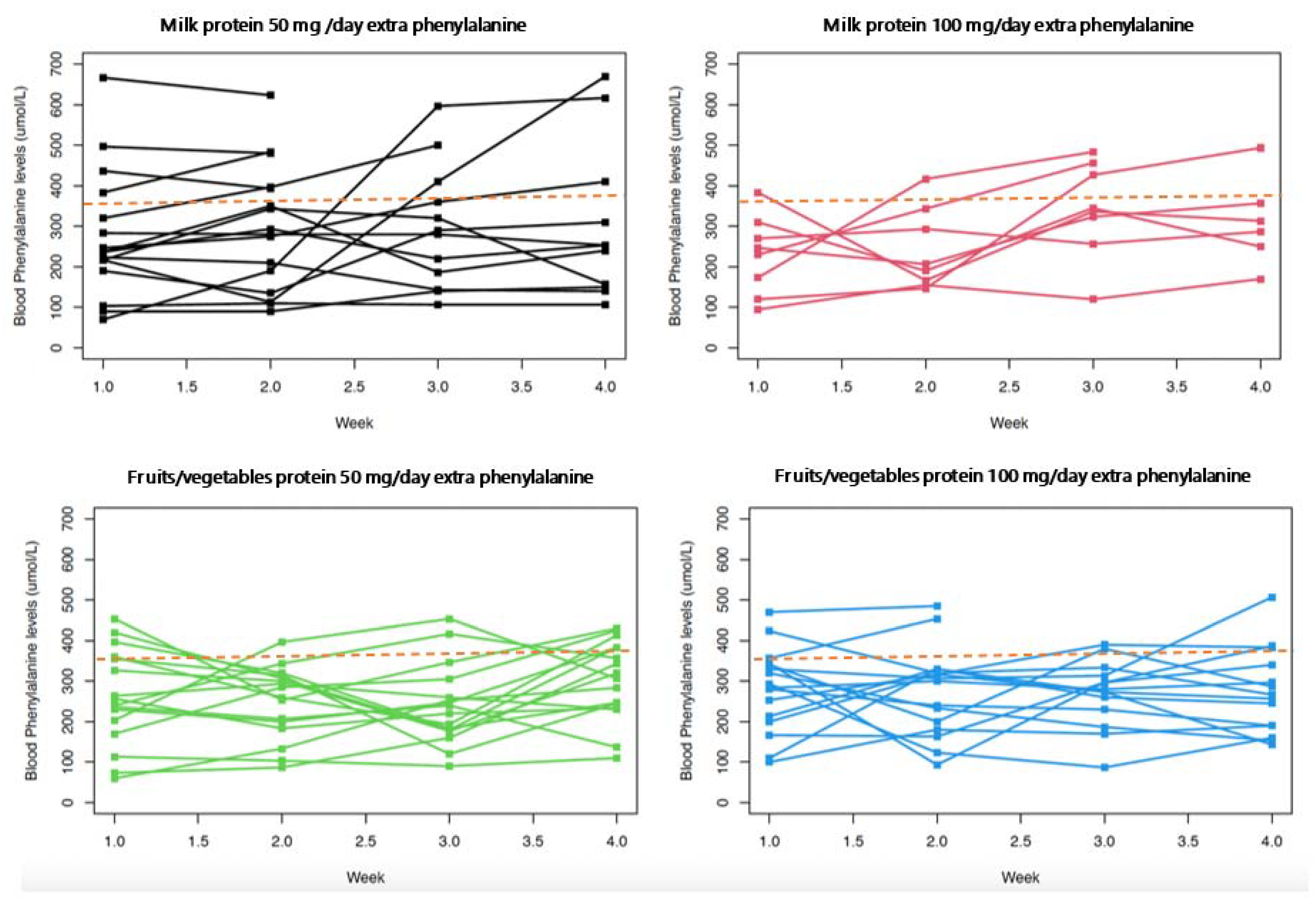
3.4. Impact on Blood Phenylalanine Control and Differences between Milk Protein vs. Fruit/Vegetable Protein
3.5. Impact on Phenylalanine Intake
3.6. Nutritional Intake
3.7. Anthropometry
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blau, N.; van Spronsen, F.J.; Levy, H.L. Phenylketonuria. Lancet 2010, 376, 1417–1427. [Google Scholar] [CrossRef]
- MacDonald, A.; van Wegberg, A.M.J.; Ahring, K.; Beblo, S.; Bélanger-Quintana, A.; Burlina, A.; Campistol, J.; Coşkun, T.; Feillet, F.; Giżewska, M.; et al. PKU dietary handbook to accompany PKU guidelines. Orphanet. J. Rare Dis. 2020, 15, 171. [Google Scholar] [CrossRef]
- Kim, J.; Boutin, M. A List of Phenylalanine to Protein Ratios for Common Foods; ECE Technical Reports, Paper 456; Purdue University: West Lafayette, IN, USA, 2014. [Google Scholar]
- Francis, D.E.; Dixon, D.J. Diets for Sick Children; Blackwell Science Ltd.: Hoboken, NJ, USA, 1969. [Google Scholar]
- Mac Donald, A.; Rylance, G.; Davies, P.; Asplin, D.; Hall, S.K.; Booth, I.W. Free use of fruits and vegetables in phenylketonuria. J. Inherit. Metab. Dis. 2003, 26, 327–338. [Google Scholar] [CrossRef]
- Rohde, C.; Mütze, U.; Schulz, S.; Thiele, A.G.; Ceglarek, U.; Thiery, J.; Mueller, A.S.; Kiess, W.; Beblo, S. Unrestricted fruits and vegetables in the PKU diet: A 1-year follow-up. Eur. J. Clin. Nutr. 2014, 68, 401–403. [Google Scholar] [CrossRef]
- Rohde, C.; Mütze, U.; Weigel, J.F.; Ceglarek, U.; Thiery, J.; Kiess, W.; Beblo, S. Unrestricted consumption of fruits and vegetables in phenylketonuria: No major impact on metabolic control. Eur. J. Clin. Nutr. 2012, 66, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.; Jacobs, P.; Fingerhut, R.; Torresani, T.; Thöny, B.; Blau, N.; Baumgartner, M.R.; Rohrbach, M. Positive effect of a simplified diet on blood phenylalanine control in different phenylketonuria variants, characterized by newborn BH4 loading test and PAH analysis. Mol. Genet. Metab. 2012, 106, 264–268. [Google Scholar] [CrossRef]
- van Wegberg, A.M.J.; MacDonald, A.; Ahring, K.; Bélanger-Quintana, A.; Blau, N.; Bosch, A.M.; Burlina, A.; Campistol, J.; Feillet, F.; Giżewska, M.; et al. The complete European guidelines on phenylketonuria: Diagnosis and treatment. Orphanet. J. Rare Dis. 2017, 12, 162. [Google Scholar] [CrossRef] [PubMed]
- Berrazaga, I.; Micard, V.; Gueugneau, M.; Walrand, S. The Role of the Anabolic Properties of Plant- versus Animal-Based Protein Sources in Supporting Muscle Mass Maintenance: A Critical Review. Nutrients 2019, 11, 1825. [Google Scholar] [CrossRef]
- Dangin, M.; Boirie, Y.; Guillet, C.; Beaufrère, B. Influence of the protein digestion rate on protein turnover in young and elderly subjects. J. Nutr. 2002, 132, 3228s–3233s. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.R.; Falvo, M.J. Protein—Which is Best? J. Sports Sci. Med. 2004, 3, 118–130. [Google Scholar]
- Protein Quality Evaluation; FAO Food Nutrition Paper; FAO/WHO: Geneve, Switzerland, 1991; Volume 51, 66p.
- Suárez López, M.M.; Kizlansky, A.; López, L.B. Assessment of protein quality in foods by calculating the amino acids score corrected by digestibility. Nutr. Hosp. 2006, 21, 47–51. [Google Scholar] [PubMed]
- Herreman, L.; Nommensen, P.; Pennings, B.; Laus, M.C. Comprehensive overview of the quality of plant- And animal-sourced proteins based on the digestible indispensable amino acid score. Food Sci. Nutr. 2020, 8, 5379–5391. [Google Scholar] [CrossRef] [PubMed]
- Phillips, S.M. The impact of protein quality on the promotion of resistance exercise-induced changes in muscle mass. Nutr. Metab. 2016, 13, 64. [Google Scholar] [CrossRef] [PubMed]
- Dixon, M.; MacDonald, A.; White, F.J. Disorders of Amino Acid Metabolism, Organic Acidaemias and Urea Cycle Disorders. In Clinical Paediatric Dietetics; Wiley: Hoboken, NJ, USA, 2020; pp. 513–598. [Google Scholar] [CrossRef]
- Rodrigues, C.; Pinto, A.; Faria, A.; Teixeira, D.; van Wegberg, A.M.J.; Ahring, K.; Feillet, F.; Calhau, C.; MacDonald, A.; Moreira-Rosário, A.; et al. Is the Phenylalanine-Restricted Diet a Risk Factor for Overweight or Obesity in Patients with Phenylketonuria (PKU)? A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 3443. [Google Scholar] [CrossRef] [PubMed]
- Daly, A.; Evans, S.; Pinto, A.; Ashmore, C.; Rocha, J.C.; MacDonald, A. A 3 Year Longitudinal Prospective Review Examining the Dietary Profile and Contribution Made by Special Low Protein Foods to Energy and Macronutrient Intake in Children with Phenylketonuria. Nutrients 2020, 12, 3153. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J.L.; Lloyd, B. Health benefits of fruits and vegetables. Adv. Nutr. 2012, 3, 506–516. [Google Scholar] [CrossRef] [PubMed]
- Dupont, D.; Tome, D. Milk proteins: Digestion and absorption in the gastrointestinal tract. In Milk Proteins; Elsevier: Amsterdam, The Netherlands, 2014; pp. 557–569. [Google Scholar]
- Auestad, N.; Layman, D.K. Dairy bioactive proteins and peptides: A narrative review. Nutr. Rev. 2021, 79, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Deglaire, A.; Fromentin, C.; Fouillet, H.; Airinei, G.; Gaudichon, C.; Boutry, C.; Benamouzig, R.; Moughan, P.J.; Tomé, D.; Bos, C. Hydrolyzed dietary casein as compared with the intact protein reduces postprandial peripheral, but not whole-body, uptake of nitrogen in humans. Am. J. Clin. Nutr. 2009, 90, 1011–1022. [Google Scholar] [CrossRef]
- Gorissen, S.H.M.; Crombag, J.J.R.; Senden, J.M.G.; Waterval, W.A.H.; Bierau, J.; Verdijk, L.B.; van Loon, L.J.C. Protein content and amino acid composition of commercially available plant-based protein isolates. Amino Acids 2018, 50, 1685–1695. [Google Scholar] [CrossRef]
- Horner, K.; Drummond, E.; Brennan, L. Bioavailability of milk protein-derived bioactive peptides: A glycaemic management perspective. Nutr. Res. Rev. 2016, 29, 91–101. [Google Scholar] [CrossRef]
- Carbonaro, M.; Maselli, P.; Nucara, A. Relationship between digestibility and secondary structure of raw and thermally treated legume proteins: A Fourier transform infrared (FT-IR) spectroscopic study. Amino Acids 2012, 43, 911–921. [Google Scholar] [CrossRef] [PubMed]
- Gilani, G.S.; Cockell, K.A.; Sepehr, E. Effects of antinutritional factors on protein digestibility and amino acid availability in foods. J. AOAC Int. 2005, 88, 967–987. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.P.; Bhandari, B.; Cichero, J.; Prakash, S. Gastrointestinal digestion of dairy and soy proteins in infant formulas: An in vitro study. Food Res. Int. 2015, 76, 348–358. [Google Scholar] [CrossRef]
- Barbé, F.; Ménard, O.; Le Gouar, Y.; Buffière, C.; Famelart, M.-H.; Laroche, B.; Le Feunteun, S.; Dupont, D.; Rémond, D. The heat treatment and the gelation are strong determinants of the kinetics of milk proteins digestion and of the peripheral availability of amino acids. Food Chem. 2013, 136, 1203–1212. [Google Scholar] [CrossRef]
- Ye, A.; Cui, J.; Dalgleish, D.; Singh, H. Effect of homogenization and heat treatment on the behavior of protein and fat globules during gastric digestion of milk. J. Dairy Sci. 2017, 100, 36–47. [Google Scholar] [CrossRef]
- Pinto, A.; Almeida, M.F.; MacDonald, A.; Ramos, P.C.; Rocha, S.; Guimas, A.; Ribeiro, R.; Martins, E.; Bandeira, A.; Jackson, R.; et al. Over Restriction of Dietary Protein Allowance: The Importance of Ongoing Reassessment of Natural Protein Tolerance in Phenylketonuria. Nutrients 2019, 11, 995. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Food | Phenylalanine Content mg/100 g * | Portion Size Weight for 1 Phenylalanine Exchange (50 mg) |
|---|---|---|
| Beansprouts | 92 mg | 60 g |
| Broccoli | 76 mg | 60 g |
| Cauliflower | 89 mg | 60 g |
| Yam | 97 mg | 60 g |
| Sugar snap peas | 75–88 mg | 60 g |
| Mange tout | 66–93 mg | 60 g |
| Bamboo Shoots | 83 mg | 60 g |
| Brussel sprouts | 83 mg | 60 g |
| Figs | 83 mg | 60 g |
| Milk | 180 mg | 30 mL |
| Yoghurt | Phenylalanine content calculated from protein content (g/100 g) of yoghurt on packaging. Assumed 1 g protein = 50 mg phenylalanine | |
| Milk based ice cream | Phenylalanine content calculated from protein content (g/100 g) of ice cream on packaging. Estimated that the weight of ice cream that provided 1 g protein = 50 mg phenylalanine | |
| Subject Number | Age (Years) | Sex | Phenotype | Randomization (Starting Intervention) | Prescribed Daily Number of 1 g Protein/50 mg Phenylalanine Exchanges | Protein Equivalent Amount (g/day) from Protein Substitute | Protein Substitute Brand, Size and Manufacturer |
|---|---|---|---|---|---|---|---|
| 1 | 9 | Female | Classical PKU | Fruit/vegetables | 4 | 65 | PKU Air 15® Vit |
| (45 g PE) | |||||||
| PKU Air 20® Vit | |||||||
| (20 g PE) | |||||||
| 2 | 7 | Male | Classical PKU | Milk products | 6.5 | 60 | PKU Express 15® Vit |
| (45 g PE) | |||||||
| PKU Air 15® Vit | |||||||
| (15 g PE) | |||||||
| 3 | 12 | Male | Mild PKU | Fruit/vegetables | 25 | 60 | PKU Sphere 20® Vit |
| (60 g PE) | |||||||
| 4 | 12 | Female | Mild PKU | Fruit/vegetables | 14 | 60 | PKU Sphere 20® Vit |
| (60 g PE) | |||||||
| 5 | 9 | Female | Classical PKU | Milk products | 6 | 60 | PKU Sphere 20® Vit |
| (60 g PE) | |||||||
| 6 | 12 | Male | Classical PKU | Milk products | 7.5 | 80 | PKU Sphere 20® Vit |
| (60 g PE) | |||||||
| PKU Cooler 20® Vit | |||||||
| (20 g PE) | |||||||
| 7 | 12 | Female | Classical PKU | Milk products | 4.5 | 80 | PKU Sphere 20® Vit |
| (80 g PE) | |||||||
| 8 | 8 | Male | Classical PKU | Fruit/vegetables | 3 | 80 | PKU Sphere 20® Vit |
| (60 g PE) | |||||||
| PKU Cooler 20® Vit | |||||||
| (20 g PE) | |||||||
| 9 | 6 | Female | Classical PKU | Milk products | 5.5 | 60 | PKU Cooler 15® Vit |
| (60 g PE) | |||||||
| 10 | 11 | Female | Classical PKU | Fruit/vegetables | 4 | 60 | PKU Air 20® Vit |
| (40 g PE) | |||||||
| PKU Sphere 20® Vit | |||||||
| (20 g PE) | |||||||
| 11 | 11 | Female | Classical PKU | Milk products | 6 | 60 | PKU Lophlex LQ 10® Nu |
| (60 g PE) | |||||||
| 12 | 11 | Female | Classical PKU | Fruit/vegetables | 5 | 60 | PKU Air 20® Vit |
| (40 g PE) | |||||||
| PKU Sphere 20® Vit | |||||||
| (20 g PE) | |||||||
| 13 | 10 | Female | Classical PKU | Milk products | 5.5 | 60 | PKU Lophlex LQ 20® Nu |
| (60 g PE) | |||||||
| 14 | 12 | Female | Classical PKU | Fruit/vegetables | 6 | 70 | PKU Cooler 20® Vit |
| (60 g PE) | |||||||
| PKU Cooler 10® Vit | |||||||
| (10 g PE) | |||||||
| 15 | 8 | Male | Classical PKU | Milk products | 4 | 60 | PKU Air 20® Vit |
| (40 g PE) | |||||||
| PKU Sphere 20® Vit | |||||||
| (20 g PE) | |||||||
| 16 | 9 | Female | Classical PKU | Fruit/vegetables | 6 | 60 | PKU Air 20® Vit |
| (60 g PE) |
| Dietary Intervention | ||||
|---|---|---|---|---|
| Phase B: An Additional 50 mg/day Phenylalanine from Fruits and Vegetables (Phenylalanine Containing 76–100 mg /100 g) | Phase C: An Additional 100 mg/day Phenylalanine from Fruits and Vegetables (Phenylalanine containing 76–100 mg /100 g) | Phase D: An Additional 50 mg/day Phenylalanine from Milk Protein | Phase E: An Additional 100 mg/day Phenylalanine from Milk Protein | |
| % subjects that maintained blood phenylalanine control * within target range over 4 weeks | 100% (n = 16/16) | 69% (n = 11/16) | 50% (n = 8/16) | 31% (n = 5/16) |
| Number of Weeks Need for Blood Phenylalanine Levels Above Target Range | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Subject 1 | Subject 2 | Subject 3 | Subject 4 | Subject 5 | Subject 6 | Subject 7 | Subject 8 | Subject 9 | Subject 10 | Subject 11 | Subject 12 | Subject 13 | Subject 14 | Subject 15 | Subject 16 | |
| Milk protein intervention | 8 weeks | N/A | N/A | 2 weeks | 4 weeks | 3 weeks | 2 weeks | 2 weeks | 2 weeks | 4 weeks | N/A | 4 weeks | N/A | 6 weeks | N/A | 7 weeks |
| Fruits and vegetables protein intervention | N/A | 6 weeks | N/A | 8 weeks | N/A | N/A | N/A | N/A | 8 weeks | N/A | N/A | N/A | N/A | N/A | 6 weeks | 8 weeks |
| Change in Blood Phenylalanine from Baseline by Week and Study Intervention | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 50 mg/day Phenylalanine from Fruit and Vegetable Protein | 100 mg/day Phenylalanine from Fruit and Vegetable Protein | 50 mg/day Phenylalanine from Milk Protein | 100 mg/day Phenylalanine from Milk Protein | |||||||||||||
| Week 1 | Week 2 | Week 3 | Week 4 | Week 1 | Week 2 | Week 3 | Week 4 | Week 1 | Week 2 | Week 3 | Week 4 | Week 1 | Week 2 | Week 3 | Week 4 | |
| Mean change of blood phenylalanine from baseline (µmol/L) | 4 | −7 | −29 | 76 | 24 | 18 | 2 | 35 | 20 | 41 | 60 | 131 | 6 | 10 | 98 | 154 |
| Number of subjects | 16 | 16 | 16 | 16 | 16 | 16 | 14 | 14 | 16 | 16 | 12 | 11 | 8 | 8 | 7 | 6 |
| p-value | 0.924 | 0.788 | 0.492 | 0.082 | 0.496 | 0.617 | 0.955 | 0.364 | 0.59 | 0.292 | 0.231 | 0.062 | 0.893 | 0.846 | 0.208 | 0.049 |
| Dietary Intake in Each Study Phase | |||||
|---|---|---|---|---|---|
| Phase A (No Intervention) | Phase B (An Additional 50 mg/day Phenylalanine from Fruits and Vegetables) | Phase C (An Additional 100 mg/day Phenylalanine from Fruits and Vegetables) | Phase D (An Additional 50 mg/day Phenylalanine from Milk Protein) | Phase E (An Additional 100 mg/day Phenylalanine from Milk Protein) | |
| Median phenylalanine intake (range) in mg/day | 500 (range: 325–1525) | 588 (range: 450–1650) | 638 (range: 400–1725) | 563 (range: 475–1650) | 625 (range: 600–1725) |
| Number of patients completing 4 weeks of intervention | 16 | 16 | 14 | 11 | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinto, A.; Daly, A.; Rocha, J.C.; Ashmore, C.; Evans, S.; Jackson, R.; Payne, A.; Hickson, M.; MacDonald, A. Impact of Fruit and Vegetable Protein vs. Milk Protein on Metabolic Control of Children with Phenylketonuria: A Randomized Crossover Controlled Trial. Nutrients 2022, 14, 4268. https://doi.org/10.3390/nu14204268
Pinto A, Daly A, Rocha JC, Ashmore C, Evans S, Jackson R, Payne A, Hickson M, MacDonald A. Impact of Fruit and Vegetable Protein vs. Milk Protein on Metabolic Control of Children with Phenylketonuria: A Randomized Crossover Controlled Trial. Nutrients. 2022; 14(20):4268. https://doi.org/10.3390/nu14204268
Chicago/Turabian StylePinto, Alex, Anne Daly, Júlio César Rocha, Catherine Ashmore, Sharon Evans, Richard Jackson, Anne Payne, Mary Hickson, and Anita MacDonald. 2022. "Impact of Fruit and Vegetable Protein vs. Milk Protein on Metabolic Control of Children with Phenylketonuria: A Randomized Crossover Controlled Trial" Nutrients 14, no. 20: 4268. https://doi.org/10.3390/nu14204268
APA StylePinto, A., Daly, A., Rocha, J. C., Ashmore, C., Evans, S., Jackson, R., Payne, A., Hickson, M., & MacDonald, A. (2022). Impact of Fruit and Vegetable Protein vs. Milk Protein on Metabolic Control of Children with Phenylketonuria: A Randomized Crossover Controlled Trial. Nutrients, 14(20), 4268. https://doi.org/10.3390/nu14204268