
Food Protein-Induced Enterocolitis Syndrome in Children with Down Syndrome: A Pilot Case-Control Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
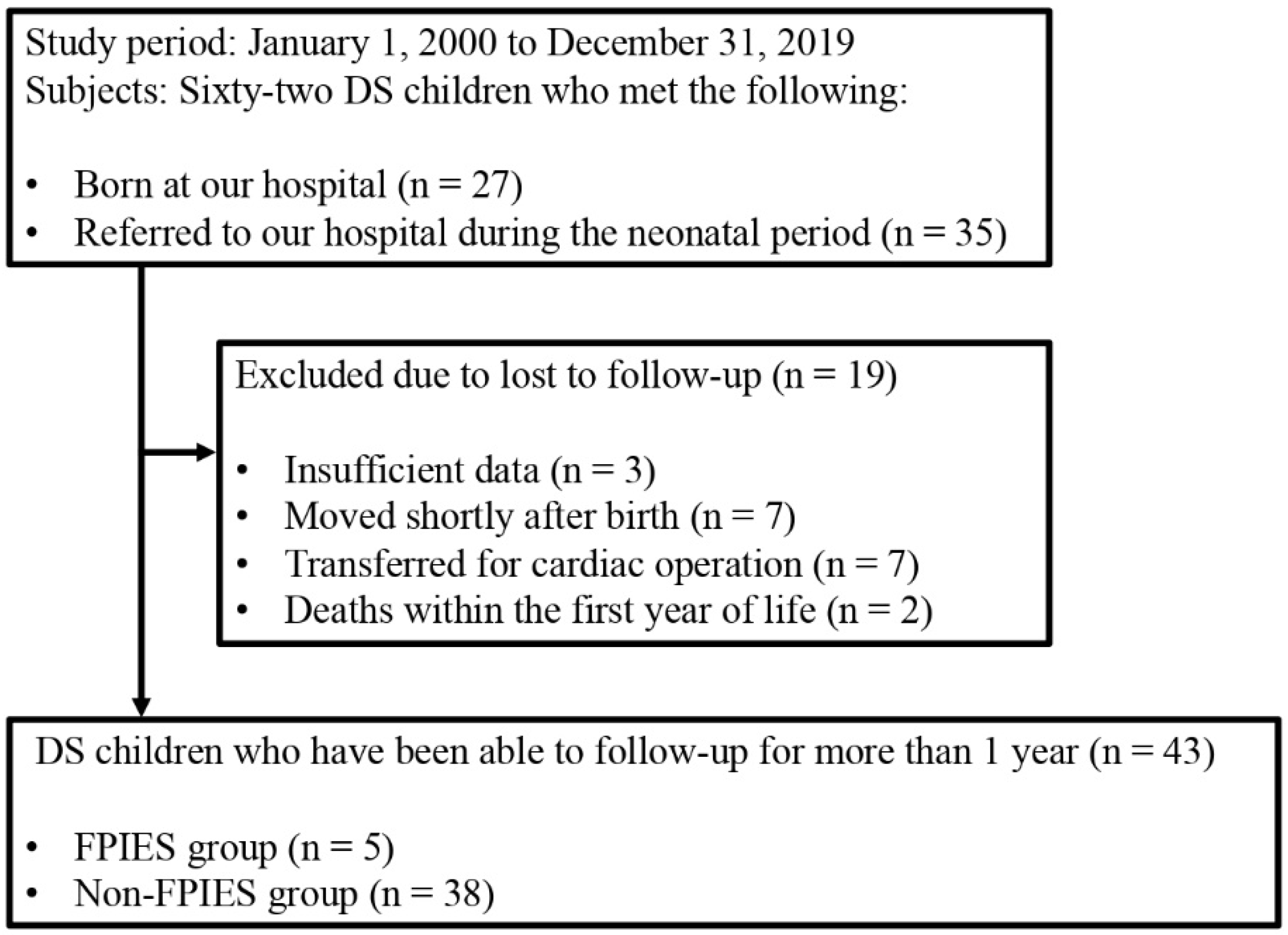
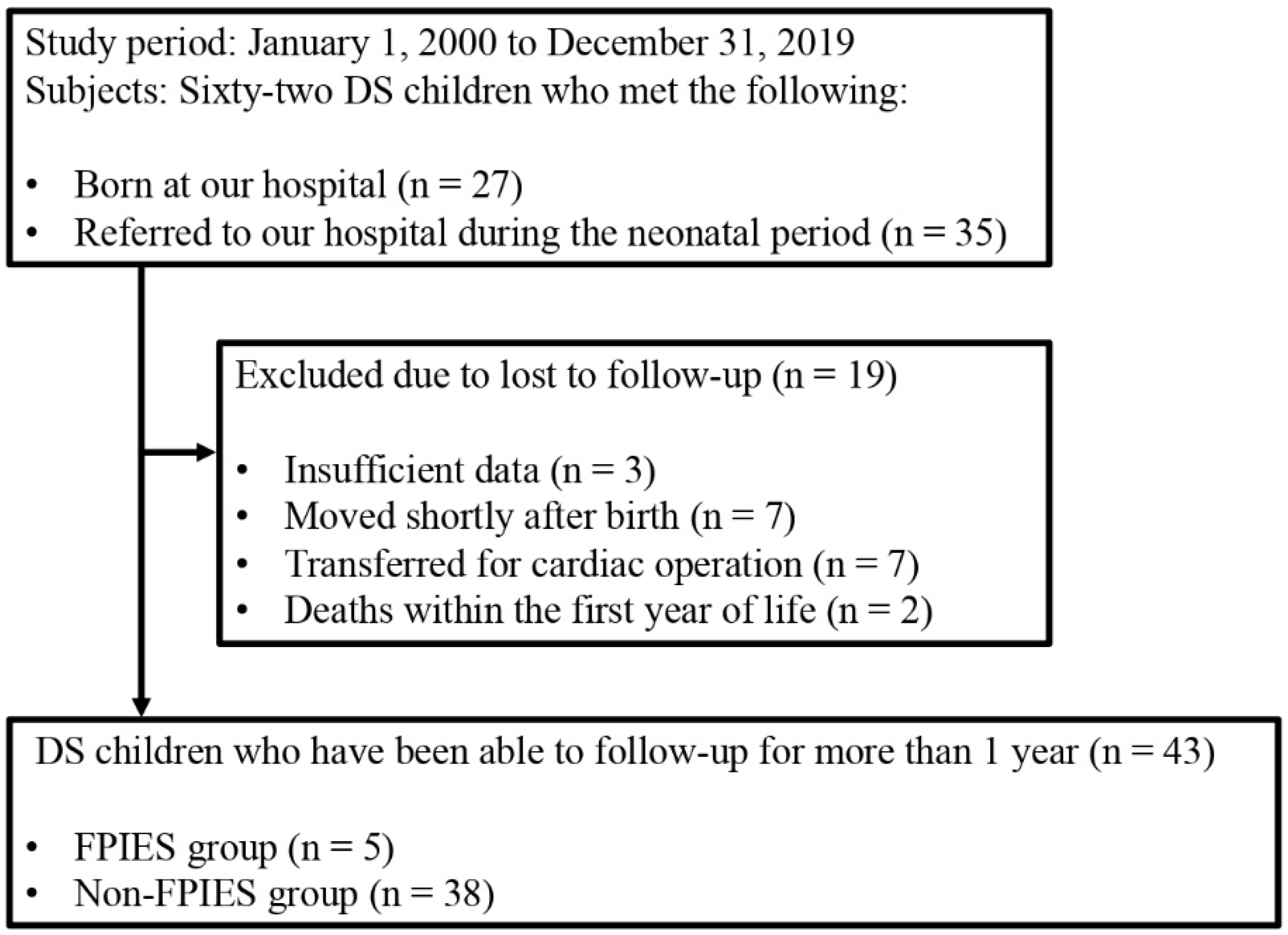
2.1. Study Population and Data
2.2. Outcome Measurements
2.3. Statistical Analyses
3. Results
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nowak-Węgrzyn, A.; Katz, Y.; Mehr, S.S.; Koletzko, S. Non-IgE-mediated gastrointestinal food allergy. J. Allergy Clin. Immunol. 2015, 135, 1114–1124. [Google Scholar] [CrossRef]
- Powell, G.K. Food protein-induced enterocolitis of infancy: Differential diagnosis and management. Compr. Ther. 1986, 12, 28–37. [Google Scholar]
- Järvinen, K.M.; Nowak-Węgrzyn, A. Food protein-induced enterocolitis syndrome (FPIES): Current management strategies and review of the literature. J. Allergy Clin. Immunol. Pract. 2013, 1, 317–322. [Google Scholar] [CrossRef]
- Caubet, J.C.; Bencharitiwong, R.; Ross, A.; Sampson, H.A.; Berin, M.C.; Nowak-Węgrzyn, A. Humoral and cellular responses to casein in patients with food protein-induced enterocolitis to cow’s milk. J. Allergy Clin. Immunol. 2017, 139, 572–583. [Google Scholar] [CrossRef] [Green Version]
- Katz, Y.; Goldberg, M.R.; Rajuan, N.; Cohen, A.; Leshno, M. The prevalence and natural course of food protein-induced enterocolitis syndrome to cow’s milk: A large-scale, prospective population-based study. J. Allergy Clin. Immunol. 2011, 127, 647–653. [Google Scholar] [CrossRef]
- Alonso, S.B.; Ezquiaga, J.G.; Berzal, P.T.; Tardón, S.D.; San José, M.M.; López, P.A.; Bermejo, T.B.; Teruel, S.Q.; Echeverría Zudaire, L.Á. Food protein-induced enterocolitis syndrome: Increased prevalence of this great unknown-results of the PREVALE study. J. Allergy Clin. Immunol. 2019, 143, 430–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nowak-Wegrzyn, A.; Warren, C.M.; Brown-Whitehorn, T.; Cianferoni, A.; Schultz-Matney, F.; Gupta, R.S. Food protein-induced enterocolitis syndrome in the US population-based study. J. Allergy Clin. Immunol. 2019, 144, 1128–1130. [Google Scholar] [CrossRef] [Green Version]
- Caubet, J.C.; Nowak-Węgrzyn, A. Current understanding of the immune mechanisms of food protein-induced enterocolitis syndrome. Expert Rev. Clin. Immunol. 2011, 7, 317–327. [Google Scholar] [CrossRef]
- Konstantinou, G.N.; Bencharitiwong, R.; Grishin, A.; Caubet, J.C.; Bardina, L.; Sicherer, S.H.; Sampson, H.A.; Nowak-Węgrzyn, A. The role of casein-specific IgA and TGF-β in children with food protein-induced enterocolitis syndrome to milk. Pediatr. Allergy Immunol. 2014, 25, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Hoshi, N.; Hattori, R.; Hanatani, K.; Okuyama, K.; Yamada, H.; Kishida, T.; Yamada, T.; Sagawa, T.; Sumiyoshi, Y.; Fujimoto, S. Recent trends in the prevalence of Down syndrome in Japan, 1980–1997. Am. J. Med. Genet. 1999, 84, 340–345. [Google Scholar] [CrossRef]
- Shin, M.; Besser, L.M.; Kucik, J.E.; Lu, C.; Siffel, C.; Correa, A.; Congenital anomaly multistate prevalence and survival collaborative. Prevalence of Down syndrome among children and adolescents in 10 regions of the United States. Pediatrics 2009, 124, 1565–1571. [Google Scholar] [CrossRef]
- Loane, M.; Morris, J.K.; Addor, M.C.; Arriola, L.; Budd, J.; Doray, B.; Garne, E.; Gatt, M.; Haeusler, M.; Khoshnood, B.; et al. Twenty-year trends in the prevalence of Down syndrome and other trisomies in Europe: Impact of maternal age and prenatal screening. Eur. J. Hum. Genet. 2013, 21, 27–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bull, M.J.; Committee on Genetics. Health supervision for children with Down syndrome. Pediatrics 2011, 128, 393–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eijsvoogel, N.B.; Hollegien, M.I.; Bok, L.A.; Derksen-Lubsen, G.; Dikken, F.P.J.; Leenders, A.C.A.P.; Pijning, A.; Post, E.D.M.; Wojciechowski, M.; Schmitz, R.; et al. Lower percentage of allergic sensitization in children with Down syndrome. Pediatr. Allergy Immunol. 2017, 28, 852–857. [Google Scholar] [CrossRef] [PubMed]
- Wakiguchi, H.; Hasegawa, S.; Kaneyasu, H.; Kajimoto, M.; Fujimoto, Y.; Hirano, R.; Katsura, S.; Matsumoto, K.; Ichiyama, T.; Ohga, S. Long-lasting non-IgE-mediated gastrointestinal cow’s milk allergy in infants with Down syndrome. Pediatr. Allergy Immunol. 2015, 26, 821–823. [Google Scholar] [CrossRef]
- Nowak-Węgrzyn, A.; Chehade, M.; Groetch, M.E.; Spergel, J.M.; Wood, R.A.; Allen, K.; Atkins, D.; Bahna, S.; Barad, A.V.; Berin, C.; et al. International consensus guidelines for the diagnosis and management of food protein-induced enterocolitis syndrome: Executive summary-Workgroup Report of the Adverse Reactions to Foods Committee, American Academy of Allergy, Asthma & Immunology. J. Allergy Clin. Immunol. 2017, 139, 1111–1126. [Google Scholar]
- Korai, T.; Kouchi, K.; Takenouchi, A.; Matsuoka, A.; Yabe, K.; Nakata, C. Neonates undergoing gastrointestinal surgery have a higher incidence of non-IgE-mediated gastrointestinal food allergies. Pediatr. Surg. Int. 2018, 34, 1009–1017. [Google Scholar] [CrossRef]
- Schmitt, E.G.; Williams, C.B. Generation and function of induced regulatory T cells. Front. Immunol. 2013, 4, 152. [Google Scholar] [CrossRef] [Green Version]
- Levin, S.; Schlesinger, M.; Handzel, Z.; Hahn, T.; Altman, Y.; Czernobilsky, B.; Boss, J. Thymic deficiency in Down’s syndrome. Pediatrics 1979, 63, 80–87. [Google Scholar] [CrossRef]
- Karlsson, M.R.; Rugtveit, J.; Brandtzaeg, P. Allergen-responsive CD4+CD25+ regulatory T cells in children who have outgrown cow’s milk allergy. J. Exp. Med. 2004, 199, 1679–1688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellegrini, F.P.; Marinoni, M.; Frangione, V.; Tedeschi, A.; Gandini, V.; Ciglia, F.; Mortara, L.; Accolla, R.S.; Nespoli, L. Down syndrome, autoimmunity and T regulatory cells. Clin. Exp. Immunol. 2012, 169, 238–243. [Google Scholar] [CrossRef]
- Sanjabi, S.; Zenewicz, L.A.; Kamanaka, M.; Flavell, R.A. Anti-inflammatory and pro-inflammatory roles of TGF-beta, IL-10, and IL-22 in immunity and autoimmunity. Curr. Opin. Pharmacol. 2009, 9, 447–453. [Google Scholar] [CrossRef] [Green Version]
- Li, M.O.; Wan, Y.Y.; Sanjabi, S.; Robertson, A.K.; Flavell, R.A. Transforming growth factor-beta regulation of immune responses. Ann. Rev. Immunol. 2006, 24, 99–146. [Google Scholar] [CrossRef] [PubMed]
- Mori, F.; Barni, S.; Cianferoni, A.; Pucci, N.; de Martino, M.; Novembre, E. Cytokine expression in CD3+ cells in an infant with food protein-induced enterocolitis syndrome (FPIES): Case report. Clin. Dev. Immunol. 2009, 2009, 679381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motomura, Y.; Kitamura, H.; Hijikata, A.; Matsunaga, Y.; Matsumoto, K.; Inoue, H.; Atarashi, K.; Hori, S.; Watarai, H.; Zhu, J.; et al. The transcription factor E4BP4 regulates the production of IL-10 and IL-13 in CD4+ T cells. Nat. Immunol 2011, 12, 450–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, B.N.; Boyle, R.J.; Gore, C.; Simpson, A.; Custovic, A. Food protein-induced enterocolitis syndrome can occur in adults. J. Allergy Clin. Immunol. 2012, 130, 1199–1200. [Google Scholar] [CrossRef] [PubMed]
- Gleich, G.J.; Sebastian, K.; Firszt, R.; Wagner, L.A. Shrimp allergy: Gastrointestinal symptoms commonly occur in the absence of IgE sensitization. J. Allergy Clin. Immunol. Pract. 2016, 4, 316–318. [Google Scholar] [CrossRef]
- Du, Y.J.; Nowak-Wegrzyn, A.; Vadas, P. FPIES in adults. Ann. Allergy Asthma Immunol. 2018, 121, 736–738. [Google Scholar] [CrossRef]
- Tan, J.A.; Smith, W.B. Non-IgE-mediated gastrointestinal food hypersensitivity syndrome in adults. J. Allergy Clin. Immunol. Pract. 2014, 2, 355–357. [Google Scholar] [CrossRef]
- Gonzalez-Delgado, P.; Caparrós, E.; Moreno, M.V.; Cueva, B.; Fernández, J. Food protein-induced enterocolitis-like syndrome in a population of adolescents and adults caused by seafood. J. Allergy Clin. Immunol. Pract. 2019, 7, 670–672. [Google Scholar] [CrossRef] [PubMed]
- Caubet, J.C.; Cianferoni, A.; Groetch, M.; Nowak-Wegrzyn, A. Food protein-induced enterocolitis syndrome. Clin. Exp. Allergy 2019, 49, 1178–1190. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| FPIES (n = 5) | Non–FPIES (n = 38) | p-Value | |
|---|---|---|---|
| Male (n (%)) | 3 (60.0) | 20 (52.6) | 1.000 † |
| Median gestational age (weeks (range)) | 37 (31–38) | 38 (30–40) | 0.168 ‡ |
| Median birth weight (g (range)) | 2803 (1714–3224) | 2802 (978–3500) | 0.910 ‡ |
| Delivery type (n (%)) | |||
| Vaginal | 3 (60.0) | 27 (71.1) | 0.630 † |
| Emergency cesarean section | 1 (20.0) | 8 (21.1) | 1.000 † |
| Elective cesarean section | 1 (20.0) | 3 (7.9) | 0.402 † |
| Neonatal asphyxia (n (%)) | 1/4 (25.0) | 5/37 (13.5) | 0.483 † |
| Neonatal jaundice (n (%)) | 2/4 (50.0) | 16/37 (43.2) | 1.000 † |
| Nutrition (n (%)) | |||
| Mixed feeding | 4 (80.0) | 28/32 (87.5) | 0.538 † |
| Formula milk | 1 (20.0) | 4/32 (12.5) | 0.538 † |
| Breast milk only | 0 (0) | 0/32 (0) | 1.000 † |
| Comorbidities (n (%)) | |||
| Cardiac disease | 3 (60.0) | 26 (68.4) | 1.000 † |
| ASD | 1 (20.0) | 7 (18.4) | 1.000 † |
| TOF/DORV | 1 (20.0) | 5 (13.2) | 0.547 † |
| PDA | 0 (0) | 4 (10.5) | 1.000 † |
| AVSD | 1 (20.0) | 3 (7.9) | 0.402 † |
| VSD + PDA | 0 (0) | 3 (7.9) | 1.000 † |
| VSD | 0 (0) | 1 (2.6) | 1.000 † |
| VSD + ASD | 0 (0) | 1 (2.6) | 1.000 † |
| VSD + ASD + PDA | 0 (0) | 1 (2.6) | 1.000 † |
| PVP | 0 (0) | 1 (2.6) | 1.000 † |
| Gastrointestinal disease | 2 (40.0) | 4 (10.5) | 0.136 † |
| Duodenal atresia | 0 (0) | 3 (7.9) | 1.000 † |
| Imperforate anus | 1 (20.0) | 1 (2.6) | 0.222 † |
| Rectovaginal fistula | 1 (20.0) | 0 (0) | 0.116 † |
| Hematological disorder | 1 (20.0) | 2 (5.3) | 0.316 † |
| TAM | 1 (20.0) | 2 (5.3) | 0.316 † |
| FPIES (n = 5) | Non–FPIES (n = 38) | p-Value † | |
|---|---|---|---|
| Surgical history (n (%)) | 3 (60.0) | 12 (31.6) | 0.324 |
| Surgery for cardiac disease (n (%)) | 1 (20.0) | 10 (26.3) | 1.000 |
| Intracardiac repair | 0 (0) | 5 (13.2) | 1.000 |
| Ductus arteriosus ligation | 0 (0) | 3 (7.9) | 1.000 |
| BT shunt | 0 (0) | 2 (5.3) | 1.000 |
| PA banding | 1 (20.0) | 0 (0) | 0.116 |
| Surgery for gastrointestinal disease (n (%)) | 2 (40.0) | 4 (10.5) § | 0.136 |
| Duodenal atresia repair | 0 (0) | 3 (7.9) § | 1.000 |
| Colostomy | 2 (40.0) | 1 (2.6) | 0.032 * |
| FPIES (n = 5) | Non–FPIES (n = 6) | p-Value | |
|---|---|---|---|
| Male (n (%)) | 3 (60.0) | 3 (50.0) | 1.000 † |
| Median age at total IgE test (months (range)) | 3 (1–12) | 10 (1–12) | 0.230 ‡ |
| Median total IgE (IU/mL (range)) | <11 (<11–11) | <11 (<11–16) | 1.000 ‡ |
| Participant | 1 [15] | 2 | 3 | 4 [15] | 5 |
|---|---|---|---|---|---|
| Sex | male | male | male | female | female |
| Age at onset (days) | 7 | 84 | 321 | 64 | 104 |
| Causative foods | CM | CM | wheat | CM | CM |
| Clinical symptoms | |||||
| Vomiting | + | + | + | + | + |
| Diarrhea | + | + | + | + | + |
| Bloody stools | – | + | – | + | – |
| Abdominal distention | + | N/A | N/A | N/A | + |
| Fever | – | + | + | + | + |
| Metabolic acidosis | + | + | – | + | + |
| Dehydration/Shock | – | – | – | + | + |
| Severity [16] | severe | severe | severe | severe | severe |
| Comorbidities | |||||
| Cardiac disease | – | + (TOF) | – | + (ASD) | + (AVSD) |
| Gastrointestinal disease | – | – | – | + (rectovaginal fistula) | + (imperforate anus) |
| Hematological disorder | – | – | + (TAM) | – | – |
| Surgical history | N/A | PA banding | N/A | colostomy | colostomy |
| Age at surgery (days) | N/A | 50 | N/A | 63 | 1 |
| Age at tolerance (months) | 132 | 26 | N/A | 49 | 18 |
| Total IgE (IU/mL) | 11 | <11 | <11 | <11 | <11 |
| Antigen-specific IgE (kUA/L) | <0.35 | <0.35 | <0.35 | <0.35 | <0.35 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okazaki, F.; Wakiguchi, H.; Korenaga, Y.; Takahashi, K.; Yasudo, H.; Fukuda, K.; Shimokawa, M.; Hasegawa, S. Food Protein-Induced Enterocolitis Syndrome in Children with Down Syndrome: A Pilot Case-Control Study. Nutrients 2022, 14, 388. https://doi.org/10.3390/nu14020388
Okazaki F, Wakiguchi H, Korenaga Y, Takahashi K, Yasudo H, Fukuda K, Shimokawa M, Hasegawa S. Food Protein-Induced Enterocolitis Syndrome in Children with Down Syndrome: A Pilot Case-Control Study. Nutrients. 2022; 14(2):388. https://doi.org/10.3390/nu14020388
Chicago/Turabian StyleOkazaki, Fumiko, Hiroyuki Wakiguchi, Yuno Korenaga, Kazumasa Takahashi, Hiroki Yasudo, Ken Fukuda, Mototsugu Shimokawa, and Shunji Hasegawa. 2022. "Food Protein-Induced Enterocolitis Syndrome in Children with Down Syndrome: A Pilot Case-Control Study" Nutrients 14, no. 2: 388. https://doi.org/10.3390/nu14020388
APA StyleOkazaki, F., Wakiguchi, H., Korenaga, Y., Takahashi, K., Yasudo, H., Fukuda, K., Shimokawa, M., & Hasegawa, S. (2022). Food Protein-Induced Enterocolitis Syndrome in Children with Down Syndrome: A Pilot Case-Control Study. Nutrients, 14(2), 388. https://doi.org/10.3390/nu14020388