
Additive Effects of Exercise or Nutrition Intervention in a 24-Month Multidisciplinary Treatment with a Booster Intervention for Children and Adolescents with Overweight or Obesity: The ICAAN Study

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
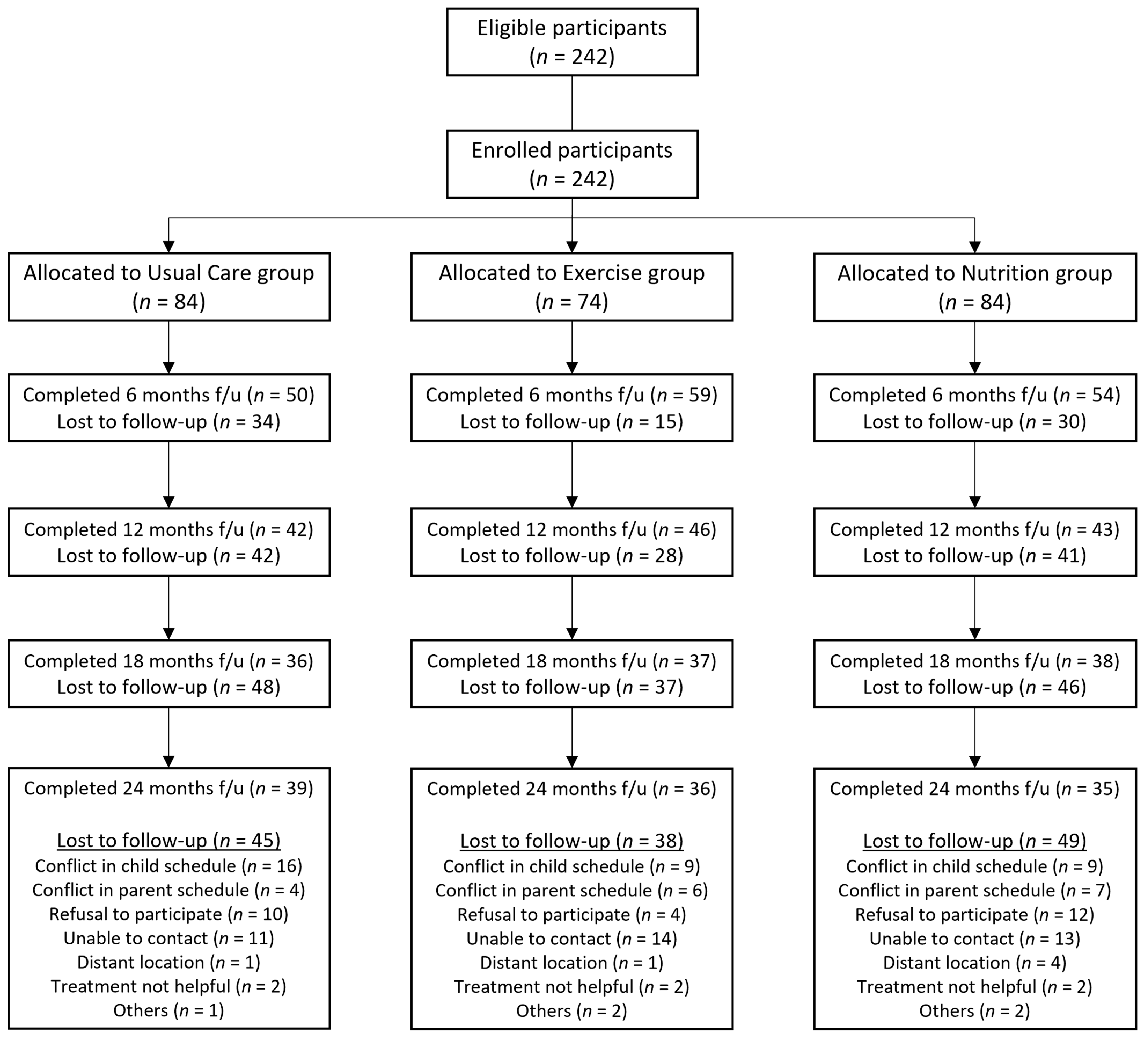
2.1. Participants
2.2. Study Design
2.3. Intervention
2.3.1. Usual Care Group
2.3.2. Exercise Group
2.3.3. Nutrition Group
2.4. Measurement
2.4.1. Anthropometric Measurement
2.4.2. Biochemical Assessment
2.4.3. Dietary and Physical Activity Assessment
2.5. Procedures
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
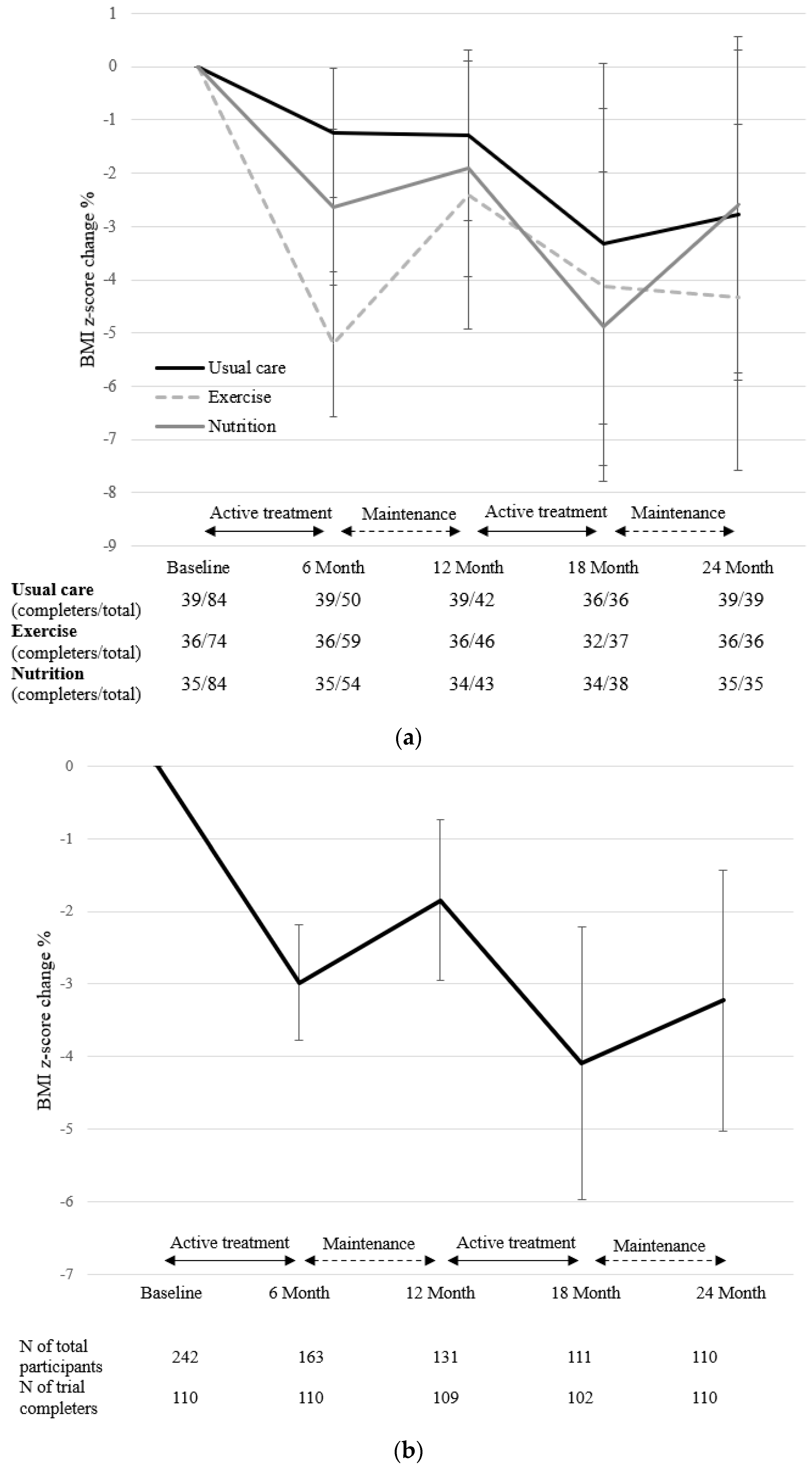
3.2. Changes in Primary Outcomes
3.3. Changes in Secondary Outcomes
3.4. Changes in Outcome Variables According to Sex
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weiss, R.; Dziura, J.; Burgert, T.S.; Tamborlane, W.V.; Taksali, S.E.; Yeckel, C.W.; Allen, K.; Lopes, M.; Savoye, M.; Morrison, J.; et al. Obesity and the metabolic syndrome in children and adolescents. N. Engl. J. Med. 2004, 350, 2362–2374. [Google Scholar] [CrossRef] [PubMed]
- Nobili, V. Non Alcoholic Fatty Liver Disease In Children. In The ECOG’s eBook on Child and Adolescent Obesity; De Onis, M., Ed.; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Wabitsch, M.; Moss, A.; Kromeyer-Hauschild, K. Unexpected plateauing of childhood obesity rates in developed countries. BMC Med. 2014, 12, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Chung, A.; Backholer, K.; Wong, E.; Palermo, C.; Keating, C.; Peeters, A. Trends in child and adolescent obesity prevalence in economically advanced countries according to socioeconomic position: A systematic review. Obes. Rev. 2016, 17, 276–295. [Google Scholar] [CrossRef]
- Ha, K.H.; Kim, D.J. Epidemiology of childhood obesity in Korea. Endocrinol. Metab. 2016, 31, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Ma, H.; Lee, Y.; Oh, H. Trends in Intervention Study for Childhood Obesity in Korea. Child Health Nurs. Res. 2017, 23, 81–90. [Google Scholar] [CrossRef][Green Version]
- American Dietetic Association. Position of the American dietetic association: Individual-, family-, school-, and community-based interventions for pediatric overweight. J. Am. Diet. Assoc. 2006, 106, 925–945. [Google Scholar] [CrossRef]
- Grossman, D.C.; Bibbins-Domingo, K.; Curry, S.J.; Barry, M.J.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W.; Kemper, A.R.; Krist, A.H.; Kurth, A.E.; et al. Screening for obesity in children and adolescents us preventive services task force recommendation statement. J. Am. Med. Assoc. 2017, 317, 2417–2426. [Google Scholar]
- Raynor, H.A.; Barroso, C.; Propst, S.; Berlin, K.; Robson, S.; Khatri, P. Reach of a low-intensity, multicomponent childhood overweight and obesity intervention delivered in an integrated primary care setting. Transl. Behav. Med. 2019, 10, 760–769. [Google Scholar] [CrossRef]
- Tsao-Wu, M.; Williams, R.J.; Hendy, H.M.; Novick, M.B. Associations between obesity severity and medical comorbidities for children with obesity in low intensity hospital intervention. Obes. Res. Clin. Pract. 2019, 13, 555–560. [Google Scholar] [CrossRef]
- Anastasiou, C.A.; Karfopoulou, E.; Yannakoulia, M. Weight regaining: From statistics and behaviors to physiology and metabolism. Metabolism 2015, 64, 1395–1407. [Google Scholar] [CrossRef] [PubMed]
- Aronne, L.J.; Hall, K.D.; Jakicic, J.M.; Leibel, R.L.; Lowe, M.R.; Rosenbaum, M.; Klein, M. Describing the Weight-Reduced State: Physiology, Behavior, and Interventions. Obesity 2021, 29, S9–S24. [Google Scholar] [CrossRef] [PubMed]
- Chapman, J.; Armitage, C. Evidence that boosters augment the long-term impact of implementation intentions on fruit and vegetable intake. Psychol. Health 2010, 25, 365–381. [Google Scholar] [CrossRef] [PubMed]
- Fleig, L.; Pomp, S.; Schwarzer, R.; Lippke, S. Promoting exercise maintenance: How interventions with booster sessions improve long-term rehabilitation outcomes. Rehabil. Psychol. 2013, 58, 323–333. [Google Scholar] [CrossRef]
- Moon, J.S.; Lee, S.Y.; Nam, C.M.; Choi, J.-M.; Choe, B.-K.; Seo, J.-W.; Oh, K.; Jang, M.-J.; Hwang, S.-S.; Yoo, M.H.; et al. 2007 Korean National Growth Charts: Review of developmental process and an outlook. Korean J. Pediatr. 2008, 51, 1–25. [Google Scholar] [CrossRef]
- Lee, S.Y.; Kim, J.; Oh, S.; Kim, Y.; Woo, S.; Jang, H.B.; Lee, H.-J.; Park, S.I.; Park, K.H.; Lim, H. A 24-week intervention based on nutrition care process improves diet quality, body mass index, and motivation in children and adolescents with obesity. Nutr. Res. 2020, 84, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Lacey, K.; Pritchett, E. Nutrition Care Process and Model: ADA adopts road map to quality care and outcomes management. J. Am. Diet. Assoc. 2003, 103, 1061–1072. [Google Scholar] [CrossRef]
- Armstrong, T.; Bull, F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). J. Public Health 2006, 14, 66–70. [Google Scholar] [CrossRef]
- Lee, J.; Lee, C.; Min, J.; Kang, D.-W.; Kim, J.-Y.; Yang, H.I.; Park, J.; Lee, M.-K.; Park, I.; Jae, S.Y.; et al. Development of the Korean Global Physical Activity Questionnaire: Reliability and validity study. Glob. Health Promot. 2020, 27, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Medrano, M.; Arenaza, L.; Ramírez-Vélez, R.; Ortega, F.B.; Ruiz, J.R.; Labayen, I. Prevalence of responders for hepatic fat, adiposity and liver enzyme levels in response to a lifestyle intervention in children with overweight/obesity: EFIGRO randomized controlled trial. Pediatr. Diabetes 2019, 21, 215–223. [Google Scholar] [CrossRef]
- Labayen, I.; Medrano, M.; Arenaza, L.; Maíz, E.; Osés, M.; Martínez-Vizcaíno, V.; Ruiz, J.R.; Ortega, F.B. Effects of exercise in addition to a family-based lifestyle intervention program on hepatic fat in children with overweight. Diabetes Care 2019, 43, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Seo, Y.-G.; Lim, H.; Kim, Y.; Ju, Y.-S.; Choi, Y.-J.; Lee, H.-J.; Jang, H.B.; Park, S.I.; Park, K.H. Effects of circuit training or a nutritional intervention on body mass index and other cardiometabolic outcomes in children and adolescents with overweight or obesity. PLoS ONE 2021, 16, e0245875. [Google Scholar] [CrossRef] [PubMed]
- Hao, M.; Han, W.; Yamauchi, T. Short-Term and Long-Term Effects of a Combined Intervention of Rope Skipping and Nutrition Education for Overweight Children in Northeast China. Asia Pac. J. Public Health 2019, 31, 348–358. [Google Scholar] [CrossRef]
- Meyer, U.; Schindler, C.; Zahner, L.; Ernst, D.; Hebestreit, H.; Van Mechelen, W.; Rocca, H.-P.B.-L.; Probst-Hensch, N.; Puder, J.; Kriemler, S. Long-term effect of a school-based physical activity program (kiss) on fitness and adiposity in children: A cluster-randomized controlled trial. PLoS ONE 2014, 9, e87929. [Google Scholar] [CrossRef] [PubMed]
- Ruotsalainen, H.; Kyngäs, H.; Tammelin, T.; Kääriäinen, M. Systematic review of physical activity and exercise interventions on body mass indices, subsequent physical activity and psychological symptoms in overweight and obese adolescents. J. Adv. Nurs. 2015, 71, 2461–2477. [Google Scholar] [CrossRef] [PubMed]
- Alberga, A.S.; Medd, E.R.; Adamo, K.B.; Goldfield, G.S.; Prud’Homme, D.; Kenny, G.P.; Sigal, R.J. Top 10 practical lessons learned from physical activity interventions in overweight and obese children and adolescents. Appl. Physiol. Nutr. Metab. 2013, 38, 249–258. [Google Scholar] [CrossRef] [PubMed]
- St. Laurent, C.W.; Burkart, S.; Alhassan, S. Feasibility, Acceptability, and Preliminary Efficacy of a Recess-Based Fitness Intervention in Elementary School Children. Int. J. Exerc. Sci. 2019, 12, 1225–1243. [Google Scholar]
- Horsak, B.; Schwab, C.; Baca, A.; Greber-Platzer, S.; Kreissl, A.; Nehrer, S.; Keilani, M.; Crevenna, R.; Kranzl, A.; Wondrasch, B. Effects of a lower extremity exercise program on gait biomechanics and clinical outcomes in children and adolescents with obesity: A randomized controlled trial. Gait Posture 2019, 70, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Ma, Y.; Mo, D.; Zhang, S.; Xiang, M.; Zhang, Z. Methodology of an exercise intervention program using social incentives and gamification for obese children. BMC Public Health 2019, 19, 686. [Google Scholar] [CrossRef] [PubMed]
- Alberga, A.S.; Sigal, R.J.; Sweet, S.N.; Doucette, S.; Russell-Mayhew, S.; Tulloch, H.; Kenny, G.P.; Prud’Homme, D.; Hadjiyannakis, S.; Goldfield, G.S. Understanding low adherence to an exercise program for adolescents with obesity: The HEARTY trial. Obes. Sci. Pract. 2019, 5, 437–448. [Google Scholar] [CrossRef]
- Dulloo, A.G. Physiology of weight regain: Lessons from the classic Minnesota Starvation Experiment on human body composition regulation. Obes. Rev. 2021, 22, e13189. [Google Scholar] [CrossRef] [PubMed]
- Melby, C.L.; Paris, H.L.; Foright, R.M.; Peth, J. Attenuating the biologic drive for weight regain following weight loss: Must what goes down always go back up? Nutrients 2017, 9, 468. [Google Scholar] [CrossRef] [PubMed]
- Ek, A.; Chamberlain, K.L.; Sorjonen, K.; Hammar, U.; Malek, M.E.; Sandvik, P.; Somaraki, M.; Nyman, J.; Lindberg, L.; Nordin, K.; et al. A Parent Treatment Program for Preschoolers With Obesity: A Randomized Controlled Trial. Pediatrics 2019, 144, e20183457. [Google Scholar] [CrossRef] [PubMed]
- van der Heijden, L.B.; Feskens, E.J.M.; Janse, A.J. Maintenance interventions for overweight or obesity in children: A systematic review and meta-analysis. Obes. Rev. 2018, 19, 798–809. [Google Scholar] [CrossRef] [PubMed]
- Gow, M.L.; Baur, L.A.; Ho, M.; Chisholm, K.; Noakes, M.; Cowell, C.T.; Garnett, S.P. Can early weight loss, eating behaviors and socioeconomic factors predict successful weight loss at 12- and 24-months in adolescents with obesity and insulin resistance participating in a randomised controlled trial? Int. J. Behav. Nutr. Phys. Act. 2016, 13, 43. [Google Scholar] [CrossRef]
- Lazzer, S.; Vermorel, M.; Montaurier, C.; Meyer, M.; Boirie, Y. Changes in adipocyte hormones and lipid oxidation associated with weight loss and regain in severely obese adolescents. Int. J. Obes. 2005, 29, 1184–1191. [Google Scholar] [CrossRef] [PubMed]
- Wilfley, D.E.; Stein, R.; Saelens, B.; Mockus, D.S.; Matt, G.; Hayden-Wade, H.A.; Welch, R.R.; Schechtman, K.B.; Thompson, P.A.; Epstein, L.H. Efficacy of Maintenance Treatment Approaches for Childhood Overweight. JAMA 2007, 298, 1661–1673. [Google Scholar] [CrossRef]
- Hampl, S.; Stough, C.O.; Cordts, K.P.; Best, C.; Blackburn, K.; Gillette, M.L.D. Effectiveness of a hospital-based multidisciplinary pediatric weight management program: Two-year outcomes of phit kids. Child. Obes. 2016, 12, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Siervogel, R.M.; Demerath, E.W.; Schubert, C.; Remsberg, K.E.; Chumlea, W.C.; Sun, S.; Czerwinski, S.A.; Towne, B. Puberty and body composition. Horm. Res. Paediatr. 2003, 60, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Lazzer, S.; Boirie, Y.; Poissonnier, C.; Petit, I.; Duché, P.; Taillardat, M.; Meyer, M.; Vermorel, M. Longitudinal changes in activity patterns, physical capacities, energy expenditure, and body composition in severely obese adolescents during a multidisciplinary weight-reduction program. Int. J. Obes. 2004, 29, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Vander Wyst, K.B.; Olson, M.L.; Keller, C.S.; Soltero, E.G.; Williams, A.N.; Peña, A.; Ayers, S.L.; Jager, J.; Shaibi, G.Q. Sex as a moderator of body composition following a randomized controlled lifestyle intervention among Latino youth with obesity. Pediatr. Obes. 2020, 15, e12620. [Google Scholar] [CrossRef] [PubMed]
- Simen-Kapeu, A.; Veugelers, P.J. Should public health interventions aimed at reducing childhood overweight and obesity be gender-focused? BMC Public Health 2010, 10, 340. [Google Scholar] [CrossRef] [PubMed]
- Sweeting, H.N. Gendered dimensions of obesity in childhood and adolescence. Nutr. J. 2008, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, A.N.; Metcalf, B.S.; Hosking, J.; Streeter, A.J.; Voss, L.D.; Wilkin, T.J. Age before stage: Insulin resistance rises before the onset of puberty: A 9-year longitudinal study (earlybird 26). Diabetes Care 2012, 35, 536–541. [Google Scholar] [CrossRef] [PubMed]
- Reinehr, T.; Kiess, W.; Kapellen, T.; Andler, W. Insulin sensitivity among obese children and adolescents, according to degree of weight loss. Pediatrics 2004, 114, 1569–1573. [Google Scholar] [CrossRef] [PubMed]
- Marson, E.C.; Delevatti, R.S.; Prado, A.K.G.; Netto, N.; Kruel, L.F.M. Effects of aerobic, resistance, and combined exercise training on insulin resistance markers in overweight or obese children and adolescents: A systematic review and meta-analysis. Prev. Med. 2016, 93, 211–218. [Google Scholar] [CrossRef]
- Skelton, J.A.; Beech, B.M. Attrition in paediatric weight management: A review of the literature and new directions. Obes. Rev. 2011, 12, e273–e281. [Google Scholar] [CrossRef]
- Park, J.; Woo, S.; Ju, Y.-S.; Seo, Y.-G.; Lim, H.-J.; Kim, Y.-M.; Noh, H.-M.; Lee, H.-J.; Park, S.I.; Park, K.H. Factors associated with dropout in a lifestyle modification program for weight management in children and adolescents. Obes. Res. Clin. Pract. 2020, 14, 566–572. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total Participants (n = 242) | Completers (n = 110) | |||||||
|---|---|---|---|---|---|---|---|---|
| Usual Care Group (n = 84) | Exercise Group (n = 74) | Nutrition Group (n = 84) | p-Value | Usual Care Group (n = 39) | Exercise Group (n = 36) | Nutrition Group (n = 35) | p-Value | |
| Age * | 11.02 (10.01, 12.09) | 10.08 (9.04, 12.03) | 11.01 (9.11, 12.05) | 0.163 | 10.10 (9.10, 12.01) | 10.05 (9.01, 11.76) | 11.00 (9.06, 12.11) | 0.461 |
| Sex | ||||||||
| Male | 51 (60.7%) | 38 (51.4%) | 56 (66.7%) | 0.144 | 25 (64.1%) | 18 (50.0%) | 24 (68.6%) | 0.243 |
| Female | 33 (39.3%) | 36 (48.6%) | 28 (33.3%) | 14 (35.9%) | 18 (50.0%) | 11 (31.4%) | ||
| BMI (kg/m2) * | 27.65 (25.24, 30.13) | 27.40 (25.08, 30.53) | 27.65 (25.78, 30.85) | 0.774 | 27.40 (24.60, 29.20) | 27.50 (24.93, 30.48) | 28.30 (25.30, 30.70) | 0.549 |
| BMI z-score * | 2.15 (1.93, 2.55) | 2.34 (2.01, 2.73) | 2.23 (1.92, 2.59) | 0.175 | 2.12 (1.94, 2.52) | 2.37 (2.02, 2.73) | 2.22 (1.98, 2.64) | 0.322 |
| Fat mass index * | 11.30 (10.25, 12.93) | 11.74 (9.83, 13.25) | 11.45 (10.49, 13.29) | 0.928 | 11.33 (10.30, 12.73) | 11.08 (9.61, 13.23) | 11.45 (10.54, 13.08) | 0.660 |
| Fat-free mass index * | 15.72 (14.41, 17.67) | 15.75 (14.72, 18.03) | 16.27 (15.06, 17.61) | 0.667 | 15.51 (14.40, 17.28) | 15.73 (14.48, 17.65) | 16.37 (14.55, 17.43) | 0.464 |
| Body fat % | 41.87 ± 4.17 | 41.96 ± 4.51 | 41.83 ± 3.65 | 0.979 | 42.35 ± 3.87 | 41.48 ± 5.22 | 41.83 ± 3.16 | 0.661 |
| Monthly household income | ||||||||
| <3 million KRW | 8 (10.7%) | 17 (23.0%) | 13 (16.7%) | 0.303 | 3 (8.1%) | 2 (5.6%) | 7 (20.6%) | 0.272 |
| 3–5 million KRW | 45 (60.0%) | 37 (50.0%) | 47 (60.3%) | 22 (59.5%) | 24 (66.7%) | 20 (58.8%) | ||
| ≥5 million KRW | 22 (29.3%) | 20 (27.0%) | 18 (23.1%) | 12 (32.4%) | 10 (27.8%) | 7 (20.6%) | ||
| AST (U/L) * | 21.50 (18.00, 27.00) | 22.00 (18.75, 27.25) | 24.00 (19.00, 33.00) | 0.117 | 21.00 (18.00, 28.00) | 22.00 (18.00, 25.50) | 25.00 (19.00, 33.00) | 0.165 |
| ALT (U/L) * | 20.00 (14.00, 30.50) | 21.50 (13.00, 2.35) | 26.00 (16.00, 51.75) | 0.053 | 19.00 (16.00, 29.00) | 19.00 (13.00, 31.75) | 26.00 (16.00, 53.00) | 0.143 |
| TG (mg/dL) * | 99.00 (62.00, 147.50) | 97.00 (80.00, 134.75) | 103.00 (74.00, 137.75) | 0.815 | 93.00 (67.00, 151.00) | 101.50 (83.50, 144.00) | 123.00 (68.00, 161.00) | 0.623 |
| HDL-C (mg/dL) * | 50.00 (41.25, 59.00) | 50.00 (41.75, 58.25) | 48.50 (42.25, 57.00) | 0.774 | 51.00 (42.00, 60.00) | 47.00 (41.25, 53.75) | 47.00 (40.00, 53.00) | 0.279 |
| LDL-C (mg/dL) | 113.57 ± 23.64 | 110.49 ± 23.24 | 108.54 ± 25.96 | 0.403 | 118.03 ± 21.03 | 110.31 ± 23.44 | 110.60 ± 23.67 | 0.250 |
| FBS (mg/dL) * | 88.00 (82.25, 93.00) | 88.00 (83.75, 94.00) | 89.00 (95.00, 93.75) | 0.424 | 89.00 (81.00, 93.00) | 88.00 (84.00, 94.00) | 89.00 (86.00, 93.00) | 0.692 |
| Insulin (μU/mL) * | 16.80 (12.40, 23.48) | 19.75 (13.08, 27.25) | 19.20 (14.13, 26.25) | 0.185 | 16.20 (12.40, 23.70) | 20.30 (13.13, 25.25) | 18.60 (14.20, 24.20) | 0.578 |
| HOMA-IR * | 3.97 (2.64, 4.92) | 4.09 (2.97, 6.23) | 4.09 (3.00, 6.03) | 0.140 | 3.63 (2.63, 5.05) | 4.41 (2.92, 5.50) | 4.09 (2.99, 5.61) | 0.424 |
| Total energy intake (kcal) * | 2066.90 (1808.86, 2429.10) | 2084.34 (1767.26, 2402.37) | 2181.52 (1927.96, 2434.87) | 0.234 | 2061.37 (1850.96, 2357.49) | 1998.27 (1698.82, 2393.29) | 2221.56 (1948.25, 2437.43) | 0.267 |
| Physical activity (METs) * | 1146.00 (390.00, 4120.00) | 1040.00 (390.00, 2530.00) | 2240.00 (910.00, 4050.00) | 0.014 † | 1080.00 (480.00, 4000.00) | 1080.00 (400.00, 2400.00) | 2760.00 (600.00, 4560.00) | 0.054 |
| Usual Care Group (n = 39) | Exercise Group (n = 36) | Nutrition Group (n = 35) | p a | Total Participants (n = 110) | β (95% CI) | p b | |
|---|---|---|---|---|---|---|---|
| zBMI | |||||||
| Baseline | 2.27 (0.06) | 2.39 (0.06) | 2.27 (0.05) | 2.31 (0.05) | reference | ||
| change at 6 mo | −0.02 (0.05) | −0.12 (0.05) | −0.07 (0.05) | −0.07 (0.03) | −0.07 (−0.13, −0.02) | ||
| change at 12 mo | −0.03 (0.05) | −0.06 (0.05) | −0.05 (0.05) | −0.04 (0.03) | −0.05 (−0.10, 0.01) | ||
| change at 18 mo | −0.06 (0.05) | −0.10 (0.05) | −0.12 (0.05) | −0.09 (0.03) | −0.09 (−0.15, −0.04) | ||
| change at 24 mo | −0.04 (0.05) | −0.09 (0.05) | −0.06 (0.05) | 0.931 | −0.07 (0.03) | −0.07 (−0.12, −0.01) | 0.016 |
| FMI | |||||||
| Baseline | 11.77 (0.36) | 11.61 (0.48) | 11.94 (0.41) | 11.77 (0.24) | reference | ||
| change at 6 mo | −0.01 (0.22) | −0.32 (0.24) | −0.01 (0.24) | −0.11 (0.14) | −0.14 (−0.42, 0.14) | ||
| change at 12 mo | 0.03 (0.22) | −0.01 (0.24) | −0.07 (0.24) | −0.02 (0.14) | −0.05 (−0.33, 0.24) | ||
| change at 18 mo | 0.12 (0.23) | 0.19 (0.25) | −0.26 (0.25) | −0.02 (0.14) | −0.01 (−0.30, 0.28) | ||
| change at 24 mo | 0.20 (0.22) | 0.27 (0.24) | 0.15 (0.24) | 0.753 | 0.21 (0.14) | 0.18 (−0.11, 0.46) | 0.279 |
| FFMI | |||||||
| Baseline | 15.96 (0.39) | 16.15 (0.37) | 16.49 (0.37) | 16.19 (0.22) | reference | ||
| change at 6 mo | 0.32 (0.11) | 0.03 (0.12) | 0.24 (0.12) | 0.20 (0.07) | 0.22 (0.08, 0.36) | ||
| change at 12 mo | 0.74 (0.11) | 0.76 (0.12) | 0.73 (0.12) | 0.74 (0.07) | 0.76 (0.62, 0.90) | ||
| change at 18 mo | 1.20 (0.11) | 0.82 (0.12) | 1.04 (0.12) | 1.02 (0.07) | 1.04 (0.90, 1.18) | ||
| change at 24 mo | 1.44 (0.11) | 1.18 (0.11) | 1.21 (0.12) | 0.162 | 1.28 (0.07) | 1.30 (1.16, 1.44) | <0.001 |
| Body fat percentage (%) | |||||||
| Baseline | 42.35 (0.62) | 41.48 (0.87) | 41.83 (0.53) | 41.90 (0.40) | reference | ||
| change at 6 mo | −0.57 (0.49) | −0.63 (0.52) | −0.49 (0.53) | −0.56 (−1.14, 0.02) | −0.63 (−1.24, −0.02) | ||
| change at 12 mo | −1.03 (0.49) | −1.21 (0.53) | −1.20 (0.53) | −1.14 (−1.72, −0.55) | −1.21 (−1.82, −0.60) | ||
| change at 18 mo | −1.73 (0.51) | −0.91 (0.54) | −2.13 (0.55) | −1.60 (−2.20, −1.00) | −1.66 (−2.29, −1.03) | ||
| change at 24 mo | −1.96 (0.49) | −1.37 (0.52) | −1.67 (0.53) | 0.674 | −1.68 (−2.26, −1.10) | −1.74 (−2.35, −1.13) | <0.001 |
| AST (U/L) | |||||||
| Baseline | 27.51 (3.26) | 25.39 (2.53) | 32.40 (3.80) | 28.37 (1.87) | reference | ||
| change at 6 mo | −4.05 (2.55) | −0.98 (2.71) | −7.20 (2.73) | −4.09 (1.53) | −4.46 (−7.23, −1.69) | ||
| change at 12 mo | −2.48 (2.57) | 0.45 (2.71) | −7.19 (2.77) | −3.05 (1.55) | −3.42 (−6.21, −v0.62) | ||
| change at 18 mo | −3.53 (2.63) | 1.52 (2.82) | −8.26 (2.75) | −3.53 (1.57) | −3.90 (−6.76, −1.05) | ||
| change at 24 mo | −3.34 (2.57) | −2.34 (2.73) | −7.66 (2.73) | 0.473 | −4.42 (1.54) | −4.79 (−7.58, −2.01) | 0.006 |
| ALT (U/L) | |||||||
| Baseline | 31.46 (6.41) | 32.69 (6.21) | 44.86 (7.60) | 36.13 (3.90) | reference | ||
| change at 6 mo | −7.59 (4.60) | −4.38 (4.87) | −14.94 (4.89) | −8.94 (2.76) | −16.87 (−23.67, −10.08) | ||
| change at 12 mo | −0.73 (4.65) | 7.31 (4.87) | 0.49 (5.03) | 2.21 (2.80) | −5.72 (−12.57, 1.13) | ||
| change at 18 mo | −0.08 (4.83) | −1.47 (5.21) | −12.70 (4.95) | −4.74 (2.88) | −12.67 (−19.67, −5.68) | ||
| change at 24 mo | −1.52 (4.65) | −3.36 (4.92) | −9.65 (4.89) | 0.398 | −4.76 (2.78) | −12.69 (−19.52, −5.86) | <0.001 |
| TG (mg/dL) | |||||||
| Baseline | 110.13 (8.97) | 114.22 (7.56) | 118.63 (9.29) | 114.17 (4.96) | reference | ||
| change at 6 mo | 6.15 (7.68) | 10.21 (8.14) | −12.01 (8.20) | 1.39 (4.62) | 2.28 (−7.59, 12.14) | ||
| change at 12 mo | 15.58 (7.75) | −10.22 (8.14) | 0.58 (8.38) | 2.09 (4.67) | 2.98 (−6.97, 12.93) | ||
| change at 18 mo | 3.55 (7.99) | −5.92 (8.59) | −13.13 (8.28) | −5.21 (4.78) | −4.33 (−14.49, 5.83) | ||
| change at 24 mo | 3.84 (7.75) | −5.03 (8.21) | −1.33 (8.20) | 0.113 | −0.88 (4.65) | 0.00 (−9.92, 9.93) | 0.664 |
| HDL-C (mg/dL) | |||||||
| Baseline | 51.03 (1.66) | 49.44 (2.06) | 47.69 (1.63) | 49.45 (1.03) | reference | ||
| change at 6 mo | −0.26 (1.17) | −1.39 (1.24) | 2.05 (1.25) | 0.15 (0.70) | −0.03 (−1.49, 1.44) | ||
| change at 12 mo | 0.12 (1.18) | 2.24 (1.24) | 3.76 (1.28) | 1.99 (0.71) | 1.82 (0.34, 3.30) | ||
| change at 18 mo | 0.66 (1.22) | 1.44 (1.31) | 3.02 (1.26) | 1.71 (0.73) | 1.54 (0.03, 3.05) | ||
| change at 24 mo | 0.02 (1.18) | 2.08 (1.25) | 0.56 (1.25) | 0.182 | 0.87 (0.71) | 0.70 (−0.78, 2.17) | 0.040 |
| LDL-C (mg/dL) | |||||||
| Baseline | 118.03 (3.37) | 110.31 (3.91) | 110.60 (4.00) | 113.14 (2.17) | reference | ||
| change at 6 mo | −7.54 (2.54) | −3.47 (2.70) | −1.25 (2.71) | −4.15 (1.53) | −4.87 (−8.12, −1.62) | ||
| change at 12 mo | −5.40 (2.57) | −3.38 (2.70) | −2.62 (2.77) | −3.80 (1.55) | −4.52 (−7.80, −1.25) | ||
| change at 18 mo | −0.89 (2.64) | −2.08 (2.84) | 1.31 (2.74) | −0.44 (1.58) | −1.17 (−4.52, 2.18) | ||
| change at 24 mo | −8.35 (2.57) | −0.41 (2.72) | −6.42 (2.71) | 0.233 | −5.14 (1.54) | −5.87 (−9.14, −2.60) | 0.001 |
| HOMA-IR | |||||||
| Baseline | 4.18 (0.39) | 4.89 (0.55) | 4.44 (0.30) | 4.49 (0.25) | reference | ||
| change at 6 mo | 0.41 (0.49) | 0.05 (0.52) | 0.87 (0.53) | 0.44 (0.30) | 0.39 (−0.28, 1.05) | ||
| change at 12 mo | 1.40 (0.50) | 0.34 (0.52) | 1.31 (0.54) | 1.02 (0.30) | 0.97 (0.30, 1.64) | ||
| change at 18 mo | 1.28 (0.52) | 0.34 (0.56) | 1.50 (0.53) | 1.05 (0.31) | 1.00 (0.32, 1.69) | ||
| change at 24 mo | 2.41 (0.50) | 1.97 (0.53) | 2.20 (0.53) | 0.940 | 2.19 (0.30) | 2.14 (1.47, 2.81) | <0.001 |
| Female (n = 43) | Male (n = 67) | |||
|---|---|---|---|---|
| Baseline | Post (24 Months) | Baseline | Post (24 Months) | |
| BMI z score | 2.43 (0.08) | 2.39 (0.11) | 2.23 (0.06) | 2.16 (0.08) * |
| Body fat % | 41.83 (0.66) | 41.13 (0.72) | 41.95 (0.50) | 39.58 (0.75) *** |
| FMI | 11.38 (0.36) | 11.97 (0.47) *** | 12.02 (0.32) | 11.95 (0.38) |
| FFMI | 15.71 (0.32) | 16.77 (0.33) *** | 16.50 (0.28) | 17.94 (0.31) *** |
| AST (U/L) | 24.74 (2.67) | 23.88 (3.11) | 30.70 (2.52) | 23.09 (1.71) ** |
| ALT (U/L) | 26.81 (5.05) | 26.98 (5.26) | 42.10 (5.42) | 32.60 (3.81) |
| TG (mg/dL) | 120.58 (7.78) | 114.33 (7.82) | 110.06 (6.43) | 115.20 (7.87) |
| HDL (mg/dL) | 49.02 (1.76) | 52.09 (1.84) * | 49.72 (1.27) | 48.91 (1.41) |
| LDL (mg/dL) | 114.58 (2.82) | 114.42 (4.36) | 112.31 (2.85) | 102.78 (2.93) *** |
| HOMA-IR | 4.05 (0.24) | 6.67 (0.81) *** | 4.78 (0.37) | 6.57 (0.47) *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Woo, S.; Ju, Y.-S.; Seo, Y.-G.; Kim, Y.-M.; Lim, H.; Park, K.-H. Additive Effects of Exercise or Nutrition Intervention in a 24-Month Multidisciplinary Treatment with a Booster Intervention for Children and Adolescents with Overweight or Obesity: The ICAAN Study. Nutrients 2022, 14, 387. https://doi.org/10.3390/nu14020387
Woo S, Ju Y-S, Seo Y-G, Kim Y-M, Lim H, Park K-H. Additive Effects of Exercise or Nutrition Intervention in a 24-Month Multidisciplinary Treatment with a Booster Intervention for Children and Adolescents with Overweight or Obesity: The ICAAN Study. Nutrients. 2022; 14(2):387. https://doi.org/10.3390/nu14020387
Chicago/Turabian StyleWoo, Sarah, Young-Su Ju, Young-Gyun Seo, Yoon-Myung Kim, Hyunjung Lim, and Kyung-Hee Park. 2022. "Additive Effects of Exercise or Nutrition Intervention in a 24-Month Multidisciplinary Treatment with a Booster Intervention for Children and Adolescents with Overweight or Obesity: The ICAAN Study" Nutrients 14, no. 2: 387. https://doi.org/10.3390/nu14020387
APA StyleWoo, S., Ju, Y.-S., Seo, Y.-G., Kim, Y.-M., Lim, H., & Park, K.-H. (2022). Additive Effects of Exercise or Nutrition Intervention in a 24-Month Multidisciplinary Treatment with a Booster Intervention for Children and Adolescents with Overweight or Obesity: The ICAAN Study. Nutrients, 14(2), 387. https://doi.org/10.3390/nu14020387