
Threshold of Reactivity and Tolerance to Precautionary Allergen-Labelled Biscuits of Baked Milk- and Egg-Allergic Children

 ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Caseload and Methods
2.1. Patients
2.2. Study Design
2.3. Diagnostic Challenges
2.4. Milk/egg IgE Sensitization
2.5. Evaluation of the Clinical Tolerance to the Biscuits Labelled without Milk and Egg
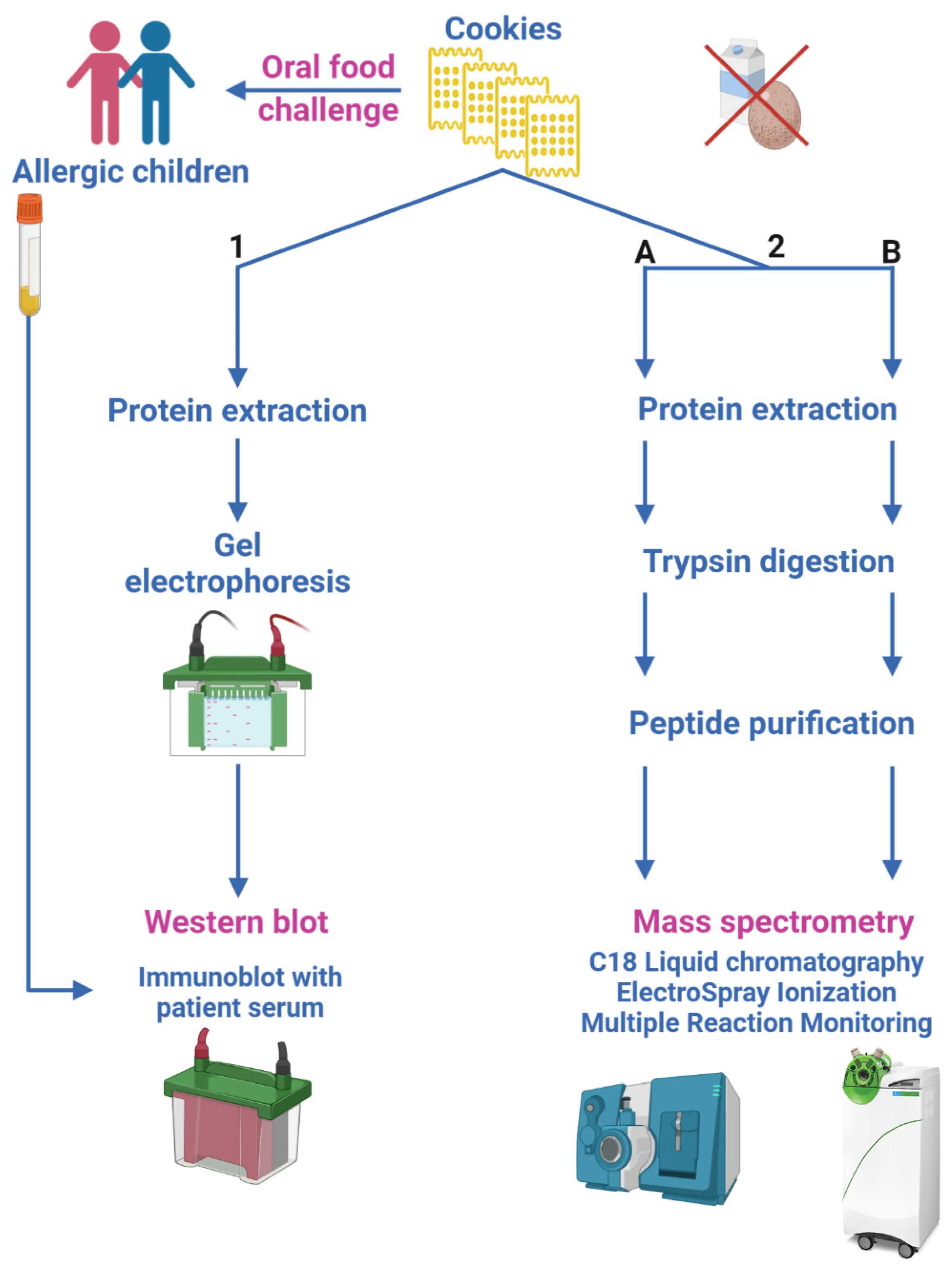
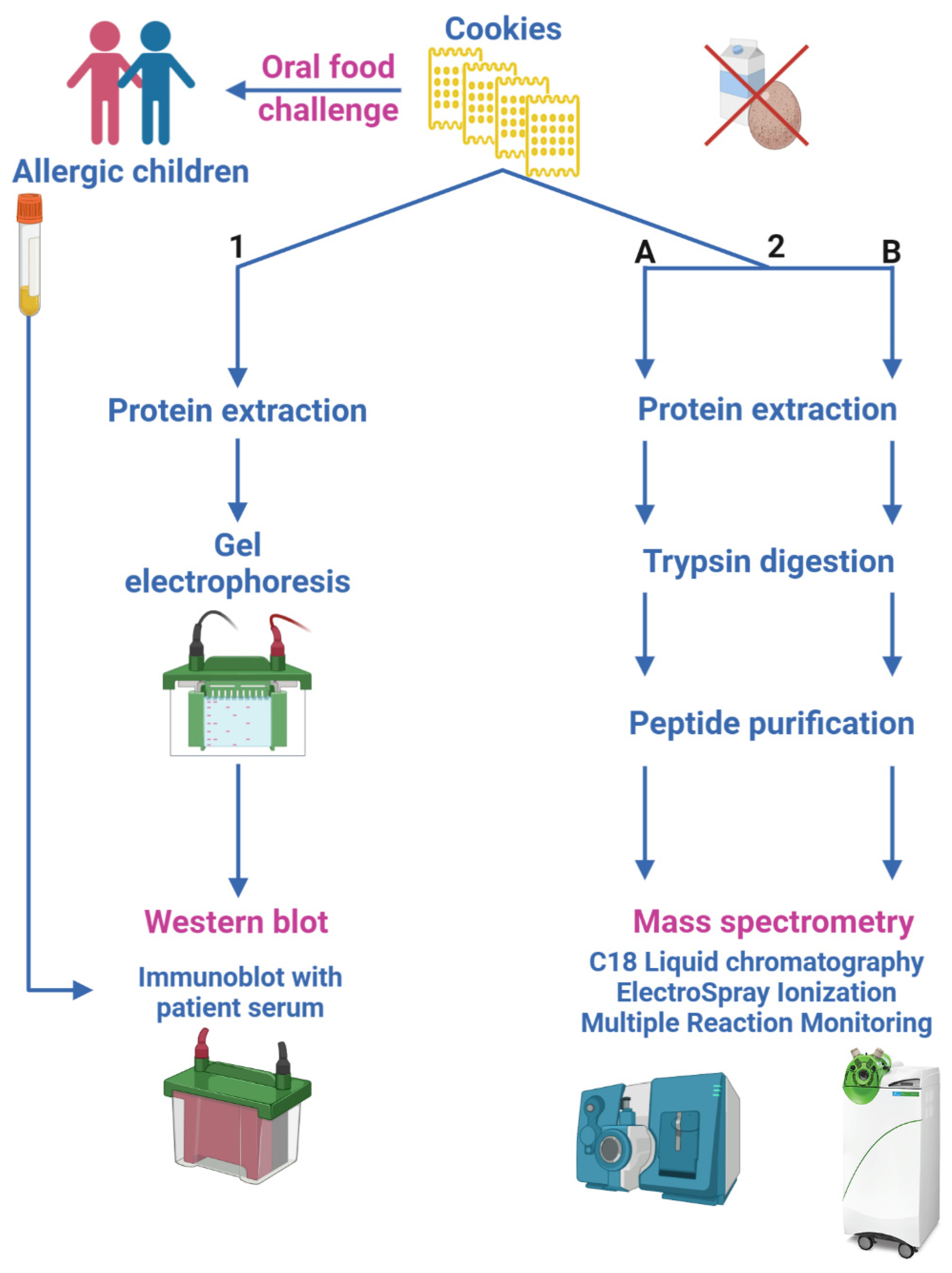
2.6. Evaluation of the Presence of Milk/Egg Traces in Biscuits Labelled without Milk and Egg
- immunoblot, to determine patient serum binding to egg and milk allergens possibly contained in tested biscuits (Section 2.6.1);
- two different LC-ESI-MS/MS methods, aimed at quantifying egg and milk allergens in biscuits by monitoring their marker peptides (Section 2.6.2).
2.6.1. Protein Extraction, Gel Electrophoresis Separation and Immunoblot Analysis
2.6.2. LC-ESI-MS/MS Analysis
2.7. Statistics
3. Results
3.1. Clinical Characteristics
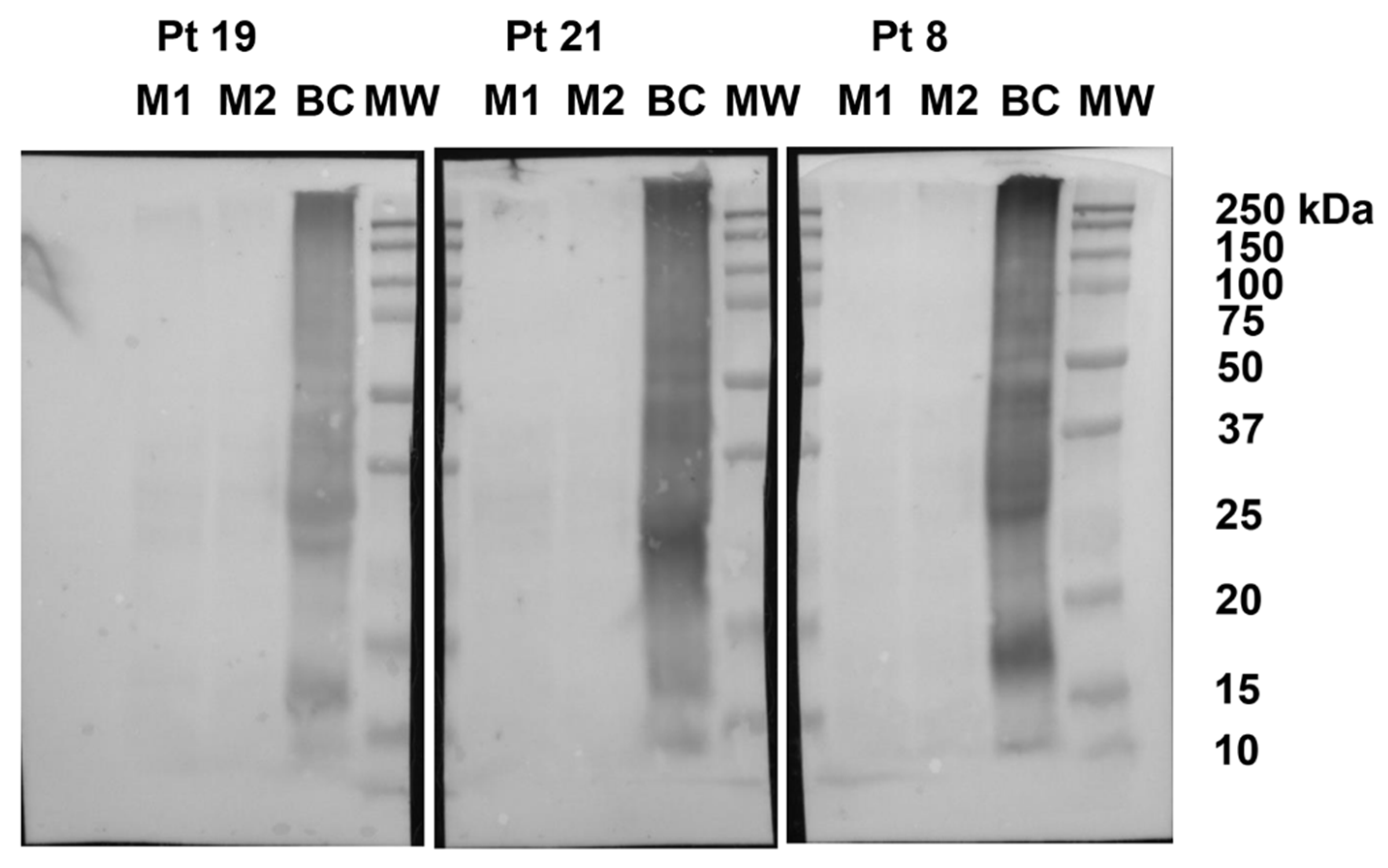
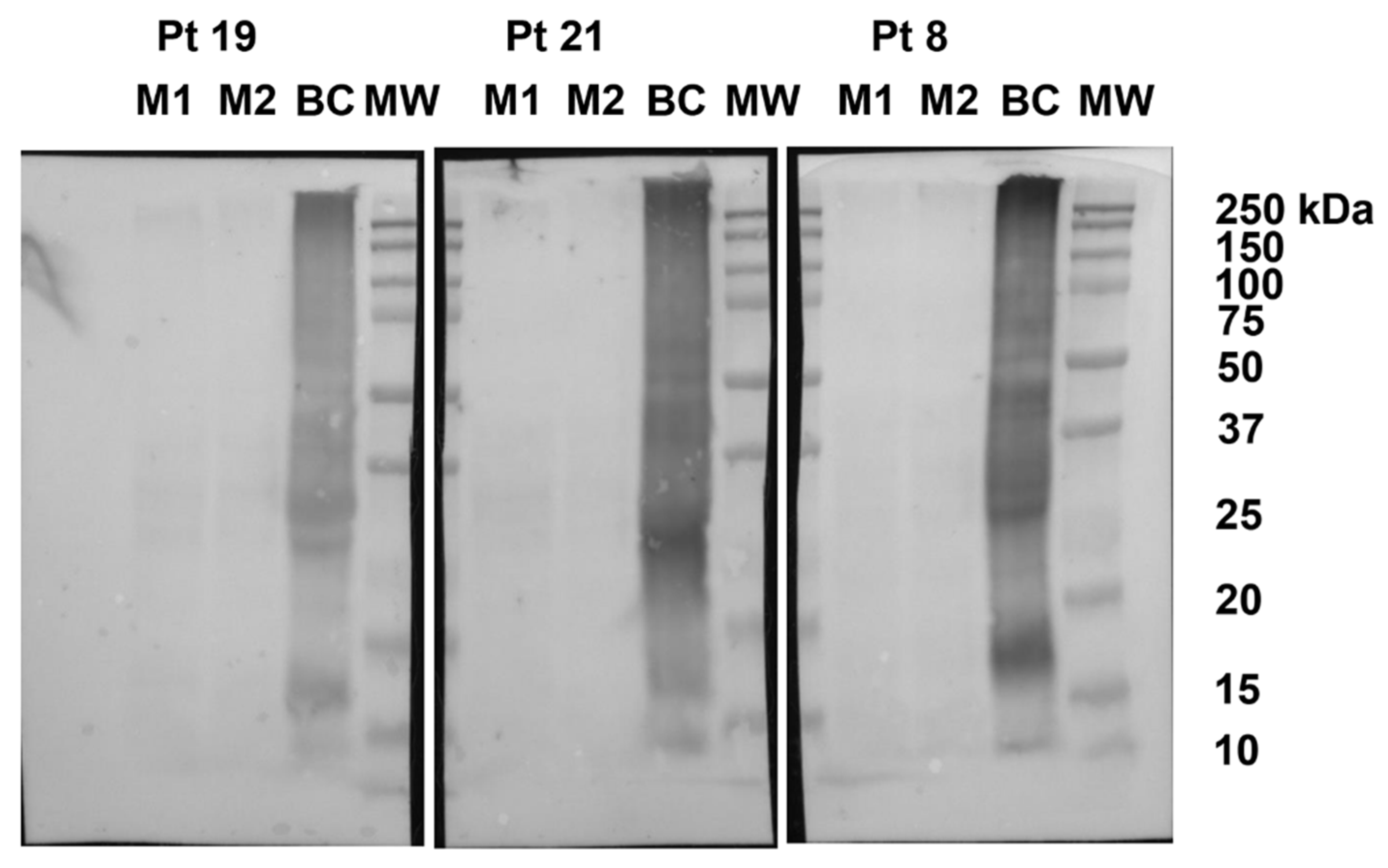
3.2. Determination of Patient Serum Binding to Egg and Milk Allergens Contained in Biscuits
3.3. Determination of Cow’s Milk and Hen’s Egg Allergen Levels in Commercial “Milk and Egg Free” Biscuits by Targeted Mass Spectrometry Methods
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roberts, G.; Allen, K.; Ballmer-Weber, B.; Clark, A.; Crevel, R.; Galvin, A.D.; Fernandez-Rivas, M.; Grimshaw, K.E.C.; Hourihane, J.O.; Poulsen, L.K.; et al. Identifying and managing patients at risk of severe allergic reactions to food: Report from two iFAAM workshops. Clin. Exp. Allergy 2019, 49, 1558–1566. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://Farrp.Unl.Edu/Documents/Regulatory/International_%20Allergens_061021.Pdf (accessed on 4 November 2021).
- Fierro, V.; Di Girolamo, F.; Marzano, V.; Dahdah, L.; Mennini, M. Food labeling issues in patients with severe food allergies: Solving a hamlet-like doubt. Curr. Opin. Allergy Clin. Immunol. 2017, 17, 204–211. [Google Scholar] [CrossRef]
- Allen, K.J.; Turner, P.J.; Pawankar, R.; Taylor, S.; Sicherer, S.; Lack, G.; Rosario, N.; Ebisawa, M.; Wong, G.; Mills, E.; et al. Precautionary labelling of foods for allergen content: Are we ready for a global framework? World Allergy Organ. J. 2014, 7, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, L.S.; Taylor, S.L.; Pacenza, R.; Niemann, L.M.; Lambrecht, D.M.; Sicherer, S.H. Food allergen advisory labeling and product contamination with egg, milk, and peanut. J. Allergy Clin. Immunol. 2010, 126, 384–385. [Google Scholar] [CrossRef] [PubMed]
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Food and Nutrition Board; Committee on Food Allergies. Global Burden, Causes, Treatment, Prevention, and Public Policy Finding a Path to Safety in Food Allergy: Assessment of the Global Burden, Causes, Prevention, Management, and Public Policy; Oria, M.P., Stallings, V.A., Eds.; National Academies Press: Washington, DC, USA, 2016. [Google Scholar]
- Allen, K.J.; Remington, B.; Baumert, J.L.; Crevel, R.W.; Houben, G.; Brooke-Taylor, S.; Kruizinga, A.G.; Taylor, S.L. Allergen reference doses for precautionary labeling (VITAL 2.0): Clinical implications. J. Allergy Clin. Immunol. 2014, 133, 156–164. [Google Scholar] [CrossRef]
- Remington, B.C.; Westerhout, J.; Meima, M.Y.; Blom, W.M.; Kruizinga, A.G.; Wheeler, M.W.; Taylor, S.L.; Houben, G.; Baumert, J.L. Updated population minimal eliciting dose distributions for use in risk assessment of 14 priority food allergens. Food Chem. Toxicol. 2020, 139, 111259. [Google Scholar] [CrossRef]
- Houben, G.F.; Baumert, J.L.; Blom, W.M.; Kruizinga, A.G.; Meima, M.Y.; Remington, B.C.; Wheeler, M.W.; Westerhout, J.; Taylor, S.L. Full range of population Eliciting Dose values for 14 priority allergenic foods and recommendations for use in risk characterization. Food Chem. Toxicol. 2020, 146, 111831. [Google Scholar] [CrossRef]
- Madsen, C.B.; Dungen, M.W.V.D.; Cochrane, S.; Houben, G.F.; Knibb, R.; Knulst, A.C.; Ronsmans, S.; Yarham, R.A.; Schnadt, S.; Turner, P.; et al. Can we define a level of protection for allergic consumers that everyone can accept? Regul. Toxicol. Pharmacol. 2020, 117, 104751. [Google Scholar] [CrossRef]
- Gruzelle, V.; Juchet, A.; Martin-Blondel, A.; Michelet, M.; Chabbert-Broue, A.; Didier, A. Benefits of baked milk oral immunotherapy in French children with cow’s milk allergy. Pediatr. Allergy Immunol. 2020, 31, 364–370. [Google Scholar] [CrossRef]
- Lemon-Mulé, H.; Sampson, H.A.; Sicherer, S.H.; Shreffler, W.G.; Noone, S.; Nowak-Wegrzyn, A. Immunologic changes in children with egg allergy ingesting extensively heated egg. J. Allergy Clin. Immunol. 2008, 122, 977–983.e1. [Google Scholar] [CrossRef]
- Remington, B.C.; Westerhout, J.; Campbell, D.E.; Turner, P.J. Minimal impact of extensive heating of hen’s egg and cow’s milk in a food matrix on threshold dose-distribution curves. Allergy 2017, 72, 1816–1819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grabenhenrich, L.B.; Reich, A.; Bellach, J.; Trendelenburg, V.; Sprikkelman, A.B.; Roberts, G.; Grimshaw, K.E.C.; Sigurdardottir, S.; Kowalski, M.L.; Papadopoulos, N.G.; et al. A new framework for the documentation and interpretation of oral food challenges in population-based and clinical research. Allergy 2016, 72, 453–461. [Google Scholar] [CrossRef] [Green Version]
- Nowak-Wegrzyn, A.; Assa’Ad, A.H.; Bahna, S.L.; Bock, S.A.; Sicherer, S.H.; Teuber, S.S. Work Group report: Oral food challenge testing. J. Allergy Clin. Immunol. 2009, 123, S365–S383. [Google Scholar] [CrossRef] [PubMed]
- Keil, T.; McBride, D.; Grimshaw, K.; Niggemann, B.; Xepapadaki, P.; Zannikos, K.; Sigurdardottir, S.T.; Clausen, M.; Reche, M.; Pascual, C.; et al. The multinational birth cohort of EuroPrevall: Background, aims and methods. Allergy 2010, 65, 482–490. [Google Scholar] [CrossRef]
- Grabenhenrich, L.B.; Reich, A.; McBride, D.; Sprikkelman, A.; Roberts, G.; Grimshaw, K.E.C.; Fiocchi, A.G.; Saxoni-Papageorgiou, P.; Papadopoulos, N.G.; Fiandor, A.; et al. Physician’s appraisal vs documented signs and symptoms in the interpretation of food challenge tests: The EuroPrevall birth cohort. Pediatr. Allergy Immunol. 2017, 29, 58–65. [Google Scholar] [CrossRef] [Green Version]
- Fiocchi, A.; Bouygue, G.R.; Restani, P.; Bonvini, G.; Startari, R.; Terracciano, L. Accuracy of skin prick tests in IgE-mediated adverse reactions to bovine proteins. Ann. Allergy Asthma Immunol. 2002, 89, 26–32. [Google Scholar] [CrossRef]
- Fiocchi, A.; Artesani, M.C.; Riccardi, C.; Mennini, M.; Pecora, V.; Fierro, V.; Calandrelli, V.; Dahdah, L.; Valluzzi, R.L. Impact of Omalizumab on Food Allergy in Patients Treated for Asthma: A Real-Life Study. J. Allergy Clin. Immunol. Pract. 2019, 7, 1901–1909.e5. [Google Scholar] [CrossRef]
- Monaci, L.; De Angelis, E.; Guagnano, R.; Ganci, A.; Garaguso, I.; Fiocchi, A.; Pilolli, R. Validation of a MS Based Proteomics Method for Milk and Egg Quantification in Cookies at the Lowest VITAL Levels: An Alternative to the Use of Precautionary Labeling. Foods 2020, 9, 1489. [Google Scholar] [CrossRef]
- Pilolli, R.; De Angelis, E.; Monaci, L. Streamlining the analytical workflow for multiplex MS/MS allergen detection in processed foods. Food Chem. 2017, 221, 1747–1753. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics. Committee on Nutrition Hypoallergenic Infant Formulas. Pediatrics 2000, 106, 346–349. [Google Scholar] [CrossRef] [Green Version]
- Agyemang, A.; Feuille, E.; Tang, J.; Steinwandtner, I.; Sampson, H.; Nowak-Węgrzyn, A. Outcomes of 84 consecutive open food challenges to extensively heated (baked) milk in the allergy office. J. Allergy Clin. Immunol. Pr. 2018, 6, 653–655.e2. [Google Scholar] [CrossRef]
- Mehr, S.; Turner, P.J.; Joshi, P.; Wong, M.; Campbell, D.E. Safety and clinical predictors of reacting to extensively heated cow’s milk challenge in cow’s milk-allergic children. Ann. Allergy Asthma Immunol. 2014, 113, 425–429. [Google Scholar] [CrossRef]
- Bartnikas, L.M.; Sheehan, W.J.; Hoffman, E.B.; Permaul, P.; Dioun, A.F.; Friedlander, J.; Baxi, S.N.; Schneider, L.C.; Phipatanakul, W. Predicting food challenge outcomes for baked milk: Role of specific IgE and skin prick testing. Ann. Allergy Asthma Immunol. 2012, 109, 309–313.e1. [Google Scholar] [CrossRef] [PubMed]
- Nowak-Wegrzyn, A.; Bloom, K.A.; Sicherer, S.H.; Shreffler, W.G.; Noone, S.; Wanich, N.; Sampson, H.A. Tolerance to extensively heated milk in children with cow’s milk allergy. J. Allergy Clin. Immunol. 2008, 122, 342–347.e2. [Google Scholar] [CrossRef]
- Taylor, S.L.; Hefle, S.L.; Bindslev-Jensen, C.; Bock, S.; Burks, A.; Christie, L.; Hill, D.J.; Host, A.; Hourihane, J.O.; Lack, G.; et al. Factors affecting the determination of threshold doses for allergenic foods: How much is too much? J. Allergy Clin. Immunol. 2002, 109, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Dahdah, L.; Ceccarelli, S.; Amendola, S.; Campagnano, P.; Cancrini, C.; Mazzina, O.; Fiocchi, A. IgE Immunoadsorption Knocks Down the Risk of Food-Related Anaphylaxis. Pediatrics 2015, 136, e1617–e1620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dantzer, J.A.; Dunlop, J.H.; Wood, R.A. Standard testing fails to identify patients who tolerate baked milk. J. Allergy Clin. Immunol. 2020, 146, 1434–1437.e2. [Google Scholar] [CrossRef]
- Putignani, L.; Dallapiccola, B. Foodomics as part of the host-microbiota-exposome interplay. J. Proteom. 2016, 147, 3–20. [Google Scholar] [CrossRef] [PubMed]
- Marzano, V.; Tilocca, B.; Fiocchi, A.G.; Vernocchi, P.; Mortera, S.L.; Urbani, A.; Roncada, P.; Putignani, L. Perusal of food allergens analysis by mass spectrometry-based proteomics. J. Proteom. 2020, 215, 103636. [Google Scholar] [CrossRef]
- Fiocchi, A.; Ebisawa, M. Severe food allergies: Can they be considered rare diseases? Curr. Opin. Allergy Clin. Immunol. 2017, 17, 201–203. [Google Scholar] [CrossRef]
- Arasi, S.; Nurmatov, U.; Turner, P.J.; Ansotegui, I.J.; Daher, S.; Dunn-Galvin, A.; Ebisawa, M.; Eigenmann, P.; Fernandez-Rivas, M.; Gupta, R.; et al. Consensus on DEfinition of Food Allergy SEverity (DEFASE): Protocol for a systematic review. World Allergy Organ. J. 2020, 13, 100493. [Google Scholar] [CrossRef] [PubMed]
- Arasi, S.; Nurmatov, U.; Dunn-Galvin, A.; Daher, S.; Roberts, G.; Turner, P.J.; Shinder, S.B.; Gupta, R.; Eigenmann, P.; Nowak-Wegrzyn, A.; et al. Consensus on DEfinition of Food Allergy SEverity (DEFASE) an integrated mixed methods systematic review. World Allergy Organ. J. 2021, 14, 100503. [Google Scholar] [CrossRef] [PubMed]
- Remington, B.C.; Westerhout, J.; Dubois, A.E.J.; Blom, W.M.; Kruizinga, A.G.; Taylor, S.L.; Houben, G.F.; Baumert, J.L. Suitability of low-dose, open food challenge data to supplement double-blind, placebo-controlled data in generation of food allergen threshold dose distributions. Clin. Exp. Allergy 2021, 51, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Holzhauser, T.; Johnson, P.; Hindley, J.P.; O’Connor, G.; Chan, C.-H.; Costa, J.; Fæste, C.K.; Hirst, B.J.; Lambertini, F.; Miani, M.; et al. Are current analytical methods suitable to verify VITAL® 2.0/3.0 allergen reference doses for EU allergens in foods? Food Chem. Toxicol. 2020, 145, 111709. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Ingredient | Quantity |
|---|---|
| Type 2 soft wheat flour | 63% |
| Sugar | |
| Cereal flour | 10% (corn 5%, barley 5%, on the finished product) |
| High oleic sunflower oil | 10% |
| Honey | |
| Barley malt and corn extract | |
| Raising agents | ammonium acid carbonate, disodium diphosphate, sodium hydrogen carbonate |
| Whole sea salt | 0.5% |
| Emulsifier | |
| Aromas | |
| Allergy warning | The recipe does not contain milk and eggs. It cannot be excluded that any traces of these allergens are present, in any case less than 5 mg/kg. The product can also contain soy, hazelnuts and other nuts; therefore, it is not suitable for consumption by people allergic to these substances. |
| sIgE > 0.35 kUI/L | c-SPT > 3 mm | ffSPT > 3 mm | ||||
|---|---|---|---|---|---|---|
| # | # | # | ||||
| Milk | 23 | 48.4 ± 39.7 | 24 | 10.3 ± 5.3 | 25 | 11.4 ± 4.5 |
| Casein | 19 | 49.1 ± 45.4 | 15 | 9.7 ± 4.9 | ||
| Egg white | 15 | 27.1 ± 46.2 | 19 | 7.6 ± 2.5 | 15 | 7.0 ± 2.2 |
| Egg yolk | 9 | 32.4 ± 45.2 | 14 | 9.0 ± 3.5 | 10 | 8.0 ± 1.2 |
| Baked milk biscuit (Plasmon) | 21 | 7.2 ± 3.8 | ||||
| Baked egg biscuit (Pavesini) | 11 | 4.7 ± 1.2 | ||||
| Magretti-Frollini con orzo e mais biscuit | 0 | |||||
| Allergen | Protein | Quantifier Peptide (m/z) | Product ion (m/z) | LOD µg tot protein/g matrix | R2 | Route |
|---|---|---|---|---|---|---|
| Milk | α-S1-Casein Bos d9 | 634.4 (YLG) | 991.6 | 0.63 | 0.99 | 2.A (QTrap 6500+) |
| 692.9 (FFV) | 991.4 | 0.10 | 0.99 | 2.B (QSight 220) | ||
| Egg | Ovalbumin Gal d2 | 844.4 (GGL) | 666.3 | 0.61 | 0.98 | 2.A (QTrap 6500+) |
| 592.1 (ISQ) | 858.9 | 0.30 | 0.99 | 2.B (QSight 220) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fierro, V.; Marzano, V.; Monaci, L.; Vernocchi, P.; Mennini, M.; Valluzzi, R.; Levi Mortera, S.; Pilolli, R.; Dahdah, L.; Calandrelli, V.; et al. Threshold of Reactivity and Tolerance to Precautionary Allergen-Labelled Biscuits of Baked Milk- and Egg-Allergic Children. Nutrients 2021, 13, 4540. https://doi.org/10.3390/nu13124540
Fierro V, Marzano V, Monaci L, Vernocchi P, Mennini M, Valluzzi R, Levi Mortera S, Pilolli R, Dahdah L, Calandrelli V, et al. Threshold of Reactivity and Tolerance to Precautionary Allergen-Labelled Biscuits of Baked Milk- and Egg-Allergic Children. Nutrients. 2021; 13(12):4540. https://doi.org/10.3390/nu13124540
Chicago/Turabian StyleFierro, Vincenzo, Valeria Marzano, Linda Monaci, Pamela Vernocchi, Maurizio Mennini, Rocco Valluzzi, Stefano Levi Mortera, Rosa Pilolli, Lamia Dahdah, Veronica Calandrelli, and et al. 2021. "Threshold of Reactivity and Tolerance to Precautionary Allergen-Labelled Biscuits of Baked Milk- and Egg-Allergic Children" Nutrients 13, no. 12: 4540. https://doi.org/10.3390/nu13124540
APA StyleFierro, V., Marzano, V., Monaci, L., Vernocchi, P., Mennini, M., Valluzzi, R., Levi Mortera, S., Pilolli, R., Dahdah, L., Calandrelli, V., Bracaglia, G., Arasi, S., Riccardi, C., Fiocchi, A., & Putignani, L. (2021). Threshold of Reactivity and Tolerance to Precautionary Allergen-Labelled Biscuits of Baked Milk- and Egg-Allergic Children. Nutrients, 13(12), 4540. https://doi.org/10.3390/nu13124540