

The Problem of Vitamin D Scarcity: Cultural and Genetic Solutions by Indigenous Arctic and Tropical Peoples

{kind=link}
Abstract
1. Introduction
- The Arctic, where sunlight is weak in summer and absent in winter. The skin thus receives little of the solar UVB that helps produce vitamin D. This is the environment of people indigenous to the North American and Eurasian Arctic, notably the Aleut, the Inuit (Eskimos), the Sámi (Lapps), the Samoyeds, the Khanty-Mansi, the Yakuts, the Yukaghir, the Tungus, the Koryaks, and the Chukchi.
- The Tropics, where intense sunlight has favored the survival of individuals with highly melanized skin that blocks UVB. This is notably the environment of people indigenous to sub-Saharan Africa, southern India, Australia, Papua New Guinea, and Melanesia.
2. Vitamin D Scarcity in Arctic Peoples
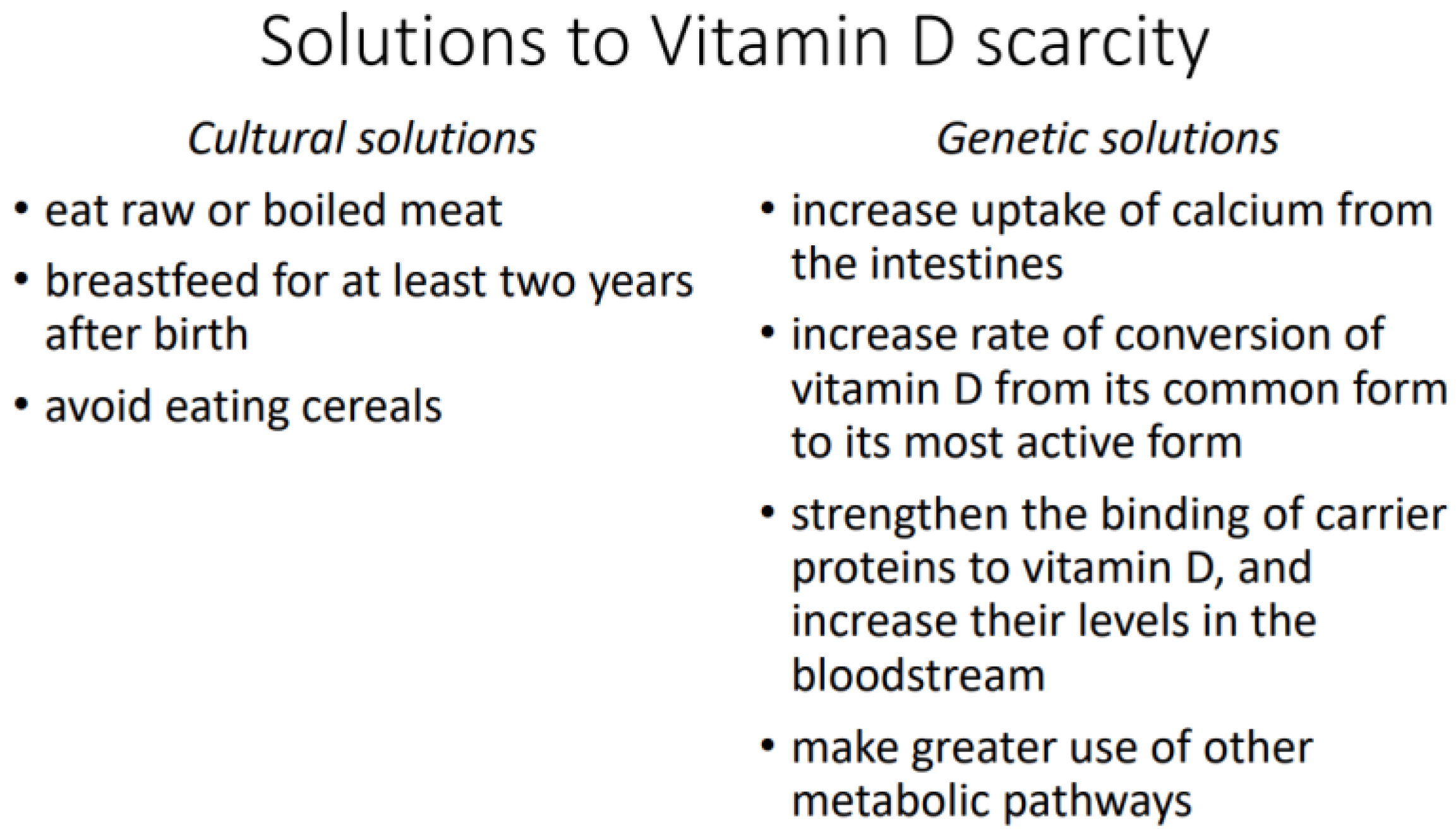
2.1. Cultural Solutions
2.1.1. Consumption of Raw or Boiled Meat
2.1.2. Extended Breastfeeding
“Babies are wholly breast-fed until the end of the 2nd year when meat is added to their diet. Children often nurse irregularly until the age of 4 or 6”.[11] (p. 463)
“Among these primitive, carnivorous people there is neither scurvy nor rickets. Children are nursed for four and not infrequently six years”.[20] (p. 1560)
“The reason, however, for the failure to find rickets at the above-mentioned places appears to be that infants are nursed for as much as two years and more, and the fact that the vitamin D content of seal oil is equal to that of the best cod-liver oil. According to Dr. Urquhart, infants are nursed for very long periods of time amongst the Western Arctic Eskimos also”.[21] (p. 494)
2.1.3. No Consumption of Cereals
2.2. Genetic Solutions
2.2.1. Higher Calcium Uptake
2.2.2. Higher Rate of Conversion
2.2.3. Stronger Binding by Carrier Proteins
3. Vitamin D Scarcity in Tropical Peoples
3.1. Cultural Solutions
3.2. Genetic Solutions
3.2.1. Higher Rate of Conversion
3.2.2. Greater Use of Alternative Metabolic Pathways
4. Discussion
- The total mortality rate is about 50% greater among men whose 25(OH)D levels are lower than 46 nmol/L or higher than 98 nmol/L [60];
- For endometrial, esophageal, gastric, kidney, non-Hodgkin’s lymphoma, pancreatic, and ovarian cancer, the mortality rate is significantly greater at levels lower than 45 nmol/L or higher than 124 nmol/L [63];
- The risk of pancreatic cancer is significantly greater at levels higher than 100 nmol/L [64];
- The risk of cardiovascular disease is significantly greater at levels lower than 50 nmol/L or higher than 62.5 nmol/L, and the mortality rate for all causes is significantly greater at levels higher than 122.5 nmol/L [65].
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Jiang, X.; Kiel, D.P.; Kraft, P. The genetics of vitamin D. Bone 2019, 126, 59–77. [Google Scholar] [CrossRef]
- Jiang, X.; O’Reilly, P.F.; Aschard, H.; Hsu, Y.H.; Richards, J.B.; Dupuis, J.; Ingelsson, E.; Karasik, D.; Pilz, S.; Berry, D.; et al. Genome-wide association study in 79,366 European-ancestry individuals informs the genetic architecture of 25-hydroxyvitamin D levels. Nat. Commun. 2018, 9, 260. [Google Scholar] [CrossRef]
- Harpending, H.; Cochran, G. In our genes. Proc. Natl. Acad. Sci. USA 2002, 99, 10–12. [Google Scholar] [CrossRef]
- Acerbi, A.; Enquist, M.; Ghirlanda, S. Cultural evolution and individual development of openness and conservatism. Proc. Natl. Acad. Sci. USA 2009, 106, 18931–18935. [Google Scholar] [CrossRef]
- Kolahdooz, F.; Barr, A.; Roache, C.; Sheehy, T.; Corriveau, A.; Sharma, S. Dietary adequacy of vitamin D and calcium among Inuit and Inuvialuit women of child-bearing age in Arctic Canada: A growing concern. PLoS ONE 2013, 8, e78987. [Google Scholar] [CrossRef]
- Dunnigan, M.G.; Henderson, J.B.; Hole, D.J.; Mawer, E.B.; Berry, J.L. Meat Consumption Reduces the Risk of Nutritional Rickets and Osteomalacia. Br. J. Nutr. 2005, 94, 983–991. [Google Scholar] [CrossRef]
- Mellanby, E. The part played by an ‘accessory factor’ in the production of experimental rickets. Proc. Physiol. Soc. 1918, 52, xi–xii. [Google Scholar]
- Draper, H.H. The Aboriginal Eskimo Diet in Modern Perspective. Am. Anthropol. 1977, 79, 309–316. [Google Scholar] [CrossRef]
- Geraci, J.R.; Smith, T.G. Vitamin C in the Diet of Inuit Hunters from Holman, Northwest Territories. Arctic 1979, 32, 135–139. [Google Scholar] [CrossRef][Green Version]
- Sinclair, H. The Diet of Canadian Indians and Eskimos. Proc. Nutr. Soc. 1953, 12, 69–82. [Google Scholar] [CrossRef]
- Heinbecker, P. Studies on the metabolism of Eskimos. J. Biol. Chem. 1928, 80, 461–475. [Google Scholar] [CrossRef]
- Reclus, E. Studies in Comparative Ethnology. In Primitive Folk; Walter Scott: London, UK, 1891. [Google Scholar]
- Taylor, J.G. Did the First Eskimos Speak Algonquian? Papers of the Ninth Algonquian Conference; Carleton University: Ottawa, ON, Canada, 1978; Volume 9. [Google Scholar]
- Jackson, F.G.; Montefiore, A. Notes on the Samoyads of the Great Tundra. J. R. Anthropol. Inst. 1895, 24, 388–410. [Google Scholar] [CrossRef]
- Clifford, W.M. The effect of cooking on the digestibility of meat. Biochem. J. 1930, 24, 1728–1733. [Google Scholar] [CrossRef] [PubMed]
- Searles, E. Inuit identity in the Canadian Arctic. Ethnology 2008, 47, 239–255. [Google Scholar]
- Kane, E.K. Arctic Explorations: The Second Grinnell Expedition in Search of Sir John Franklin, 1853, ’54, ’55; Thomas Nelson and Sons: London, UK, 1861. [Google Scholar]
- Lönnerdal, B. Nutritional and Physiologic Significance of Human Milk Proteins. Am. J. Clin. Nutr. 2003, 77, 1537S–1543S. [Google Scholar] [CrossRef]
- Kent, J.C.; Arthur, P.G.; Mitoulas, L.R.; Hartmann, P.E. Why calcium in breastmilk is independent of maternal dietary calcium and vitamin D. Breastfeed. Rev. 2009, 17, 5–11. [Google Scholar]
- Thomas, W.A. Health of a Carnivorous Race. A Study of the Eskimo. J. Amer. Med. Assoc. 1927, 88, 1559–1560. [Google Scholar] [CrossRef]
- Rabinowitch, I.M. Clinical and Other Observations on Canadian Eskimos in the Eastern Arctic. Can. Med. Assoc. J. 1936, 34, 487–501. [Google Scholar]
- Schehk, E. Untersuchungen über die Rachitishaufigkeit bei Lapplandern (Incidence of rickets in Lapland). Münchener Med. Wochenschr. 1936, 88, 1395–1396. [Google Scholar]
- Kerezsi, A. Ethnic characteristics of the Trom-yogan Khanty. In The Man Who Sees: The World of Ivan Stepanovich Sopochin, 1st ed.; Studies in Native Religion; Clive, T., Ed.; Molnar & Kelemen: Budapest, Hungary, 2021; Volume 2, pp. 109–214. [Google Scholar]
- Harris, A. Palaeodiet and Infant Feeding in Coastal Arctic Settlements. Insights from stable isotope analysis of bone and dentine collagen and amino acids. In Theses and Papers in Scientific Archaeology 18; University of York/Stockholm University: Stockholm, Sweden, 2020. [Google Scholar]
- Harrison, D.C.; Mellanby, E. Phytic acid and the rickets-producing action of cereals. Biochem. J. 1939, 33, 1660–1680. [Google Scholar] [CrossRef]
- McCance, R.A.; Widdowson, E.M. Mineral metabolism of healthy adults on white and brown bread dietaries. J. Physiol. 1942, 101, 44–85. [Google Scholar] [CrossRef] [PubMed]
- McCance, R.A.; Widdowson, E.M. Mineral metabolism on dephytinized bread. J. Physiol. 1942, 101, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Wills, M.R.; Phillips, J.B.; Day, R.C.; Bateman, E.C. Phytic acid and nutritional rickets in immigrants. Lancet 1972, 299, 771–773. [Google Scholar] [CrossRef]
- Sellers, E.A.C.; Sharma, A.; Rodd, C. Adaptation of Inuit children to a low-calcium diet. Can. Med. Assoc. J. 2003, 168, 1141–1143. [Google Scholar]
- Waiters, B.; Godel, J.C.; Basu, T.K. Perinatal Vitamin D and Calcium Status of Northern Canadian Mothers and their Newborn Infants. J. Am. Coll. Nutr. 1999, 18, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Perry, H.M.; Bernard, M.; Horowitz, M.; Miller, D.K.; Fleming, S.; Baker, M.Z.; Flaherty, J.; Purushothaman, R.; Hajjar, R.; Kaiser, F.E.; et al. The Effect of Aging on Bone Mineral Metabolism and Bone Mass in Native American Women. J. Am. Geriatr. Soc. 1998, 46, 1418–1422. [Google Scholar] [CrossRef]
- Barrett-Connor, E.; Siris, E.S.; Wehren, L.E.; Miller, P.D.; Abbott, T.A.; Berger, M.L.; Santora, A.C.; Sherwood, L.M. Osteoporosis and Fracture Risk in Women of Different Ethnic Groups. J. Bone Miner. Res. 2005, 20, 185–194. [Google Scholar] [CrossRef]
- Rejnmark, L.; Jørgensen, M.E.; Pedersen, M.B.; Hansen, J.C.; Heickendorff, L.; Lauridsen, A.L.; Mulvad, G.; Siggaard, C.; Skjoldborg, H.; Sørensen, T.B.; et al. Vitamin D insufficiency in Greenlanders on a Westernized fare: Ethnic differences in calcitropic hormones between Greenlanders and Danes. Calcif. Tissue Int. 2004, 74, 255–263. [Google Scholar] [CrossRef]
- Malyarchuk, B.A. Polymorphism of GC gene, encoding vitamin D binding protein, in aboriginal populations of Siberia. Ecol. Genet. 2020, 18, 243–250. [Google Scholar] [CrossRef]
- Larcombe, L.; Mookherjee, N.; Slater, J.; Slivinski, C.; Singer, M.; Whaley, C.; Denechezhe, L.; Matyas, S.; Turner-Brannen, E.; Nickerson, P.; et al. Vitamin D in a Northern Canadian First Nation Population: Dietary Intake, Serum Concentrations and Functional Gene Polymorphisms. PLoS ONE 2012, 7, e49872. [Google Scholar] [CrossRef]
- Khrunin, A.V.; Khvorykh, G.V.; Fedorov, A.N.; Limborska, S.A. Genomic landscape of the signals of positive natural selection in populations of Northern Eurasia: A view from Northern Russia. PLoS ONE 2020, 15, e0228778. [Google Scholar] [CrossRef] [PubMed]
- Signorello, L.B.; Williams, S.M.; Zheng, W.; Smith, J.R.; Long, J.; Cai, Q.; Hargreaves, M.K.; Hollis, B.W.; Blot, W.J. Blood vitamin D levels in relation to genetic estimation of African ancestry. Cancer Epidem. Biomar. 2010, 19, 2325–2331. [Google Scholar] [CrossRef] [PubMed]
- Harris, S.S. Vitamin D and African Americans. J. Nutr. 2006, 136, 1126–1129. [Google Scholar] [CrossRef] [PubMed]
- Harinarayan, C.V.; Ramalakshmi, T.; Prasad, U.V.; Sudhakar, D.; Srinivasarao, P.V.L.N.; Sarma, K.V.S.; Kumar, E.G.T. High prevalence of low dietary calcium, high phytate consumption, and vitamin D deficiency in healthy south Indians. Am. J. Clin. Nutr. 2007, 85, 1062–1067. [Google Scholar] [CrossRef] [PubMed]
- Goswami, R.; Kochupillai, N.; Gupta, N.; Goswami, D.; Singh, N.; Dudha, A. Presence of 25(OH) D deficiency in a rural North Indian village despite abundant sunshine. J. Assoc. Physicians India 2008, 56, 755–757. [Google Scholar]
- Hamilton, B.; Grantham, J.; Racinais, S.; Chalabi, H. Vitamin D deficiency is endemic in Middle Eastern sportsmen. Public Health Nutr. 2020, 13, 1528–1534. [Google Scholar] [CrossRef]
- Sedrani, S.H. Low 25-hydroxyvitamin D and normal serum calcium concentrations in Saudi Arabia: Riyadh region. Ann. Nutr. Metab. 1984, 28, 181–185. [Google Scholar] [CrossRef]
- Hagenau, T.; Vest, R.; Gissel, T.N.; Poulsen, C.S.; Erlandsen, M.; Mosekilde, L.; Vestergaard, P. Global vitamin D levels in relation to age, gender, skin pigmentation and latitude: An ecologic meta-regression analysis. Osteoporos. Int. 2009, 20, 133–140. [Google Scholar] [CrossRef]
- Jones, W.O. The Food and Agricultural Economies of Tropical Africa: A Summary View; Food Research Institute Studies; Stanford University, Food Research Institute: Stanford, CA, USA, 1961; Volume 2, pp. 1–18. [Google Scholar] [CrossRef]
- Léder, I. Sorghum and Millets. In Cultivated Plants, Primarily as Food Sources; UNESCO: Oxford, UK, 2004; Volume 1, pp. 66–84. [Google Scholar]
- Parsons, R.T. Religion in an African Society; E.J. Brill: Leiden, The Netherlands, 1964. [Google Scholar]
- Altman, I.; Chemers, M.M. Culture and Environment; Brooks/Cole: Monterey, CA, USA, 1984. [Google Scholar]
- Robins, A.H. The evolution of light skin color: Role of vitamin D disputed. Am. J. Phys. Anthropol. 2009, 139, 447–450. [Google Scholar] [CrossRef]
- Bryant, R.J.; Wastney, M.E.; Martin, B.R.; Wood, O.; McCabe, G.P.; Morshidi, M.; Smith, D.L.; Peacock, M.; Weaver, C.M. Racial differences in bone turnover and calcium metabolism in adolescent females. J. Clin. Endocr. Metab. 2003, 88, 1043–1047. [Google Scholar] [CrossRef]
- McGillivray, G.; Skull, S.A.; Davie, G.; Kofoed, S.E.; Frydenberg, A.; Rice, J.; Cooke, R.; Carapetis, J.R. High prevalence of asymptomatic vitamin-D and iron deficiency in East African immigrant children and adolescents living in a temperate climate. Arch. Dis. Child. 2007, 92, 1088–1093. [Google Scholar] [CrossRef] [PubMed]
- Hearney, R.P. Ethnicity, bone status, and the calcium requirement. Nutr. Res. 2002, 22, 153–178. [Google Scholar] [CrossRef]
- Hannan, M.T.; Litman, H.J.; Araujo, A.B.; McLennan, C.E.; McLean, R.R.; McKinlay, J.B.; Chen, T.C.; Holick, M.F. Serum 25-hydroxyvitamin D and bone mineral density in a racially and ethnically diverse group of men. J. Clin. Endocrinol. Metab. 2008, 93, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Freedman, B.I.; Wagenknecht, L.E.; Hairston, K.G.; Bowden, D.W.; Carr, J.J.; Hightower, R.C.; Gordon, E.J.; Xu, J.; Langefeld, C.D.; Divers, J. Vitamin D, adiposity, and calcified atherosclerotic plaque in African-Americans. J. Clin. Endocr. Metab. 2010, 95, 1076–1083. [Google Scholar] [CrossRef] [PubMed]
- Aloia, J.F.; Talwar, S.A.; Pollack, S.; Yeh, J. A randomized controlled trial of vitamin D3 supplementation in African American women. Arch. Intern. Med. 2005, 165, 1618–1623. [Google Scholar] [CrossRef]
- Matsuoka, L.Y.; Wortsman, J.; Haddad, J.G.; Kolm, P.; Hollis, B.W. Racial pigmentation and the cutaneous synthesis of vitamin D. Arch. Dermatol. 1991, 127, 536–538. [Google Scholar] [CrossRef]
- Matsuoka, L.Y.; Wortsman, J.; Chen, T.C.; Holick, M.F. Compensation for the interracial variance in the cutaneous synthesis of vitamin D. J. Lab. Clin. Med. 1995, 126, 452–457. [Google Scholar]
- Lips, P. Interaction between Vitamin D and calcium. Scand. J. Clin. Lab. Investig. 2012, 72, 60–64. [Google Scholar] [CrossRef]
- Lee, D.B.; Hardwick, L.L.; Hu, M.S.; Jamgotchian, N. Vitamin D-independent regulation of calcium and phosphate absorption. Miner. Electrolyte Metab. 1990, 16, 167–173. [Google Scholar]
- Zhang, J.; Zhang, Z.; Yu, A. Discussion on the mechanism of the calcium absorption in the human body. Chin. Sci. Bull. 2001, 46, 1403–1408. [Google Scholar] [CrossRef]
- Michaëlsson, K.; Baron, J.A.; Snellman, G.; Gedeborg, R.; Byberg, L.; Sundström, J.; Berglund, L.; Ärnlöv, J.; Hellman, P.; Blomhoff, R.; et al. Plasma vitamin D and mortality in older men: A community-based prospective cohort study. Am. J. Clin. Nutr. 2010, 92, 841–848. [Google Scholar] [CrossRef]
- Tuohimaa, P. Vitamin D and aging. J. Steroid Biochem. Mol. Biol. 2009, 114, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Tuohimaa, P.; Keisala, T.; Minasyan, A.; Cachat, J.; Kalueff, A. Vitamin D, nervous system and aging. Psychoneuroendocrinology 2009, 34S, S278–S286. [Google Scholar] [CrossRef] [PubMed]
- Helzlsouer, K.J.; Steering Committee of Vitamin D Pooling Project of Rarer Cancers. Abstract PL04-05: Vitamin D: Panacea or a Pandora’s box for prevention? Cancer Prev. Res. 2010, 3, PL04–PL05. [Google Scholar] [CrossRef]
- Stolzenberg-Solomon, R.Z.; Jacobs, E.J.; Arslan, A.A.; Qi, D.; Patel, A.V.; Helzlsouer, K.J.; Weinstein, S.J.; McCullough, M.L.; Purdue, M.P.; Shu, X.O.; et al. Circulating 25-hydroxyvitamin D and risk of pancreatic cancer, Cohort Consortium Vitamin D Pooling Project of Rarer Cancers. Am. J. Epidemiol. 2010, 172, 81–93. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.D. Vitamin D and health: Can too much be harmful? Am. J. Lifestyle Med. 2009, 3, 407–408. [Google Scholar] [CrossRef]
- Lam, V.; Takechi, R.; Mamo, J.C. Vitamin D, Cerebrocapillary Integrity and Cognition in Murine Model of Accelerated Ageing. Alzheimer′s Dement. 2017, 13, P1304. [Google Scholar] [CrossRef]
- Huang, S.-J.; Wang, X.-H.; Liu, Z.-D.; Cao, W.-L.; Han, Y.; Ma, A.-G.; Xu, S.-F. Vitamin D deficiency and the risk of tuberculosis: A meta-analysis. Drug Des. Dev. Ther. 2016, 11, 91–102. [Google Scholar] [CrossRef]
- Power, C.E.; Evans, M.K.; Wenger, J.; Zonderman, A.B.; Berg, A.H.; Nalls, M.; Tamex, H.; Zhang, D.; Bhan, I.; Karumanchi, S.A. Vitamin D-Binding Protein and Vitamin D Status of Black Americans and White Americans. N. Engl. J. Med. 2013, 369, 1991–2000. [Google Scholar] [CrossRef]
- Hilliard, C. Is an Unacknowledged Eurocentric Paradigm Widening Ethnic Disparities in U.S. Health Care? African-American Health. 20 August 2015. Available online: https://african-americanhealth.blogspot.com/2014/11/is-unacknowledged-eurocentric-paradigm.html (accessed on 29 August 2022).
- Frost, P. Black-White differences in cancer risk and the vitamin-D hypothesis. J. Natl. Med. Assoc. 2009, 101, 1310–1313. [Google Scholar] [CrossRef]
- Frost, P. Vitamin D deficiency among northern Native Peoples: A real or apparent problem? Int. J. Circumpolar Health 2012, 71, 18001. [Google Scholar] [CrossRef]
- Frost, P. To supplement or not to supplement: Are Inuit getting enough vitamin D? Études Inuit Stud. 2018, 40, 271–291. [Google Scholar] [CrossRef]
- Larcombe, L.; Mookherjee, N.; Slater, J.; Slivinski, C.; Dantouze, J.; Singer, M.; Whaley, C.; Denechezhe, L.; Matyas, S.; Decter, K.; et al. Vitamin D, serum 25(OH)D, LL-37 and polymorphisms in a Canadian First Nation population with endemic tuberculosis. Int. J. Circumpolar Health 2017, 74, 28952. [Google Scholar] [CrossRef]
- Sharma, L.K.; Dutta, D.; Sharma, N.; Gadpayle, A.K. The increasing problem of subclinical and overt hypervitaminosis D in India: An institutional experience and review. Nutrition 2017, 34, 76–81. [Google Scholar] [CrossRef]
- Nielsen, N.O.; Skifte, T.; Andersson, M.; Wohlfahrt, J.; Søborg, B.; Koch, A.; Melbye, M.; Ladefoged, K. Both high and low serum vitamin D concentrations are associated with tuberculosis: A case–control study in Greenland. Brit. J. Nutr. 2010, 104, 1487–1491. [Google Scholar] [CrossRef]
- Bosch, E.; Calafell, F.; Rosser, Z.H.; Nørby, S.; Lynnerup, N.; Hurles, M.E.; Jobling, M.A. High level of male-biased Scandinavian admixture in Greenlandic Inuit shown by Y-chromosomal analysis. Hum. Genet. 2003, 112, 353–363. [Google Scholar] [CrossRef]
- Ford, J.D.; Macdonald, J.P.; Huet, C.; Statham, S.; MacRury, A. Food policy in the Canadian North: Is there a role for country food markets? Soc. Sci. Med. 2016, 152, 35–40. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frost, P. The Problem of Vitamin D Scarcity: Cultural and Genetic Solutions by Indigenous Arctic and Tropical Peoples. Nutrients 2022, 14, 4071. https://doi.org/10.3390/nu14194071
Frost P. The Problem of Vitamin D Scarcity: Cultural and Genetic Solutions by Indigenous Arctic and Tropical Peoples. Nutrients. 2022; 14(19):4071. https://doi.org/10.3390/nu14194071
Chicago/Turabian StyleFrost, Peter. 2022. "The Problem of Vitamin D Scarcity: Cultural and Genetic Solutions by Indigenous Arctic and Tropical Peoples" Nutrients 14, no. 19: 4071. https://doi.org/10.3390/nu14194071
APA StyleFrost, P. (2022). The Problem of Vitamin D Scarcity: Cultural and Genetic Solutions by Indigenous Arctic and Tropical Peoples. Nutrients, 14(19), 4071. https://doi.org/10.3390/nu14194071