
Ketoanalogues Supplemental Low Protein Diet Safely Decreases Short-Term Risk of Dialysis among CKD Stage 4 Patients
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
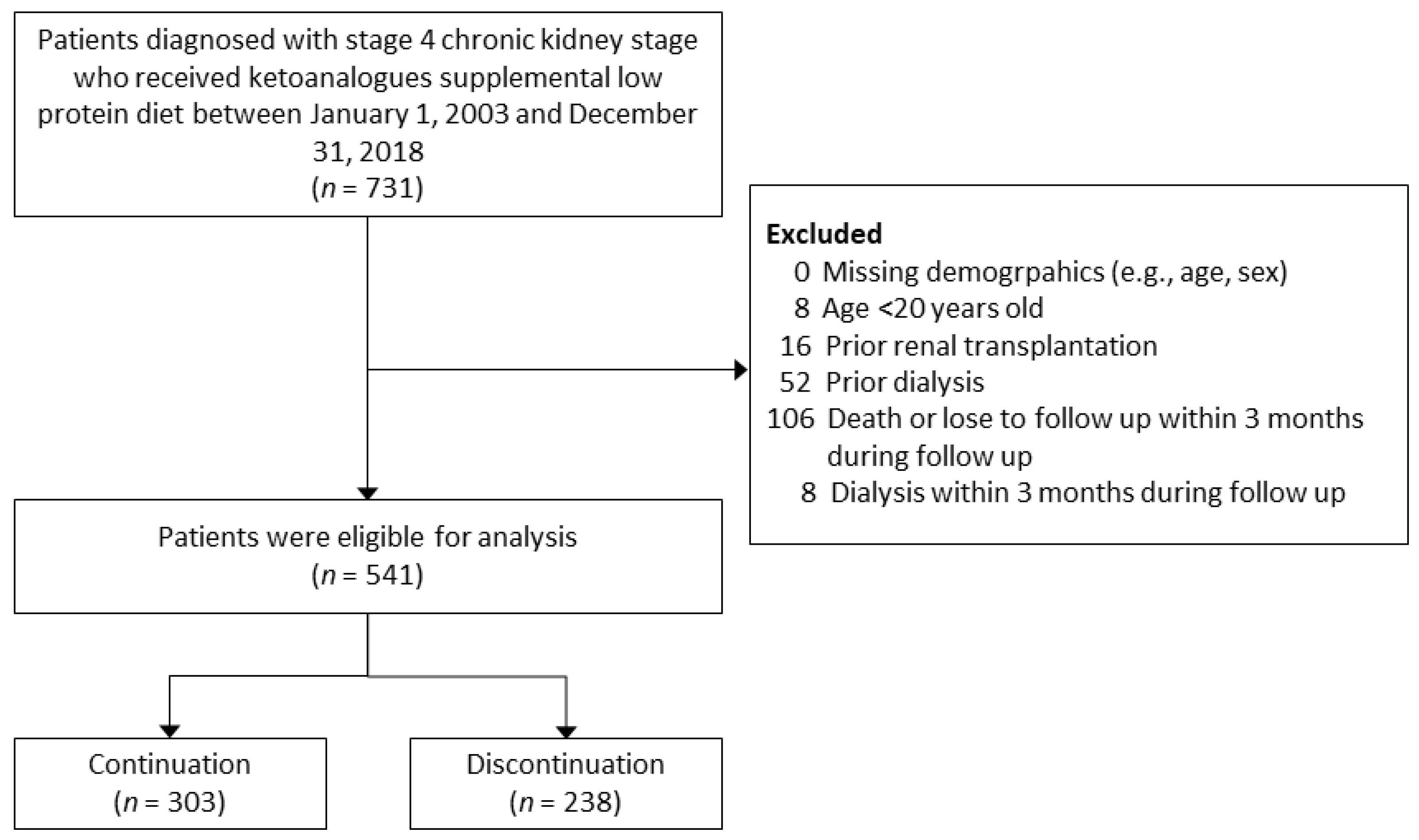
2.2. Study Design
2.3. Assessment of Covariates
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
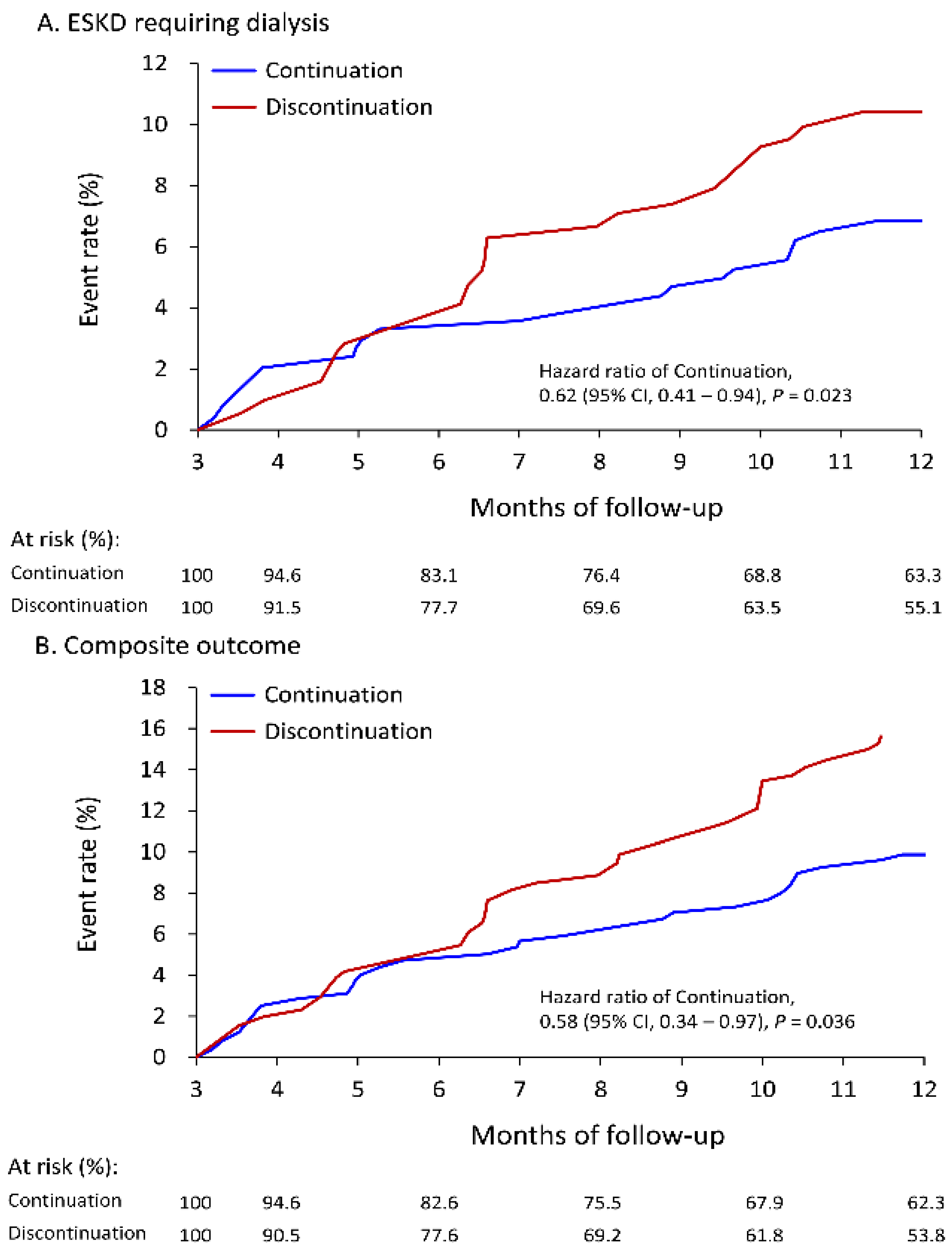
3.2. Follow-Up Outcomes
3.3. Subgroup Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kalantar-Zadeh, K.; Fouque, D. Nutritional Management of Chronic Kidney Disease. N. Engl. J. Med. 2018, 378, 584–585. [Google Scholar] [CrossRef] [PubMed]
- Addis, T.; Lew, W. Diet and Death in Acute Uremia. J. Clin. Investig. 1939, 18, 773–775. [Google Scholar] [CrossRef] [PubMed]
- Lewis, D.S. On the Influence of a Diet with High Protein Content on the Kidney. Can. Med. Assoc. J. 1921, 11, 682–683. [Google Scholar] [PubMed]
- Cuppari, L.; Meireles, M.S.; Ramos, C.I.; Kamimura, M.A. Subjective global assessment for the diagnosis of protein-energy wasting in nondialysis-dependent chronic kidney disease patients. J. Ren. Nutr. 2014, 24, 385–389. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Cano, N.J.; Franch, H.; Fouque, D.; Himmelfarb, J.; Kalantar-Zadeh, K.; Kuhlmann, M.K.; Stenvinkel, P.; TerWee, P.; Teta, D.; et al. Prevention and treatment of protein energy wasting in chronic kidney disease patients: A consensus statement by the International Society of Renal Nutrition and Metabolism. Kidney Int. 2013, 84, 1096–1107. [Google Scholar] [CrossRef]
- Hanna, R.M.; Ghobry, L.; Wassef, O.; Rhee, C.M.; Kalantar-Zadeh, K. A Practical Approach to Nutrition, Protein-Energy Wasting, Sarcopenia, and Cachexia in Patients with Chronic Kidney Disease. Blood Purif. 2020, 49, 202–211. [Google Scholar] [CrossRef]
- Walser, M. Ketoacids in the treatment of uremia. Clin. Nephrol. 1975, 3, 180–186. [Google Scholar]
- Walser, M.; Lund, P.; Ruderman, N.B.; Coulter, A.W. Synthesis of essential amino acids from their alpha-keto analogues by perfused rat liver and muscle. J. Clin. Investig. 1973, 52, 2865–2877. [Google Scholar] [CrossRef]
- Kang, C.W.; Tungsanga, K.; Walser, M. Effect of the level of dietary protein on the utilization of alpha-ketoisocaproate for protein synthesis. Am. J. Clin. Nutr. 1986, 43, 504–509. [Google Scholar] [CrossRef]
- Jiang, N.; Qian, J.; Sun, W.; Lin, A.; Cao, L.; Wang, Q.; Ni, Z.; Wan, Y.; Linholm, B.; Axelsson, J.; et al. Better preservation of residual renal function in peritoneal dialysis patients treated with a low-protein diet supplemented with keto acids: A prospective, randomized trial. Nephrol. Dial. Transpl. 2009, 24, 2551–2558. [Google Scholar] [CrossRef]
- Yen, C.L.; Fan, P.C.; Lee, C.C.; Kuo, G.; Tu, K.H.; Chen, J.J.; Lee, T.H.; Hsu, H.H.; Tian, Y.C.; Chang, C.H. Advanced Chronic Kidney Disease with Low and Very Low GFR: Can a Low-Protein Diet Supplemented with Ketoanalogues Delay Dialysis? Nutrients 2020, 12, 3358. [Google Scholar] [CrossRef] [PubMed]
- Satirapoj, B.; Vongwattana, P.; Supasyndh, O. Very low protein diet plus ketoacid analogs of essential amino acids supplement to retard chronic kidney disease progression. Kidney Res. Clin. Pract. 2018, 37, 384–392. [Google Scholar] [CrossRef]
- Bolasco, P. Very low protein plus ketoacid analogs of essential aminoacids do not confirm superiority of a low protein diet to retard chronic kidney disease progression. Kidney Res. Clin. Pract. 2019, 38, 124–125. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Xie, H.; Fang, M.; Wang, K.; Chen, J.; Sun, W.; Yang, L.; Lin, H. Keto-supplemented Low Protein Diet: A Valid Therapeutic Approach for Patients with Steroid-resistant Proteinuria during Early-stage Chronic Kidney Disease. J. Nutr. Health Aging 2016, 20, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Di Iorio, B.R.; Marzocco, S.; Bellasi, A.; De Simone, E.; Dal Piaz, F.; Rocchetti, M.T.; Cosola, C.; Di Micco, L.; Gesualdo, L. Nutritional therapy reduces protein carbamylation through urea lowering in chronic kidney disease. Nephrol. Dial. Transpl. 2018, 33, 804–813. [Google Scholar] [CrossRef]
- David, C.; Peride, I.; Niculae, A.; Constantin, A.M.; Checherita, I.A. Very low protein diets supplemented with keto-analogues in ESRD predialysis patients and its effect on vascular stiffness and AVF Maturation. BMC Nephrol. 2016, 17, 131. [Google Scholar] [CrossRef]
- Garneata, L.; Stancu, A.; Dragomir, D.; Stefan, G.; Mircescu, G. Ketoanalogue-Supplemented Vegetarian Very Low-Protein Diet and CKD Progression. J. Am. Soc. Nephrol. 2016, 27, 2164–2176. [Google Scholar] [CrossRef]
- Bellizzi, V.; Signoriello, S.; Minutolo, R.; Di Iorio, B.; Nazzaro, P.; Garofalo, C.; Calella, P.; Chiodini, P.; De Nicola, L.; The ERIKA Study Group Investigators of the Italian Society of Nephrology-Conservative Therapy of CKD Work Group. No additional benefit of prescribing a very low-protein diet in patients with advanced chronic kidney disease under regular nephrology care: A pragmatic, randomized, controlled trial. Am. J. Clin. Nutr. 2022, 115, 1404–1417. [Google Scholar] [CrossRef]
- Ikizler, T.A. Very low-protein diets in advanced kidney disease: Safe, effective, but not practical. Am. J. Clin. Nutr. 2022, 115, 1266–1267. [Google Scholar] [CrossRef]
- Lin, M.Y.; Cheng, L.J.; Chiu, Y.W.; Hsieh, H.M.; Wu, P.H.; Lin, Y.T.; Wang, S.L.; Jian, F.X.; Hsu, C.C.; Yang, S.A.; et al. Effect of national pre-ESRD care program on expenditures and mortality in incident dialysis patients: A population-based study. PLoS ONE 2018, 13, e0198387. [Google Scholar] [CrossRef]
- Wu, C.H.; Yang, Y.W.; Hung, S.C.; Kuo, K.L.; Wu, K.D.; Wu, V.C.; Hsieh, T.C. National Taiwan University Study Group on Acute Renal, F. Ketoanalogues supplementation decreases dialysis and mortality risk in patients with anemic advanced chronic kidney disease. PLoS ONE 2017, 12, e0176847. [Google Scholar] [CrossRef]
- Yen, C.L.; Fan, P.C.; Kuo, G.; Chen, C.Y.; Cheng, Y.L.; Hsu, H.H.; Tian, Y.C.; Chatrenet, A.; Piccoli, G.B.; Chang, C.H. Supplemented Low-Protein Diet May Delay the Need for Preemptive Kidney Transplantation: A Nationwide Population-Based Cohort Study. Nutrients 2021, 13, 3002. [Google Scholar] [CrossRef] [PubMed]
- Yen, C.L.; Tu, K.H.; Lin, M.S.; Chang, S.W.; Fan, P.C.; Hsiao, C.C.; Chen, C.Y.; Hsu, H.H.; Tian, Y.C.; Chang, C.H. Does a Supplemental Low-Protein Diet Decrease Mortality and Adverse Events After Commencing Dialysis? A Nationwide Cohort Study. Nutrients 2018, 10, 1035. [Google Scholar] [CrossRef]
- Shao, S.C.; Chan, Y.Y.; Kao Yang, Y.H.; Lin, S.J.; Hung, M.J.; Chien, R.N.; Lai, C.C.; Lai, E.C. The Chang Gung Research Database-A multi-institutional electronic medical records database for real-world epidemiological studies in Taiwan. Pharmacoepidemiol. Drug Saf. 2019, 28, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.S.; Lin, M.H.; Lee, C.P.; Yang, Y.H.; Chen, W.C.; Chang, G.H.; Tsai, Y.T.; Chen, P.C.; Tsai, Y.H. Chang Gung Research Database: A multi-institutional database consisting of original medical records. Biomed. J. 2017, 40, 263–269. [Google Scholar] [CrossRef]
- Austin, P.C.; Stuart, E.A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef]
- Mircescu, G.; Garneata, L.; Stancu, S.H.; Capusa, C. Effects of a supplemented hypoproteic diet in chronic kidney disease. J. Ren. Nutr. 2007, 17, 179–188. [Google Scholar] [CrossRef]
- Cianciaruso, B.; Capuano, A.; D’Amaro, E.; Ferrara, N.; Nastasi, A.; Conte, G.; Bellizzi, V.; Andreucci, V.E. Dietary compliance to a low protein and phosphate diet in patients with chronic renal failure. Kidney Int. Suppl. 1989, 27, S173–S176. [Google Scholar]
- Cupisti, A.; Gallieni, M.; Avesani, C.M.; D’Alessandro, C.; Carrero, J.J.; Piccoli, G.B. Medical Nutritional Therapy for Patients with Chronic Kidney Disease not on Dialysis: The Low Protein Diet as a Medication. J. Clin. Med. 2020, 9, 3644. [Google Scholar] [CrossRef]
- Chiang, H.H.; Hong, R.M.; Tsai, J.P.; Chen, M.Y. The Lived Experiences of Living with LPD among CKD Patients in Southern Taiwan. Neuropsychiatry 2017, 7, 48–56. [Google Scholar] [CrossRef]
- Bellizzi, V.; Calella, P.; Hernandez, J.N.; Gonzalez, V.F.; Lira, S.M.; Torraca, S.; Arronte, R.U.; Cirillo, P.; Minutolo, R.; Montufar Cardenas, R.A. Safety and effectiveness of low-protein diet supplemented with ketoacids in diabetic patients with chronic kidney disease. BMC Nephrol. 2018, 19, 110. [Google Scholar] [CrossRef] [PubMed]
- Milovanova, L.; Fomin, V.; Moiseev, S.; Taranova, M.; Milovanov, Y.; Lysenko Kozlovskaya, L.; Kozlov, V.; Kozevnikova, E.; Milovanova, S.; Lebedeva, M.; et al. Effect of essential amino acid small ka, Cyrillicetoanalogues and protein restriction diet on morphogenetic proteins (FGF-23 and capital KA, Cyrilliclotho) in 3b-4 stages chronic small ka, Cyrillicidney disease patients: A randomized pilot study. Clin. Exp. Nephrol. 2018, 22, 1351–1359. [Google Scholar] [CrossRef] [PubMed]
- Laville, S.M.; Couturier, A.; Lambert, O.; Metzger, M.; Mansencal, N.; Jacquelinet, C.; Laville, M.; Frimat, L.; Fouque, D.; Combe, C.; et al. Urea levels and cardiovascular disease in patients with chronic kidney disease. Nephrol. Dial. Transpl. 2022, 1–9. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Available Number | Continuation (n = 303) | Discontinuation (n = 238) | STD | p Value |
|---|---|---|---|---|---|
| Age, years | 541 | 67.1 ± 14.1 | 68.5 ± 14.4 | −0.10 | 0.24 |
| Age ≥ 65 years | 541 | 171 (56.4) | 157 (66.0) | −0.20 | 0.02 |
| Male | 541 | 187 (61.7) | 147 (61.8) | <0.01 | 0.99 |
| Body mass index, kg/m2 | 438 | 26.4 ± 24.2 | 24.8 ± 4.7 | 0.09 | 0.34 |
| eGFR at index, mL/min/1.73 m2 | 541 | 20.9 ± 4.8 | 20.9 ± 4.6 | <0.01 | 0.97 |
| Comorbidities | |||||
| Coronary artery disease | 541 | 87 (28.7) | 62 (26.1) | 0.06 | 0.49 |
| Hypertension | 541 | 248 (81.8) | 197 (82.8) | −0.02 | 0.78 |
| Diabetes mellitus | 541 | 152 (50.2) | 131 (55.0) | −0.10 | 0.26 |
| Atrial fibrillation | 541 | 18 (5.9) | 16 (6.7) | −0.03 | 0.71 |
| Liver cirrhosis | 541 | 26 (8.6) | 17 (7.1) | 0.05 | 0.54 |
| Peripheral artery disease | 541 | 29 (9.6) | 23 (9.7) | <0.01 | 0.97 |
| Dementia | 541 | 15 (5.0) | 18 (7.6) | −0.11 | 0.21 |
| Systemic lupus erythematosus | 541 | 5 (1.7) | 3 (1.3) | 0.03 | 0.71 |
| Hepatitis B infection | 541 | 20 (6.6) | 11 (4.6) | 0.09 | 0.33 |
| Hepatitis C infection | 541 | 12 (4.0) | 9 (3.8) | 0.01 | 0.92 |
| Heart failure hospitalization | 541 | 24 (7.9) | 20 (8.4) | −0.02 | 0.84 |
| Myocardial infarction | 541 | 25 (8.3) | 15 (6.3) | 0.08 | 0.39 |
| Stroke | 541 | 29 (9.6) | 30 (12.6) | −0.10 | 0.26 |
| No. of outpatient visits on nephrology in the previous year | 541 | 0.52 | |||
| 0 | 39 (12.9) | 37 (15.5) | −0.08 | ||
| 1–5 | 174 (57.4) | 139 (58.4) | −0.02 | ||
| 6–10 | 74 (24.4) | 47 (19.7) | 0.11 | ||
| >10 | 16 (5.3) | 15 (6.3) | −0.04 | ||
| No. of outpatient visits on all departments in the previous year | 541 | 12.8 ± 9.5 | 13.1 ± 9.1 | −0.03 | 0.75 |
| Admission in the previous year | 541 | 99 (32.7) | 99 (41.6) | −0.19 | 0.03 |
| Follow-up years | 541 | 1.5 [0.8, 3.4] | 1.3 [0.6, 3.2] | 0.03 | 0.74 |
| Variables | Available Number | Continuation (n = 303) | Discontinuation (n = 238) | STD | p Value |
|---|---|---|---|---|---|
| Medication at baseline | |||||
| ACEi/ARB | 541 | 179 (59.1) | 138 (58.0) | 0.02 | 0.80 |
| Beta-blockers | 541 | 79 (26.1) | 67 (28.2) | −0.05 | 0.59 |
| Calcium-channel blocker | 541 | 139 (45.9) | 106 (44.5) | 0.03 | 0.76 |
| Mineralocortocoid receptor antagonis | 541 | 23 (7.6) | 21 (8.8) | −0.04 | 0.60 |
| Loop diuretics | 541 | 99 (32.7) | 91 (38.2) | −0.12 | 0.18 |
| Nitrates | 541 | 40 (13.2) | 31 (13.0) | 0.01 | 0.95 |
| Vasodilator | 541 | 19 (6.3) | 17 (7.1) | −0.03 | 0.69 |
| Thiazide | 541 | 22 (7.3) | 22 (9.2) | −0.07 | 0.40 |
| Antiplatelet agents | 541 | 99 (32.7) | 72 (30.3) | 0.05 | 0.55 |
| NSAIDs | 541 | 31 (10.2) | 31 (13.0) | −0.09 | 0.31 |
| Steroid | 541 | 40 (13.2) | 39 (16.4) | −0.09 | 0.30 |
| Proton pump inhibitor | 541 | 48 (15.8) | 47 (19.7) | −0.10 | 0.24 |
| Insulin | 541 | 41 (13.5) | 35 (14.7) | −0.03 | 0.70 |
| Oral hypoglycemic agents | 541 | 107 (35.3) | 92 (38.7) | −0.07 | 0.42 |
| Pentoxyfillin | 541 | 136 (44.9) | 103 (43.3) | 0.03 | 0.71 |
| Sodium bicarbonate | 541 | 37 (12.2) | 20 (8.4) | 0.13 | 0.15 |
| Fibrate | 541 | 18 (5.9) | 13 (5.5) | 0.02 | 0.81 |
| Statin | 541 | 123 (40.6) | 93 (39.1) | 0.03 | 0.72 |
| Laboratory data at baseline | |||||
| Blood urine nitrogen, mg/dL | 497 | 43.6 ± 17.0 | 42.9 ± 19.2 | 0.04 | 0.67 |
| Creatinine, mg/dL | 541 | 2.9 ± 0.8 | 2.9 ± 0.8 | 0.06 | 0.46 |
| Proteinuria group, mg/dL | 335 | 0.02 | |||
| Negative (0–4) | 38 (20.2) | 14 (9.5) | 0.30 | ||
| Trace (5–29) | 14 (7.4) | 10 (6.8) | 0.03 | ||
| ≥1+ (≥30) | 136 (72.3) | 123 (83.7) | −0.28 | ||
| CO2 | 160 | 22.7 ± 3.8 | 22.5 ± 4.2 | 0.03 | 0.83 |
| Potassium, mg/dL | 496 | 4.4 ± 0.7 | 4.4 ± 0.7 | −0.05 | 0.55 |
| Sodium, mg/dL | 351 | 138.9 ± 4.2 | 138.6 ± 4.2 | 0.07 | 0.52 |
| Calcium, mg/dL | 429 | 8.9 ± 0.6 | 8.9 ± 0.7 | 0.07 | 0.46 |
| Phosphorus, mg/dL | 323 | 3.8 ± 0.7 | 4.0 ± 0.9 | −0.19 | 0.10 |
| HDL, mg/dL | 174 | 46.2 ± 13.2 | 43.4 ± 12.8 | 0.21 | 0.18 |
| LDL, mg/dL | 222 | 79.1 ± 56.7 | 79.3 ± 49.4 | <0.01 | 0.98 |
| Total cholesterol, mg/dL | 122 | 174.9 ± 41.2 | 176.3 ± 55.0 | −0.03 | 0.87 |
| HbA1C, % | 249 | 7.0 ± 1.5 | 7.1 ± 1.7 | −0.08 | 0.51 |
| Albumin, mg/dL | 400 | 3.8 ± 0.5 | 3.8 ± 0.6 | 0.05 | 0.62 |
| Hemoglobin, g/dL | 464 | 10.5 ± 1.8 | 10.4 ± 1.8 | 0.02 | 0.83 |
| Serum uric acid, mg/dL | 386 | 7.1 ± 2.0 | 7.5 ± 2.2 | −0.21 | 0.04 |
| Continuation | Discontinuation | HR (95% CI) of | ||||
|---|---|---|---|---|---|---|
| Follow Up/Outcome | Event Rate | Incidence (95% CI) * | Event Rate | Incidence (95% CI) * | Continuation | p Value |
| 1-year follow-up | ||||||
| Primary outcome: ESKD requiring dialysis | 6.8% | 8.2 (6.0–10.8) | 10.4% | 13.1 (9.7–16.5) | 0.62 (0.41–0.94) * | 0.023 |
| MACCE † | 3.2% | 3.8 (2.0–5.6) | 5.3% | 6.4 (4.0–8.8) | 0.59 (0.25–1.39) | 0.225 |
| Cardiovascular death | 2.0% | 2.3 (1.0–3.7) | 3.3% | 4.0 (2.1–5.8) | 0.57 (0.19–1.71) | 0.314 |
| Acute myocardial infarction | 0.9% | 1.1 (0.0–2.0) | 2.5% | 3.0 (1.4–4.7) | 0.36 (0.09–1.48) | 0.156 |
| Ischemic stroke | 0.3% | 0.4 (0.0–1.0) | 0.8% | 0.9 (0.0–1.8) | 0.44 (0.03–6.83) | 0.557 |
| All-cause death | 3.8% | 4.4 (3.0–6.4) | 5.6% | 6.7 (4.3–9.1) | 0.65 (0.27–1.54) | 0.329 |
| Infection related death | 3.1% | 3.6 (2.0–5.3) | 3.6% | 4.3 (2.4–6.2) | 0.82 (0.29–2.33) | 0.714 |
| Composite outcome # | 9.9% | 11.8 (9.0–15.0) | 15.9% | 20.2 (15.9–24.4) | 0.58 (0.34–0.97) * | 0.036 |
| At the end of follow-up | ||||||
| Primary outcome: ESKD requiring dialysis | 25.6% | 12.1 (10.0–14.2) | 26.8% | 13.9 (11.6–16.2) | 0.91 (0.72–1.14) | 0.406 |
| MACCE † | 11.5% | 4.6 (3.0–5.8) | 13.2% | 5.7 (4.4–7.1) | 0.81 (0.49–1.33) | 0.396 |
| Cardiovascular death | 8.6% | 3.3 (2.0–4.2) | 9.8% | 4.1 (3.0–5.2) | 0.79 (0.44–1.39) | 0.408 |
| Acute myocardial infarction | 3.3% | 1.3 (1.0–1.9) | 3.7% | 1.6 (0.9–2.3) | 0.83 (0.33–2.09) | 0.698 |
| Ischemic stroke | 2.9% | 1.2 (1.0–1.7) | 3.6% | 1.5 (0.8–2.2) | 0.75 (0.28–2.03) | 0.573 |
| All-cause death | 11.4% | 4.4 (3.0–5.4) | 13.9% | 5.8 (4.5–7.2) | 0.74 (0.45–1.21) | 0.228 |
| Infection related death | 8.4% | 3.2 (2.0–4.2) | 9.2% | 3.9 (2.8–4.9) | 0.82 (0.45–1.50) | 0.521 |
| Composite outcome # | 31.4% | 15.3 (13.0–17.6) | 36.9% | 19.6 (16.9–22.3) | 0.77 (0.57–1.05) | 0.100 |
| Event Rate | HR (95% CI) of Continuation | p for Interaction § | ||
|---|---|---|---|---|
| Subgroup | Continuation | Discontinuation | ||
| Age group | 0.375 | |||
| 20–65 | 8.3% | 9.0% | 0.88 (0.32–2.39) | |
| >65 | 5.9% | 11.3% | 0.48 (0.20–1.15) | |
| Gender | 0.186 | |||
| Female | 7.6% | 6.5% | 1.15 (0.38–3.45) | |
| Male | 6.4% | 12.7% | 0.46 (0.21–1.01) | |
| Body mass index, kg/m2 | 0.974 | |||
| <24 | 11.3% | 18.1% | 0.58 (0.27–1.27) | |
| ≥24 | 4.7% | 7.4% | 0.60 (0.18–2.01) | |
| eGFR at baseline | 0.843 | |||
| 15–20 mL/min/1.73 m2 | 10.3% | 16.4% | 0.60 (0.29–1.25) | |
| 21–30 mL/min/1.73 m2 | 3.1% | 4.0% | 0.71 (0.18–2.71) | |
| Hypertension | 0.934 | |||
| No | 4.8% | 7.1% | 0.67 (0.10–4.45) | |
| Yes | 7.3% | 11.1% | 0.61 (0.31–1.21) | |
| Diabetes mellitus | 0.430 | |||
| No | 5.7% | 10.8% | 0.46 (0.17–1.26) | |
| Yes | 7.9% | 10.1% | 0.78 (0.34–1.78) | |
| Cardiovascular disease * | 0.531 | |||
| No | 7.4% | 9.4% | 0.72 (0.31–1.71) | |
| Yes | 5.9% | 12.2% | 0.48 (0.18–1.29) | |
| ACEi/ARB | 0.514 | |||
| No | 7.2% | 7.7% | 0.82 (0.28–2.39) | |
| Yes | 6.6% | 12.3% | 0.53 (0.24–1.17) | |
| Loop diuretics | 0.412 | |||
| No | 5.6% | 10.0% | 0.50 (0.21–1.18) | |
| Yes | 9.4% | 11.3% | 0.86 (0.32–2.31) | |
| Pentoxyfilline | 0.719 | |||
| No | 7.0% | 10.1% | 0.69 (0.28–1.68) | |
| Yes | 6.7% | 10.8% | 0.54 (0.22–1.36) | |
| Proteinuria | 0.603 | |||
| Negative/Trace | 3.7% | 14.2% | 0.26 (0.02–3.46) | |
| ≥1+ | 7.7% | 13.7% | 0.53 (0.24–1.16) | |
| Albumin, mg/dL | 0.242 | |||
| <3.5 | 15.4% | 13.6% | 1.02 (0.35–2.95) | |
| ≥3.5 | 5.8% | 12.1% | 0.45 (0.18–1.10) | |
| Hemoglobin, g/dL | 0.388 | |||
| <10 | 10.4% | 14.1% | 0.66 (0.29–1.52) | |
| ≥10 | 4.1% | 10.7% | 0.36 (0.12–1.12) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yen, C.-L.; Fan, P.-C.; Chen, J.-J.; Kuo, G.; Hsiao, C.-C.; Chen, C.-Y.; Tu, Y.-R.; Hsu, H.-H.; Chen, Y.-C.; Chang, C.-H. Ketoanalogues Supplemental Low Protein Diet Safely Decreases Short-Term Risk of Dialysis among CKD Stage 4 Patients. Nutrients 2022, 14, 4020. https://doi.org/10.3390/nu14194020
Yen C-L, Fan P-C, Chen J-J, Kuo G, Hsiao C-C, Chen C-Y, Tu Y-R, Hsu H-H, Chen Y-C, Chang C-H. Ketoanalogues Supplemental Low Protein Diet Safely Decreases Short-Term Risk of Dialysis among CKD Stage 4 Patients. Nutrients. 2022; 14(19):4020. https://doi.org/10.3390/nu14194020
Chicago/Turabian StyleYen, Chieh-Li, Pei-Chun Fan, Jia-Jin Chen, George Kuo, Ching-Chung Hsiao, Chao-Yu Chen, Yi-Ran Tu, Hsiang-Hao Hsu, Yung-Chang Chen, and Chih-Hsiang Chang. 2022. "Ketoanalogues Supplemental Low Protein Diet Safely Decreases Short-Term Risk of Dialysis among CKD Stage 4 Patients" Nutrients 14, no. 19: 4020. https://doi.org/10.3390/nu14194020
APA StyleYen, C.-L., Fan, P.-C., Chen, J.-J., Kuo, G., Hsiao, C.-C., Chen, C.-Y., Tu, Y.-R., Hsu, H.-H., Chen, Y.-C., & Chang, C.-H. (2022). Ketoanalogues Supplemental Low Protein Diet Safely Decreases Short-Term Risk of Dialysis among CKD Stage 4 Patients. Nutrients, 14(19), 4020. https://doi.org/10.3390/nu14194020