
Association between the Severity of Dental Caries and the Degree of Adherence to the Mediterranean Diet in the Pediatric Population

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Variables
2.3. Statistical Analysis
3. Results
3.1. Sex and Age of the Sample
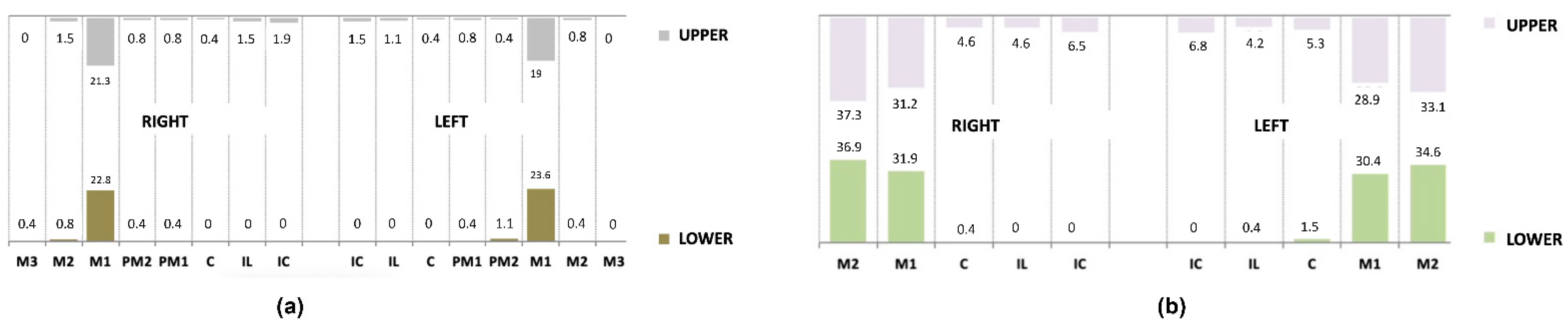
3.2. Prevalence and Extension of Carious Lesions
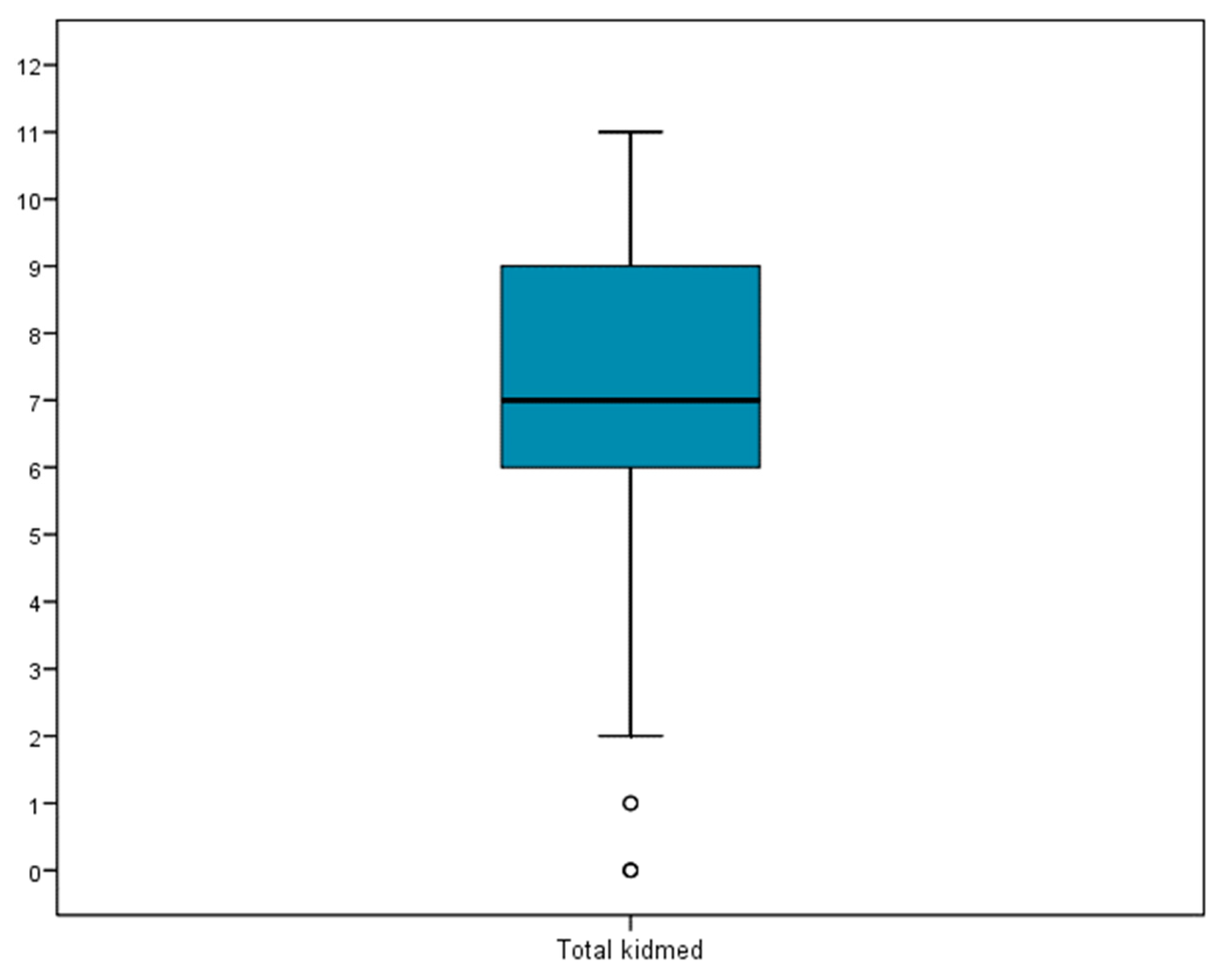
3.3. Adherence to Mediterranean Diet
3.4. Association between Caries and Adherence to the Mediterranean Diet
3.4.1. Prevalence of Dental Caries and Adherence to Mediterranean Diet
3.4.2. Global Caries Prevalence and Adherence to the Mediterranean Diet
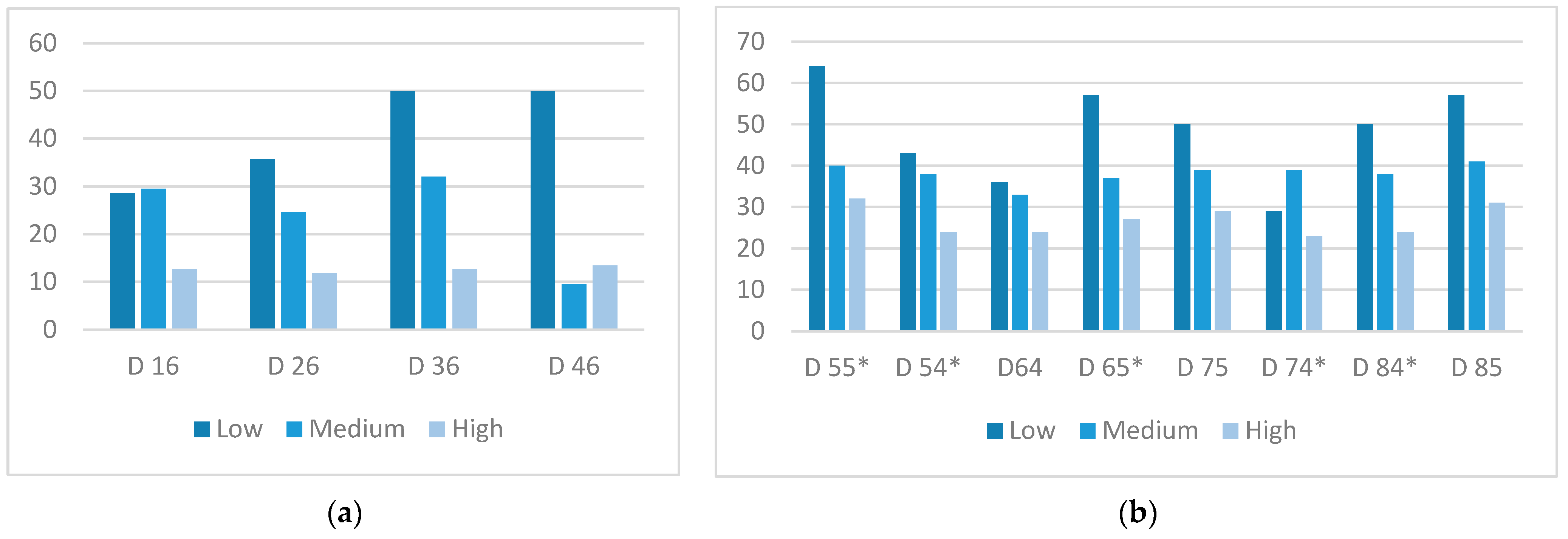
3.4.3. Caries Extension (Number of Affected Teeth) and Adherence to Mediterranean Diet
3.4.4. Caries severity (ICCMS) and Adherence to the Mediterranean Diet
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Mathur, V.P.; Dhillon, J.K. Dental Caries: A Disease Which Needs Attention. Indian J Pediatr. 2018, 85, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Chaffee, B.W.; Rodrigues, P.H.; Kramer, P.F.; Vítolo, M.R.; Feldens, C.A. Oral health-related quality-of-life scores differ by socioeconomic status and caries experience. Community Dent. Oral Epidemiol. 2017, 45, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Kastenbom, L.; Falsen, A.; Larsson, P.; Sunnegårdh-Grönberg, K.; Davidson, T. Costs and health-related quality of life in relation to caries. BMC Oral Health 2019, 19, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Almerich-Torres, T.; Montiel-Company, J.M.; Bellot-Arcis, C.; Iranzo-Cortes, J.E.; Ortola-Siscar, J.C.; Almerich-Silla, J.M. Caries Prevalence Evolution and Risk Factors among Schoolchildren and Adolescents from Valencia (Spain): Trends 1998–2018. Int. J. Environ. Res. Public Health 2020, 17, 6561. [Google Scholar] [CrossRef]
- Rugg-Gunn, A. Dental Caries: Strategies to Control This Preventable Disease. Acta Med. Acad. 2013, 42, 117–130. [Google Scholar] [CrossRef] [PubMed]
- Inan-Eroglu, E.; Ozşin-Ozler, C.; Erçim, R.E.; Buyuktuncer, Z.; Uzamış-Tekçiçek, M.; Guçiz-Dogan, B. Is diet quality associated with early childhood caries in preschool children? A descriptive study. Turk. J. Pediatr. 2017, 59, 537–547. [Google Scholar] [CrossRef]
- Zeng, L.; Zeng, Y.; Zhou, Y.; Wen, J.; Wan, L.; Ou, X.; Zhou, X. Diet and Lifestyle Habits Associated with Caries in Deciduous Teeth among 3- to 5-Year-Old Preschool Children in Jiangxi Province, China. BMC Oral Health 2018, 18, 224. [Google Scholar] [CrossRef]
- Van Loveren, C. Sugar Restriction for Caries Prevention: Amount and Frequency. Which Is More Important? Caries Res. 2019, 53, 168–175. [Google Scholar] [CrossRef]
- Kashket, S.; DePaola, D.P. Cheese Consumption and the Development and Progression of Dental Caries. Nutr. Rev. 2002, 60, 97–103. [Google Scholar] [CrossRef]
- Touger-Decker, R.; Mobley, C.C. Position of the American Dietetic Association: Oral Health and Nutrition. J. Am. Diet. Assoc. 2003, 103, 615–625. [Google Scholar] [CrossRef]
- Giacaman, R.A. Sugars and beyond. The Role of Sugars and the Other Nutrients and Their Potential Impact on Caries. Oral Dis. 2018, 24, 1185–1197. [Google Scholar] [CrossRef] [PubMed]
- Dernini, S.; Berry, E.M.; Serra-Majem, L.; La Vecchia, C.; Capone, R.; Medina, F.X.; Aranceta-Bartrina, J.; Belahsen, R.; Burlingame, B.; Calabrese, G.; et al. Med Diet 4.0: The Mediterranean diet with four sustainable benefits. Public Health Nutr. 2017, 20, 1322–1330. [Google Scholar] [CrossRef] [PubMed]
- Urquiaga, I.; Echeverría, G.; Dussaillant, C.; Rigotti, A. Origin components and mechanisms of action of the Mediterranean diet. Rev. Med. Chil. 2017, 145, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Carrillo, H.A.; Ramírez-Vélez, R. Adherence to the Mediterranean diet in a sample of Colombian schoolchildren: An evaluation of the psychometric properties of the KIDMED questionnaire. Nutr. Hosp. 2020, 37, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet: A Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Lacoba, R.; Pardo-Garcia, I.; Amo-Saus, E.; Escribano-Sotos, F. Mediterranean Diet and Health Outcomes: A Systematic Meta-Review. Eur. J. Public Health 2018, 28, 955–961. [Google Scholar] [CrossRef]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to Mediterranean diet and health status: Meta-analysis. BMJ 2008, 337, 1344. [Google Scholar] [CrossRef]
- Barja-Fernandez, S.; Pino, M.; Portela, I.; Leis, R. Evaluation of food habits and physical activity in Galician students. Nutr. Hosp. 2020, 37, 93–100. [Google Scholar] [CrossRef]
- Kabi, N.S.; Eltawil, S. Prioritizing the Risk Factors of Severe Early Childhood Caries. Dent. J. 2017, 5, 4. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, M.R.; Garcia, A.; Perez-Rodriguez, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean diet quality index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef]
- Pitts, N.B.; Ekstrand, K.R.; ICDAS Foundation. International Caries Detection and Assessment System (ICDAS) and its International Caries Classification and Management System (ICCMS)—Methods for staging of the caries process and enabling dentists to manage caries. Community Dent. Oral Epidemiol. 2013, 41, e41–e52. [Google Scholar] [CrossRef] [PubMed]
- Berkowitz, R.J. Causes, Treatment and Prevention of Early Childhood Caries: A Microbiologic Perspective. J. Can. Dent. Assoc. 2003, 69, 304–307. [Google Scholar] [CrossRef] [PubMed]
- Dye, B.A.; Hsu, K.L.C.; Afful, J. Prevalence and Measurement of Dental Caries in Young Children. Pediatr. Dent. 2015, 37, 200–216. [Google Scholar] [CrossRef]
- Uribe, S.E.; Innes, N.; Maldupa, I. The global prevalence of early childhood caries: A systematic review with meta-analysis using the WHO diagnostic criteria. Int. J. Paediatr Dent. 2021, 31, 817–830. [Google Scholar] [CrossRef] [PubMed]
- Moynihan, P. Sugars and Dental Caries: Evidence for Setting a Recommended Threshold for Intake. Adv. Nutr. 2016, 7, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Kale, S.; Kakodkar, P.; Shetiya, S.; Abdulkader, R. Prevalence of dental caries among children aged 5–15 years from 9 countries in the Eastern Mediterranean Region: A meta-analysis. East Mediterr. Health J. 2020, 26, 726–735. [Google Scholar] [CrossRef]
- Iranzo-Cortes, J.E.; Montiel-Company, J.; Almerich-Silla, J. Caries Diagnosis: Agreement between WHO and ICDAS II Criteria in Epidemiological Surveys. Community Dent. Health 2013, 30, 108–111. [Google Scholar]
- Braga, M.M.; Mendes, F.M.; Martignon, S.; Ricketts, D.N.J.; Ekstrand, K.R. In Vitro Comparison of Nyvad’s System and ICDAS-II with Lesion Activity Assessment for Evaluation of Severity and Activity of Occlusal Caries Lesions in Primary Teeth. Caries Res. 2009, 43, 405–412. [Google Scholar] [CrossRef]
- Stefan, L.; Prosoli, R.; Juranko, D.; Cule, M.; Milinovic, I.; Nova, D.; Sporis, G. The Reliability of the Mediterranean Diet Quality Index (KIDMED) Questionnaire. Nutrients 2017, 9, 419. [Google Scholar] [CrossRef]
- Iaccarino, P.; Scalfi, L.; Valerio, G. Adherence to the Mediterranean Diet in Children and Adolescents: A Systematic Review. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 283–299. [Google Scholar] [CrossRef]
- Mariscal-Arcas, M.; Rivas, A.; Velasco, J.; Ortega, M.; Caballero, A.M.; Olea-Serrano, F. Evaluation of the Mediterranean Diet Quality Index (KIDMED) in Children and Adolescents in Southern Spain. Public Health Nutr. 2009, 12, 1408–1412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tapia-Serrano, M.A.; Vaquero-Solis, M.; Lopez-Gajardo, M.A.; Sanchez-Miguel, P.A. Adherence to the Mediterranean diet, and importance in the physical activity and screen time in High School adolescents from Extremadura (Spain). Nutr. Hosp. 2021, 38, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Borrell, C.; Garcia, E.; Marques, L. Association between eating behavior pattern and caries in a population of children aged 3 to 9 years in the province of Alicante. Nutr. Hosp. 2022, 39, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Ojeda-Rodriguez, A.; Zazpe, I.; Morell-Azanza, L.; Chueca, M.J.; Azcona-Sanjulian, M.C.; Marti, A. Improved Diet Quality and Nutrient Adequacy in Children and Adolescents with Abdominal Obesity after a Lifestyle Intervention. Nutrients 2018, 10, 1500. [Google Scholar] [CrossRef]
- Onieva-Zafra, M.D.; Fernandez-Martinez, E.; Abreu-Sanchez, A.; Iglesias-Lopez, M.T.; Garcia-Padilla, F.M.; Pedregal-Gonzalez, M.; Parra, M.L. Relationship between Diet, Menstrual Pain and Other Menstrual Characteristics among Spanish Students. Nutrients 2020, 12, 1759. [Google Scholar] [CrossRef]
- Marques, L.; Garcia, E.; Borrell, C. Relationship between Dental Caries and Adherence to Mediterranean Diet in a Population of Children. Clin. Nutr. Hosp. Diet. 2021, 41, 105–110. [Google Scholar] [CrossRef]
- Amazouz, H.; Roda, C.; Beydon, N.; Lezmi, G.; Bourgoin-Heck, M.; Just, J.; Momas, I.; Rancière, F. Mediterranean Diet and Lung Function, Sensitization, and Asthma at School Age: The PARIS Cohort. Pediatr. Allergy Immunol. 2021, 32, 1437–1444. [Google Scholar] [CrossRef]
- Kanellopoulou, A.; Giannakopoulou, S.P.; Notara, V.; Antonogeorgos, G.; Rojas-Gil, A.P.; Kornilaki, E.N.; Konstantinou, E.; Lagiou, A.; Panagiotakos, D.B. The Association between Adherence to the Mediterranean Diet and Childhood Obesity; the Role of Family Structure: Results from an Epidemiological Study in 1728 Greek Students. Nutr. Health 2021, 27, 39–47. [Google Scholar] [CrossRef]
- Docimo, R.; Costacurta, M.; Gualtieri, P.; Pujia, A.; Leggeri, C.; Attina, A.; Cinelli, G.; Giannattasio, S.; Rampello, T.; Di Renzo, L. Cariogenic Risk and COVID-19 Lockdown in a Paediatric Population. Int. J. Environ. Res. Public Health 2021, 18, 7558. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Lagiou, P. Healthy Traditional Mediterranean Diet: An Expression of Culture, History, and Lifestyle. Nutr. Rev. 1997, 55, 383–389. [Google Scholar] [CrossRef]
- Makinen, K.K. Sugar Alcohol Sweeteners as Alternatives to Sugar with Special Consideration of Xylitol. Med. Princ. Pract. 2011, 20, 303–320. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, A.; Jadad, A.R. The Impact of Polyol-Containing Chewing Gums on Dental Caries a Systematic Review of Origi-nal Randomized Controlled Trials and Observational Studies. J. Am. Dent. Assoc. 2008, 139, 1602–1614. [Google Scholar] [CrossRef] [PubMed]
- Runnel, R.; Makinen, K.K.; Honkala, S.; Olak, J.; Makinen, P.L.; Nommela, R.; Vahlberg, T.; Honkala, E.; Saag, M. Effect of Three-Year Consumption of Erythritol, Xylitol and Sorbitol Candies on Various Plaque and Salivary Caries-Related Variables. J. Dent. 2013, 41, 1236–1244. [Google Scholar] [CrossRef]
- Burt, B.A. The Use of Sorbitol and Xylitol Sweetened Chewing Gum in Caries Control. J. Am. Dent. Assoc. 2006, 137, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Riley, P.; Moore, D.; Ahmed, F.; Sharif, M.; Worthington, H. Xylitol-Containing Products for Preventing Dental Caries in Children and Adults. Cochrane Database Syst. Rev. 2015, 3, CD010743. [Google Scholar] [CrossRef]
- Yamanaka, A.; Kimizuka, R.; Kato, T.; Okuda, K. Inhibitory Effects of Cranberry Juice on Attachment of Oral Streptococci and Biofilm Formation. Oral Microbiol. Immunol. 2004, 19, 150–154. [Google Scholar] [CrossRef]
- Nakahara, K.; Kawabata, S.; Ono, H.; Ogura, K.; Tanaka, T.; Ooshima, T.; Hamada, S. Inhibitory effect of oolong tea polyphenols on glycosyltransferases of mutans Streptococci. Appl. Environ. Microbiol. 1993, 59, 968–973. [Google Scholar] [CrossRef] [PubMed]
- Marshall, T.A. Nomenclature, Characteristics, and Dietary Intakes of Sugars. J. Am. Dent. Assoc. 2015, 146, 61–64. [Google Scholar] [CrossRef]
- Moynihan, P.J.; Kelly, S.A.M. Effect on Caries of Restricting Sugars Intake: Systematic Review to Inform WHO Guidelines. J. Dent. Res. 2014, 93, 8–18. [Google Scholar] [CrossRef]
- Attiguppe, P.; Malik, N.; Ballal, S.; Naik, S.V. CPP-ACP and Fluoride: A Synergism to Combat Caries. Int. J. Clin. Pediatr. Dent. 2019, 12, 120–125. [Google Scholar] [CrossRef]
- Coelho, A.S.E.C.; Paula, A.B.P.; Carrilho, T.M.P.; Da Silva, M.J.R.F.; Botelho, M.F.R.R.; Carrilho, E.V.V.F. Chlorhexidine mouthwash as an anticaries agent: A systematic review. Quintessence Int. 2017, 48, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.H.; Lin, C.H.; Pan, T.M. The Implication of Probiotics in the Prevention of Dental Caries. Appl. Microbiol. Biotechnol. 2018, 102, 577–586. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Permanent Tooth | p-Value | Primary Tooth | p-Value |
|---|---|---|---|
| 1.7 | 0.123 | 5.5 | 0.037 * |
| 1.6 | 0.001 ** | 5.4 | 0.035 * |
| 1.5 | 0.499 | 5.3 | 0.031 * |
| 1.4 | 0.499 | 5.2 | 0.018 * |
| 1.3 | 1.000 | 5.1 | 0.264 |
| 1.2 | 0.623 | 6.1 | 0.183 |
| 1.1 | 0.372 | 6.2 | 0.029 * |
| 2.1 | 0.623 | 6.3 | 0.137 |
| 2.2 | 1.000 | 6.4 | 0.292 |
| 2.3 | 1.000 | 6.5 | 0.034 * |
| 2.4 | 1.000 | 7.5 | 0.137 |
| 2.5 | 1.000 | 7.4 | 0.027 * |
| 2.6 | 0.004 ** | 7.3 | 0.891 |
| 2.7 | 0.499 | 7.2 | 0.560 |
| 3.7 | 1.000 | 7.1 | - |
| 3.6 | <0.001 *** | 8.1 | - |
| 3.5 | 0.248 | 8.2 | - |
| 3.4 | 1.000 | 8.3 | 0.548 |
| 3.3 | - | 8.4 | 0.026 * |
| 3.2 | - | 8.5 | 0.066 |
| 3.1 | - | ||
| 4.1 | - | ||
| 4.2 | - | ||
| 4.3 | - | ||
| 4.4 | 1.000 | ||
| 4.5 | 1.000 | ||
| 4.6 | <0.001 *** | ||
| 4.7 | 1.000 |
| Adherence to Mediterranean Diet | ||||||||
|---|---|---|---|---|---|---|---|---|
| Total | Low | Medium | High | |||||
| n | % | n | % | n | % | n | % | |
| Total | 263 | 100% | 14 | 100 | 122 | 100% | 127 | 100% |
| No | 65 | 24.7% | 2 | 14.3% | 21 | 17.2% | 42 | 33.1% |
| Yes | 198 | 75.3% | 12 | 85.7% | 101 | 82.8% | 85 | 66.9% |
| Adherence to Mediterranean Diet | ||||
|---|---|---|---|---|
| Total | Low | Medium | High | |
| n | 263 | 14 | 122 | 127 |
| Mean | 4.0 | 6.1 | 5.0 | 2.9 |
| Typical deviation | 3.8 | 4.4 | 4.1 | 3.1 |
| Minimum | 0 | 0 | 0 | 0 |
| Maximum | 17.0 | 12.0 | 17.0 | 13.0 |
| 25th Percentile | 1.0 | 3.0 | 1.0 | 0 |
| Median | 3.0 | 5.5 | 4.0 | 2.0 |
| 75th Percentile | 6.0 | 11.0 | 8.0 | 4.0 |
| Permanent Tooth | r | p-Value | Primary Tooth | r | p-Value |
|---|---|---|---|---|---|
| 1.7 | −0.14 | 0.027 * | 5.5 | −0.17 | 0.005 ** |
| 1.6 | −0.19 | 0.002 ** | 5.4 | −0.16 | 0.009 ** |
| 1.5 | −0.02 | 0.735 | 5.3 | −0.13 | 0.031 * |
| 1.4 | −0.02 | 0.735 | 5.2 | −0.13 | 0.038 * |
| 1.3 | −0.02 | 0.811 | 5.1 | −0.08 | 0.187 |
| 1.2 | −0.02 | 0.745 | 6.1 | −0.10 | 0.097 |
| 1.1 | −0.03 | 0.692 | 6.2 | −0.12 | 0.062 |
| 2.1 | −0.02 | 0.745 | 6.3 | −0.08 | 0.178 |
| 2.2 | −0.02 | 0.810 | 6.4 | −0.12 | 0.049 * |
| 2.3 | −0.02 | 0.810 | 6.5 | −0.20 | 0.001 ** |
| 2.4 | 0.01 | 0.913 | 7.5 | −0.18 | 0.004 ** |
| 2.5 | −0.02 | 0.811 | 7.4 | −0.20 | 0.001 ** |
| 2.6 | −0.20 | 0.001 ** | 7.3 | −0.01 | 0.815 |
| 2.7 | −0.06 | 0.304 | 7.2 | −0.01 | 0.811 |
| 3.7 | −0.08 | 0.227 | 7.1 | − | − |
| 3.6 | −0.24 | <0.001 *** | 8.1 | − | − |
| 3.5 | −0.03 | 0.678 | 8.2 | − | − |
| 3.4 | −0.02 | 0.811 | 8.3 | 0.02 | 0.695 |
| 3.3 | − | − | 8.4 | −0.20 | 0.001 ** |
| 3.2 | − | − | 8.5 | −0.16 | 0.010 * |
| 3.1 | − | − | |||
| 4.1 | − | − | |||
| 4.2 | − | − | |||
| 4.3 | − | − | |||
| 4.4 | −0.02 | 0.811 | |||
| 4.5 | −0.02 | 0.811 | |||
| 4.6 | −0.24 | <0.001 *** | |||
| 4.7 | −0.04 | 0.560 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marqués-Martínez, L.; Pérez-Bermejo, M.; Lairón-Peris, A.R.; Guinot-Barona, C.; Borrell-García, C.; García-Miralles, E. Association between the Severity of Dental Caries and the Degree of Adherence to the Mediterranean Diet in the Pediatric Population. Nutrients 2022, 14, 3622. https://doi.org/10.3390/nu14173622
Marqués-Martínez L, Pérez-Bermejo M, Lairón-Peris AR, Guinot-Barona C, Borrell-García C, García-Miralles E. Association between the Severity of Dental Caries and the Degree of Adherence to the Mediterranean Diet in the Pediatric Population. Nutrients. 2022; 14(17):3622. https://doi.org/10.3390/nu14173622
Chicago/Turabian StyleMarqués-Martínez, Laura, Marcelino Pérez-Bermejo, Ana Rosa Lairón-Peris, Clara Guinot-Barona, Carla Borrell-García, and Esther García-Miralles. 2022. "Association between the Severity of Dental Caries and the Degree of Adherence to the Mediterranean Diet in the Pediatric Population" Nutrients 14, no. 17: 3622. https://doi.org/10.3390/nu14173622
APA StyleMarqués-Martínez, L., Pérez-Bermejo, M., Lairón-Peris, A. R., Guinot-Barona, C., Borrell-García, C., & García-Miralles, E. (2022). Association between the Severity of Dental Caries and the Degree of Adherence to the Mediterranean Diet in the Pediatric Population. Nutrients, 14(17), 3622. https://doi.org/10.3390/nu14173622