
Reduction of Cardiovascular Events and Related Healthcare Expenditures through Achieving Population-Level Targets of Dietary Salt Intake in Japan: A Simulation Model Based on the National Health and Nutrition Survey

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
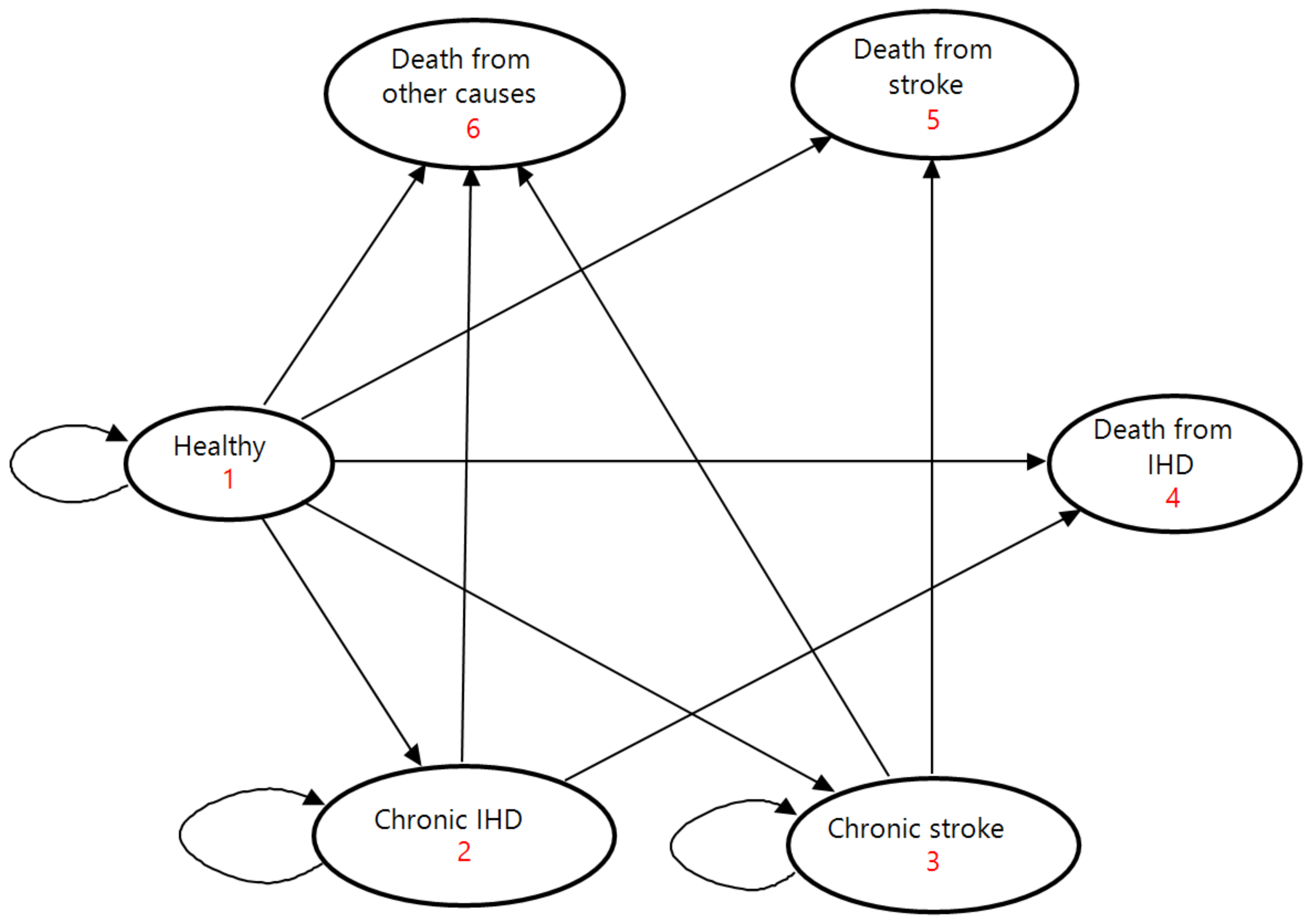
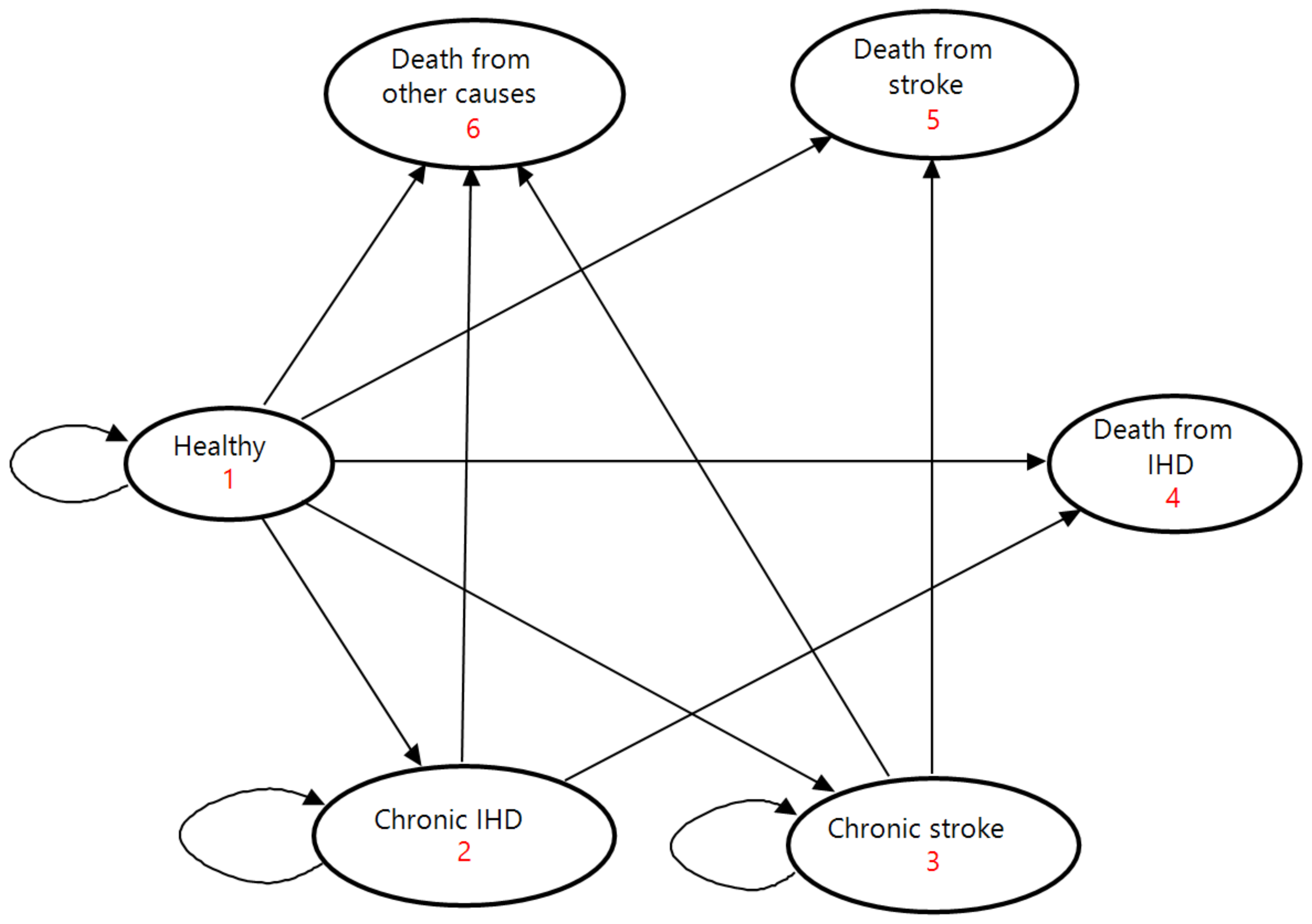
2.1. Modeling Framework and Study Population
2.2. Scenarios
2.3. Input Parameters
2.4. Model Validation and Sensitivity Analyses
3. Results
3.1. Projected Incidence, Mortality, and National Healthcare Expenditures on the Base Case
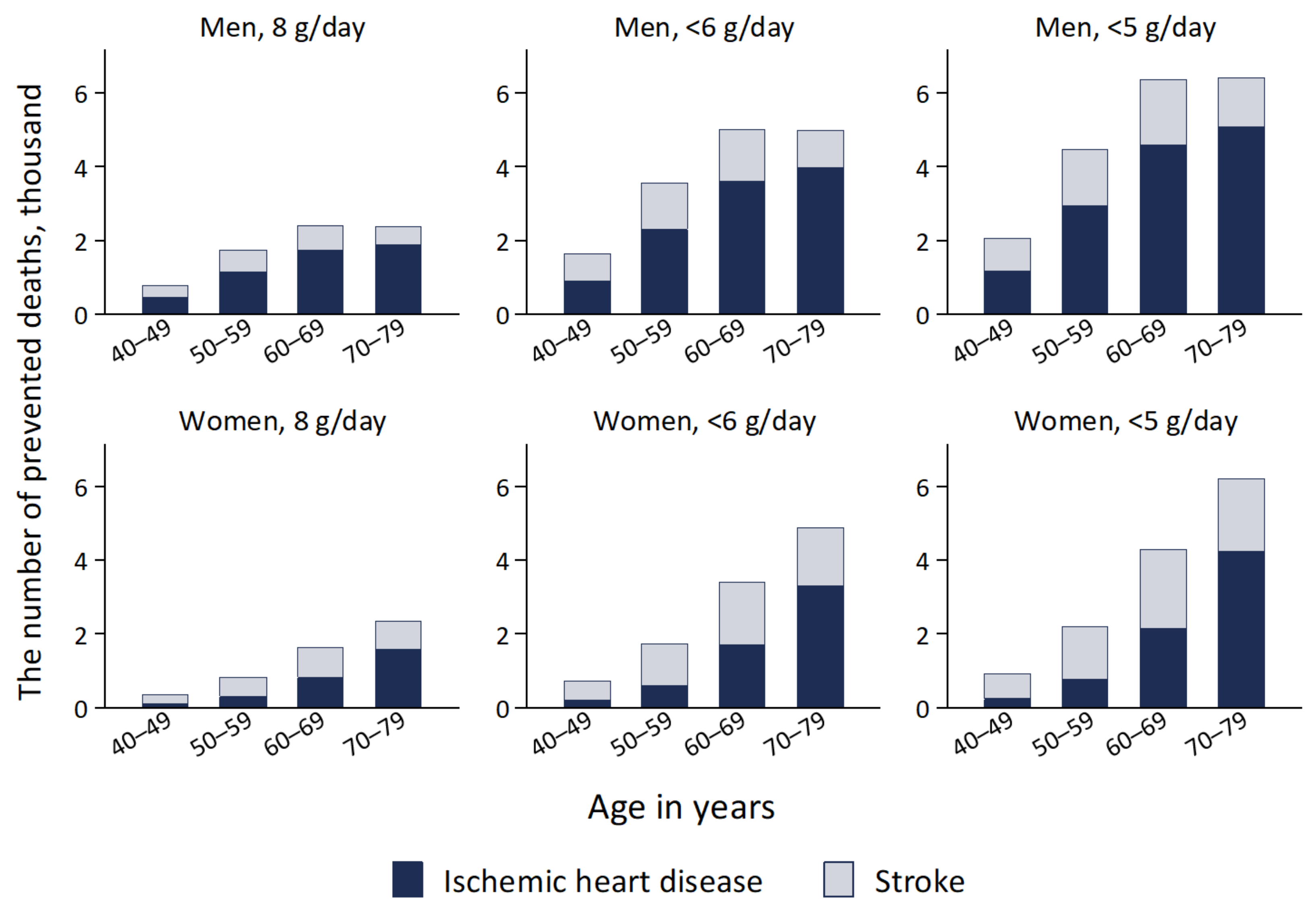
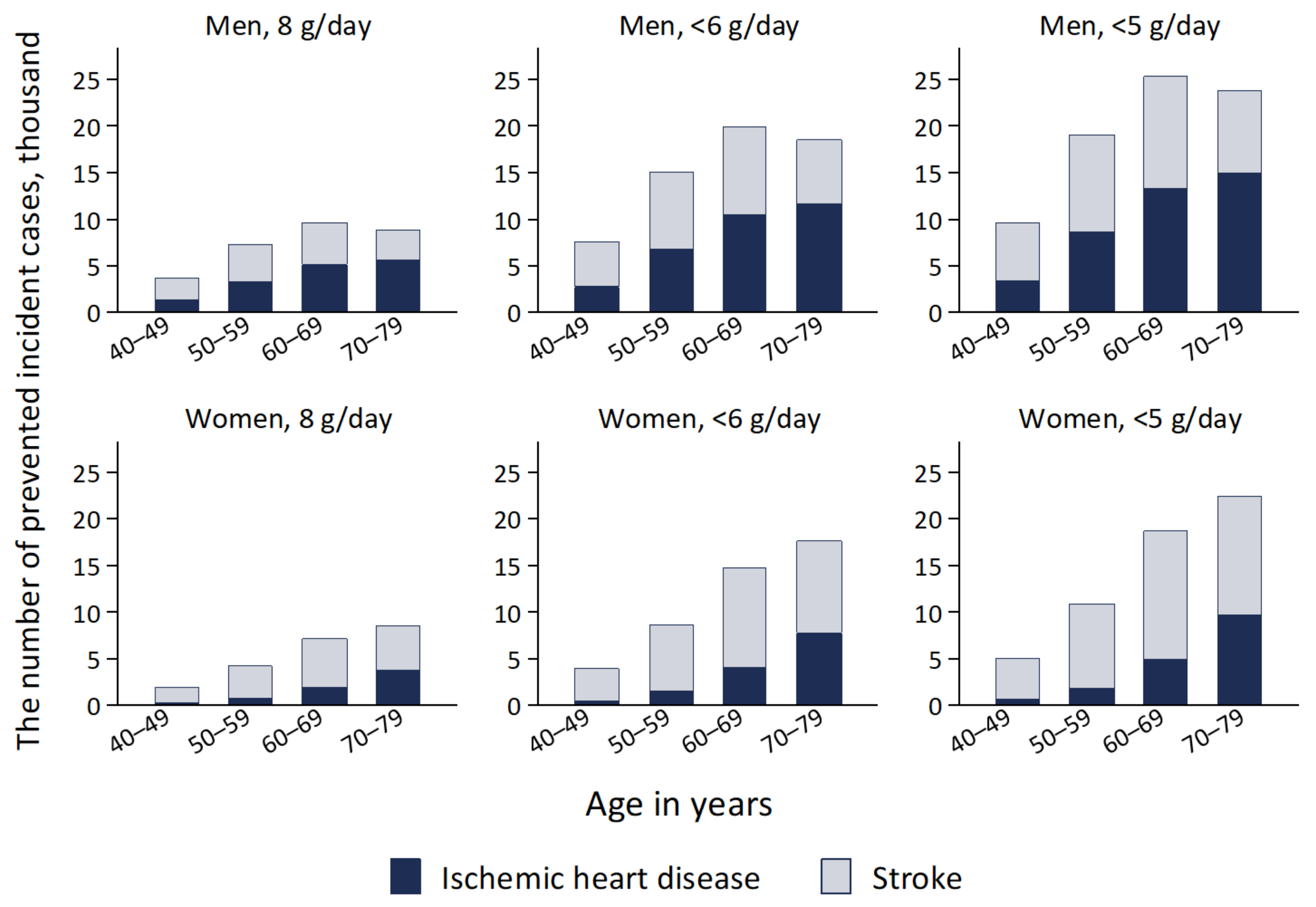
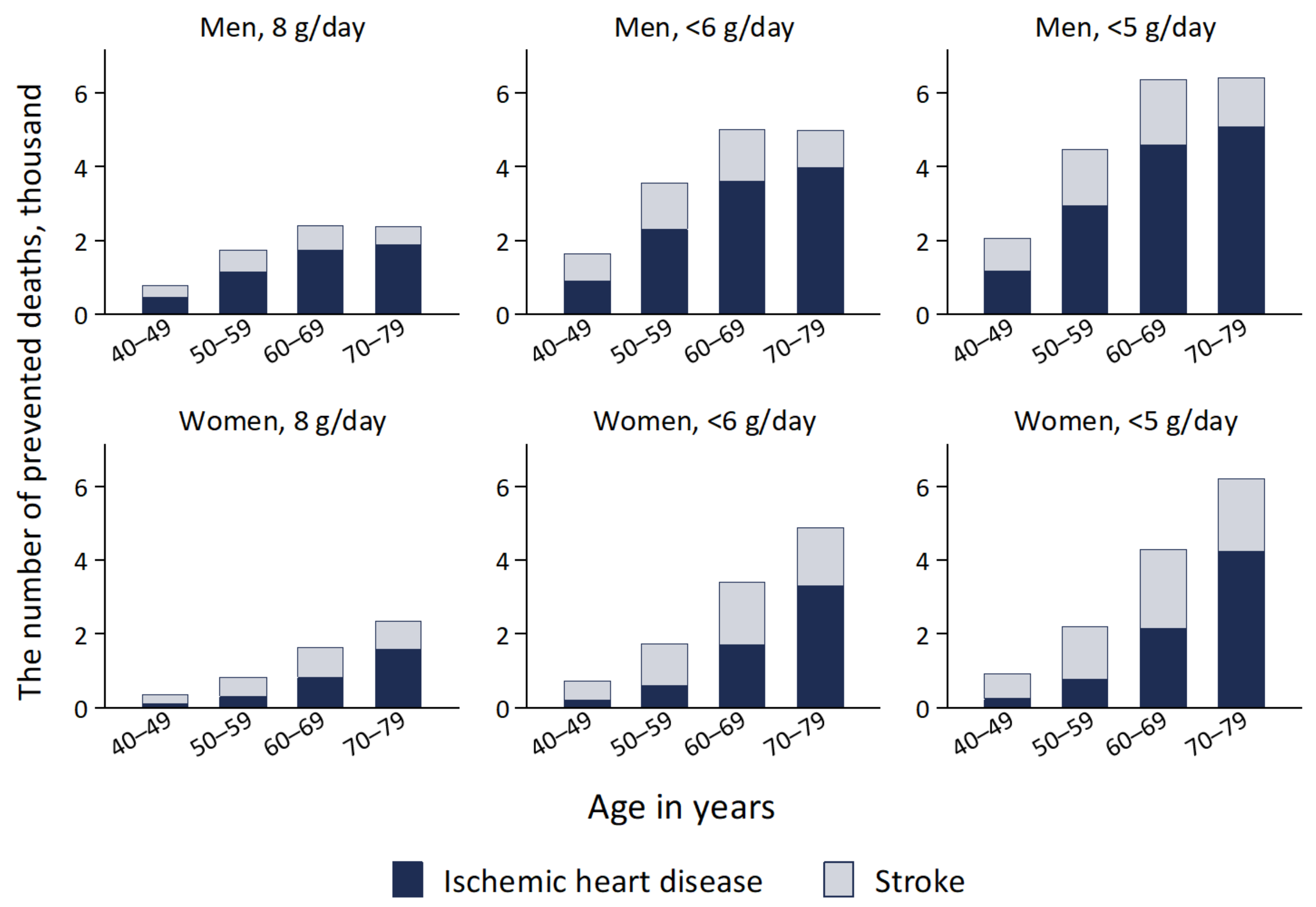
3.2. Health Gains by Achieving Dietary Salt Reduction Targets
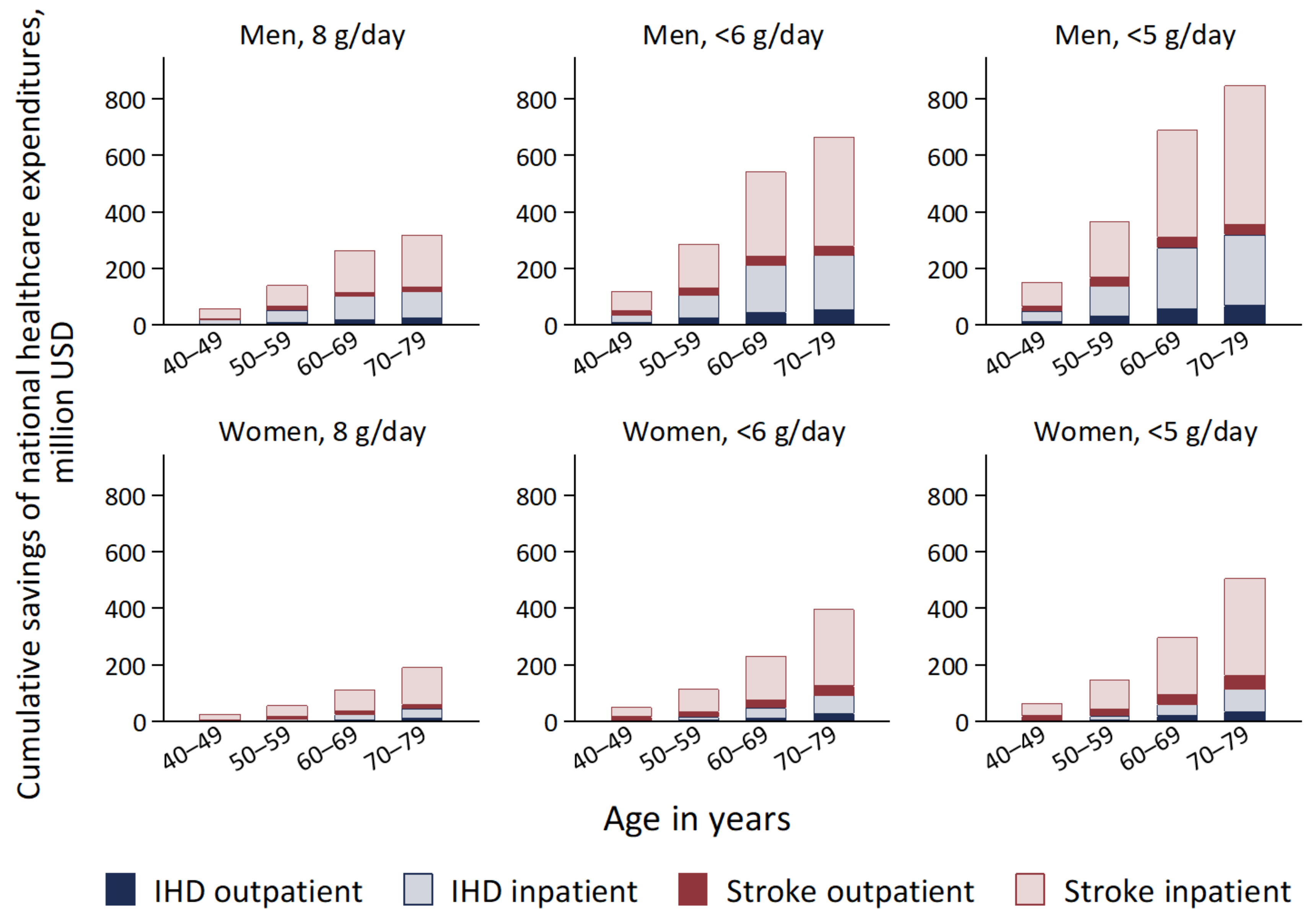
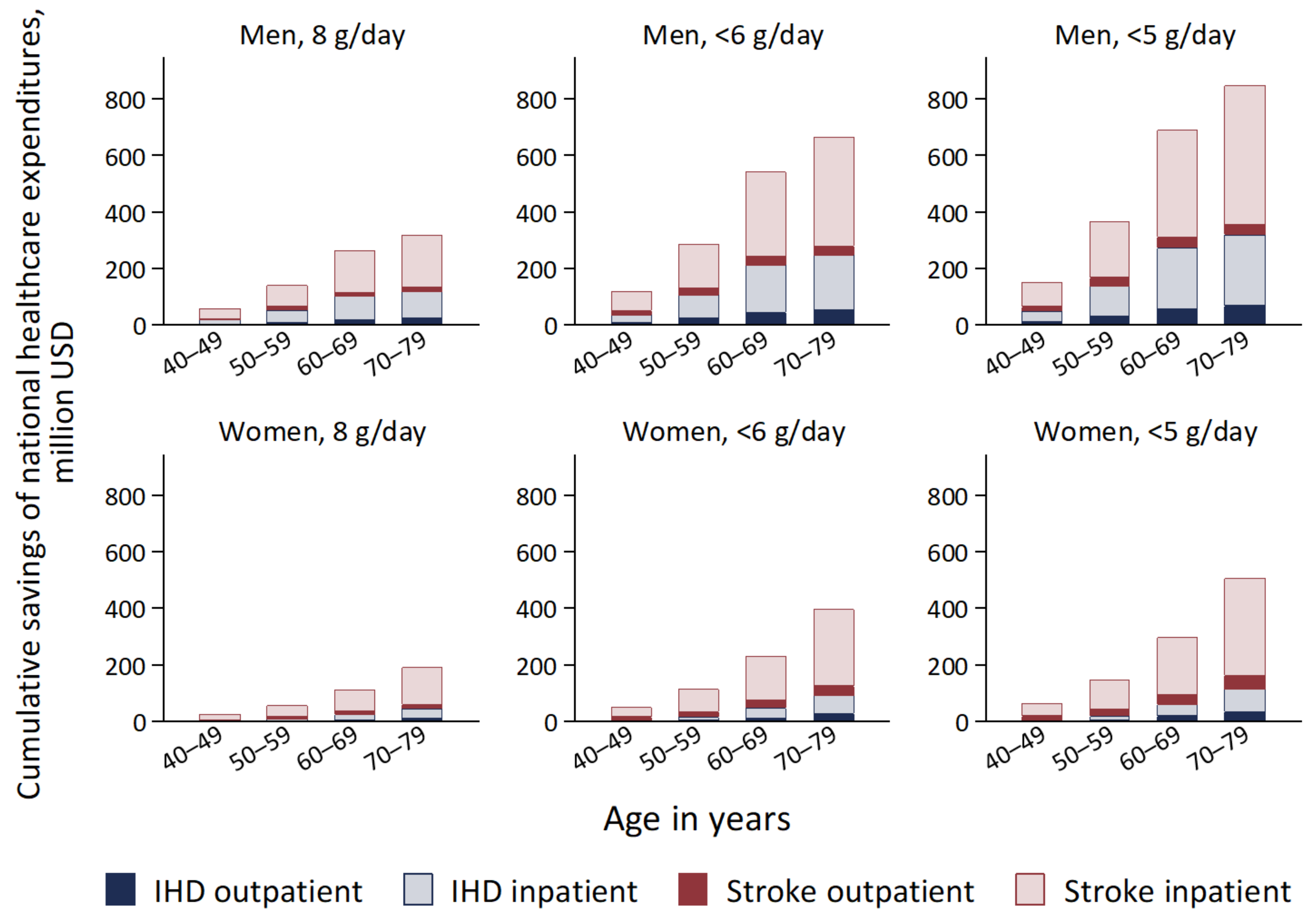
3.3. National Healthcare Expenditures Saved by Achieving Dietary Salt Reduction Targets
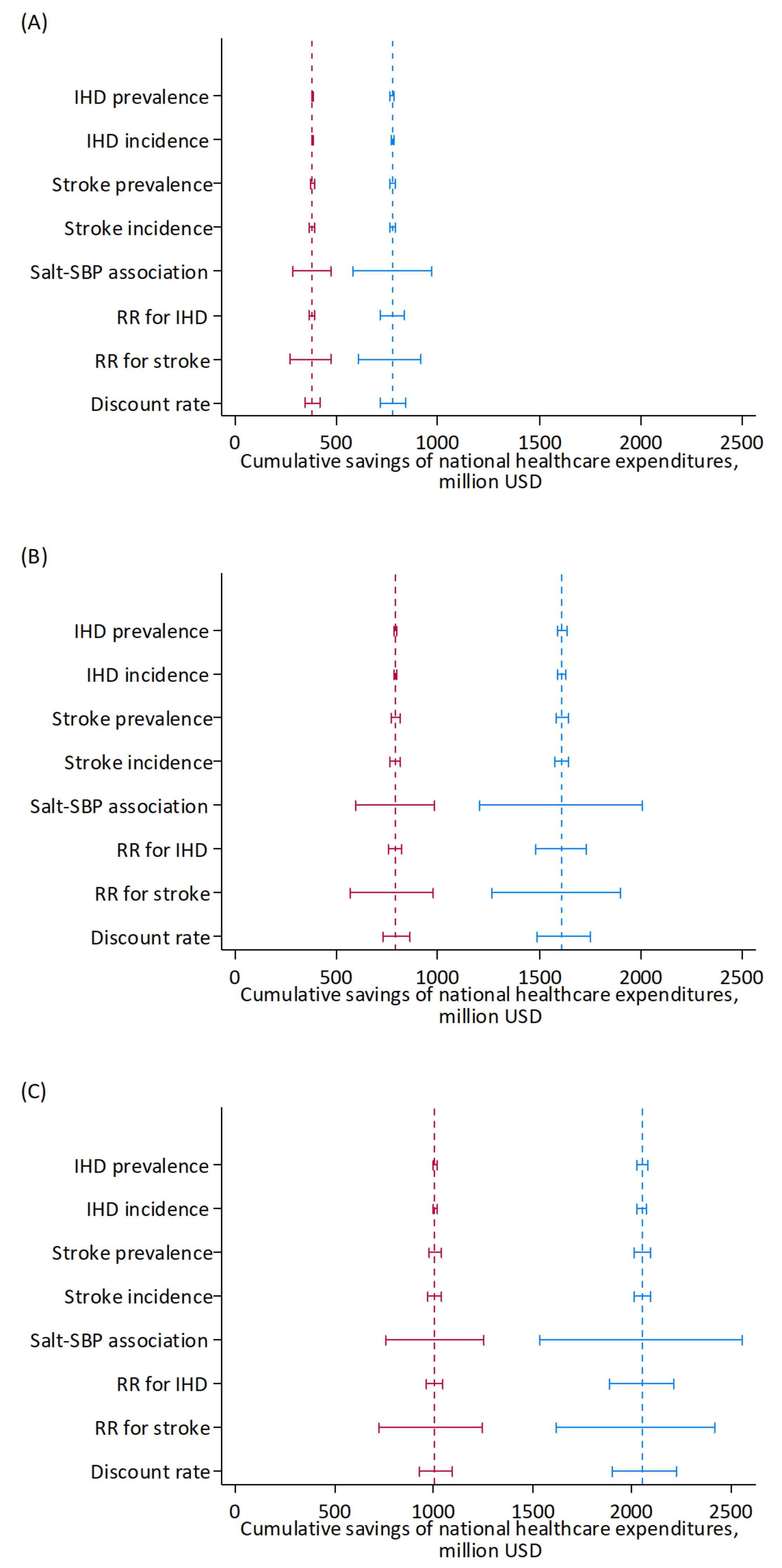
3.4. Sensitivity Analyses
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Powles, J.; Fahimi, S.; Micha, R.; Khatibzadeh, S.; Shi, P.; Ezzati, M.; Engell, R.E.; Lim, S.S.; Danaei, G.; Mozaffarian, D.; et al. Global, regional and national sodium intakes in 1990 and 2010: A systematic analysis of 24 h urinary sodium excretion and dietary surveys worldwide. BMJ Open 2013, 3, e003733. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guideline: Sodium Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar] [CrossRef]
- Beaglehole, R.; Bonita, R.; Horton, R.; Adams, C.; Alleyne, G.; Asaria, P.; Baugh, V.; Bekedam, H.; Billo, N.; Casswell, S.; et al. Priority actions for the non-communicable disease crisis. Lancet 2011, 377, 1438–1447. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Murray, C.J.L.; Lauer, J.A.; Hutubessy, R.C.W.; Niessen, L.; Tomijima, N.; Rodgers, A.; Lawes, C.M.M.; Evans, D.B. Effectiveness and costs of interventions to lower systolic blood pressure and cholesterol: A global and regional analysis on reduction of cardiovascular-disease risk. Lancet 2003, 361, 717–725. [Google Scholar] [CrossRef]
- Asaria, P.; Chisholm, D.; Mathers, C.; Ezzati, M.; Beaglehole, R. Chronic disease prevention: Health effects and financial costs of strategies to reduce salt intake and control tobacco use. Lancet 2007, 370, 2044–2053. [Google Scholar] [CrossRef]
- Bibbins-Domingo, K.; Chertow, G.M.; Coxson, P.G.; Moran, A.; Lightwood, J.M.; Pletcher, M.J.; Goldman, L. Projected effect of dietary salt reductions on future cardiovascular disease. N. Engl. J. Med. 2010, 362, 590–599. [Google Scholar] [CrossRef]
- Smith-Spangler, C.M.; Juusola, J.L.; Enns, E.A.; Owens, D.K.; Garber, A.M. Population strategies to decrease sodium intake and the burden of cardiovascular disease: A cost-effectiveness analysis. Ann. Intern. Med. 2010, 152, 481–487. [Google Scholar] [CrossRef]
- Martikainen, J.A.; Soini, E.J.; Laaksonen, D.E.; Niskanen, L. Health economic consequences of reducing salt intake and replacing saturated fat with polyunsaturated fat in the adult Finnish population: Estimates based on the FINRISK and FINDIET studies. Eur. J. Clin. Nutr. 2011, 65, 1148–1155. [Google Scholar] [CrossRef]
- Nghiem, N.; Blakely, T.; Cobiac, L.J.; Pearson, A.L.; Wilson, N. Health and economic impacts of eight different dietary salt reduction interventions. PLoS ONE 2015, 10, e0123915. [Google Scholar] [CrossRef]
- Wang, M.; Moran, A.E.; Liu, J.; Coxson, P.G.; Penko, J.; Goldman, L.; Bibbins-Domingo, K.; Zhao, D. Projected Impact of Salt Restriction on Prevention of Cardiovascular Disease in China: A Modeling Study. PLoS ONE 2016, 11, e0146820. [Google Scholar] [CrossRef] [PubMed]
- Webb, M.; Fahimi, S.; Singh, G.M.; Khatibzadeh, S.; Micha, R.; Powles, J.; Mozaffarian, D. Cost effectiveness of a government supported policy strategy to decrease sodium intake: Global analysis across 183 nations. BMJ (Clin. Res. Ed.) 2017, 356, i6699. [Google Scholar] [CrossRef]
- Aminde, L.N.; Phung, H.N.; Phung, D.; Cobiac, L.J.; Veerman, J.L. Dietary Salt Reduction, Prevalence of Hypertension and Avoidable Burden of Stroke in Vietnam: Modelling the Health and Economic Impacts. Front. Public Health 2021, 9, 682975. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Ikeda, N.; Sugiyama, T.; Nomura, M.; Yoshita, K.; Nishi, N. Use of simulation models in health economic evaluation studies of dietary salt-reduction policies for cardiovascular disease prevention. Nihon Koshu Eisei Zasshi 2021, 68, 631–643. [Google Scholar] [CrossRef] [PubMed]
- Brown, I.J.; Tzoulaki, I.; Candeias, V.; Elliott, P. Salt intakes around the world: Implications for public health. Int. J. Epidemiol. 2009, 38, 791–813. [Google Scholar] [CrossRef]
- Saito, A.; Imai, S.; Htun, N.C.; Okada, E.; Yoshita, K.; Yoshiike, N.; Takimoto, H. The trends in total energy, macronutrients and sodium intake among Japanese: Findings from the 1995–2016 National Health and Nutrition Survey. Br. J. Nutr. 2018, 120, 424–434. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. The National Health and Nutrition Survey in Japan, 2019; Ministry of Health, Labour and Welfare: Tokyo, Japan, 2020.
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019) Results. Available online: https://vizhub.healthdata.org/gbd-results/ (accessed on 25 July 2022).
- Ministry of Health, Labour and Welfare. Overview of National Medical Care Expenditure. 2019. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/k-iryohi/19/index.html (accessed on 13 April 2022).
- Statistics Bureau of Japan, Ministry of Internal Affairs and Communications. Current Population Estimates as of 1 October 2021. Available online: https://www.stat.go.jp/english/data/jinsui/2021np/index.html (accessed on 3 August 2022).
- Ministry of Health, Labour and Welfare. A Basic Direction for Comprehensive Implementation of National Health Promotion. Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-10900000-Kenkoukyoku/0000047330.pdf (accessed on 25 July 2022).
- Japanese Society of Hypertension Committee for Guidelines for the Management of Hypertension. Guidelines for the Management of Hypertension 2019; Japanese Society of Hypertension: Tokyo, Japan, 2019. [Google Scholar]
- Ito, S.; Sasaki, S. Dietary Reference Intakes for Japanese, 2020; Daiichi Shuppan, Co.: Tokyo, Japan, 2020. [Google Scholar]
- TreeAge Software, Inc. TreeAge Pro 2021, R1; TreeAge Software: Williamstown, MA, USA, 2021. [Google Scholar]
- Statistics Bureau of Japan, Ministry of Internal Affairs and Communications. Current Population Estimates as of 1 October 2019. Available online: https://www.stat.go.jp/english/data/jinsui/2019np/index.html (accessed on 4 February 2022).
- Director-General for Statistics and Information Policy, Ministry of Health, Labour and Welfare. Vital Statistics of Japan 2019; Ministry of Health, Labour and Welfare: Tokyo, Japan, 2021.
- Statistics Bureau of Japan, Ministry of Internal Affairs and Communications. Population and Households of Japan: Final Report of the 2010 Population Census; Ministry of Internal Affairs and Communications: Tokyo, Japan, 2014.
- Uchiyama, S.; Shibata, Y.; Hirabayashi, T.; Mihara, B.; Hamashige, N.; Kitagawa, K.; Goto, S.; Origasa, H.; Shimada, K.; Kobayashi, H.; et al. Risk factor profiles of stroke, myocardial infarction, and atrial fibrillation: A Japanese Multicenter Cooperative Registry. J. Stroke Cereb. Dis 2010, 19, 190–197. [Google Scholar] [CrossRef]
- Takashima, N.; Arima, H.; Kita, Y.; Fujii, T.; Miyamatsu, N.; Komori, M.; Sugimoto, Y.; Nagata, S.; Miura, K.; Nozaki, K. Incidence, Management and Short-Term Outcome of Stroke in a General Population of 1.4 Million Japanese―Shiga Stroke Registry―. Circ. J. 2017, 81, 1636–1646. [Google Scholar] [CrossRef]
- Rumana, N.; Kita, Y.; Turin, T.C.; Nakamura, Y.; Takashima, N.; Ichikawa, M.; Sugihara, H.; Morita, Y.; Hirose, K.; Kawakami, K.; et al. Acute case-fatality rates of stroke and acute myocardial infarction in a Japanese population: Takashima stroke and AMI registry, 1989–2005. Int. J. Stroke 2014, 9 (Suppl. A100), 69–75. [Google Scholar] [CrossRef]
- Law, M.R.; Frost, C.D.; Wald, N.J. By how much does dietary salt reduction lower blood pressure? I—Analysis of observational data among populations. BMJ 1991, 302, 811–815. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health, Labour and Welfare. Survey on Medical Care Benefit. 2019. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00450389&tstat=000001044924&cycle=0&tclass1=000001044945&tclass2=000001156339&tclass3val=0 (accessed on 7 February 2022).
- Ministry of Health, Labour and Welfare. Survey on Prescription Drug Expenditure. 2019. Available online: https://www.mhlw.go.jp/bunya/iryouhoken/database/zenpan/cyouzai_doukou.html (accessed on 10 February 2022).
- Ikeda, N.; Takimoto, H.; Imai, S.; Miyachi, M.; Nishi, N. Data Resource Profile: The Japan National Health and Nutrition Survey (NHNS). Int. J. Epidemiol. 2015, 44, 1842–1849. [Google Scholar] [CrossRef]
- Ministry of Education, Culture, Sports, Science, and Technology. Standard Tables of Food Composition in Japan; Seventh Revised Edition; Ministry of Education, Culture, Sports, Science, and Technology: Tokyo, Japan, 2015. Available online: https://www.mext.go.jp/a_menu/syokuhinseibun/1365297.htm (accessed on 24 February 2022).
- International Monetary Fund. IMF Data Access to Macroeconomic & Financial Data. Available online: https://data.imf.org/?sk=388dfa60-1d26-4ade-b505-a05a558d9a42 (accessed on 4 February 2022).
- Fukuda, T.; Shiroiwa, T.; Ikeda, S.; Igarashi, A.; Akazawa, M.; Ishida, H.; Noto, S.; Saito, S.; Sakamaki, H.; Shimozuma, K.; et al. Guideline for economic evaluation of healthcare in Japan. J. Natl. Inst. Public Health 2013, 62, 625–640. [Google Scholar]
- GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Mo, X.; Gai, R.T.; Sawada, K.; Takahashi, Y.; Cox, S.E.; Nakayama, T.; Mori, R. Coronary heart disease and stroke disease burden attributable to fruit and vegetable intake in Japan: Projected DALYS to 2060. BMC Public Health 2019, 19, 707. [Google Scholar] [CrossRef]
- Tanaka, S.; Yoneoka, D.; Ishizuka, A.; Ueda, P.; Nakamura, K.; Uneyama, H.; Hayashi, N.; Shibuya, K.; Nomura, S. Projections of disability-adjusted life years for major diseases due to a change in vegetable intake in 2017–2040 in Japan. BMC Public Health 2021, 21, 770. [Google Scholar] [CrossRef]
- Yoneoka, D.; Nomura, S.; Tanaka, S.; Ishizuka, A.; Peter, U.; Rauniyar, S.K.; Nakamura, K.; Uneyama, H.; Hayashi, N.; Shibuya, K. Prediction of disability-adjusted life years for diseases due to low fruit intake in 2017–2040 in Japan. Public Health Nutr. 2021, 24, 3156–3166. [Google Scholar] [CrossRef]
- Nomura, S.; Yoneoka, D.; Tanaka, S.; Ishizuka, A.; Ueda, P.; Nakamura, K.; Uneyama, H.; Hayashi, N.; Shibuya, K. Forecasting disability-adjusted life years for chronic diseases: Reference and alternative scenarios of salt intake for 2017–2040 in Japan. BMC Public Health 2020, 20, 1475. [Google Scholar] [CrossRef]
- Matsumoto, M.; Tajima, R.; Fujiwara, A.; Yuan, X.; Okada, E.; Takimoto, H. Trends in dietary salt sources in Japanese adults: Data from the 2007-2019 National Health and Nutrition Survey. Br. J. Nutr 2022, 1–14. [Google Scholar] [CrossRef]
- Nishi, N.; Ikeda, N.; Sugiyama, T.; Kurotani, K.; Miyachi, M. Simulating the Impact of Long-Term Care Prevention Among Older Japanese People on Healthcare Costs From 2020 to 2040 Using System Dynamics Modeling. Front. Public Health 2020, 8, 592471. [Google Scholar] [CrossRef]
- Ikeda, N.; Gakidou, E.; Hasegawa, T.; Murray, C.J. Understanding the decline of mean systolic blood pressure in Japan: An analysis of pooled data from the National Nutrition Survey, 1986–2002. Bull. World Health Organ. 2008, 86, 978–988. [Google Scholar] [CrossRef]
- FAO; WHO. Sustainable Healthy Diets: Guiding Principles; FAO and WHO: Rome, Italy, 2019. [Google Scholar]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Input Parameters | Data Sources | Values |
|---|---|---|
| Total population | Population Estimates [27] | Table S1 |
| Mean dietary salt intake | National Health and Nutrition Survey in Japan, 2019 [19] | Table S1 |
| Mean SBP | National Health and Nutrition Survey in Japan, 2019 [19] | Table S1 |
| Prevalence rates of IHD and stroke | Global Burden of Disease Study 2019 [20] | Table S2 |
| Incidence rates of IHD and stroke | Global Burden of Disease Study 2019 [20] | Table S2 |
| Mortality rates of IHD, stroke, and all causes | Global Burden of Disease Study 2019 [20] | Table S2 |
| Proportion of first-ever events in incident cases | ||
| IHD | Japan Thrombosis Registry for Atrial Fibrillation, Coronary, or Cerebrovascular Events (J-TRACE) [30] | Table S3 |
| Stroke | Shiga Stroke Registry [31] | Table S3 |
| 28-day case fatality rates of IHD and stroke | Takashima Cardiovascular Disease Registration System [32] | Table S3 |
| Changes in SBP associated with changes in salt intake | Analysis of observational studies in 24 communities [33] | Table S4 |
| Relative risks for IHD and stroke associated with SBP | Global Burden of Disease Study 2019 [20] | Table S4 |
| National healthcare expenditures | Survey on Medical Care Benefit, 2019 [34], Survey on Prescription Drug Expenditure, 2019 [35] | Table S5 |
| Sex, Age (Years) | Population, 2019 | Incidence | Deaths | National Healthcare Expenditures, Million USD | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IHD | Stroke | IHD | Stroke | Outpatient | Inpatient | ||||||||
| No. | No. | (%) | No. | (%) | No. | (%) | No. | (%) | IHD | Stroke | IHD | Stroke | |
| Men | |||||||||||||
| 40–79 | 32,795,000 | 1,322,550 | (4.0) | 1,151,035 | (3.5) | 453,635 | (1.4) | 171,504 | (0.5) | 24,671 | 21,160 | 20,001 | 36,052 |
| 40–49 | 9,373,000 | 125,027 | (1.3) | 201,224 | (2.1) | 42,884 | (0.5) | 29,982 | (0.3) | 1504 | 2060 | 1314 | 2798 |
| 50–59 | 8,160,000 | 263,831 | (3.2) | 292,985 | (3.6) | 90,494 | (1.1) | 43,655 | (0.5) | 3560 | 3814 | 3227 | 5418 |
| 60–69 | 7,930,000 | 403,995 | (5.1) | 340,586 | (4.3) | 138,570 | (1.7) | 50,747 | (0.6) | 7642 | 6298 | 6416 | 10,520 |
| 70–79 | 7,332,000 | 529,697 | (7.2) | 316,240 | (4.3) | 181,686 | (2.5) | 47,120 | (0.6) | 11,965 | 8989 | 9043 | 17,317 |
| Women | |||||||||||||
| 40–79 | 34,160,000 | 678,243 | (2.0) | 1,444,273 | (4.2) | 293,679 | (0.9) | 226,751 | (0.7) | 11,514 | 21,908 | 5448 | 25,479 |
| 40–49 | 9,147,000 | 25,083 | (0.3) | 170,857 | (1.9) | 10,861 | (0.1) | 26,825 | (0.3) | 603 | 1855 | 160 | 1842 |
| 50–59 | 8,118,000 | 64,238 | (0.8) | 291,997 | (3.6) | 27,815 | (0.3) | 45,844 | (0.6) | 1174 | 3608 | 439 | 3267 |
| 60–69 | 8,302,000 | 171,860 | (2.1) | 443,201 | (5.3) | 74,415 | (0.9) | 69,582 | (0.8) | 2953 | 6421 | 1410 | 6252 |
| 70–79 | 8,593,000 | 417,062 | (4.9) | 538,218 | (6.3) | 180,588 | (2.1) | 84,500 | (1.0) | 6783 | 10,024 | 3439 | 14,118 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ikeda, N.; Yamashita, H.; Hattori, J.; Kato, H.; Yoshita, K.; Nishi, N. Reduction of Cardiovascular Events and Related Healthcare Expenditures through Achieving Population-Level Targets of Dietary Salt Intake in Japan: A Simulation Model Based on the National Health and Nutrition Survey. Nutrients 2022, 14, 3606. https://doi.org/10.3390/nu14173606
Ikeda N, Yamashita H, Hattori J, Kato H, Yoshita K, Nishi N. Reduction of Cardiovascular Events and Related Healthcare Expenditures through Achieving Population-Level Targets of Dietary Salt Intake in Japan: A Simulation Model Based on the National Health and Nutrition Survey. Nutrients. 2022; 14(17):3606. https://doi.org/10.3390/nu14173606
Chicago/Turabian StyleIkeda, Nayu, Hitomi Yamashita, Jun Hattori, Hiroki Kato, Katsushi Yoshita, and Nobuo Nishi. 2022. "Reduction of Cardiovascular Events and Related Healthcare Expenditures through Achieving Population-Level Targets of Dietary Salt Intake in Japan: A Simulation Model Based on the National Health and Nutrition Survey" Nutrients 14, no. 17: 3606. https://doi.org/10.3390/nu14173606
APA StyleIkeda, N., Yamashita, H., Hattori, J., Kato, H., Yoshita, K., & Nishi, N. (2022). Reduction of Cardiovascular Events and Related Healthcare Expenditures through Achieving Population-Level Targets of Dietary Salt Intake in Japan: A Simulation Model Based on the National Health and Nutrition Survey. Nutrients, 14(17), 3606. https://doi.org/10.3390/nu14173606