Abstract
Three metabolite patterns have previously shown prospective inverse associations with the risk of aggressive prostate cancer within the European Prospective Investigation into Cancer and Nutrition (EPIC). Here, we investigated dietary and lifestyle correlates of these three prostate cancer-related metabolite patterns, which included: 64 phosphatidylcholines and three hydroxysphingomyelins (Pattern 1), acylcarnitines C18:1 and C18:2, glutamate, ornithine, and taurine (Pattern 2), and 8 lysophosphatidylcholines (Pattern 3). In a two-stage cross-sectional discovery (n = 2524) and validation (n = 518) design containing 3042 men free of cancer in EPIC, we estimated the associations of 24 dietary and lifestyle variables with each pattern and the contributing individual metabolites. Associations statistically significant after both correction for multiple testing (False Discovery Rate = 0.05) in the discovery set and at p < 0.05 in the validation set were considered robust. Intakes of alcohol, total fish products, and its subsets total fish and lean fish were positively associated with Pattern 1. Body mass index (BMI) was positively associated with Pattern 2, which appeared to be driven by a strong positive BMI-glutamate association. Finally, both BMI and fatty fish were inversely associated with Pattern 3. In conclusion, these results indicate associations of fish and its subtypes, alcohol, and BMI with metabolite patterns that are inversely associated with risk of aggressive prostate cancer.
1. Introduction
Metabolomics is a rapidly evolving field, which involves the measurement of multiple metabolites with an aim of establishing biomarkers of exposure and disease risk [1,2]. Several observational studies have measured prediagnostic blood metabolites in order to identify novel risk factors and pathways in prostate cancer aetiology [1,2,3,4], including analyses of metabolite profiles, as well as specific analytes. In a previous case-control study nested within the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort, three patterns (treelet components) were identified and assessed in relation to risk for prostate cancer [1]; a metabolite pattern of 64 diacyl- and acyl-alkyl phosphatidylcholines and three hydroxysphingomyelins, as well as a metabolite pattern of two acylcarntines, glutamate, ornithine, and taurine, were both found to be inversely associated with risk of advanced and aggressive prostate cancer. Furthermore, a metabolite pattern of eight lysophosphatidylcholines was also observed to be inversely associated with risk of advanced prostate cancer and prostate cancer death [1]. Data from other cohorts have also supported inverse associations of glycerophospholipids [3] and acylcarnitine C18:2 [4] with risk of aggressive prostate cancer.
Blood metabolite concentrations are affected by both internal and external factors, including modifiable factors, such as diet and body mass index (BMI) [5,6]. Thus, a better understanding of how these factors are associated with prostate cancer-related metabolite patterns might offer insights into possible avenues for prostate cancer prevention.
This cross-sectional study nested in the EPIC cohort aimed to investigate associations of dietary variables and BMI with metabolite patterns previously found to be inversely associated with more aggressive prostate cancer subtypes.
2. Materials and Methods
2.1. Study Population
EPIC is a multi-center prospective cohort study, which recruited approximately 500,000 Europeans, including 153,457 men, between 1992 and 2000. The current analyses include men mainly aged between the ages of 35 and 70 years at recruitment from 19 centers in seven countries (Denmark, Germany, Italy, Netherlands, Spain, Sweden and United Kingdom). 139,600 of the men provided a blood sample. All participants in the EPIC study provided written informed consent, and the study was approved by the ethics committees of the International Agency for Research on Cancer (IARC) and all participating centers [7].
Men were eligible for the current study if they (1) were free of cancer (except non-melanoma skin cancer) at baseline; (2) had a known date of blood collection; (3) had been included as control participants in one of four case-control studies on metabolite concentrations and cancer risk nested within the EPIC cohort (on prostate [1], colorectal [8], kidney [9], and liver cancer [10]), hereafter referred to as sub-studies, with available blood concentrations of all of the metabolites included in the metabolite patterns that were previously found to be associated with more aggressive prostate cancer subtypes; and (4) had blood samples that were included in an analytical batch that had at least 10 samples, to ensure proper normalization of metabolite concentrations. Thus, data for 3198 men were available for this study.
2.2. Laboratory Measurements
For participants from Germany, Italy, the Netherlands, Spain and the UK, biological samples are stored at IARC in plastic straws at −196 °C (details published elsewhere) [7]. In Sweden and Denmark, blood samples are stored in tubes in local repositories; in Sweden, the samples are kept in freezers at −80 °C, and in Denmark in nitrogen vapor at −150 °C [7].
Regardless of sub-study, all samples were previously assayed at IARC in Lyon, France using the AbsoluteIDQ® p180 Kit (Biocrates Life Sciences AG, Innsbruck, Austria), and following the procedure recommended by the vendor. To quantify metabolites, liquid chromatography mass spectrometry (LC-MS) was applied. All samples were assayed using one LC instrument (Agilent 1290, Santa Clara, CA, USA) coupled with one of two different triple quadrupole MS instruments (Triple Quad 4500, AB Sciex, Framingham, MA, USA for prostate and colorectal cancer [1,8] and Q-Trap 5500, AB Sciex, MA for liver and kidney cancer [10,11]; Supplementary Table S1). Of note, within each sub-study a single pair of LC-MS instruments was used for all samples [12]. 118 common metabolites were measured across all sub-studies [12].
Metabolite values outside the measurable range, including metabolite values below the batch-specific limit of detection (LOD), below the kit-specific lower limit of quantification (LLOQ), and above the kit-specific upper limit of quantification (ULOQ), were imputed to LOD/2, LLOQ/2, and ULOQ, respectively.
2.3. Diet, BMI, and Covariate Data
Detailed information on dietary, lifestyle, and anthropometric data was gathered at recruitment, previously described in Riboli et al. [7]. In order to determine usual dietary intakes, center- or country-specific validated dietary questionnaires covering the previous 12 months were used [13]. The dietary variables (continuous, consumption in g/day) investigated in this study were intakes of total dairy (sum of milk, cheese, and yogurt), milk, cheese, yogurt, eggs, red meat, poultry, processed meat, total fish products (refers to fish and shellfish combined), total fish (subset of total fish products), fatty fish (subcategory of total fish), lean fish (subcategory of total fish), fats and oils (sum of butter, margarine, and vegetable oils), butter, margarine, vegetable oils, total vegetables (sum of leafy, root, and fruiting vegetables), leafy vegetables, root vegetables, fruiting vegetables, total fruit, cereals and cereal products, and alcohol. In order to reflect average daily consumption, increments were chosen for each dietary variable to represent typical intakes in an average European male population (Table 1).
Table 1.
Increments for each dietary variable.
BMI (continuous, kg/m2) was also examined as a possible correlate of the metabolite patterns, calculated from weight and height (measured, except self-reported in some participants in the EPIC-Oxford cohort) [8].
2.4. Statistical Analysis
2.4.1. Participant Characteristics
Participants’ characteristics at baseline were summarized using frequencies for categorical variables and mean (standard deviation) for continuous variables.
2.4.2. Normalization of Metabolite Concentrations
A statistical pipeline has been developed for the EPIC metabolomics data [12] and was applied in this analysis to the raw metabolite concentrations. Metabolites with more than 25% missing values in each study were removed. For the remaining missing data, if no more than 50% were missing in the batch, values were imputed to the batch-specific median (of the considered metabolite); if more than 50% were missing in the batch, they were otherwise imputed to the median of the medians of the measured values in the other batches. Log-transformed concentrations of the metabolites were then normalized using linear mixed-effects models to remove unwanted variations due to study, batch, and center; study and batch were included as random effects and center was included as a fixed effect in the models. Corrected metabolite concentrations analyzed in this work correspond to residuals from the individual models. This pipeline was shown to be efficient in removing unwanted variability and improving the comparability of measurements acquired across the different cancer-specific studies [12].
2.4.3. Metabolite Patterns
Patterns in metabolite profiles were previously identified using treelet transform in an EPIC nested case-control study of prostate cancer [1]. In summary, treelet transform is a linear dimension-reduction method aiming at summarizing the metabolite variables into fewer latent variables that best capture the observed variation in the overall set of metabolites [20,21]. Schmidt et al. identified three treelet components (henceforth referred to in the text as metabolite patterns, which together explained 31.4% of the total variance in metabolite concentrations), all of which were found to have an inverse association with advanced and/or aggressive prostate cancer risk. The first metabolite pattern (Pattern 1) had positive loadings on diacyl-phosphatidylcholines (PC aa; n = 31) and acyl-alkyl-phosphatidylcholines (PC ae; n = 33), as well as three hydroxysphingomyelins (SM(OH)): C14:1, C16:1, and C22:2. The second metabolite pattern (Pattern 2) had positive loadings on acylcarnitines C18:1 and C18:2, and the amino acids glutamate, ornithine, and taurine. Finally, the third metabolite pattern (Pattern 3) had positive loadings on eight lysophosphatidylcholines (lyso PC a): C16:0, C16:1, C17:0, C18:0, C18:1, C18:2, C20:3, and C20:4 (Table 2) [1]. Each metabolite pattern was scaled to units of one standard deviation (SD), as done in the previous study [1].
Table 2.
Metabolite Patterns and their loadings.
2.4.4. Correlates of Metabolites
After excluding participants with missing values for time at blood collection (78), fasting status (65), energy intake (2), BMI (23), and level of education (31), the current cross-sectional analysis included data from 3042 participants. These data were subsequently split into a discovery set (n = 2524; 83% of the population) and a validation set (n = 518; 17.0% of the population). Specifically, the discovery set included controls from the prostate cancer sub-study that were used in the identification of metabolite patterns, while the validation set comprised controls from the other three sub-studies (kidney [9], liver [10], and colorectal [8] cancer). A discovery-validation set design was chosen to both reduce the in-sample bias from the samples used to determine patterns, and to afford an external validation for any associations that appeared statistically significant in initial analyses.
First, analyses were run in the discovery set. For each of the three metabolite patterns and each dietary or lifestyle variable, a linear regression model was run with the metabolite pattern as the dependent variable. Models were adjusted for age at blood collection (continuous), time of day of blood collection (continuous), fasting status at blood collection (<3 h since last meal, 3–6 h, >6 h, and missing), baseline education level (primary/no schooling, secondary, professional/technical, university/higher, not specified, and missing), physical activity (Cambridge index [22]: inactive, moderately inactive, moderately active, active, and missing), smoking status (never, former, current, and missing), energy (continuous, kcal/day) and alcohol intakes (continuous, g/day), and BMI (continuous, kg/m2). Models that examined alcohol intake and BMI as main exposures were not adjusted for alcohol intake and BMI, respectively.
In the discovery set, to account for multiple testing, we used a Benjamini-Hochberg false discovery rate (FDR) by metabolite pattern at a 5% threshold to define statistical significance [23]. Each statistically significant association in the discovery set was re-assessed in the validation set, using the same variables and adjusted models. Results from the analyses in the validation set were not corrected for multiple testing. Associations between exposures and metabolites that passed the FDR threshold in the discovery set, and the significance threshold in the validation set (p < 0.05), were considered robust.
2.4.5. Individual Metabolite Analysis
A supplementary analysis was conducted of dietary exposures and BMI with the individual metabolites that contributed to metabolite patterns with which they were robustly associated (Supplementary Table S3). Models were adjusted as described above for the main analysis. Individual metabolite values were log-transformed. Linear regressions were run in the overall dataset (n between 2136 and 3042, depending on exposure). To account for multiple testing, dietary and lifestyle correlates of metabolites that passed the FDR of 0.05 were determined to be statistically significant.
3. Results
3.1. Participant Characteristics
Main characteristics of the participants, overall and in the discovery and validation sets, are shown in Table 3. 46.4% of men in the discovery set and 31.7% of men in the validation set were not considered fasting at blood collection (<3 h since last meal), while 32.0% and 45.7% of men in the discovery and validation sets, respectively, were fasting (>6 h since last meal). Otherwise, participant characteristics were relatively similar in the discovery and validation sets.
Table 3.
Main characteristics of men included in the analysis, overall and separately in discovery and validation sets.
3.2. Correlates of Metabolite Patterns
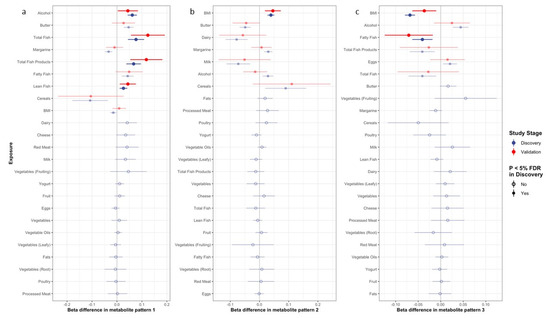
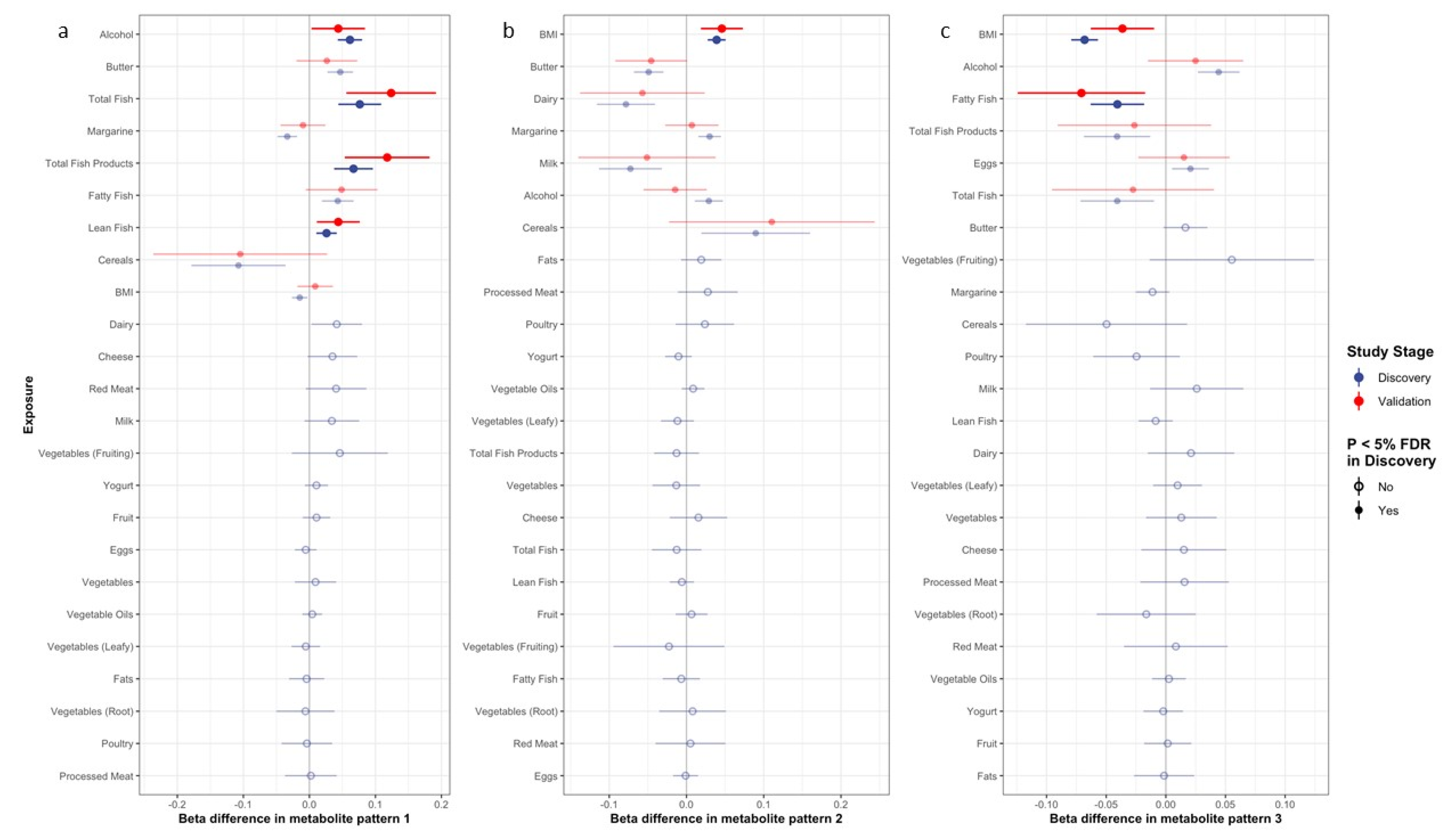
Figure 1 depicts the betas and 95% confidence intervals for associations between the metabolite patterns and selected potential correlates in the discovery and validation sets. Supplementary Table S2 shows the full results for betas, p-values, and Padj values (p-values after adjusting for multiple testing in the discovery set) for the exposure–metabolite pattern associations in the discovery and validation sets. Associations with individual metabolites are shown in Supplementary Table S3.
Figure 1.
Association of dietary and lifestyle factors with metabolite pattern 1 (a), pattern 2 (b), and pattern 3 (c). Estimates presented in bold are for dietary and lifestyle factors with both significant Padj associations in the discovery dataset (blue) and p < 0.05 in the validation dataset (red). Estimates with associations that do not pass FDR threshold are presented with hollow circles.
Of the nine exposures that passed the significance threshold after adjusting for multiple testing in the discovery set, intakes of total fish products, total fish, lean fish, and alcohol all remained statistically significantly (p < 0.05) positively associated with pattern 1 in the validation set (Figure 1a). In the analysis of individual metabolites contributing to pattern 1, the associations with the lowest p-values included alcohol with PC aa C32:1, C34:1, and C36:4, and total fish products, total fish, and lean fish with PC aa C42:2 (see Supplementary Table S3 for full results).
For metabolite pattern 2, seven exposures passed the significance threshold after multiple testing in the discovery set, though only BMI remained positively and statistically significantly associated with the metabolite pattern in the validation set (Figure 1b). This relationship appeared to be strongly driven by a strong, positive BMI-glutamate association (Supplementary Table S3).
Of the six exposures that were significant after multiple testing in the discovery set, fatty fish intake and BMI remained statistically significantly inversely associated with pattern 3 in the validation set (Figure 1c). In the analysis of individual metabolites, BMI was strongly and inversely associated with all eight lyso PCs loading on the metabolite pattern, while fatty fish was significantly inversely associated with lyso PCs C16:1, C18:0, C18:1, C20:3, and C20:4 (Supplementary Table S3).
4. Discussion
This large cross-sectional study identified several dietary factors and BMI as correlates of metabolite patterns that have previously been shown to associate inversely with more aggressive prostate cancer subtypes. The intakes of alcohol, total fish products, and its subsets total fish and lean fish, were all positively associated with a metabolite pattern with higher concentrations of 31 PC aas, 33 PC aes, and three hydroxysphingomyelins. BMI was positively associated with the second metabolite pattern of two acylcarnitines, glutamate, ornithine, and taurine, and an individual metabolite analysis showed that this was driven by a specific association with glutamate. Finally, BMI and fatty fish intake were inversely associated with scores of a third metabolite pattern of eight lyso PCs as no additional associations of dietary variables or BMI with metabolite patterns were validated.
Comparing these results to previous studies is complex; this analysis primarily investigated metabolite patterns rather than individual metabolites. Broadly in line with our results, however, positive associations of alcohol intake with some of the metabolites loading on metabolite pattern 1 (phosphatidylcholines and hydroxysphingomyelins) have previously been reported in other analyses [24,25,26,27].
Though there are limited prior studies of associations between fish intake and metabolites, a positive association between fish intake and certain phosphatidylcholines has also been previously reported in an analysis in the TwinsUK cohort [24], and in an intervention study at the University of Otago [28]. This may be partially attributed to fish being a dietary source of choline, which is a requirement for hepatic phosphatidylcholine biosynthesis [29].
The positive association between BMI and the metabolites loading on metabolite pattern 2 (driven largely by glutamate) was consistent with findings in other studies, including the Framingham Heart Study, and the Malmö Diet and Cancer Study [30]. Additionally, a Mendelian randomization analysis suggested that the positive effect of BMI on circulating glutamate may be causal [9]. Previous studies have also demonstrated that glutamate is positively linked to visceral obesity [8,9,30,31].
This study found inverse associations of fatty fish intake and BMI with pattern 3, which comprised eight lyso PCs. To date, there are still limited data available regarding the effects of diet on lyso PC concentrations. However, an 8-week sequential therapy clinical trial for adults with diabetes mellitus found a reduction in circulating levels of lyso PC C16:1 after consistent fish oil supplementation [32], which may support the current study’s findings that fatty fish is inversely associated with a metabolite pattern of eight lyso PCs, including lyso PC C16:1.
For BMI and metabolite pattern 3, similar to our study, the aforementioned Mendelian randomization analysis on BMI and metabolites also found an inverse effect of BMI on blood levels of lyso PCs C18:1 and C18:2 [9], both of which were included in the pattern.
The current analyses have identified dietary (fish and alcohol) and anthropometric (BMI) correlates of three metabolite patterns that were previously found to be inversely associated with more aggressive prostate cancer subtypes [1]. The implications of these associations are not yet clear; fish [33,34,35,36,37,38,39,40,41] and alcohol intakes [42,43,44,45,46,47,48,49,50,51] are not established risk factors for prostate cancer, while any associations of BMI with prostate cancer risk, of which positive associations with advanced disease and death have previously been reported [52], might be due to differences in the timing of detection of prostate cancer in men with obesity compared to men with a normal BMI [27,53,54,55,56,57]. Furthermore, research is ongoing to determine whether the metabolite pattern–prostate cancer associations previously reported are likely to be causal.
5. Strengths and Limitations
A major strength of this study is its large sample size owing to the pooling of metabolomics data from four sub-studies within EPIC. Furthermore, using the metabolite patterns as outcome variables accounted for correlations between metabolites [1]. In addition, having access to a wide variety of collected exposure data allowed for the investigation of a range of potential dietary variables and BMI, and adjustment for potential confounding factors. Finally, the discovery/validation approach likely reduced the in-sample bias due to participant overlap between those used to derive metabolite patterns and those used to validate the diet- and BMI-metabolite pattern associations.
One limitation of this study is its cross-sectional design, which prevents drawing any definitive conclusions about the temporality and causality of the reported associations. Potential heterogeneity in metabolite concentrations, such as between the four sub-studies, was addressed by applying a dedicated pipeline to the data prior to statistical analyses [12], and the analytical protocol used has demonstrated high reproducibility between instruments [57]. To assess dietary intakes, food frequency questionnaires were used in most EPIC centers, which can result in some measurement error due to the misreporting of food consumption, recall bias, or errors related to the food composition tables used. Despite this, numerous pilot and cross-sectional studies have supported the reproducibility and validity of the food frequency questionnaire method [27,58]. Finally, this study was conducted on a European population, and while there is limited information on racial and ethnic diversity of the participants, it is expected that the participants are primarily of European ancestry. This limited diversity may hamper the generalizability of the current findings to non-European populations. Future research should evaluate associations in different ethnic and racial groups to provide a more generalizable understanding of determinants of the circulating metabolome.
6. Conclusions
This large, cross-sectional study in European men indicates that BMI and intakes of total fish products, fish subtypes, and alcohol are associated with the metabolite patterns that have been previously linked to a lower risk of aggressive prostate cancer tumor subtypes. The nature and possible causality of these associations warrants further investigation.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/nu14163306/s1, Table S1: Instruments used to quantify metabolites in the study population; Table S2. Associations of dietary exposures and BMI with metabolite patterns in the discovery and validation sets; Table S3: Associations of validated dietary exposures and BMI with individual metabolites loading on each metabolite pattern.
Author Contributions
Conceptualization, Z.S.G., R.C.T., J.A.S., K.S.-B. and T.J.K.; methodology, Z.S.G., R.C.T., J.A.S., K.S.-B., T.J.K., U.N., V.V. and M.H; formal analysis, Z.S.G. and U.N.; resources, R.C.T. and T.J.K.; writing—original draft preparation, Z.S.G., R.C.T., J.A.S., K.S.-B., T.J.K. and U.N.; writing—review and editing, Z.S.G., R.C.T., J.A.S., K.S.-B., T.J.K., U.N., M.H., V.V., S.R., E.K.A., P.A., L.B., M.D.C., I.D., F.E., H.F., S.G., A.K.H., R.K., V.K., A.-L.M.-C., L.M., C.M.-I., V.P., A.O., M.B.S., M.-J.S., M.B.S., A.T., K.K.T., E.W., A.W. and R.Z.-R.; supervision, R.C.T., J.A.S., K.S.-B. and T.J.K.; funding acquisition, R.C.T. and T.J.K. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by Cancer Research UK [C8221/A30904 and C8221/A29017]. The coordination of EPIC is financially supported by International Agency for Research on Cancer (IARC) and also by the Department of Epidemiology and Biostatistics, School of Public Health, Imperial College London, which has additional infrastructure support provided by the NIHR Imperial Biomedical Research Centre (BRC). The national cohorts are supported by Danish Cancer Society (Denmark); Ligue Contre le Cancer, Institut Gustave Roussy, Mutuelle Générale de l’Education Nationale, Institut National de la Santé et de la Recherche Médicale (INSERM) (France); German Cancer Aid, German Cancer Research Center (DKFZ), German Institute of Human Nutrition Potsdam-Rehbruecke (DIfE), Federal Ministry of Education and Research (BMBF) (Germany); Associazione Italiana per la Ricerca sul Cancro-AIRC-Italy, Compagnia di SanPaolo and National Research Council (Italy); Dutch Ministry of Public Health, Welfare and Sports (VWS), LK Research Funds, Dutch Prevention Funds, Dutch ZON (Zorg Onderzoek Nederland), World Cancer Research Fund (WCRF) (The Netherlands); Health Research Fund (FIS)—Instituto de Salud Carlos III (ISCIII), Regional Governments of Andalucía, Asturias, Basque Country, Murcia and Navarra, and the Catalan Institute of Oncology—ICO (Spain); Swedish Cancer Society, Swedish Research Council and County Councils of Skåne and Västerbotten (Sweden); and Cancer Research UK (14136 to EPIC-Norfolk (DOI 10.22025/2019.10.105.00004); C8221/A29017 to EPIC-Oxford), Medical Research Council (1000143, MR/N003284/1, MC-UU_12015/1 and MC_UU_00006/1 to EPIC-Norfolk; MR/M012190/1 to EPIC-Oxford) (UK). The funders were not involved in designing the study; collecting, analyzing, or interpreting the data; or writing or submitting the manuscript for publication.
Institutional Review Board Statement
This study complies with the Declaration of Helsinki. The study has been approved by the IARC Ethics Committee (ref IEC 14-02). Ethical review boards of IARC and all local institutions where participants had been recruited gave approval for the study.
Informed Consent Statement
All participants gave written informed consent for data collection and storage, as well as individual follow-up.
Data Availability Statement
EPIC data are available for investigators who seek to answer important questions on health and disease in the context of research projects that are consistent with the legal and ethical standard practices of IARC/WHO and the EPIC Centers. The primary responsibility for accessing the data belongs to the EPIC centers that provided them. For information on how to submit an application for gaining access to EPIC data and/or biospecimens, please follow the instructions at http://epic.iarc.fr/access/index.php.
Acknowledgments
The authors thank the participants in the EPIC study, and Carine Biessy and Bertrand Hemon at IARC for their expertise in data handling. We would also like to thank the Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, Utrecht, The Netherlands, as well as the National Institute for Public Health and the Environment (RIVM), Bilthoven, the Netherlands, for their contribution and ongoing support to the EPIC Study.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
IARC Disclaimer
Where authors are identified as personnel of the International Agency for Research on Cancer/World Health Organization, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy, or views of the International Agency for Research on Cancer/World Health Organization.
References
- Schmidt, J.A.; Fensom, G.K.; Rinaldi, S.; Scalbert, A.; Appleby, P.N.; Achaintre, D.; Gicquiau, A.; Gunter, M.J.; Ferrari, P.; Kaaks, R.; et al. Patterns in Metabolite Profile Are Associated with Risk of More Aggressive Prostate Cancer: A Prospective Study of 3057 Matched Case–Control Sets from EPIC. Int. J. Cancer 2020, 146, 720–730. [Google Scholar] [CrossRef]
- Fages, A.; Duarte-Salles, T.; Stepien, M.; Ferrari, P.; Fedirko, V.; Pontoizeau, C.; Trichopoulou, A.; Aleksandrova, K.; Tjønneland, A.; Olsen, A.; et al. Metabolomic Profiles of Hepatocellular Carcinoma in a European Prospective Cohort. BMC Med. 2015, 13, 242. [Google Scholar] [CrossRef]
- Huang, J.; Mondul, A.M.; Weinstein, S.J.; Karoly, E.D.; Sampson, J.N.; Albanes, D. Prospective Serum Metabolomic Profile of Prostate Cancer by Size and Extent of Primary Tumor. Oncotarget 2017, 8, 45190–45199. [Google Scholar] [CrossRef] [PubMed]
- Röhnisch, H.E.; Kyrø, C.; Olsen, A.; Thysell, E.; Hallmans, G.; Moazzami, A.A. Identification of Metabolites Associated with Prostate Cancer Risk: A Nested Case-Control Study with Long Follow-up in the Northern Sweden Health and Disease Study. BMC Med. 2020, 18, 187. [Google Scholar] [CrossRef]
- Scalbert, A.; Brennan, L.; Manach, C.; Andres-Lacueva, C.; Dragsted, L.O.; Draper, J.; Rappaport, S.M.; van der Hooft, J.J.; Wishart, D.S. The Food Metabolome: A Window over Dietary Exposure. Am. J. Clin. Nutr. 2014, 99, 1286–1308. [Google Scholar] [CrossRef]
- Scalbert, A.; Brennan, L.; Fiehn, O.; Hankemeier, T.; Kristal, B.S.; van Ommen, B.; Pujos-Guillot, E.; Verheij, E.; Wishart, D.; Wopereis, S. Mass-Spectrometry-Based Metabolomics: Limitations and Recommendations for Future Progress with Particular Focus on Nutrition Research. Metabolomics 2009, 5, 435–458. [Google Scholar] [CrossRef]
- Riboli, E.; Hunt, K.; Slimani, N.; Ferrari, P.; Norat, T.; Fahey, M.; Charrondière, U.; Hémon, B.; Casagrande, C.; Vignat, J.; et al. European Prospective Investigation into Cancer and Nutrition (EPIC): Study Populations and Data Collection. Public Health Nutr. 2002, 5, 1113–1124. [Google Scholar] [CrossRef] [PubMed]
- Kliemann, N.; Viallon, V.; Murphy, N.; Beeken, R.J.; Rothwell, J.A.; Rinaldi, S.; Assi, N.; van Roekel, E.H.; Schmidt, J.A.; Borch, K.B.; et al. Metabolic Signatures of Greater Body Size and Their Associations with Risk of Colorectal and Endometrial Cancers in the European Prospective Investigation into Cancer and Nutrition. BMC Med. 2021, 19, 101. [Google Scholar] [CrossRef]
- Guida, F.; Tan, V.Y.; Corbin, L.J.; Smith-Byrne, K.; Alcala, K.; Langenberg, C.; Stewart, I.D.; Butterworth, A.S.; Surendran, P.; Achaintre, D.; et al. The Blood Metabolome of Incident Kidney Cancer: A Case-Control Study Nested within the MetKid Consortium. PLoS Med. 2021, 18, e1003786. [Google Scholar] [CrossRef]
- Stepien, M.; Duarte-Salles, T.; Fedirko, V.; Floegel, A.; Barupal, D.K.; Rinaldi, S.; Achaintre, D.; Assi, N.; Tjønneland, A.; Overvad, K.; et al. Alteration of Amino Acid and Biogenic Amine Metabolism in Hepatobiliary Cancers: Findings from a Prospective Cohort Study: Circulating Biomarkers of Hepatobiliary Cancer Risks. Int. J. Cancer 2016, 138, 348–360. [Google Scholar] [CrossRef]
- Guida, F.; Severi, G.; Giles, G.G.; Johansson, M. Metabolomics and Risk of Kidney Cancer. Rev. D’épidémiologie Et De St. Publique 2018, 66, S291. [Google Scholar] [CrossRef]
- Viallon, V.; His, M.; Rinaldi, S.; Breeur, M.; Gicquiau, A.; Hemon, B.; Overvad, K.; Tjønneland, A.; Rostgaard-Hansen, A.L.; Rothwell, J.A.; et al. A New Pipeline for the Normalization and Pooling of Metabolomics Data. Metabolites 2021, 11, 631. [Google Scholar] [CrossRef] [PubMed]
- Van Puyvelde, H.; Perez-Cornago, A.; Casagrande, C.; Nicolas, G.; Versele, V.; Skeie, G.; Schulze, M.B.; Johansson, I.; María Huerta, J.; Oliverio, A.; et al. Comparing Calculated Nutrient Intakes Using Different Food Composition Databases: Results from the European Prospective Investigation into Cancer and Nutrition (EPIC) Cohort. Nutrients 2020, 12, 2906. [Google Scholar] [CrossRef] [PubMed]
- Great Britain Ministry of Agriculture, Fisheries, and Food. Food Portion Sizes, 2nd ed.; HMSO: London, UK, 1993. [Google Scholar]
- Murphy, N.; Norat, T.; Ferrari, P.; Jenab, M.; Bueno-de-Mesquita, B.; Skeie, G.; Olsen, A.; Tjønneland, A.; Dahm, C.C.; Overvad, K.; et al. Consumption of Dairy Products and Colorectal Cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC). PLoS ONE 2013, 8, e72715. [Google Scholar] [CrossRef] [PubMed]
- Pala, V.; Krogh, V.; Berrino, F.; Sieri, S.; Grioni, S.; Tjønneland, A.; Olsen, A.; Jakobsen, M.U.; Overvad, K.; Clavel-Chapelon, F.; et al. Meat, Eggs, Dairy Products, and Risk of Breast Cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC) Cohort. Am. J. Clin. Nutr. 2009, 90, 602–612. [Google Scholar] [CrossRef]
- Zamora-Ros, R.; Castañeda, J.; Rinaldi, S.; Cayssials, V.; Slimani, N.; Weiderpass, E.; Tsilidis, K.K.; Boutron-Ruault, M.-C.; Overvad, K.; Eriksen, A.K.; et al. Consumption of Fish Is Not Associated with Risk of Differentiated Thyroid Carcinoma in the European Prospective Investigation into Cancer and Nutrition (EPIC) Study. J. Nutr. 2017, 147, 1366–1373. [Google Scholar] [CrossRef]
- Linseisen, J.; Bergström, E.; Gafá, L.; González, C.; Thiébaut, A.; Trichopoulou, A.; Tumino, R.; Sánchez, C.N.; Garcia, C.M.; Mattisson, I.; et al. Consumption of Added Fats and Oils in the European Prospective Investigation into Cancer and Nutrition (EPIC) Centres across 10 European Countries as Assessed by 24-Hour Dietary Recalls. Public Health Nutr. 2002, 5, 1227–1242. [Google Scholar] [CrossRef]
- Zamora-Ros, R.; Béraud, V.; Franceschi, S.; Cayssials, V.; Tsilidis, K.K.; Boutron-Ruault, M.-C.; Weiderpass, E.; Overvad, K.; Tjønneland, A.; Eriksen, A.K.; et al. Consumption of Fruits, Vegetables and Fruit Juices and Differentiated Thyroid Carcinoma Risk in the European Prospective Investigation into Cancer and Nutrition (EPIC) Study: Fruits, Vegetables, and Fruit Juices and Thyroid Cancer in EPIC. Int. J. Cancer 2018, 142, 449–459. [Google Scholar] [CrossRef]
- Gorst-Rasmussen, A. Tt: Treelet Transform with Stata. Stata J. Promot. Commun. Stat. Stata 2012, 12, 130–146. [Google Scholar] [CrossRef]
- Gorst-Rasmussen, A.; Dahm, C.C.; Dethlefsen, C.; Scheike, T.; Overvad, K. Exploring Dietary Patterns by Using the Treelet Transform. Am. J. Epidemiol. 2011, 173, 1097–1104. [Google Scholar] [CrossRef]
- Wareham, N.J.; Jakes, R.W.; Rennie, K.L.; Schuit, J.; Mitchell, J.; Hennings, S.; Day, N.E. Validity and Repeatability of a Simple Index Derived from the Short Physical Activity Questionnaire Used in the European Prospective Investigation into Cancer and Nutrition (EPIC) Study. Public Health Nutr. 2003, 6, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Pallister, T.; Jennings, A.; Mohney, R.P.; Yarand, D.; Mangino, M.; Cassidy, A.; MacGregor, A.; Spector, T.D.; Menni, C. Characterizing Blood Metabolomics Profiles Associated with Self-Reported Food Intakes in Female Twins. PLoS ONE 2016, 11, e0158568. [Google Scholar] [CrossRef] [PubMed]
- Jaremek, M.; Yu, Z.; Mangino, M.; Mittelstrass, K.; Prehn, C.; Singmann, P.; Xu, T.; Dahmen, N.; Weinberger, K.M.; Suhre, K.; et al. Alcohol-Induced Metabolomic Differences in Humans. Transl. Psychiatry 2013, 3, e276. [Google Scholar] [CrossRef]
- Lacruz, M.E.; Kluttig, A.; Tiller, D.; Medenwald, D.; Giegling, I.; Rujescu, D.; Prehn, C.; Adamski, J.; Frantz, S.; Greiser, K.H.; et al. Cardiovascular Risk Factors Associated with Blood Metabolite Concentrations and Their Alterations During a 4-Year Period in a Population-Based Cohort. Circ. Cardiovasc. Genet. 2016, 9, 487–494. [Google Scholar] [CrossRef]
- His, M.; Viallon, V.; Dossus, L.; Schmidt, J.A.; Travis, R.C.; Gunter, M.J.; Overvad, K.; Kyrø, C.; Tjønneland, A.; Lécuyer, L.; et al. Lifestyle Correlates of Eight Breast Cancer-Related Metabolites: A Cross-Sectional Study within the EPIC Cohort. BMC Med. 2021, 19, 312. [Google Scholar] [CrossRef]
- Hodson, L.; Crowe, F.L.; McLachlan, K.J.; Skeaff, C.M. Effect of Supplementation with Flaxseed Oil and Different Doses of Fish Oil for 2 Weeks on Plasma Phosphatidylcholine Fatty Acids in Young Women. Eur. J. Clin. Nutr. 2018, 72, 832–840. [Google Scholar] [CrossRef]
- Floegel, A.; von Ruesten, A.; Drogan, D.; Schulze, M.B.; Prehn, C.; Adamski, J.; Pischon, T.; Boeing, H. Variation of Serum Metabolites Related to Habitual Diet: A Targeted Metabolomic Approach in EPIC-Potsdam. Eur. J. Clin. Nutr. 2013, 67, 1100–1108. [Google Scholar] [CrossRef]
- Cheng, S.; Rhee, E.P.; Larson, M.G.; Lewis, G.D.; McCabe, E.L.; Shen, D.; Palma, M.J.; Roberts, L.D.; Dejam, A.; Souza, A.L.; et al. Metabolite Profiling Identifies Pathways Associated with Metabolic Risk in Humans. Circulation 2012, 125, 2222–2231. [Google Scholar] [CrossRef]
- Carayol, M.; Leitzmann, M.F.; Ferrari, P.; Zamora-Ros, R.; Achaintre, D.; Stepien, M.; Schmidt, J.A.; Travis, R.C.; Overvad, K.; Tjønneland, A.; et al. Blood Metabolic Signatures of Body Mass Index: A Targeted Metabolomics Study in the EPIC Cohort. J. Proteome Res. 2017, 16, 3137–3146. [Google Scholar] [CrossRef]
- Abdolahi, A.; Georas, S.N.; Thomas Brenna, J.; Cai, X.; Thevenet-Morrison, K.; Phipps, R.P.; Lawrence, P.; Mousa, S.A.; Block, R.C. The Effects of Aspirin and Fish Oil Consumption on Lysophosphatidylcholines and Lysophosphatidic Acids and Their Correlates with Platelet Aggregation in Adults with Diabetes Mellitus. Prostaglandins Leukot. Essent. Fat. Acids 2014, 90, 61–68. [Google Scholar] [CrossRef]
- Terry, P.; Lichtenstein, P.; Feychting, M.; Ahlbom, A.; Wolk, A. Fatty Fish Consumption and Risk of Prostate Cancer. Lancet 2001, 357, 1764–1766. [Google Scholar] [CrossRef]
- Augustsson, K.; Michaud, D.S.; Rimm, E.B.; Leitzmann, M.F.; Stampfer, M.J.; Willett, W.C.; Giovannucci, E. A Prospective Study of Intake of Fish and Marine Fatty Acids and Prostate Cancer. Cancer Epidemiol. Biomark. Prev. 2003, 12, 64–67. [Google Scholar]
- Allen, N.E.; Sauvaget, C.; Roddam, A.W.; Appleby, P.; Nagano, J.; Suzuki, G.; Key, T.J.; Koyama, K. A Prospective Study of Diet and Prostate Cancer in Japanese Men. Cancer Causes Control 2004, 15, 911–920. [Google Scholar] [CrossRef]
- Mills, P.K.; Beeson, W.L.; Phillips, R.L.; Fraser, G.E. Cohort Study of Diet, Lifestyle, and Prostate Cancer in Adventist Men. Cancer 1989, 64, 598–604. [Google Scholar] [CrossRef]
- Severson, R.K.; Nomura, A.M.; Grove, J.S.; Stemmermann, G.N. A Prospective Study of Demographics, Diet, and Prostate Cancer among Men of Japanese Ancestry in Hawaii. Cancer Res. 1989, 49, 1857–1860. [Google Scholar]
- Hsing, A.W.; McLaughlin, J.K.; Schuman, L.M.; Bjelke, E.; Gridley, G.; Wacholder, S.; Chien, H.T.; Blot, W.J. Diet, Tobacco Use, and Fatal Prostate Cancer: Results from the Lutheran Brotherhood Cohort Study. Cancer Res. 1990, 50, 6836–6840. [Google Scholar]
- Le Marchand, L.; Kolonel, L.N.; Wilkens, L.R.; Myers, B.C.; Hirohata, T. Animal Fat Consumption and Prostate Cancer: A Prospective Study in Hawaii. Epidemiol. Camb. Mass 1994, 5, 276–282. [Google Scholar] [CrossRef]
- Grönberg, H.; Damber, L.; Damber, J.E. Total Food Consumption and Body Mass Index in Relation to Prostate Cancer Risk: A Case-Control Study in Sweden with Prospectively Collected Exposure Data. J. Urol. 1996, 155, 969–974. [Google Scholar] [CrossRef]
- Schuurman, A.G.; van den Brandt, P.A.; Dorant, E.; Goldbohm, R.A. Animal Products, Calcium and Protein and Prostate Cancer Risk in the Netherlands Cohort Study. Br. J. Cancer 1999, 80, 1107–1113. [Google Scholar] [CrossRef]
- World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Expert Report 2018. Diet, Nutrition, Physical Activity, and Prostate Cancer. Available online: https://www.wcrf.org/wp-content/uploads/2021/02/prostate-cancer-report.pdf (accessed on 7 March 2022).
- Rohrmann, S.; Linseisen, J.; Key, T.J.; Jensen, M.K.; Overvad, K.; Johnsen, N.F.; Tjønneland, A.; Kaaks, R.; Bergmann, M.M.; Weikert, C.; et al. Alcohol Consumption and the Risk for Prostate Cancer in the European Prospective Investigation into Cancer and Nutrition. Cancer Epidemiol. Biomark. Prev. 2008, 17, 1282–1287. [Google Scholar] [CrossRef] [PubMed]
- Schuurman, A.G.; Goldbohm, R.A.; van den Brandt, P.A. A Prospective Cohort Study on Consumption of Alcoholic Beverages in Relation to Prostate Cancer Incidence (The Netherlands). Cancer Causes Control 1999, 10, 597–605. [Google Scholar] [CrossRef]
- Breslow, R.A.; Wideroff, L.; Graubard, B.I.; Erwin, D.; Reichman, M.E.; Ziegler, R.G.; Ballard-Barbash, R. Alcohol and Prostate Cancer in the NHANES I Epidemiologic Follow-Up Study. Ann. Epidemiol. 1999, 9, 254–261. [Google Scholar] [CrossRef]
- Nilsen, T.I.L.; Vatten, L.J. Anthropometry and Prostate Cancer Risk: A Prospective Study of 22,248 Norwegian Men. Cancer Causes Control 1999, 10, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Baglietto, L.; Severi, G.; English, D.R.; Hopper, J.L.; Giles, G.G. Alcohol Consumption and Prostate Cancer Risk: Results from the Melbourne Collaborative Cohort Study. Int. J. Cancer 2006, 119, 1501–1504. [Google Scholar] [CrossRef]
- Weinstein, S.J.; Stolzenberg-Solomon, R.; Pietinen, P.; Taylor, P.R.; Virtamo, J.; Albanes, D. Dietary Factors of One-Carbon Metabolism and Prostate Cancer Risk. Am. J. Clin. Nutr. 2006, 84, 929–935. [Google Scholar] [CrossRef]
- Sesso, H.D.; Paffenbarger, R.S.; Lee, I.-M. Alcohol Consumption and Risk of Prostate Cancer: The Harvard Alumni Health Study. Int. J. Epidemiol. 2001, 30, 749–755. [Google Scholar] [CrossRef]
- Platz, E.A. Alcohol Intake, Drinking Patterns, and Risk of Prostate Cancer in a Large Prospective Cohort Study. Am. J. Epidemiol. 2004, 159, 444–453. [Google Scholar] [CrossRef]
- Velicer, C.M.; Kristal, A.; White, E. Alcohol Use and the Risk of Prostate Cancer: Results from the VITAL Cohort Study. Nutr. Cancer 2006, 56, 50–56. [Google Scholar] [CrossRef]
- Fujita, K.; Hayashi, T.; Matsushita, M.; Uemura, M.; Nonomura, N. Obesity, Inflammation, and Prostate Cancer. J. Clin. Med. 2019, 8, 201. [Google Scholar] [CrossRef]
- Littman, A.J.; White, E.; Kristal, A.R. Anthropometrics and Prostate Cancer Risk. Am. J. Epidemiol. 2007, 165, 1271–1279. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, C.; Freedland, S.J.; Deka, A.; Jacobs, E.J.; McCullough, M.L.; Patel, A.V.; Thun, M.J.; Calle, E.E. Body Mass Index, Weight Change, and Risk of Prostate Cancer in the Cancer Prevention Study II Nutrition Cohort. Cancer Epidemiol. Biomark. Prev. 2007, 16, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Ma, J. Body Mass Index, Prostate Cancer–Specific Mortality, and Biochemical Recurrence: A Systematic Review and Meta-Analysis. Cancer Prev. Res. 2011, 4, 486–501. [Google Scholar] [CrossRef] [PubMed]
- Möller, E.; Wilson, K.M.; Batista, J.L.; Mucci, L.A.; Bälter, K.; Giovannucci, E. Body Size across the Life Course and Prostate Cancer in the Health Professionals Follow-up Study: Body Size and Prostate Cancer. Int. J. Cancer 2016, 138, 853–865. [Google Scholar] [CrossRef]
- Siskos, A.P.; Jain, P.; Römisch-Margl, W.; Bennett, M.; Achaintre, D.; Asad, Y.; Marney, L.; Richardson, L.; Koulman, A.; Griffin, J.L.; et al. Interlaboratory Reproducibility of a Targeted Metabolomics Platform for Analysis of Human Serum and Plasma. Anal. Chem. 2017, 89, 656–665. [Google Scholar] [CrossRef]
- Margetts, B.; Pietinen, P. European Prospective Investigation into Cancer and Nutrition: Validity Studies on Dietary Assessment Methods. Int. J. Epidemiol. 1997, 26, S1. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).