
Differences in Dietary Intake Exist among U.S. Adults by Diabetic Status Using NHANES 2009–2016


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Dataset
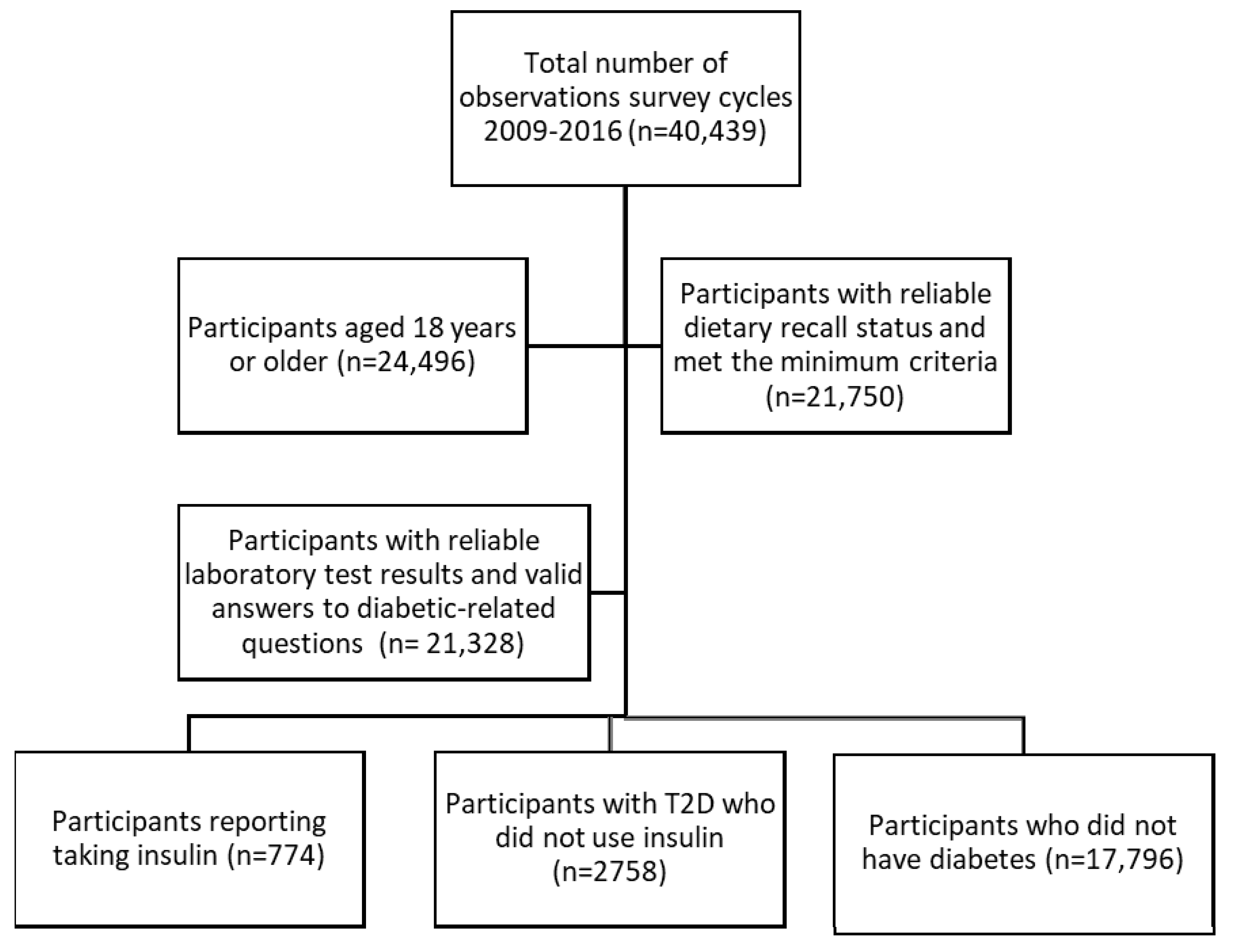
2.2. Analytic Sample
2.3. Sociodemographic and Sample Characteristics
2.4. Dietary Assessment
2.5. Statistical Analysis
3. Results
3.1. Sociodemographic and Sample Characteristics
3.2. The Most Frequently Consumed Food Items, Food Subcategories, and Food Categories
3.3. The Highest Energy Contributing Food Items, Food Subcategories, and Food Categories
3.4. Broad Food Category Intake by Frequency and Energy Contribution
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centers for Disease Control and Prevention. What is Diabetes? 11 June 2020. Available online: https://www.cdc.gov/diabetes/basics/diabetes.html (accessed on 14 July 2021).
- Centers for Disease Control and Prevention. National Diabetes Statistics Report. 2020. Available online: https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf (accessed on 14 July 2021).
- Centers for Disease Control and Prevention. The Insulin Resistance–Diabetes Connection. 23 July 2020. Available online: https://www.cdc.gov/diabetes/basics/insulin-resistance.html (accessed on 14 July 2021).
- Centers for Disease Control and Prevention. Types of Insulin. 2 April 2021. Available online: https://www.cdc.gov/diabetes/basics/type-1-types-of-insulin.html (accessed on 14 July 2021).
- Joslin, E.P.; Kahn, C.R. Joslin’s Diabetes Mellitus; Kahn, C.R., Weir, G.C., King, G.L., Moses, A.C., Smith, R.J., Jacobson, A.M., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005. [Google Scholar]
- Gillespie, S.J.; Kulkarni, K.D.; Daly, A.E. Using Carbohydrate Counting in Diabetes Clinical Practice. J. Am. Diet. Assoc. 1998, 98, 897–905. [Google Scholar] [CrossRef]
- Acierno, C.; Caturano, A.; Pafundi, P.C.; Nevola, R.; Adinolfi, L.E.; Sasso, F.C. Nonalcoholic fatty liver disease and type 2 diabetes: Pathophysiological mechanisms shared between the two faces of the same coin. Explor Med. 2020, 1, 287–306. [Google Scholar] [CrossRef]
- Patton, S.R. Adherence to Diet in Youth with Type 1 Diabetes. J. Am. Diet. Assoc. 2011, 111, 550–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McClure, S.T.; Schlechter, H.; Oh, S.; White, K.; Wu, B.; Pilla, S.J.; Maruthur, N.M.; Yeh, H.C.; Miller, E.R.; Appel, L.J. Dietary intake of adults with and without diabetes: Results from NHANES 2013–2016. BMJ Open Diabetes Res. Care 2020, 8, e001681. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Pareja, M.; León-Muñoz, L.M.; Guallar-Castillón, P.; Graciani, A.; López-García, E.; Banegas, J.R.; Rodríguez-Artalejo, F. The Diet of Diabetic Patients in Spain in 2008–2010: Accordance with the Main Dietary Recommendations—A Cross-Sectional Study. PLoS ONE 2012, 7, e39454. [Google Scholar] [CrossRef] [Green Version]
- Maffeis, C.; Tomasselli, F.; Tommasi, M.; Bresadola, I.; Trandev, T.; Fornari, E.; Marigliano, M.; Morandi, A.; Olivieri, F.; Piona, C. Nutrition habits of children and adolescents with type 1 diabetes changed in a 10 years span. Pediatr. Diabetes 2020, 21, 960–968. [Google Scholar] [CrossRef]
- NHANES—National Health and Nutrition Examination Survey Homepage. 24 June 2021. Available online: https://www.cdc.gov/nchs/nhanes/index.htm (accessed on 14 July 2021).
- NHANES—NCHS Research Ethics Review Board Approval. 8 May 2019. Available online: https://www.cdc.gov/nchs/nhanes/irba98.htm (accessed on 14 July 2021).
- American Diabetes Association. Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2014, 37 (Suppl. S1), S81–S90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, K.M.; Reiber, G.; Boyko, E.J. Diet and Exercise Among Adults with Type 2 Diabetes: Findings from the Third National Health and Nutrition Examination Survey (NHANES III). Diabetes Care 2002, 25, 1722–1728. [Google Scholar] [CrossRef] [Green Version]
- U.C. Bureau. How the Census Bureau Measures Poverty. The United States Census Bureau. Available online: https://www.census.gov/topics/income-poverty/poverty/guidance/poverty-measures.html (accessed on 15 July 2021).
- Body Mass Index—BMI. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 11 June 2021).
- AMPM—USDA Automated Multiple-Pass Method: USDA ARS. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/ampm-usda-automated-multiple-pass-method/#what (accessed on 16 July 2020).
- NHANES Dietary Data. Available online: https://wwwn.cdc.gov/nchs/nhanes/Search/DataPage.aspx?Component=Dietary (accessed on 14 July 2021).
- U.S. Department of Agriculture. Agricultural Research Service. 2012. USDA Food and Nutrient Database for Dietary Studies, 5.0. Food Surveys Research Group Home Page. Available online: http://www.ars.usda.gov/ba/bhnrc/fsrg (accessed on 14 July 2021).
- U.S. Department of Agriculture. Agricultural Research Service. 2014. USDA Food and Nutrient Database for Dietary Studies 2011–2012. Food Surveys Research Group Home Page. Available online: http://www.ars.usda.gov/ba/bhnrc/fsrg (accessed on 14 July 2021).
- U.S. Department of Agriculture. Agricultural Research Service. 2016. USDA Food and Nutrient Database for Dietary Studies 2013–2014. Food Surveys Research Group Home Page. Available online: http://www.ars.usda.gov/nea/bhnrc/fsrg (accessed on 14 July 2021).
- U.S. Department of Agriculture. Agricultural Research Service. 2018. USDA Food and Nutrient Database for Dietary Studies 2015–2016. Food Surveys Research Group Home Page. Available online: http://www.ars.usda.gov/nea/bhnrc/fsrg”.https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/fndds-download-databases/ (accessed on 13 September 2021).
- U.S. Department of Agriculture. Agricultural Research Service. What We Eat in America Food Categories 2015–2016. Available online: https://www.ars.usda.gov/ARSUserFiles/80400530/pdf/1516/Food_categories_2015-2016.pdf (accessed on 14 July 2021).
- Eicher-Miller, H.A.; Boushey, C.J. How Often and How Much? Differences in Dietary Intake by Frequency and Energy Contribution Vary among U.S. Adults in NHANES 2007–2012. Nutrients 2017, 9, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eicher-Miller, H.A.; Boushey, C.J.; Bailey, R.L.; Yang, Y.J. Frequently Consumed Foods and Energy Contributions among Food Secure and Insecure U.S. Children and Adolescents. Nutrients 2020, 12, 304. [Google Scholar] [CrossRef] [Green Version]
- Hiza, H.A.B.; Casavale, K.O.; Guenther, P.M.; Davis, C.A. Diet Quality of Americans Differs by Age, Sex, Race/Ethnicity, Income, and Education Level. J. Acad. Nutr. Diet. 2013, 113, 297–306. [Google Scholar] [CrossRef]
- Forshee, R.A.; Storey, M.L. Demographics, not beverage consumption, is associated with diet quality. Int. J. Food Sci. Nutr. 2006, 57, 494–511. [Google Scholar] [CrossRef]
- Sundararajan, K.K.M.; Campbell, C.Y.-H.; Sarma, S. The Relationship Between Diet Quality and Adult Obesity: Evidence from Canada. J. Am. Coll. Nutr. 2014, 33, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Livingstone, K.M.; McNaughton, S.A. Diet quality is associated with obesity and hypertension in Australian adults: A cross sectional study. BMC Public Health 2016, 16, 1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NHANES-FSP.pdf. Available online: https://fns-prod.azureedge.us/sites/default/files/NHANES-FSP.pdf (accessed on 10 April 2022).
- Wang, Z.; Adair, L.S.; Cai, J.; Gordon-Larsen, P.; Siega-Riz, A.M.; Zhang, B.; Popkin, B.M. Diet Quality Is Linked to Insulin Resistance among Adults in China. J. Nutr. 2017, 147, 2102–2108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sebire, S.J.; Toumpakari, Z.; Turner, K.M.; Cooper, A.R.; Page, A.S.; Malpass, A.; Andrews, R.C. “I’ve made this my lifestyle now”: A prospective qualitative study of motivation for lifestyle change among people with newly diagnosed type two diabetes mellitus. BMC Public Health 2018, 18, 204. [Google Scholar] [CrossRef] [Green Version]
- Niewind, A.C.; Friele, R.D.; Kandou, C.T.; Hautvast, J.G.a.J.; Edema, J.M.P. Changes in food choices of recently diagnosed insulin-dependent diabetic patients. Eur. J. Clin. Nutr. 1990, 44, 505–513. [Google Scholar]
- Fung, T.T.; Hu, F.B.; Pereira, M.A.; Liu, S.; Stampfer, M.J.; Colditz, G.A.; Willett, W.C. Whole-grain intake and the risk of type 2 diabetes: A prospective study in men. Am. J. Clin. Nutr. 2002, 76, 535–540. [Google Scholar] [CrossRef] [Green Version]
- Clifton, P. High-protein and low-glycaemic diets improve dietary compliance and maintenance of weight loss in overweight adults who have lost weight on a low-calorie diet. BMJ Evid.-Based Med. 2011, 16, 112–113. [Google Scholar] [CrossRef] [PubMed]
- MWesterterp-Plantenga, S.; Nieuwenhuizen, A.; Tomé, D.; Soenen, S.; Westerterp, K.R. Dietary Protein, Weight Loss, and Weight Maintenance. Annu. Rev. Nutr. 2009, 29, 21–41. [Google Scholar] [CrossRef] [Green Version]
- Dias, J.S. Nutritional Quality and Health Benefits of Vegetables: A Review. Food Nutr. Sci. 2012, 3, 1354–1374. [Google Scholar] [CrossRef] [Green Version]
- Carlos, J.; Dias, J.; Imai, S. Vegetables Consumption and its Benefits on Diabetes. J. Nutr. Ther. 2017, 6, 1–10. [Google Scholar] [CrossRef]
- Platel, K.; Srinivasan, K. Plant foods in the management of Diabetes mellitus: Vegetables as potential hypoglycaemic agents. Food Nahr. 1997, 41, 68–74. [Google Scholar] [CrossRef]
- Nicklas, T.A.; O’Neil, C.E. Development of the SoFAS (Solid Fats and Added Sugars) Concept: The 2010 Dietary Guidelines for Americans. Adv. Nutr. 2015, 6, 368S–375S. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025; The U.S. Department of Agriculture: Washington, DC, USA; U.S. Department of Health and Human Services: Washington, DC, USA; p. 164.
- Mackenzie, T.; Brooks, B.; O’Connor, G. Beverage Intake, Diabetes, and Glucose Control of Adults in America. Ann. Epidemiol. 2006, 16, 88–691. [Google Scholar] [CrossRef]
- Nöthlings, U.; Boeing, H.; Maskarinec, G.; Sluik, D.; Teucher, B.; Kaaks, R.; Tjønneland, A.; Halkjaer, J.; Dethlefsen, C.; K Overvad, P.A.; et al. Food intake of individuals with and without diabetes across different countries and ethnic groups. Eur. J. Clin. Nutr. 2011, 65, 635–641. [Google Scholar] [CrossRef]
- Howard, A.A.; Arnsten, J.H.; Gourevitch, M.N. Effect of Alcohol Consumption on Diabetes Mellitus. Ann. Intern. Med. 2004, 140, 211–219. [Google Scholar] [CrossRef]
- Ahmed, A.T.; Karter, A.J.; Liu, J. Alcohol consumption is inversely associated with adherence to diabetes self-care behaviours. Diabet. Med. 2006, 23, 795–802. [Google Scholar] [CrossRef] [Green Version]
- Chhimwal, J.; Patial, V.; Padwad, Y. Beverages and Non-alcoholic fatty liver disease (NAFLD): Think before you drink. Clin. Nutr. 2021, 40, 2508–2519. [Google Scholar] [CrossRef]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Després, J.-P.; Hu, F.B. Sugar-Sweetened Beverages, Obesity, Type 2 Diabetes Mellitus, and Cardiovascular Disease Risk. Circulation 2010, 121, 1356–1364. [Google Scholar] [CrossRef]
- Caturano, A.; Acierno, C.; Nevola, R.; Pafundi, P.C.; Galiero, R.; Rinaldi, L.; Salvatore, T.; Adinolfi, L.E.; Sasso, F.C. Non-Alcoholic Fatty Liver Disease: From Pathogenesis to Clinical Impact. Processes 2021, 9, 135. [Google Scholar] [CrossRef]
- Salvatore, T.; Galiero, R.; Caturano, A.; Vetrano, E.; Rinaldi, L.; Coviello, F.; di Martino, A.; Albanese, G.; Colantuoni, S.; Medicamento, G.; et al. Dysregulated Epicardial Adipose Tissue as a Risk Factor and Potential Therapeutic Target of Heart Failure with Preserved Ejection Fraction in Diabetes. Biomolecules 2022, 12, 176. [Google Scholar] [CrossRef]
- Hess, J.M.; Cifelli, C.J.; Agarwal, S.; Fulgoni, V.L. Comparing the cost of essential nutrients from different food sources in the American diet using NHANES 2011–2014. Nutr. J. 2019, 18, 68. [Google Scholar] [CrossRef] [Green Version]
- Murphy, M.M.; Scrafford, C.G.; Barraj, L.M.; Bi, X.; Higgins, K.A.; Jaykus, L.A.; Tran, N.L. Potassium chloride-based replacers: Modeling effects on sodium and potassium intakes of the US population with cross-sectional data from NHANES 2015–2016 and 2009–2010. Am. J. Clin. Nutr. 2021, 114, 220–230. [Google Scholar] [CrossRef]
- Slining, M.M.; Popkin, B.M. Trends in intakes and sources of solid fats and added sugars among U.S. children and adolescents: 1994–2010. Pediatr. Obes. 2013, 8, 307–324. [Google Scholar] [CrossRef] [Green Version]
- Lowden, A.; Moreno, C.; Holmbäck, U.; Lennernäs, M.; Tucker, P. Eating and shift work—Effects on habits, metabolism, and performance. Scand. J. Work. Environ. Health 2010, 36, 150–162. [Google Scholar] [CrossRef]
- Aqeel, M.; Forster, A.; Richards, E.A.; Hennessy, E.; McGowan, B.; Bhadra, A.; Guo, J.; Gelfand, S.; Delp, E.; Eicher-Miller, H.A. The Effect of Timing of Exercise and Eating on Postprandial Response in Adults: A Systematic Review. Nutrients 2020, 12, 221. [Google Scholar] [CrossRef] [Green Version]
- Johnston, J.D. Physiological responses to food intake throughout the day. Nutr. Res. Rev. 2014, 27, 107–118. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, D.R., Jr.; Steffen, L.M. Nutrients, foods, and dietary patterns as exposures in research: A framework for food synergy. Am. J. Clin. Nutr. 2003, 78, 508S–513S. [Google Scholar] [CrossRef]
- Winham, D.M.; Hutchins, A.M.; Thompson, S.V. Glycemic Response to Black Beans and Chickpeas as Part of a Rice Meal: A Randomized Cross-Over Trial. Nutrients 2017, 9, 95. [Google Scholar] [CrossRef] [Green Version]
- Klesges, R.C.; Eck, L.H.; Ray, J.W. Who underreports dietary intake in a dietary recall? Evidence from the Second National Health and Nutrition Examination Survey. J. Consult. Clin. Psychol. 1995, 63, 438–444. [Google Scholar] [CrossRef]
- Freedman, L.S.; Commins, J.M.; Moler, J.E.; Arab, L.; Baer, D.J.; Kipnis, V.; Midthune, D.; Moshfegh, A.J.; Neuhouser, M.L.; Prentice, R.L. Pooled Results From 5 Validation Studies of Dietary Self-Report Instruments Using Recovery Biomarkers for Energy and Protein Intake. Am. J. Epidemiol. 2014, 180, 172–188. [Google Scholar] [CrossRef] [Green Version]
- Lissner, L.; Troiano, R.P.; Midthune, D.; Heitmann, B.L.; Kipnis, V.; Subar, A.F.; Potischman, N. OPEN about obesity: Recovery biomarkers, dietary reporting errors and BMI. Int. J. Obes. 2007, 31, 956–961. [Google Scholar] [CrossRef] [Green Version]
- Ocké, M.C.; Larrañaga, N.; Grioni, S.; van den Berg, S.W.; Ferrari, P.; Salvini, S.; Benetou, V.; Linseisen, J.; Wirfält, E.; Rinaldi, S.; et al. Energy intake and sources of energy intake in the European Prospective Investigation into Cancer and Nutrition. Eur. J. Clin. Nutr. 2009, 63, S3–S15. [Google Scholar] [CrossRef] [Green Version]
- Livingstone, M.B.E.; Black, A.E. Markers of the Validity of Reported Energy Intake. J. Nutr. 2003, 133, 895S–920S. [Google Scholar] [CrossRef]
- Underreporting of Food Intake in Obese Diabetic and Nondiabetic Patients. Diabetes Care. Available online: https://care.diabetesjournals.org/content/29/12/2726.short (accessed on 6 September 2021).
- Gregg, E.W.; Cheng, Y.J.; Narayan, K.M.V.; Thompson, T.J.; Williamson, D.F. The relative contributions of different levels of overweight and obesity to the increased prevalence of diabetes in the United States: 1976–2004. Prev. Med. 2007, 45, 348–352. [Google Scholar] [CrossRef]
- Nuttall, F.Q. Diet and the Diabetic Patient. Diabetes Care 1983, 6, 11. [Google Scholar] [CrossRef]


{kind=link}
| The Group Reporting Taking Insulin (n = 774) | The Group Reporting T2D w/o Insulin (n = 2758) | The Group w/o Diabetes (n = 17,796) | p-Value 2 | |
|---|---|---|---|---|
| Sex | 0.0003 * | |||
| Male | 403 (52.1%) | 1416 (51.3%) | 8578 (48.2%) | |
| Female | 371 (47.9%) | 1342 (48.7%) | 9218 (51.8%) | |
| Age in Years | <0.0001 * | |||
| 18–34 | 44 (5.6%) | 121 (4.4%) | 6247 (35.1%) | |
| 35–49 | 91 (11.8%) | 470 (17.0%) | 4633 (26.0%) | |
| 50–80 | 639 (82.6%) | 2167 (78.6%) | 6916 (38.9%) | |
| Survey year | 0.4 | |||
| 2009–2010 | 193 (24.9%) | 766 (27.8%) | 5005 (28.1%) | |
| 2011–2012 | 181 (23.4%) | 647 (23.5%) | 4168 (23.4%) | |
| 2013–2014 | 181 (23.4%) | 660 (23.9%) | 4387 (24.7%) | |
| 2015–2016 | 219 (28.3%) | 685 (24.8%) | 4236 (23.8%) | |
| Race/Ethnicity | <0.0001 * | |||
| Hispanic | 205 (27.7%) | 859 (31.1%) | 4448 (25.0%) | |
| White | 276 (35.7%) | 905 (32.8%) | 7517 (42.2%) | |
| Black | 229 (29.6%) | 692 (25.1%) | 3640 (20.5%) | |
| Other | 54 (7.0%) | 302 (11.0%) | 2191 (12.3%) | |
| Poverty Income Ratio | <0.0001 * | |||
| 0.00–0.99 | 201 (28.1%) | 623 (25.0%) | 3776 (23.2%) | |
| 1.00–1.99 | 220 (30.7%) | 748 (30.0%) | 4219 (25.9%) | |
| 2.00–2.99 | 106 (14.8%) | 384 (15.4%) | 2353 (14.4%) | |
| 3.00–3.99 | 66 (9.2%) | 277 (11.1%) | 1793 (11.0%) | |
| 4.00–5.00 | 123 (17.2%) | 463 (18.5%) | 4156 (25.5%) | |
| Body Mass Index | <0.0001 * | |||
| <25 | 81 (10.9%) | 364 (13.3%) | 5981 (33.9%) | |
| 25–29.9 | 182 (24.5%) | 780 (28.6%) | 5813 (33.0%) | |
| ≥30 | 481 (64.7%) | 1586 (58.1%) | 5843 (33.1%) |
| The Group Reporting Taking Insulin (n = 774) | The Group Reporting T2D w/o Insulin (n = 2758) | The Group w/o Diabetes (n = 17,796) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rank | What We Eat in America item 1 | Weighted Frequency 3,4 | Frequency 5 | Wtd% 4,6 (SE) | What We Eat in America item 1 | Weighted Frequency 3,4 | Frequency 5 | Wtd% 4,6 (SE) | What We Eat in America item 1 | Weighted Frequency 3,4 | Frequency 5 | Wtd% 4,6 (SE) |
| Total | 98,959,094 | 12,095 | 376,469,886 | 43,421 | 3,245,557,852 | 277,244 | ||||||
| 1 | Tap water | 5,294,037 | 579 | 5.3 (0.4) | Tap water | 20,867,328 | 2231 | 5.5 (0.2) | Tap water | 202,005,485 | 15,400 | 6.2 (0.2) |
| 2 | Unsweetened bottled water | 4,341,351 | 600 | 4.4 (0.3) | Unsweetened bottled water | 15,815,995 | 2157 | 4.2 (0.3) | Unsweetened bottled water | 114,654,421 | 11,820 | 3.5 (0.1) |
| 3 | Coffee | 2,867,410 | 336 | 2.9 (0.2) | Coffee | 10,982,634 | 1212 | 2.9 (0.1) | Coffee | 92,688,711 | 6906 | 2.9 (0.1) |
| 4 | Tomatoes | 1,583,968 | 179 | 1.6 (0.2) | Lettuce | 5,520,635 | 597 | 1.5 (0.1) | White sugar | 48,766,824 | 5271 | 1.5 (0.1) |
| 5 | 2% reduced fat milk | 1,483,662 | 187 | 1.5 (0.2) | Tomatoes | 5,499,873 | 598 | 1.5 (0.1) | Lettuce | 45,653,422 | 3684 | 1.4 (0.0) |
| 6 | Soft drink (cola-type, sugar-free) | 1,367,532 | 155 | 1.4 (0.2) | 2% reduced fat milk | 5,377,691 | 613 | 1.4 (0.1) | Soft drink (cola-type) | 43,801,567 | 4172 | 1.3 (0.1) |
| 7 | Lettuce | 1,277,944 | 156 | 1.3 (0.1) | Soft drink (cola-type, sugar-free) | 4,446,739 | 344 | 1.2 (0.1) | Tomatoes | 43,656,646 | 3468 | 1.3 (0.0) |
| 8 | Soft drink (cola-type, decaffeinated) | 867,827 | 86 | 0.9 (0.2) | White sugar | 4,285,836 | 633 | 1.1 (0.1) | 2% Fat-reduced milk | 37,409,699 | 3298 | 1.2 (0.0) |
| 9 | Sugar substitute (saccharin-based) | 850,553 | 124 | 0.9 (0.1) | Banana | 3,928,098 | 530 | 1.0 (0.1) | Banana | 31,398,643 | 2737 | 1.0 (0.0) |
| 10 | Banana | 818,469 | 125 | 0.8 (0.1) | Soft drink (cola-type) | 3,726,509 | 460 | 1.0 (0.1) | Whole milk | 23,685,000 | 2338 | 0.7 (0.0) |
| The Group Reporting Taking Insulin (n = 774) | The Group Reporting T2D w/o Insulin (n = 2758) | The Group w/o Diabetes (n = 17,796) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rank | What We Eat in America subcategory 1 | Weighted Frequency 3,4 | Frequency 5 | Wtd% 4,6 (SE) | What We Eat in America subcategory 1 | Weighted Frequency 3,4 | Frequency 5 | Wtd% 4,6 (SE) | What We Eat in America subcategory 1 | Weighted Frequency 3,4 | Frequency 5 | Wtd% 4,6 (SE) |
| Total | 98,959,094 | 12,095 | 376,469,886 | 43,421 | 3,245,557,852 | 277,244 | ||||||
| 1 | Tap water | 5,356,421 | 585 | 5.4 (0.4) | Tap water | 21,157,722 | 2272 | 5.6 (0.2) | Tap water | 205,305,226 | 15,673 | 6.3 (0.2) |
| 2 | Coffee | 4,409,221 | 560 | 4.5 (0.3) | Coffee | 17,061,047 | 2097 | 4.5 (0.1) | Coffee | 136,685,004 | 11,227 | 4.2 (0.1) |
| 3 | Bottled water | 4,341,351 | 600 | 4.4 (0.3) | Bottled water | 15,815,995 | 2157 | 4.2 (0.3) | Bottled water | 114,654,421 | 11,820 | 3.5 (0.1) |
| 4 | Diet soft drinks | 3,718,166 | 391 | 3.8 (0.4) | Yeast breads | 13,091,450 | 1529 | 3.5 (0.1) | Cheese | 95,913,887 | 7342 | 3.0 (0.1) |
| 5 | Yeast bread | 3,652,103 | 449 | 3.7 (0.2) | Cheese | 9,577,396 | 969 | 2.5 (0.1) | Yeast breads | 95,137,901 | 8275 | 2.9 (0.1) |
| 6 | Tea | 2,584,194 | 293 | 2.6 (0.3) | Tea | 9,519,279 | 1070 | 2.5 (0.2) | Soft drinks | 92,330,988 | 8918 | 2.8 (0.1) |
| 7 | Cheese | 2,261,411 | 265 | 2.3 (0.2) | Diet soft drinks | 8,358,603 | 685 | 2.2 (0.1) | Tea | 73,796,069 | 6327 | 2.3 (0.1) |
| 8 | Sugar substitutes | 2,220,376 | 326 | 2.2 (0.3) | Soft drinks | 7,651,814 | 957 | 2.0 (0.1) | Other vegetables and combinations | 61,835,369 | 5004 | 1.9 (0.0) |
| 9 | Eggs and omelets | 2,000,524 | 255 | 2.0 (0.2) | Other vegetables and combinations | 7,539,753 | 823 | 2.0 (0.1) | Sugars and honey | 60,595,579 | 6302 | 1.9 (0.1) |
| 10 | Cold cuts and cured meats | 1,973,622 | 222 | 2.0 (0.2) | Cream and cream substitutes | 7,361,081 | 858 | 2.0 (0.1) | Lettuce and lettuce salads | 60,358,697 | 4650 | 1.9 (0.0) |
| The Group Reporting Taking Insulin (n = 774) | The Group Reporting T2D w/o Insulin (n = 2758) | The Group w/o Diabetes (n = 17,796) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rank | What We Eat in America Category 1 | Weighted Frequency 3,4 | Frequency 5 | Wtd% 4,6 (SE) | What We Eat in America Category 1 | Weighted Frequency 3,4 | Frequency 5 | Wtd% 4,6 (SE) | What We Eat in America Category 1 | Weighted Frequency 3,4 | Frequency 5 | Wtd% 4,6 (SE) |
| Total | 98,578,506 | 12,039 | 374,707,908 | 43,155 | 3,232,070,662 | 275,796 | ||||||
| 1 | Plain water | 9,697,772 | 1185 | 9.8 (0.4) | Plain water | 36,973,717 | 4429 | 9.9 (0.3) | Plain water | 319,959,647 | 27,493 | 9.9 (0.2) |
| 2 | Vegetables w/o white potato | 9,059,302 | 982 | 9.2 (0.6) | Vegetables w/o white potato | 33,386,898 | 3683 | 8.9 (0.3) | Vegetables w/o white potato | 274,695,816 | 22,064 | 8.5 (0.1) |
| 3 | Coffee & tea | 6,993,415 | 853 | 7.1 (0.3) | Coffee & tea | 26,580,326 | 3167 | 7.1 (0.2) | Coffee & tea | 210,481,073 | 17,554 | 6.5 (0.1) |
| 4 | Fats & oil | 6,975,164 | 799 | 7.1 (0.4) | Fats & oils | 24,735,148 | 2599 | 6.6 (0.2) | Fats & oils | 196,833,742 | 15,227 | 6.1 (0.1) |
| 5 | Breads, rolls, tortillas | 5,814,047 | 704 | 5.9 (0.3) | Breads, rolls, tortillas | 21,868,818 | 2632 | 5.8 (0.1) | Breads, rolls, tortillas | 161,270,439 | 14,243 | 5.0 (0.1) |
| 6 | Fruits | 4,539,100 | 604 | 4.6 (0.3) | Fruits | 17,789,900 | 2199 | 4.7 (0.2) | Fruits | 150,617,266 | 12,803 | 4.7 (0.1) |
| 7 | Diet beverages | 4,191,552 | 449 | 4.3 (0.4) | Condiments and sauces | 15,875,817 | 1788 | 4.2 (0.2) | Condiments and sauces | 148,905,014 | 12,777 | 4.6 (0.1) |
| 8 | Condiments and sauces | 4,117,112 | 470 | 4.2 (0.3) | Sugars | 14,422,141 | 1877 | 3.8 (0.2) | Sweetened beverages | 144,772,013 | 14,108 | 4.5 (0.1) |
| 9 | Sugar | 3,757,238 | 562 | 3.8 (0.3) | Milk | 13,242,566 | 1459 | 3.5 (0.2) | Sugars | 110,810,638 | 10,222 | 3.4 (0.1) |
| 10 | Cured meats/poultry | 3,366,292 | 397 | 3.4 (0.3) | Sweet bakery product | 12,011,790 | 1339 | 3.2 (0.1) | Milk | 103,668,977 | 8770 | 3.2 (0.1) |
| The Group Reporting Taking Insulin (n = 774) | The Group Reporting T2D w/o Insulin (n = 2758) | The Group w/o Diabetes (n = 17,796) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rank | What We Eat in America item 1 | Weighted Energy Contribution 3,4 | Frequency 5 | Wtd% 4,6 (SE) | What We Eat in America item 1 | Weighted Energy Contribution 3,4 | Frequency 5 | Wtd% 4,6 (SE) | What We Eat in America item 1 | Weighted Energy Contribution 3,4 | Frequency 5 | Wtd% 4,6 (SE) |
| Total | 11,173,326,140 | 10,655 | 45,994,398,876 | 38,344 | 438,552,576,789 | 246,981 | ||||||
| 1 | 2% reduced fat milk | 175,158,078 | 187 | 1.5 (0.3) | Soft drink, cola-type | 620,925,847 | 460 | 1.4 (0.1) | Soft drink, cola-type | 7,727,219,654 | 4172 | 1.8 (0.1) |
| 2 | Wheat or cracked wheat bread | 107,505,626 | 85 | 1.0 (0.6) | 2% reduced fat milk | 542,124,845 | 613 | 1.2 (0.1) | Beer (include ale) | 7,624,446,189 | 1643 | 1.7 (0.1) |
| 3 | Soft white roll | 100,546,094 | 54 | 0.9 (0.2) | Whole milk | 495,105,225 | 345 | 1.1 (0.2) | French fries | 4,536,464,186 | 1608 | 1.0 (0.0) |
| 4 | Regular ice cream (not chocolate) | 97,758,809 | 28 | 0.9 (0.3) | Beer (include ale) | 446,611,096 | 133 | 1.0 (0.2) | 2% reduced fat milk | 4,370,770,940 | 3298 | 1.0 (0.1) |
| 5 | White bread | 92,313,363 | 100 | 0.8 (0.1) | French fries | 390,088,888 | 171 | 0.8 (0.1) | Beer, lite | 4,119,958,979 | 1005 | 0.9 (0.1) |
| 6 | Whole wheat bread | 88,551,645 | 59 | 0.8 (0.2) | Banana | 370,150,703 | 530 | 0.8 (0.1) | Ice cream (not chocolate) | 3,839,785,911 | 1133 | 0.9 (0.1) |
| 7 | Soft drink, cola-type | 85,779,001 | 77 | 0.8 (0.2) | Ice cream (not chocolate) | 358,175,595 | 157 | 0.8 (0.1) | Banana | 3,167,442,419 | 2737 | 0.7 (0.0) |
| 8 | White potato | 79,297,997 | 56 | 0.7 (0.1) | White bread | 339,050,117 | 328 | 0.7 (0.1) | Whole milk | 3,063,855,299 | 2338 | 0.7 (0.0) |
| 9 | Banana | 77,782,509 | 125 | 0.7 (0.1) | Soft white roll | 293,239,277 | 242 | 0.6 (0.1) | White bread | 3,028,693,277 | 1902 | 0.7 (0.0) |
| 10 | Whole milk | 77,426,678 | 85 | 0.7 (0.1) | Wheat or cracked wheat bread | 267,359,710 | 275 | 0.6 (0.1) | Soft drink, fruit-flavored, caffeine free | 2,649,165,951 | 2007 | 0.6 (0.0) |
| The Group Reporting Taking Insulin (n = 774) | The Group Reporting T2D w/o Insulin (n = 2758) | The Group w/o Diabetes (n = 17,796) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rank | What we Eat in America subcategory 1 | Weighted Energy Contribution 3,4 | Frequency 5 | Wtd% 4,6 (SE) | What we Eat in America subcategory 1 | Weighted Energy Contribution 3,4 | Frequency 5 | Wtd% 4,6 (SE) | What we Eat in America subcategory 1 | Weighted Energy Contribution 3,4 | Frequency 5 | Wtd% 4,6 (SE) |
| Total | 11,173,326,140 | 10,655 | 45,994,398,876 | 38,344 | 438,552,576,789 | 246,981 | ||||||
| 1 | Yeast breads | 542,059,395 | 449 | 4.9 (0.3) | Yeast breads | 2,015,776,561 | 1529 | 4.4 (0.2) | Pizza | 17,155,217,138 | 2325 | 3.9 (0.2) |
| 2 | Pizza | 352,519,439 | 74 | 3.2 (0.6) | Pizza | 1,630,091,499 | 249 | 3.5 (0.5) | Soft drinks | 16,878,162,486 | 8918 | 3.8 (0.1) |
| 3 | Chicken, whole pieces | 344,627,978 | 182 | 3.1 (0.5) | Cakes and pies | 1,406,511,677 | 386 | 3.1 (0.3) | Yeast breads | 15,025,292,371 | 8275 | 3.4 (0.1) |
| 4 | Eggs and omelets | 322,535,347 | 255 | 2.9 (0.3) | Chicken, whole pieces | 1,276,775,627 | 731 | 2.8 (0.2) | Beer | 12,606,044,121 | 2790 | 2.9 (0.1) |
| 5 | Meat mixed dishes | 279,742,218 | 105 | 2.5 (0.4) | Soft drinks | 1,266,355,047 | 957 | 2.8 (0.2) | Chicken, whole pieces | 11,830,893,925 | 4719 | 2.7 (0.1) |
| 6 | Cakes and pies | 258,928,280 | 91 | 2.3 (0.4) | Cookies and brownies | 1,132,693,357 | 630 | 2.5 (0.2) | Nuts and seeds | 11,385,283,950 | 3925 | 2.6 (0.1) |
| 7 | Cookies and brownies | 245,466,831 | 185 | 2.2 (0.2) | Nuts and seeds | 1,129,967,899 | 563 | 2.5 (0.2) | Burritos and tacos | 10,936,204,042 | 1480 | 2.5 (0.1) |
| 8 | Cheese | 241,035,357 | 265 | 2.2 (0.3) | Burritos and tacos | 1,116,149,548 | 203 | 2.4 (0.4) | Cookies and brownies | 10,449,344,792 | 4386 | 2.4 (0.1) |
| 9 | Burritos and tacos | 238,780,285 | 49 | 2.1 (0.5) | Eggs and omelets | 1,062,625,029 | 770 | 2.3 (0.1) | Cakes and pies | 10,399,896,397 | 2373 | 2.4 (0.1) |
| 10 | Cold cuts and cured meats | 218,354,393 | 222 | 2.0 (0.4) | Meat mixed dishes | 980,422,000 | 371 | 2.1 (0.2) | Cheese | 9,908,844,842 | 7342 | 2.3 (0.1) |
| The Group Reporting Taking Insulin (n = 774) | The Group Reporting T2D w/o Insulin (n = 2758) | The Group w/o Diabetes (n = 17,796) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rank | What We Eat in America category 1 | Weighted Energy Contribution 3,4 | Frequency 5 | Wtd% 4,6 (SE) | What We Eat in America category 1 | Weighted Energy Contribution 3,4 | Frequency 5 | Wtd% 4,6 (SE) | What We Eat in America category 1 | Weighted Energy Contribution 3,4 | Frequency 5 | Wtd% 4,6 (SE) |
| Total | 11,067,583,100 | 10,599 | 45,507,634,682 | 38,078 | 434,779,439,791 | 245,533 | ||||||
| 1 | Breads, rolls, tortillas | 923,994,769 | 704 | 8.3 (0.4) | Breads, rolls, tortillas | 3,653,085,399 | 2632 | 8.0 (0.2) | Sweet bakery product | 27,904,006,131 | 9010 | 6.4 (0.1) |
| 2 | Sweet bakery product | 629,785,636 | 341 | 5.7 (0.5) | Sweet bakery product | 3,257,752,964 | 1339 | 7.2 (0.4) | Breads, rolls, tortillas | 27,497,056,987 | 14,243 | 6.3 (0.1) |
| 3 | Mixed dishes- sandwiches | 550,338,991 | 155 | 5.0 (0.6) | Sweetened beverages | 2,041,686,370 | 1518 | 4.5 (0.2) | Sweetened beverages | 26,867,482,295 | 14,106 | 6.2 (0.1) |
| 4 | Mixed dishes-meat, poultry, seafood | 487,328,523 | 194 | 4.4 (0.5) | Mixed dishes- sandwiches | 1,918,027,605 | 477 | 4.2 (0.3) | Alcoholic beverages | 21,928,960,736 | 5463 | 5.0 (0.2) |
| 5 | Fats & oils | 449,849,893 | 799 | 4.1 (0.3) | Mixed dishes- meat, poultry, seafood | 1,846,139,541 | 703 | 4.1 (0.3) | Mixed dishes- sandwiches | 18,966,260,477 | 3297 | 4.4 (0.1) |
| 6 | Poultry | 441,972,521 | 233 | 4.0 (0.5) | White potatoes | 1,762,408,554 | 842 | 3.9 (0.2) | Mixed dishes- pizza | 17,155,217,138 | 2325 | 3.9 (0.2) |
| 7 | Cured meats/poultry | 427,895,678 | 397 | 3.9 (0.4) | Plant based protein foods | 1,711,721,004 | 1041 | 3.8 (0.2) | Mixed dishes- Mexican | 16,503,304,178 | 2545 | 3.8 (0.2) |
| 8 | White potatoes | 377,782,656 | 216 | 3.4 (0.4) | Poultry | 1,654,562,156 | 915 | 3.6 (0.2) | Poultry | 16,063,883,380 | 6066 | 3.7 (0.1) |
| 9 | Mixed dishes- Mexican | 362,937,339 | 96 | 3.3 (0.6) | Mixed dishes- pizza | 1,630,091,499 | 249 | 3.6 (0.5) | Plant based protein foods | 15,960,314,784 | 6477 | 3.7 (0.1) |
| 10 | Sweetened beverages | 361,977,279 | 336 | 3.3 (0.3) | Mixed dishes- Mexican | 1,602,969,844 | 361 | 3.5 (0.4) | Mixed dishes- grain based | 15,334,421,326 | 2991 | 3.5 (0.1) |
| The Group Reporting Taking Insulin (n = 774) | The Group Reporting T2D w/o Insulin (n = 2758) | the Group w/o Diabetes (n = 17,796) | X2 p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| Broad WWEIA food category 1 | Wtd % 3 of reported foods (SE) | Wtd % 3 of reported energy (SE) | Wtd % 3 of reported foods (SE) | Wtd % 3 of reported energy (SE) | Wtd % 3 of reported foods (SE) | Wtd % 3 of reported energy (SE) | Frequency 4 | Energy 4 |
| Milk/Dairy 5 | 6.9 (0.4) | 6.9 (0.5) | 7.1 (0.2) | 6.6 (0.3) | 7.4 (0.1) | 6.3 (0.1) | 0.1 | 0.3 |
| Protein 6 | 11.4 (0.5) | 18.8 (1.0) | 11.2 (0.2) | 17.2 (0.4) | 10.6 (0.1) | 15.7 (0.2) | 0.01 | <0.0001 * |
| Mixed Dish 7 | 6.9 (0.4) | 22.2 (1.2) | 6.9 (0.2) | 21.7 (0.6) | 7.5 (0.1) | 22.7 (0.3) | 0.004 | 0.3 |
| Grain 8 | 9.7 (0.3) | 15.2 (0.6) | 9.6 (0.2) | 14.3 (0.4) | 8.8 (0.1) | 12.1 (0.2) | <0.0001 * | <0.0001 * |
| Snack/Sweet 9 | 8.5 (0.4) | 13.8 (0.8) | 9.5 (0.2) | 15.4 (0.3) | 10.2 (0.1) | 15.1 (0.2) | <0.0001 * | 0.2 |
| Fruit 10 | 4.6 (0.3) | 2.8 (0.2) | 4.7 (0.2) | 2.7 (0.1) | 4.6 (0.1) | 2.5 (0.1) | 0.9 | 0.05 |
| Vegetable 11 | 11.0 (0.6) | 6.1 (0.5) | 11.0 (0.3) | 6.3 (0.2) | 10.4 (0.1) | 5.4 (0.1) | 0.1 | 0.0009 * |
| Beverage 12 | 14.8 (0.3) | 6.1 (0.4) | 13.9 (0.3) | 7.3 (0.3) | 13.8 (0.1) | 9.5 (0.2) | 0.09 | <0.0001 * |
| Alcohol 13 | 0.9 (0.2) | 2.4 (0.5) | 1.2 (0.1) | 2.9 (0.3) | 2.1 (0.1) | 5.0 (0.2) | <0.0001 * | <0.0001 * |
| Water 14 | 10.2 (0.4) | 0.0 (0.0) | 10.1 (0.4) | 0.0 (0.0) | 10.2 (0.2) | 0.1 (0.0) | 0.9 | 0.0011 * |
| Fat/Oil 15 | 7.1 (0.4) | 4.0 (0.3) | 6.6 (0.2) | 3.5 (0.1) | 6.1 (0.1) | 3.2 (0.1) | 0.002 | 0.003 |
| Cond 16/ Sauce 17 | 4.2 (0.3) | 0.9 (0.1) | 4.2 (0.2) | 0.9 (0.1) | 4.6 (0.1) | 1.0 (0.0) | 0.09 | 0.6 |
| Sugars 18 | 3.8 (0.3) | 0.8 (0.1) | 3.8 (0.2) | 1.1 (0.1) | 3.4 (0.1) | 1.2 (0.0) | 0.05 | 0.08 |
| Other | 0.2 (0.1) | 0.1 (0.0) | 0.2 (0.0) | 0.1 (0.0) | 0.4 (0.0) | 0.3 (0.0) | 0.006 | <0.0001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, L.; Zhu, F.; Delp, E.J.; Eicher-Miller, H.A. Differences in Dietary Intake Exist among U.S. Adults by Diabetic Status Using NHANES 2009–2016. Nutrients 2022, 14, 3284. https://doi.org/10.3390/nu14163284
Lin L, Zhu F, Delp EJ, Eicher-Miller HA. Differences in Dietary Intake Exist among U.S. Adults by Diabetic Status Using NHANES 2009–2016. Nutrients. 2022; 14(16):3284. https://doi.org/10.3390/nu14163284
Chicago/Turabian StyleLin, Luotao, Fengqing Zhu, Edward J. Delp, and Heather A. Eicher-Miller. 2022. "Differences in Dietary Intake Exist among U.S. Adults by Diabetic Status Using NHANES 2009–2016" Nutrients 14, no. 16: 3284. https://doi.org/10.3390/nu14163284
APA StyleLin, L., Zhu, F., Delp, E. J., & Eicher-Miller, H. A. (2022). Differences in Dietary Intake Exist among U.S. Adults by Diabetic Status Using NHANES 2009–2016. Nutrients, 14(16), 3284. https://doi.org/10.3390/nu14163284