
Methodological Rigor and Transparency in Clinical Practice Guidelines for Nutrition Care in Critically Ill Adults: A Systematic Review Using the AGREE II and AGREE-REX Tools

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
- A CPG intended to guide nutrition care in a critically ill adult population within the intensive care unit (ICU);
- Developed via a systematic search of the literature and included an accepted system to rate the level of evidence and;
- Developed by a professional society or academic group.
- Previous versions of the same guideline (if recommendations on a similar topic were included);
- Guidelines that focus on the recovery, rehabilitation, or post-ICU period only;
- Guidelines or independent CPG recommendations that are specific to patients with COVID-19;
- Published prior to 2011.
2.2. Information Sources and Search Strategy
2.3. Selection Process
2.4. Data Collection Process and Collation of Materials
2.5. Quality Assessment
2.6. Synthesis of Results
2.7. Intraclass Correlation (ICC) Analysis
3. Results
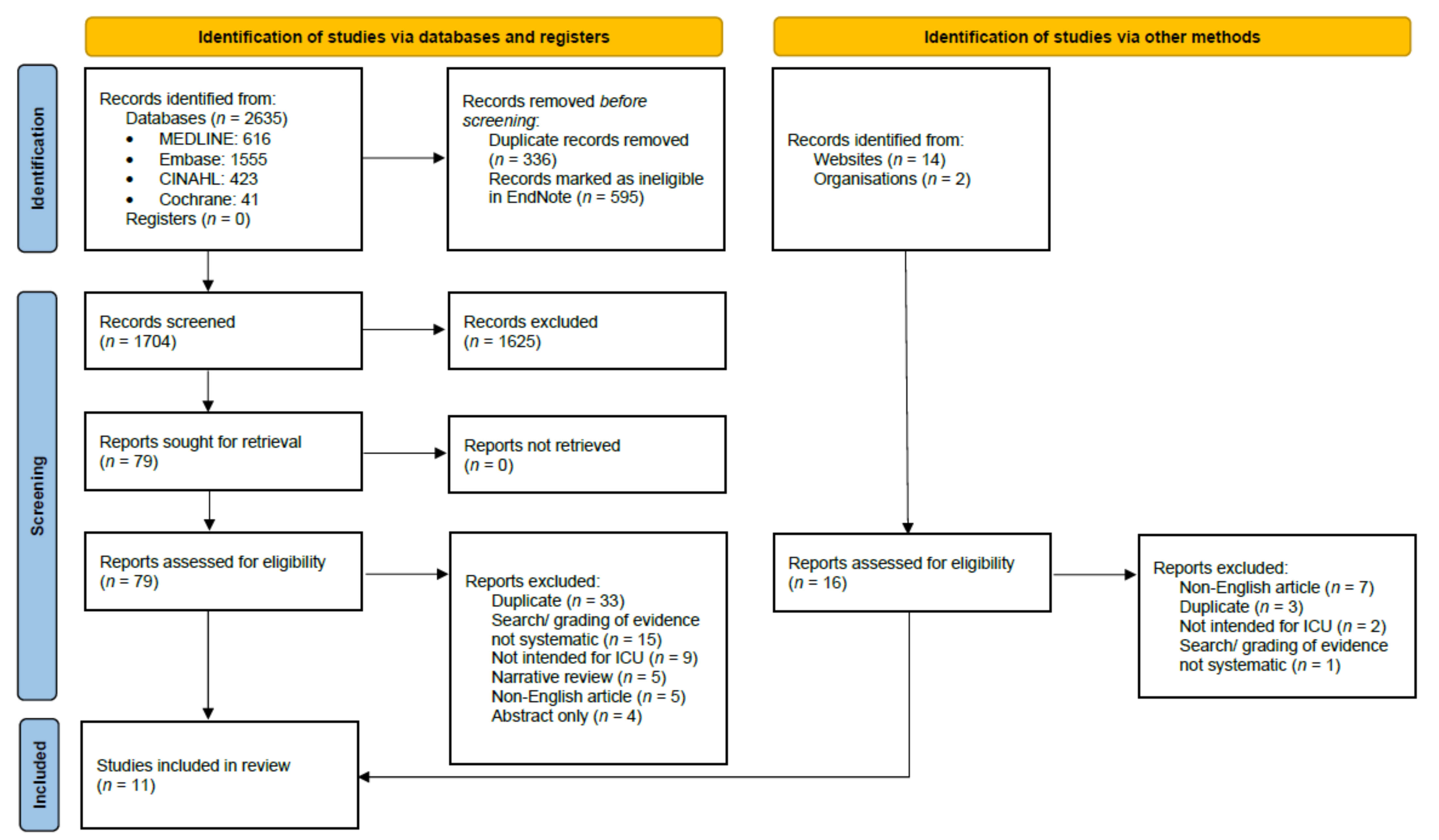
3.1. Study Selection
3.2. Study Characteristics
3.3. Assessment of CPGs Using the AGREE II Tool
3.3.1. Domain and Overall Scores
3.3.2. Item Scores
3.3.3. Agreement between Assessors with the AGREE II Tool
3.4. Assessment of Recommendations Using the AGREE-REX Tool
3.4.1. Domain and Overall Scores
3.4.2. Item Scores
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cruz, J.E.; Fahim, G.; Moore, K. Practice Guideline Development, Grading, and Assessment. Pharm. Ther. 2015, 40, 854–857. [Google Scholar]
- Johnston, A.; Kelly, S.E.; Hsieh, S.-C.; Skidmore, B.; Wells, G.A. Systematic reviews of clinical practice guidelines: A methodological guide. J. Clin. Epidemiol. 2019, 108, 64–76. [Google Scholar] [CrossRef] [PubMed]
- Lambell, K.J.; Tatucu-Babet, O.A.; Chapple, L.A.; Gantner, D.; Ridley, E.J. Nutrition therapy in critical illness: A review of the literature for clinicians. Crit. Care 2020, 24, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakr, Y.; Alhussami, I.; Nanchal, R.; Wunderink, R.G.; Pellis, T.; Wittebole, X.; Martin-Loeches, I.; François, B.; Leone, M.; Vincent, J.-L. Being Overweight Is Associated with Greater Survival in ICU Patients: Results From the Intensive Care Over Nations Audit. Crit. Care Med. 2015, 43, 2623–2632. [Google Scholar] [CrossRef] [Green Version]
- Kross, E.K.; Sena, M.; Schmidt, K.; Stapleton, R.D. A comparison of predictive equations of energy expenditure and measured energy expenditure in critically ill patients. J. Crit. Care 2012, 27, 321.e5–321.e12. [Google Scholar] [CrossRef] [Green Version]
- Walker, R.N.; Heuberger, R.A. Predictive equations for energy needs for the critically ill. Respir. Care 2009, 54, 509–521. [Google Scholar]
- Brouwers, M.C.; Kho, M.E.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Grimshaw, J.; Hanna, S.E.; et al. AGREE II: Advancing guideline development, reporting and evaluation in health care. Can. Med. Assoc. J. 2010, 182, E839–E842. [Google Scholar] [CrossRef] [Green Version]
- Brouwers, M.C.; Spithoff, K.; Kerkvliet, K.; Alonso-Coello, P.; Burgers, J.; Cluzeau, F.; Férvers, B.; Graham, I.; Grimshaw, J.; Hanna, S.; et al. Development and Validation of a Tool to Assess the Quality of Clinical Practice Guideline Recommendations. JAMA Netw. Open 2020, 3, e205535. [Google Scholar] [CrossRef]
- Patel, J.J.; Lemieux, M.; McClave, S.A.; Martindale, R.G.; Hurt, R.T.; Heyland, D.K. Critical Care Nutrition Support Best Practices: Key Differences Between Canadian and American Guidelines. Nutr. Clin. Pract. 2017, 32, 633–644. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Tatucu-Babet, O.A.; Nguo, K.; Lambell, K.J.; Romero, L.; Earthman, C.P.; Ridley, E.J. Doubly labelled water for determining total energy expenditure in adult critically ill and acute care hospitalized inpatients: A scoping review. Clin. Nutr. 2022, 41, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Chapple, L.A.S.; Tatucu-Babet, O.A.; Lambell, K.J.; Fetterplace, K.; Ridley, E.J. Nutrition guidelines for critically ill adults admitted with COVID-19: Is there consensus? Clin. Nutr. ESPEN 2021, 44, 69–77. [Google Scholar] [CrossRef] [PubMed]
- AGREE-REX Research Team. The Appraisal of Guidelines Research & Evaluation—Recommendation EXcellence (AGREE-REX) [Electronic Version]. 2019. Available online: https://www.agreetrust.org/wp-content/uploads/2021/07/AGREE-REX-Tool-PDF-version.pdf (accessed on 12 September 2021).
- AGREE Next Steps Consortium. The AGREE II Instrument [Electronic Version]. 2013. Available online: http://www.agreetrust.org. (accessed on 12 September 2021).
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, P.; Blaser, A.R.; Berger, M.M.; Alhazzani, W.; Calder, P.C.; Casaer, M.P.; Hiesmayr, M.; Mayer, K.; Montejo, J.C.; Pichard, C.; et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin. Nutr. 2019, 38, 48–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rousseau, A.-F.; Losser, M.-R.; Ichai, C.; Berger, M.M. ESPEN endorsed recommendations: Nutritional therapy in major burns. Clin. Nutr. 2013, 32, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Elke, G.; Hartl, W.H.; Kreymann, K.G.; Adolph, M.; Felbinger, T.W.; Graf, T.; de Heer, G.; Heller, A.R.; Kampa, U.; Mayer, K.; et al. Clinical Nutrition in Critical Care Medicine—Guideline of the German Society for Nutritional Medicine (DGEM). Clin. Nutr. ESPEN 2019, 33, 220–275. [Google Scholar] [CrossRef]
- Reintam, A.; Starkopf, J.; Alhazzani, W.; Berger, M.M.; Casaer, M.P.; Deane, A.M.; Fruhwald, S.; Hiesmayr, M.; Ichai, C.; Jakob, S.M.; et al. Early enteral nutrition in critically ill patients: ESICM clinical practice guidelines. Intensive Care Med. 2017, 43, 380–398. [Google Scholar] [CrossRef]
- Mesejo, A.; Alonso, C.V.; Escribano, J.A.; Leyba, C.O.; González, J.M. [Guidelines for specialized nutritional and metabolic support in the critically-ill patient. Update. Consensus of the Spanish Society of Intensive Care Medicine and Coronary Units-Spanish Society of Parenteral and Enteral Nutrition (SEMICYUC-SENPE): Introduction and methodology]. Med. Intensiv. 2011, 35, 1–6. [Google Scholar] [CrossRef]
- Heyland, D.K.; Lee, Z.-Y.; Yap, C.; Ortiz, L.A.; Clark, J.; Dhaliwal, R. Systematic Reviews by Critical Care Nutrition. Critical Care Nutrition. 2021. Available online: https://www.criticalcarenutrition.com/systematic-reviews (accessed on 1 October 2021).
- Academy of Nutrition and Dietetics. Critical illness (CI) guidelines. [Electronic version]. 2012. Available online: https://www.andeal.org/topic.cfm?menu=4800 (accessed on 1 October 2021).
- Compher, C.; Bingham, A.L.; McCall, M.; Patel, J.; Rice, T.W.; Braunschweig, C.; McKeever, L. Guidelines for the provision of nutrition support therapy in the adult critically ill patient: The American Society for Parenteral and Enteral Nutrition. J. Parenter. Enter. Nutr. 2022, 46, 12–41. [Google Scholar] [CrossRef]
- McClave, S.A.; Taylor, B.E.; Martindale, R.G.; Warren, M.M.; Johnson, D.R.; Braunschweig, C.; McCarthy, M.S.; Davanos, E.; Rice, T.W.; Cresci, G.A.; et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (ASPEN). JPEN J. Parenter. Enter. Nutr. 2016, 40, 159–211. [Google Scholar] [CrossRef]
- Mithal, A.; Sharma, J.; Kulkarni, A.P.; Sivakumar, M.; Mehta, Y.; Chakravarti, S.; Joshi, A.; Reddy, B.R.; Bathina, H. Practice Guidelines for Enteral Nutrition Management in Dysglycemic Critically Ill Patients: A Relook for Indian Scenario. Indian, J. Crit. Care Med. 2019, 23, 594–603. [Google Scholar] [CrossRef] [PubMed]
- Mageswary, L.; Chong, M.-K.; Majid, H.; Khor, B.H.; Lee, Z.-Y.; Hafizatul, A.; Ong, S.-H.; Rosli, M.S.; Hawa, M.T.S.; Tan, H.-Y. Medical Nutrition Therapy (MNT) Guidelines for Critically Ill Adults 2017; Malaysian Dietitians’ Association: Kuala Lumpur, Malaysia, 2017. [Google Scholar]
- Solà, I.; Carrasco, J.M.; Del Campo, P.D.; Gracia, J.; Orrego, C.; Martínez, F.; Kotzeva, A.; Guillamón, I.; Calderon, E.; de Gaminde, I.; et al. Attitudes and Perceptions about Clinical Guidelines: A Qualitative Study with Spanish Physicians. PLoS ONE 2014, 9, e86065. [Google Scholar] [CrossRef] [PubMed]
- Petkovic, J.; Riddle, A.; Akl, E.A.; Khabsa, J.; Lytvyn, L.; Atwere, P.; Campbell, P.; Chalkidou, K.; Chang, S.M.; Crowe, S.; et al. Protocol for the development of guidance for stakeholder engagement in health and healthcare guideline development and implementation. Syst. Rev. 2020, 9, 21. [Google Scholar] [CrossRef] [PubMed]
- Magwood, O.; Riddle, A.; Petkovic, J.; Lytvyn, L.; Khabsa, J.; Atwere, P.; Akl, E.A.; Campbell, P.; Welch, V.; Smith, M.; et al. PROTOCOL: Barriers and facilitators to stakeholder engagement in health guideline development: A qualitative evidence synthesis. Campbell Syst. Rev. 2022, 18, e1237. [Google Scholar] [CrossRef]
- Graham, R.; Mancher, M.; Wolman, D.M.; Greenfield, S.; Steinberg, E. Current Best Practices and Proposed Standards for Development of Trustworthy CPGs: Part 1, Getting Started. In Clinical Practice Guidelines We Can Trust; National Academies Press (US): Washington, DC, USA, 2011. [Google Scholar]
- Frank, L.; Basch, E.; Selby, J.V. The PCORI Perspective on Patient-Centered Outcomes Research. JAMA 2014, 312, 1513–1514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feemster, L.C.; Saft, H.L.; Bartlett, S.J.; Parthasarathy, S.; Barnes, T.; Calverley, P.; Curtis, J.R.; Hickam, D.H.; Mularski, R.A.; Au, D.H.; et al. Patient-centered Outcomes Research in Pulmonary, Critical Care, and Sleep Medicine. An Official American Thoracic Society Workshop Report. Ann. Am. Thorac. Soc. 2018, 15, 1005–1015. [Google Scholar] [CrossRef]
- Dinglas, V.D.; Chessare, C.M.; Davis, W.E.; Parker, A.; Friedman, L.A.; Colantuoni, E.; Bingham, C.O.; Turnbull, A.; Needham, D.M. Perspectives of survivors, families and researchers on key outcomes for research in acute respiratory failure. Thorax 2018, 73, 7–12. [Google Scholar] [CrossRef]
- Tricco, A.C.; Zarin, W.; Rios, P.; Nincic, V.; Khan, P.A.; Ghassemi, M.; Diaz, S.; Pham, B.; Straus, S.E.; Langlois, E.V. Engaging policy-makers, health system managers, and policy analysts in the knowledge synthesis process: A scoping review. Implement. Sci. 2018, 13, 31. [Google Scholar] [CrossRef] [Green Version]
- Hill, J.E.; Stephani, A.-M.; Sapple, P.; Clegg, A.J. The effectiveness of continuous quality improvement for developing professional practice and improving health care outcomes: A systematic review. Implement. Sci. 2020, 15, 23. [Google Scholar] [CrossRef]
- Horbar, J.D.; Carpenter, J.H.; Buzas, J.; Soll, R.F.; Suresh, G.; Bracken, M.B.; Leviton, L.C.; Plsek, P.E.; Sinclair, J.C. Collaborative quality improvement to promote evidence based surfactant for preterm infants: A cluster randomised trial. BMJ 2004, 329, 1004. [Google Scholar] [CrossRef] [Green Version]
- Innvaer, S.; Vist, G.; Trommald, M.; Oxman, A. Health policy-makers’ perceptions of their use of evidence: A systematic review. J. Health Serv. Res. Policy 2002, 7, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Langlois, E.V.; Montekio, V.B.; Young, T.; Song, K.; Alcalde-Rabanal, J.; Tran, N. Enhancing evidence informed policymaking in complex health systems: Lessons from multi-site collaborative approaches. Health Res. Policy Syst. 2016, 14, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francke, A.L.; Smit, M.C.; de Veer, A.J.; Mistiaen, P. Factors influencing the implementation of clinical guidelines for health care professionals: A systematic meta-review. BMC Med. Inform. Decis. Mak. 2008, 8, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanabria, A.J.; Kotzeva, A.; Olid, A.S.; Pequeño, S.; Vernooij, R.W.; García, L.M.; Zhang, Y.; Solà, I.; Thornton, J.; Alonso-Coello, P. Most guideline organizations lack explicit guidance in how to incorporate cost considerations. J. Clin. Epidemiol. 2019, 116, 72–83. [Google Scholar] [CrossRef] [PubMed]
- Flodgren, G.; Hall, A.M.; Goulding, L.; Eccles, M.P.; Grimshaw, J.M.; Leng, G.C.; Shepperd, S. Tools developed and disseminated by guideline producers to promote the uptake of their guidelines. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [Green Version]
- Cattani, A.; Teixeira, P.P.; Eckert, I.d.C.; Busnello, F.M.; Gabriel, F.C.; Stein, A.T.; Silva, F.M. Quality appraisal of clinical nutrition practice guidelines for critically ill adult patients: A systematic review using the AGREE II and AGREE-REX tools. Br. J. Nutr. 2022, 1–34. [Google Scholar] [CrossRef]
- Padilla, P.F.; Martínez, G.; Vernooij, R.W.; Cosp, X.B.; Alonso-Coello, P. Nutrition in critically ill adults: A systematic quality assessment of clinical practice guidelines. Clin. Nutr. 2016, 35, 1219–1225. [Google Scholar] [CrossRef]


{kind=link}
| Organization/Group Publishing | Title of CPG | Year of Publication | Origin of Contributors | Evidence Grading Method Used | EE General Recommendations | EE Obesity Recommendations |
|---|---|---|---|---|---|---|
| ADA [22] | Critical illness: major recommendations 2012 | 2012 | USA | AAP |  | |
| ASPEN [23] | Guidelines for the provision of nutrition support therapy in the adult critically ill patient | 2022 | USA | GRADE |  | |
| ASPEN/SCCM [24] | Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: SCCM and A.S.P.E.N. | 2016 | USA | GRADE | | |
| Critical Care Nutrition [21] | Critical care nutrition systematic review | 2021 | Canada | Own grading system | | |
| DGEM [18] | Clinical nutrition in critical care medicine—Guideline of the German Society for Nutritional Medicine (DGEM) | 2019 | Germany | AWMF regulations | | |
| ESCIM [19] | Early enteral nutrition in critically illpatients: ESICM clinical practice guidelines | 2017 | Europe | GRADE | | |
| ESPEN [16] | ESPEN guideline on clinical nutrition in the intensive care unit | 2019 | Europe | GRADE | | |
| ESPEN Burns [17] | ESPEN endorsed recommendations: nutritional therapy in major burns | 2013 | France | GRADE | | |
| IAB [25] | Practice guidelines for enteral nutrition management in dysglycemic critically ill patients: a relook for Indian scenario | 2019 | India | Own grading system | | |
| MDA [26] | Medical nutrition therapy (MNT) guidelines for critically ill adults | 2017 | Malaysia | GRADE | | |
| SEMICYUC-SENPE [20] | Guidelines for specialized nutritional and metabolic support in the critically ill patient. Update. Consensus SEMICYUC-SENPE | 2011 | Spain | GRADE | | |
, energy expenditure recommendation included in CPG; , energy expenditure recommendation not included in CPG. Abbreviations: AAP, American Association of Pediatrics; ADA, Academy of Nutrition and Dietetics; ASPEN, American Society for Parenteral and Enteral Nutrition; AWMF, Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (the Association of the Scientific Medical Societies in Germany); CPG, clinical practice guidelines; DGEM, Deutsche Gesellschaft für Ernährungsmedizin (German Society for Nutritional Medicine); EE, energy expenditure; ESCIM, the European Society of Intensive Care Medicine (ESICM); ESPEN, European Society for Clinical Nutrition and Metabolism; GRADE; Grading of Recommendations, Assessment, Development and Evaluations; IAB, advisory board from nine healthcare centers across India; MDA, Malaysian Dietitians’ Association; SCCM, Society of Critical Care Medicine; SEMICYUC, La Sociedad Española de Medicina Intensiva, Crítica y Unidades Coronarias (Spanish Society of Intensive and Critical Care Medicine and Coronary Units); SENPE, Sociedad Española de Nutrición Clínica y Metabolismo (the Spanish Society of Parenteral and Enteral Nutrition).| Clinical Practice Guidelines | Scope and Purpose | Stakeholder Involvement | Rigor of Development | Clarity of Presentation | Applicability | Editorial Independence |
|---|---|---|---|---|---|---|
| ADA [22] | 78 b | 63 c | 63 b | 87 c | 76 c | 48 a |
| ASPEN [23] | 69 a | 46 b | 62 b | 60 a | 43 c | 63 b |
| ASPEN/SCCM [24] | 80 b | 64 c | 76 c | 89 c | 40 c | 68 c |
| Critical Care Nutrition [21] | 89 c | 30 a | 66 c | 82 b | 11 a | 5 a |
| DGEM [18] | 82 c | 48 b | 50 b | 81 b | 37 b | 78 c |
| ESCIM [19] | 84 c | 41 b | 66 c | 84 b | 36 b | 83 c |
| ESPEN [16] | 76 b | 27 a | 65 b | 76 a | 38 b | 65 b |
| ESPEN Burns [17] | 46 a | 20 a | 40 a | 87 c | 19 a | 67 c |
| IAB [25] | 62 a | 47 b | 26 a | 72 a | 46 c | 17 a |
| MDA [26] | 92 c | 53 c | 43 a | 88 c | 37 b | 42 a |
| SEMICYUC-SENPE [20] | 54 a | 37 a | 42 a | 76 a | 28 a | 52 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noyahr, J.K.; Tatucu-Babet, O.A.; Chapple, L.-a.S.; Barlow, C.J.; Chapman, M.J.; Deane, A.M.; Fetterplace, K.; Hodgson, C.L.; Winderlich, J.; Udy, A.A.; et al. Methodological Rigor and Transparency in Clinical Practice Guidelines for Nutrition Care in Critically Ill Adults: A Systematic Review Using the AGREE II and AGREE-REX Tools. Nutrients 2022, 14, 2603. https://doi.org/10.3390/nu14132603
Noyahr JK, Tatucu-Babet OA, Chapple L-aS, Barlow CJ, Chapman MJ, Deane AM, Fetterplace K, Hodgson CL, Winderlich J, Udy AA, et al. Methodological Rigor and Transparency in Clinical Practice Guidelines for Nutrition Care in Critically Ill Adults: A Systematic Review Using the AGREE II and AGREE-REX Tools. Nutrients. 2022; 14(13):2603. https://doi.org/10.3390/nu14132603
Chicago/Turabian StyleNoyahr, John K., Oana A. Tatucu-Babet, Lee-anne S. Chapple, Christopher Jake Barlow, Marianne J. Chapman, Adam M. Deane, Kate Fetterplace, Carol L. Hodgson, Jacinta Winderlich, Andrew A. Udy, and et al. 2022. "Methodological Rigor and Transparency in Clinical Practice Guidelines for Nutrition Care in Critically Ill Adults: A Systematic Review Using the AGREE II and AGREE-REX Tools" Nutrients 14, no. 13: 2603. https://doi.org/10.3390/nu14132603
APA StyleNoyahr, J. K., Tatucu-Babet, O. A., Chapple, L.-a. S., Barlow, C. J., Chapman, M. J., Deane, A. M., Fetterplace, K., Hodgson, C. L., Winderlich, J., Udy, A. A., Marshall, A. P., & Ridley, E. J. (2022). Methodological Rigor and Transparency in Clinical Practice Guidelines for Nutrition Care in Critically Ill Adults: A Systematic Review Using the AGREE II and AGREE-REX Tools. Nutrients, 14(13), 2603. https://doi.org/10.3390/nu14132603