
Interventions That Successfully Reduced Adults Salt Intake—A Systematic Review

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.1.1. Types of Studies
2.1.2. Types of Participants
2.1.3. Types of Intervention
2.1.4. Types of Outcome Measures
2.2. Information Sources
2.3. Search Strategy
2.4. Selection Process
2.5. Data Collection Process
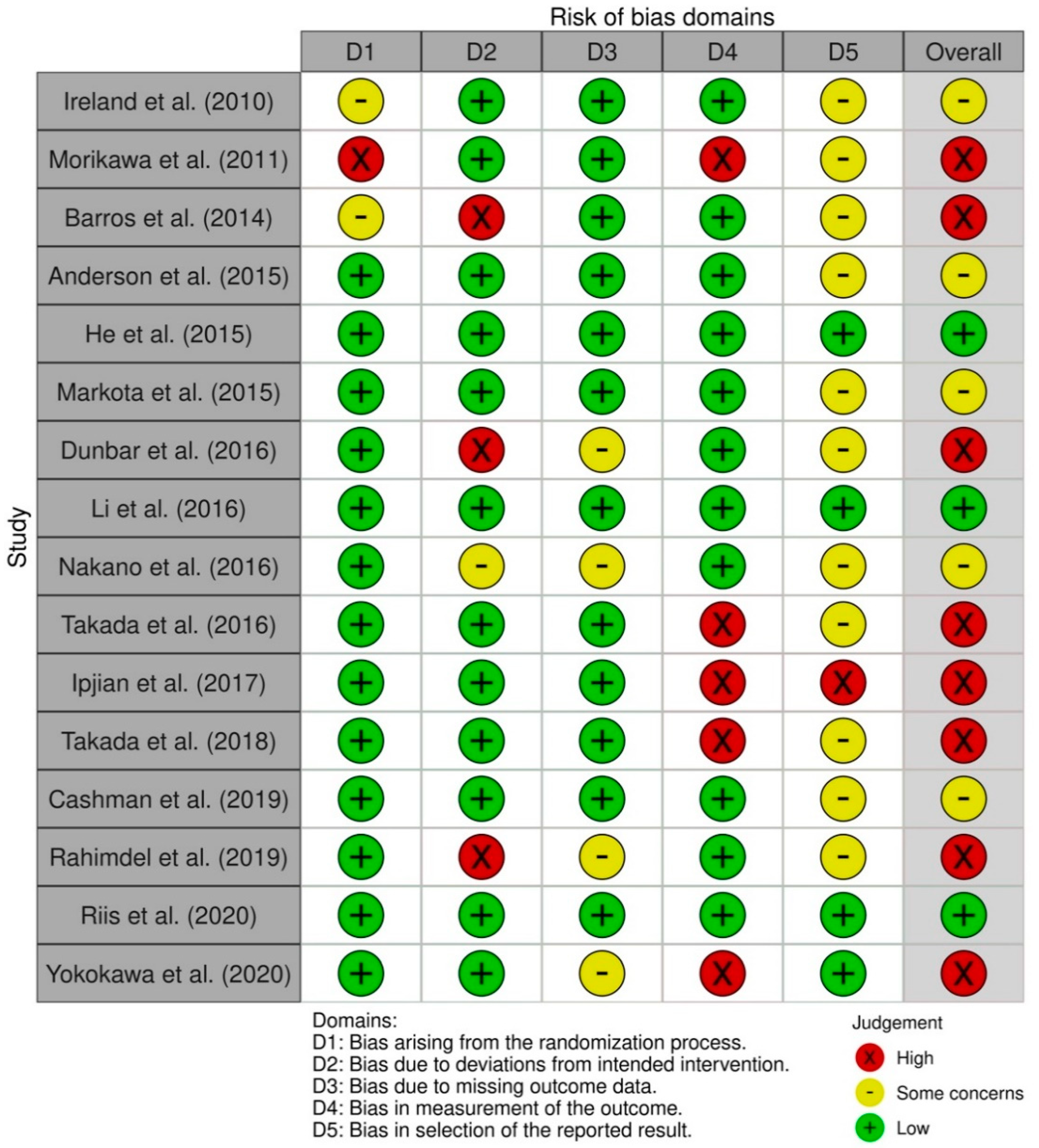
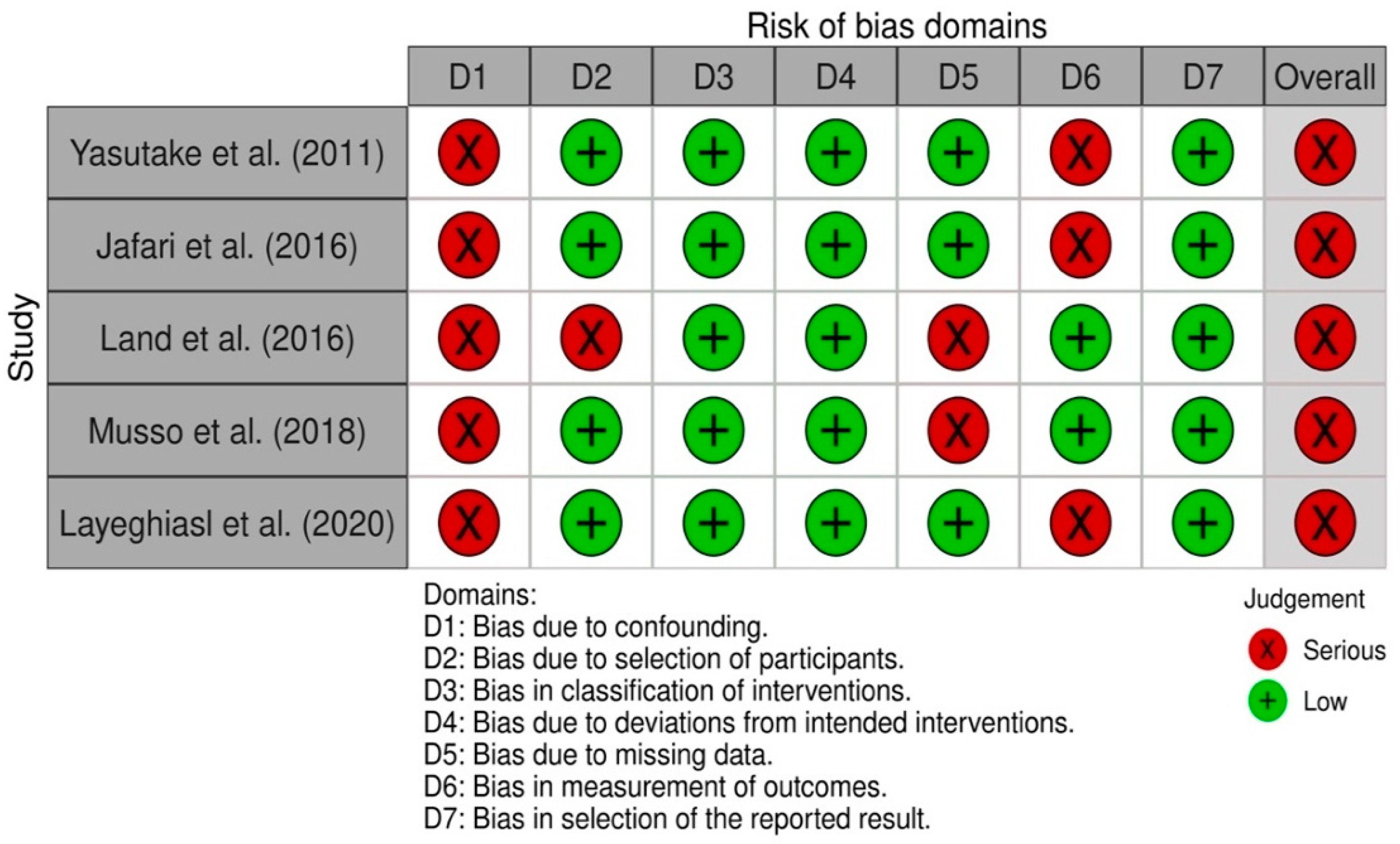
2.6. Study Risk of Bias Assessment
3. Results
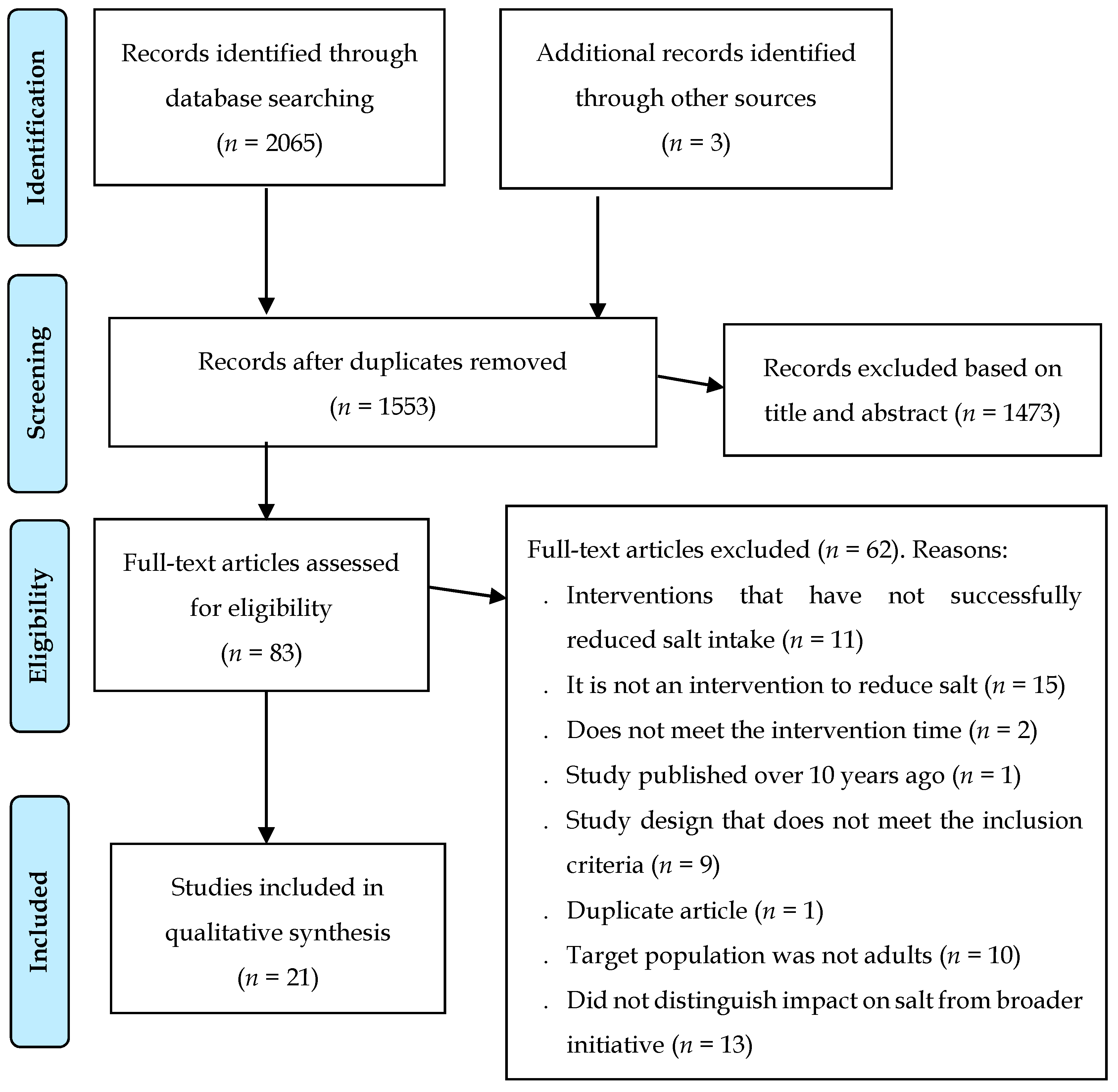
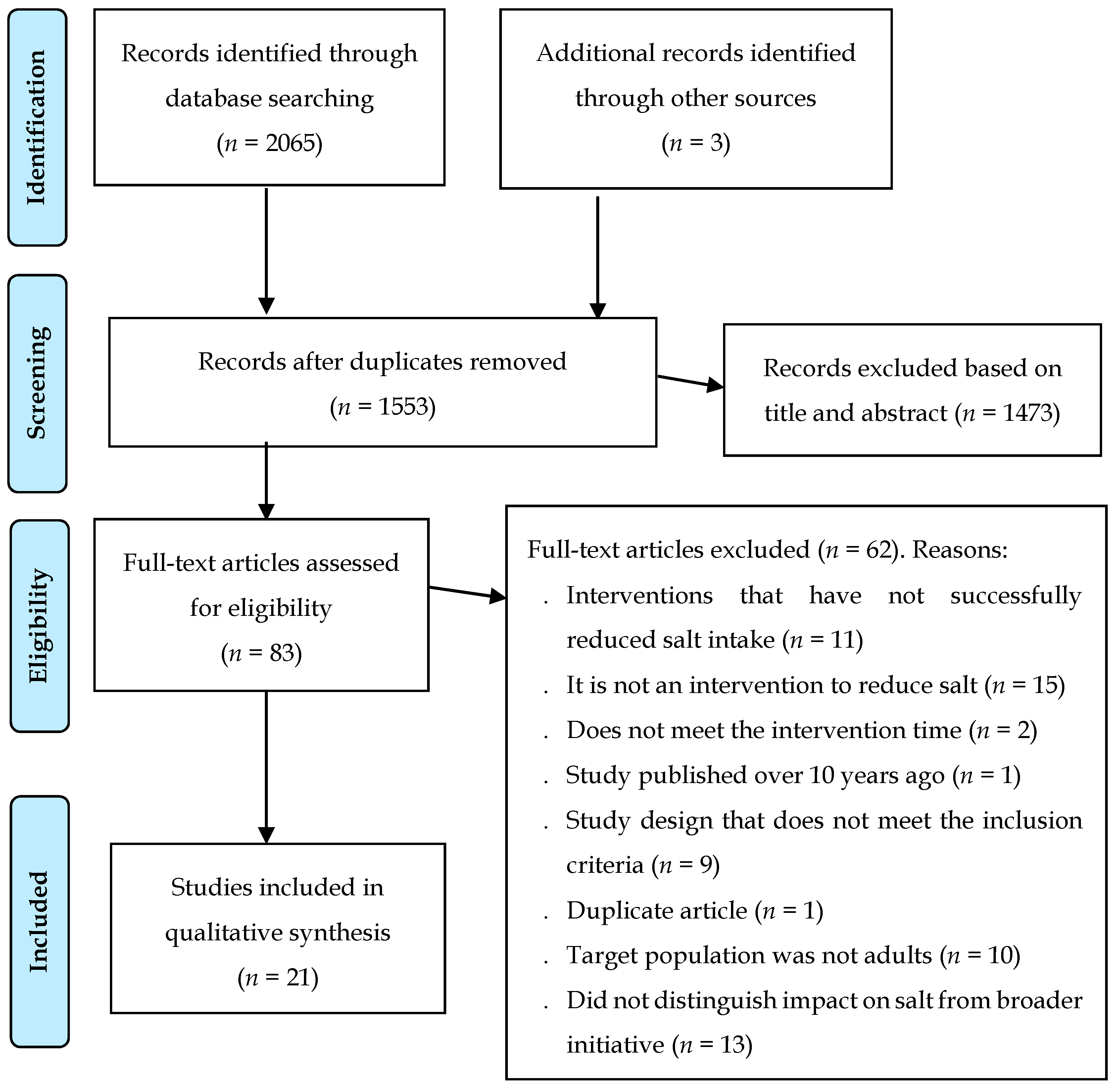
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Participants Characteristics
3.2.2. Interventions Characteristics
3.2.3. Outcome Characteristics
3.3. Types of Interventions
3.3.1. Health and Nutritional Education
3.3.2. Effects of Interventions
3.3.3. Nutritional Education plus Other Interventions
3.3.4. Effects of Interventions
3.3.5. Estimates of Salt Intake
3.3.6. Effects of Interventions
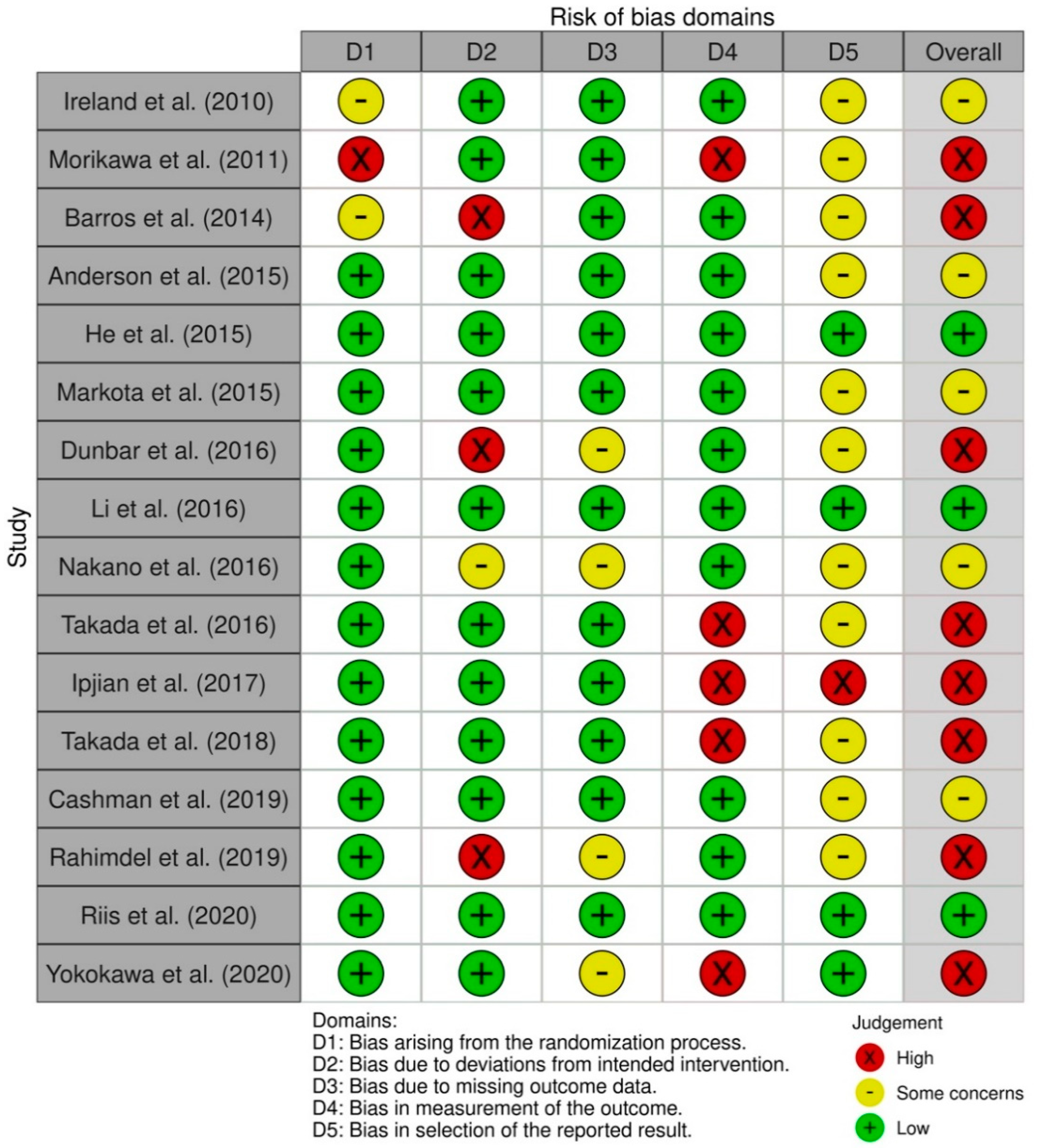
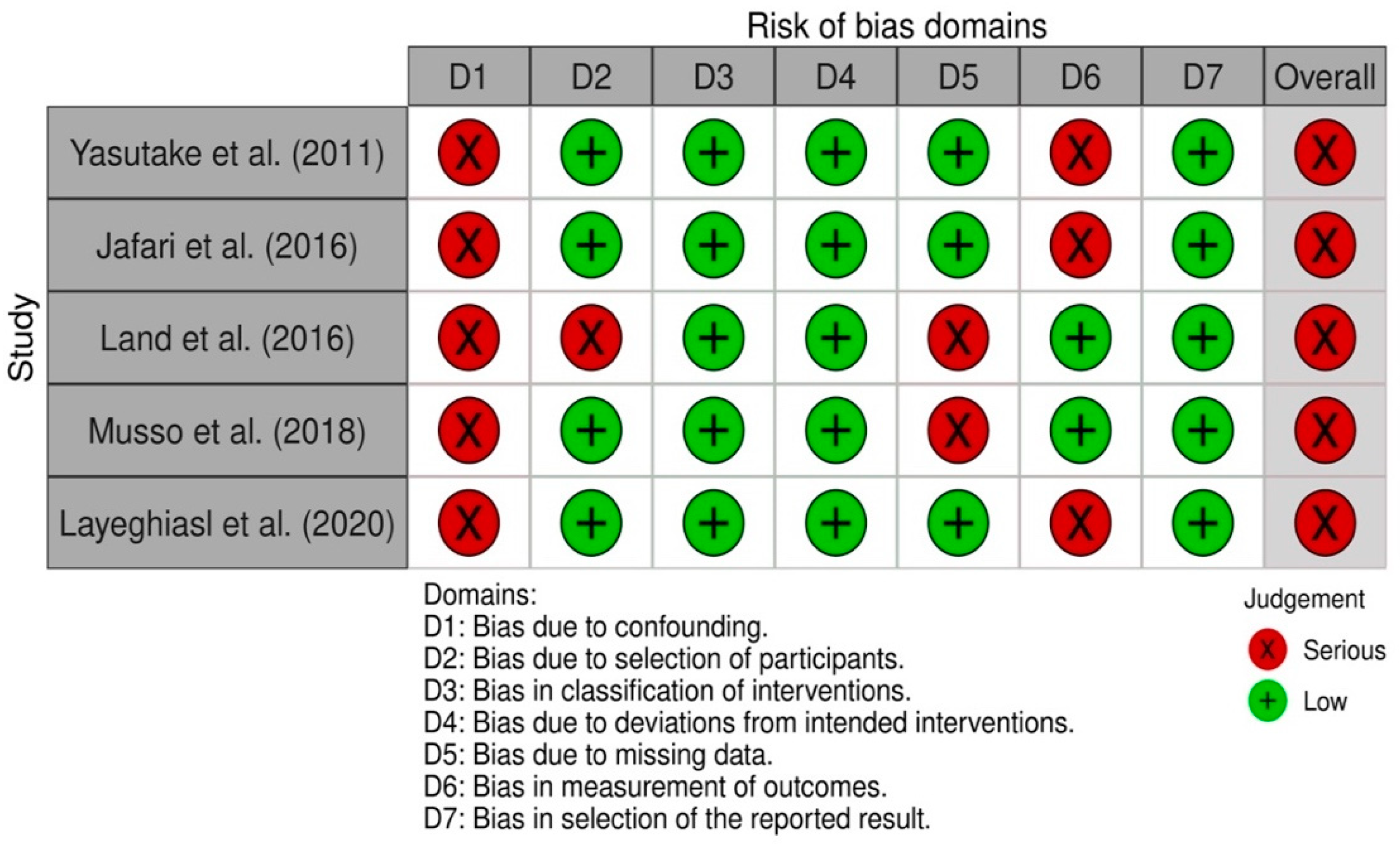
3.4. Risk Ob Bias in Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; Amann, M.; Anderson, H.R.; Andrews, K.G.; Aryee, M.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Causes of Death 2008: Data Sources and Methods; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Graudal, N.A.; Hubeck-Graudal, T.; Jurgens, G. Effects of low sodium diet versus high sodium diet on blood pressure, renin, aldosterone, catecholamines, cholesterol, and triglyceride. Cochrane Database Syst. Rev. 2011, Cd004022. [Google Scholar] [CrossRef]
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Guideline: Sodium Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- He, F.J.; Li, J.; Macgregor, G.A. Effect of longer term modest salt reduction on blood pressure: Cochrane systematic review and meta-analysis of randomised trials. BMJ 2013, 346, f1325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bibbins-Domingo, K.; Chertow, G.M.; Coxson, P.G.; Moran, A.; Lightwood, J.M.; Pletcher, M.J.; Goldman, L. Projected effect of dietary salt reductions on future cardiovascular disease. N. Engl. J. Med. 2010, 362, 590–599. [Google Scholar] [CrossRef] [Green Version]
- Beaglehole, R.; Bonita, R.; Horton, R.; Adams, C.; Alleyne, G.; Asaria, P.; Baugh, V.; Bekedam, H.; Billo, N.; Casswell, S.; et al. Priority actions for the non-communicable disease crisis. Lancet 2011, 377, 1438–1447. [Google Scholar] [CrossRef]
- World Health Assembly. Follow-Up to the Political Declaration of the High-Level Meeting of the General Assembly on the Prevention and Control of Non-Communicable Diseases; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Global Nutrition Report: Action on Equity to End Malnutrition. Available online: https://globalnutritionreport.org/reports/2020-global-nutrition-report/ (accessed on 20 December 2021).
- Trieu, K.; Neal, B.; Hawkes, C.; Dunford, E.; Campbell, N.; Rodriguez-Fernandez, R.; Legetic, B.; McLaren, L.; Barberio, A.; Webster, J. Salt Reduction Initiatives around the World-A Systematic Review of Progress towards the Global Target. PLoS ONE 2015, 10, e0130247. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. The SHAKE Technical Package for Salt Reduction. Available online: https://apps.who.int/iris/handle/10665/250135 (accessed on 20 December 2021).
- Trieu, K.; McMahon, E.; Santos, J.A.; Bauman, A.; Jolly, K.A.; Bolam, B.; Webster, J. Review of behaviour change interventions to reduce population salt intake. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 17. [Google Scholar] [CrossRef] [Green Version]
- Johnson, C.; Santos, J.A.; McKenzie, B.; Thout, S.R.; Trieu, K.; McLean, R.; Petersen, K.S.; Campbell, N.R.C.; Webster, J. The Science of Salt: A regularly updated systematic review of the implementation of salt reduction interventions (September 2016–February 2017). J. Clin. Hypertens. 2017, 19, 928–938. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomized studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Takada, T.; Imamoto, M.; Fukuma, S.; Yamamoto, Y.; Sasaki, S.; Uchida, M.; Miura, Y.; Shimizu, S.; Nihata, K.; Fukuhara, S. Effect of cooking classes for housewives on salt reduction in family members: A cluster randomized controlled trial. Public Health 2016, 140, 144–150. [Google Scholar] [CrossRef]
- Takada, T.; Imamoto, M.; Sasaki, S.; Azuma, T.; Miyashita, J.; Hayashi, M.; Fukuma, S.; Fukuhara, S. Effects of self-monitoring of daily salt intake estimated by a simple electrical device for salt reduction: A cluster randomized trial. Hypertens. Res. 2018, 41, 524–530. [Google Scholar] [CrossRef]
- Nakano, M.; Eguchi, K.; Sato, T.; Onoguchi, A.; Hoshide, S.; Kario, K. Effect of Intensive Salt-Restriction Education on Clinic, Home, and Ambulatory Blood Pressure Levels in Treated Hypertensive Patients During a 3-Month Education Period. J. Clin. Hypertens. 2016, 18, 385–392. [Google Scholar] [CrossRef] [Green Version]
- Morikawa, N.; Yamasue, K.; Tochikubo, O.; Mizushima, S. Effect of salt reduction intervention program using an electronic salt sensor and cellular phone on blood pressure among hypertensive workers. Clin. Exp. Hypertens. 2011, 33, 216–222. [Google Scholar] [CrossRef]
- Yasutake, K.; Sawano, K.; Yamaguchi, S.; Sakai, H.; Amadera, H.; Tsuchihashi, T. Self-monitoring urinary salt excretion in adults: A novel education program for restricting dietary salt intake. Exp. Ther. Med. 2011, 2, 615–618. [Google Scholar] [CrossRef] [Green Version]
- Rahimdel, T.; Morowatisharifabad, M.A.; Salehi-Abargouei, A.; Mirzaei, M.; Fallahzadeh, H. Evaluation of an education program based on the theory of planned behavior for salt intake in individuals at risk of hypertension. Health Educ. Res. 2019, 34, 268–278. [Google Scholar] [CrossRef]
- Layeghiasl, M.; Malekzadeh, J.; Shams, M.; Maleki, M. Using Social Marketing to Reduce Salt Intake in Iran. Front. Public Health 2020, 8, 207. [Google Scholar] [CrossRef]
- Jafari, M.; Mohammadi, M.; Ghazizadeh, H.; Nakhaee, N. Feasibility and Outcome of Reducing Salt in Bread: A Community Trial in Southern Iran. Glob. J. Health Sci. 2016, 8, 163–169. [Google Scholar] [CrossRef] [Green Version]
- He, F.J.; Wu, Y.; Feng, X.X.; Ma, J.; Ma, Y.; Wang, H.; Zhang, J.; Yuan, J.; Lin, C.P.; Nowson, C.; et al. School based education programme to reduce salt intake in children and their families (School-EduSalt): Cluster randomised controlled trial. BMJ 2015, 350, h770. [Google Scholar] [CrossRef] [Green Version]
- Li, N.; Yan, L.L.; Niu, W.; Yao, C.; Feng, X.; Zhang, J.; Shi, J.; Zhang, Y.; Zhang, R.; Hao, Z.; et al. The Effects of a Community-Based Sodium Reduction Program in Rural China-A Cluster-Randomized Trial. PLoS ONE 2016, 11, e0166620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokokawa, H.; Yuasa, M.; Nedsuwan, S.; Moolphate, S.; Fukuda, H.; Kitajima, T.; Minematsu, K.; Tanimura, S.; Marui, E. An impact of dietary intervention on blood pressures among diabetic and/or hypertensive patients with high cardiovascular disorders risk in northern Thailand by cluster randomized trial. J. Gen. Fam. Med. 2020, 22, 28–37. [Google Scholar] [CrossRef]
- Cashman, K.D.; Kenny, S.; Kerry, J.P.; Leenhardt, F.; Arendt, E.K. ‘Low-Salt’ Bread as an Important Component of a Pragmatic Reduced-Salt Diet for Lowering Blood Pressure in Adults with Elevated Blood Pressure. Nutrients 2019, 11, 1725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riis, N.L.; Bjoernsbo, K.S.; Lassen, A.D.; Trolle, E.; Frederiksen, A.K.S.; Andreasen, A.H.; Bysted, A.; Toft, U. Impact of a sodium-reduced bread intervention with and without dietary counseling on sodium intake-a cluster randomized controlled trial among Danish families. Eur. J. Clin. Nutr. 2020, 74, 1334–1344. [Google Scholar] [CrossRef]
- Pinjuh Markota, N.; Rumboldt, M.; Rumboldt, Z. Emphasized warning reduces salt intake: A randomized controlled trial. J. Am. Soc. Hypertens. 2015, 9, 214–220. [Google Scholar] [CrossRef]
- Musso, N.; Carloni, B.; Chiusano, M.C.; Giusti, M. Simple dietary advice reduces 24-h urinary sodium excretion, blood pressure, and drug consumption in hypertensive patients. J. Am. Soc. Hypertens. 2018, 12, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.A.; Cobb, L.K.; Miller, E.R.; Woodward, M.; Hottenstein, A.; Chang, A.R.; Mongraw-Chaffin, M.; White, K.; Charleston, J.; Tanaka, T.; et al. Effects of a behavioral intervention that emphasizes spices and herbs on adherence to recommended sodium intake: Results of the SPICE randomized clinical trial. Am. J. Clin. Nutr. 2015, 102, 671–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunbar, S.B.; Clark, P.C.; Stamp, K.D.; Reilly, C.M.; Gary, R.A.; Higgins, M.; Kaslow, N. Family partnership and education interventions to reduce dietary sodium by patients with heart failure differ by family functioning. Heart Lung 2016, 45, 311–318. [Google Scholar] [CrossRef] [Green Version]
- Ipjian, M.L.; Johnston, C.S. Smartphone technology facilitates dietary change in healthy adults. Nutrition 2017, 33, 343–347. [Google Scholar] [CrossRef]
- Barros, C.L.; Sousa, A.L.; Chinem, B.M.; Rodrigues, R.B.; Jardim, T.S.; Carneiro, S.B.; Souza, W.K.; Jardim, P.C. Impact of light salt substitution for regular salt on blood pressure of hypertensive patients. Arq. Bras. Cardiol. 2015, 104, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Ireland, D.M.; Clifton, P.M.; Keogh, J.B. Achieving the salt intake target of 6 g/day in the current food supply in free-living adults using two dietary education strategies. J. Am. Diet. Assoc. 2010, 110, 763–767. [Google Scholar] [CrossRef]
- Land, M.A.; Wu, J.H.; Selwyn, A.; Crino, M.; Woodward, M.; Chalmers, J.; Webster, J.; Nowson, C.; Jeffery, P.; Smith, W.; et al. Effects of a community-based salt reduction program in a regional Australian population. BMC Public Health 2016, 16, 388. [Google Scholar] [CrossRef] [Green Version]
- Nardini, C.; Osmani, V.; Cormio, P.G.; Frosini, A.; Turrini, M.; Lionis, C.; Neumuth, T.; Ballensiefen, W.; Borgonovi, E.; D’Errico, G. The evolution of personalized healthcare and the pivotal role of European regions in its implementation. Pers. Med. 2021, 18, 283–294. [Google Scholar] [CrossRef]
- Priorities for Personalized Medicine. Available online: http://oncotherapy.us/pdf/PM.Priorities.pdf (accessed on 1 September 2021).
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- He, F.J.; Campbell, N.R.; MacGregor, G.A. Reducing salt intake to prevent hypertension and cardiovascular disease. Rev. Panam. Salud Publica 2012, 32, 293–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neal, B.; Wu, Y.; Feng, X.; Zhang, R.; Zhang, Y.; Shi, J.; Zhang, J.; Tian, M.; Huang, L.; Li, Z.; et al. Effect of Salt Substitution on Cardiovascular Events and Death. N. Engl. J. Med. 2021, 385, 1067–1077. [Google Scholar] [CrossRef]
- Silow-Carroll, S.; Smith, B. Clinical management apps: Creating partnerships between providers and patients. Issue Brief (Commonw Fund) 2013, 30, 1–10. [Google Scholar]
- Maizes, V.; Rakel, D.; Niemiec, C. Integrative medicine and patient-centered care. Explore 2009, 5, 277–289. [Google Scholar] [CrossRef] [PubMed]
- Adler, A.J.; Taylor, F.; Martin, N.; Gottlieb, S.; Taylor, R.S.; Ebrahim, S. Reduced dietary salt for the prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2014, 2014, Cd009217. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behaviour. Organ. Behav. Hum. Decis. Processes 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Yasutake, K.; Umeki, Y.; Horita, N.; Morita, R.; Murata, Y.; Ohe, K.; Tsuchihashi, T.; Enjoji, M. A self-monitoring urinary salt excretion level measurement device for educating young women about salt reduction: A parallel randomized trial involving two groups. J. Clin. Hypertens. 2019, 21, 730–738. [Google Scholar] [CrossRef]
- Yasutake, K.; Miyoshi, E.; Misumi, Y.; Kajiyama, T.; Fukuda, T.; Ishii, T.; Moriguchi, R.; Murata, Y.; Ohe, K.; Enjoji, M.; et al. Self-monitoring of urinary salt excretion as a method of salt-reduction education: A parallel, randomized trial involving two groups. Public Health Nutr. 2018, 21, 2164–2173. [Google Scholar] [CrossRef]
- Iwahori, T.; Ueshima, H.; Ohgami, N.; Yamashita, H.; Miyagawa, N.; Kondo, K.; Torii, S.; Yoshita, K.; Shiga, T.; Ohkubo, T.; et al. Effectiveness of a Self-monitoring Device for Urinary Sodium-to-Potassium Ratio on Dietary Improvement in Free-Living Adults: A Randomized Controlled Trial. J. Epidemiol. 2018, 28, 41–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, K.S.; Torpy, D.J.; Chapman, I.M.; Guha, S.; Clifton, P.M.; Turner, K.; Keogh, J.B. Food label education does not reduce sodium intake in people with type 2 diabetes mellitus. A randomised controlled trial. Appetite 2013, 68, 147–151. [Google Scholar] [CrossRef]
- Dorsch, M.P.; Cornellier, M.L.; Poggi, A.D.; Bilgen, F.; Chen, P.; Wu, C.; An, L.C.; Hummel, S.L. Effects of a Novel Contextual Just-In-Time Mobile App Intervention (LowSalt4Life) on Sodium Intake in Adults With Hypertension: Pilot Randomized Controlled Trial. JMIR Mhealth Uhealth 2020, 8, e16696. [Google Scholar] [CrossRef]
- Lofthouse, C.; Te Morenga, L.; McLean, R. Sodium reduction in New Zealand requires major behaviour change. Appetite 2016, 105, 721–730. [Google Scholar] [CrossRef]
- Thatthong, N.; Sranacharoenpong, K.; Praditsorn, P.; Churak, P.; Ponprachanuvut, P.; Srisangwan, N.; Keeratichamroen, A. Innovative tool for health promotion for at-risk Thai people with hypertension. J. Public Health 2020, 28, 437–443. [Google Scholar] [CrossRef]
- Nakadate, M.; Ishihara, J.; Iwasaki, M.; Kitamura, K.; Kato, E.; Tanaka, J.; Nakamura, K.; Ishihara, T.; Shintani, A.; Takachi, R. Effect of monitoring salt concentration of home-prepared dishes and using low-sodium seasonings on sodium intake reduction. Eur. J. Clin. Nutr. 2018, 72, 1413–1420. [Google Scholar] [CrossRef]
- Beer-Borst, S.; Hayoz, S.; Eisenblätter, J.; Jent, S.; Siegenthaler, S.; Strazzullo, P.; Luta, X. RE-AIM evaluation of a one-year trial of a combined educational and environmental workplace intervention to lower salt intake in Switzerland. Prev. Med. Rep. 2019, 16, 100982. [Google Scholar] [CrossRef]
- Chen, J.; Tian, Y.; Liao, Y.; Yang, S.; Li, Z.; He, C.; Tu, D.; Sun, X. Salt-restriction-spoon improved the salt intake among residents in China. PLoS ONE 2013, 8, e78963. [Google Scholar] [CrossRef]
- Cornélio, M.E.; Godin, G.; Rodrigues, R.C.; de Freitas Agondi, R.; Alexandre, N.M.; Gallani, M.C. Effect of a behavioral intervention of the SALdável program to reduce salt intake among hypertensive women: A randomized controlled pilot study. Eur. J. Cardiovasc. Nurs. 2016, 15, e85–e94. [Google Scholar] [CrossRef] [PubMed]
- Holbrook, J.T.; Patterson, K.Y.; Bodner, J.E.; Douglas, L.W.; Veillon, C.; Kelsay, J.L.; Mertz, W.; Smith Jr, J.C. Sodium and potassium intake and balance in adults consuming self-selected diets. Am. J. Clin. Nutr. 1984, 40, 786–793. [Google Scholar] [CrossRef]
- Kawasaki, T.; Itoh, K.; Uezono, K.; Sasaki, H. A simple method for estimating 24 h urinary sodium and potassium excretion from second morning voiding urine specimen in adults. Clin. Exp. Pharmacol. Physiol. 1993, 20, 7–14. [Google Scholar] [CrossRef]
- Tanaka, T.; Okamura, T.; Miura, K.; Kadowaki, T.; Ueshima, H.; Nakagawa, H.; Hashimoto, T. A simple method to estimate populational 24-h urinary sodium and potassium excretion using a casual urine specimen. J. Hum. Hypertens. 2002, 16, 97–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamata, K.; Tochikubo, O. Estimation of 24-h urinary sodium excretion using lean body mass and overnight urine collected by a pipe-sampling method. J. Hypertens. 2002, 20, 2191–2197. [Google Scholar] [CrossRef]
- Yokokawa, H.; Yuasa, M.; Nedsuwan, S.; Moolphate, S.; Fukuda, H.; Kitajima, T.; Minematsu, K.; Tanimura, S.; Marui, E. Daily salt intake estimated by overnight urine collections indicates a high cardiovascular disease risk in Thailand. Asia Pac. J. Clin. Nutr. 2016, 25, 39–45. [Google Scholar] [CrossRef]
- Yamasue, K.; Tochikubo, O.; Kono, E.; Maeda, H. Self-monitoring of home blood pressure with estimation of daily salt intake using a new electrical device. J. Hum. Hypertens. 2006, 20, 593–598. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Study Author (Year), Country | Participants | Study Design | Enrolment Start and End Dates; Length of Participant Follow-Up | Intervention | Method of Assessment | Results | ||
|---|---|---|---|---|---|---|---|---|
| Reduction in Salt Intake (g/day) in the IG | Difference in Salt Intake (g/day) between IG and CG | Blood Pressure (mmHg) | ||||||
| Ireland [38] (2010), Australia | 43 Healthy free-living adults (33 women). Tick group, n = 22. Food Standards Australia New Zealand group, n = 21. | 8-week parallel design randomized | August 2008 and October 2008. | Participants received dietary education to choose foods identified by either Australia’s National Heart Foundation Tick symbol or by the Food Standards Australia and New Zealand’s low-salt guideline of 120 mg sodium/100 g food. | 24 h urinary Na excretion, 1 urine collection at 3 different times (baseline, week 4, week 8). | 0.9 in Tick group 2.0 in Food Standards group | NI | NA |
| Morikawa [22] (2011), Japan | 41 Hypertensive male workers employees of a rail-road company. IG, n = 22, (48 mean years). CG (n = 19, 47 mean years). | Quasi-randomization intervention control | 4-week follow-up. | Self-monitoring of daily salt excretion by an electronic salt sensor and sent personalized e-mail advice via cellular phone. | Overnight urine using the electronic salt sensor, only participants in IG (for 1 week at baseline and during the week 4). BP (baseline and week 4) | 0.7 | NA | SBP: −5.4 in IG DBP: −6.2 in IG |
| Barros [37] (2014), Brazil | 38 Hypertensive individuals (56 mean years, 65.7% women). IG, n = 19. CG, n = 16. | Single-blind randomized controlled trial | May to October 2012, 4-week intervention. | All patients were instructed to consume only the provided salt throughout this study (light salt for the intervention group and regular salt for the control group). In addition, they were instructed to reduce sodium-rich food consumption during the study period, being particularly warned about industrialized foods. | 24 h urinary Na excretion, 1 urine collection at 2 different times (baseline and at the end of the trial). BP (baseline and at the end of the trial). | 4.5 | −3.2 | SBP −12.47 (p = 0.034) in IG×CG. DBP −7.58 (p = 0.046) in IG×CG |
| Anderson [34] (2015), USA | 40 Individuals for whom the Dietary Guidelines for Americans recommends 1500 mg Na/day (61 mean years, 88% African American). IG, n = 20. CG, n = 20. | Randomized clinical trial | 2012 to 2014, 20-week intervention. | 2-phase study. In phase 1, all participants consumed a low-sodium diet for 4 weeks. Participants were provided all foods, snacks, and calorie-containing drinks. In phase 2, were randomly assigned to either a multifactorial behavioral intervention emphasizing spices and herbs to reduce sodium intake or a self-directed control group. | 24 h urinary Na excretion, 7 urine samples as follows: 2 samples at screening, 2 samples at week 4 (baseline), one sample at week 14, and 2 samples at week 24. | 2.3 | −2.4 | NA |
| He [27] (2015), China | 553 Adult family members of primary school children. CG, n = 275 (44 mean years). IG, n = 278; 44 mean years. | Cluster-randomized controlled trial | May to December 2013, 3.5-month intervention. | Children in the intervention group were educated on the harmful effects of salt and how to reduce salt intake within the schools’ usual health education lessons. Children then delivered the salt reduction message to their families. Parents were provided with educational materials in the form of a newsletter. | 24 h urinary Na excretion, 2 urine collections at 2 different times (at baseline and at the end of the trial). BP (at baseline and at the end of the trial). | 2.1 | −2.9 | SBP −2.3 (p < 0.05) in IG×CG. DBP −0.9 (p = 0.31) in IG×CG |
| Markota [32] (2015), Bosnia-Herzegovina | 150 Adults treated hypertensives. CG, n = 74 (59 mean years, 37 women). IG, n = 76 (59 mean years, 40 women). | Randomized clinical trial | September 2012 to July 2013 | Intervention group: received individual information leaflets about the untoward effects of excessive salt consumption and received warning stickers to be mounted on all salt containers. Control group: only information leaflets. | 24 h urinary Na excretion, 1 urine collection at 3 different times (baseline; 1 month and 2 months after the intervention). BP (baseline, 1 month and 2 months after the intervention). | 2.0 | NI | SBP: −5.3 in IG DBP: −2.9 in IG |
| Dunbar [35] (2016), USA | 117 Heart Failure patients and one family member–dyads (56 mean years, 37% women). Usual Care (UC), n = 37. Family Education (PFE), n = 41. Family Partnership Intervention (FPI), n = 37. | 3-Group randomized control trial | 4-Month behavior change. 4 to 8-month maintenance phase of behavior change. | UC group: received usual care from their providers and was provided with educational pamphlets that were created by the Heart Failure Society of America (HFSA). PFE group: received usual care, the HFSA pamphlets, and educational sessions. FPI group: received the same education and counseling as described in the UC and PFE groups plus 2-additional group sessions that focused on teaching the dyads how to give support, communication, empathy, and autonomy support for one another’s roles. | 24 h urinary Na excretion, 1 urine collection at 3 different times (baseline, 4 and 8 months after the intervention). | 3.1 in FPI | NI | NA |
| Li [28] (2016), China | 120 Townships from five provinces (n = 1903). Control villages, n = 60. Intervention villages, n = 60. | Two parallel cluster-randomized trial. | May 2011 to November 2012. 18-month intervention. | Intervention villages-Community-based health education and availability of reduced-sodium, added-potassium salt substitute at village shops. Control villages-Continued their usual practices | 24 h urinary Na excretion, 1 urine collection in a single moment (end of intervention). BP (end of intervention). | NI | −0.8 | SBP: −1.1 (p = 0.33) in IG×CG. DBP: −0.7 (p = 0.35) in IG×CG |
| Nakano [21] (2016), Japan | 95 Hypertensives IG, n = 51 (35 women, 58 mean years). CG, n = 44 (24 women, 60 mean years). | Prospective, randomized, and open-label study | September 2012 to May 2014, 3-month follow-up. | Intervention: intensive nutritional education aimed at salt restriction to 6 g/d by nutritionists. Control: conventional salt-restriction education. | 24 h urinary Na excretion, 1 urine collection at 2 different times (baseline and after intervention). Monitoring of clinic, home, and ambulatory BP values (baseline and after intervention). | 1.8 | NI | SBP: −4,5 in IG (Ambulatory 24 h SBP) |
| Takada [19] (2016), Japan | 35 Housewife’s and 31 family members. IG, n = 36 (63 mean years, 20 women). CG, n = 32 (65 mean years, 22 women). | Single-blinded, family-based Cluster randomized controlled trial | September 2015 to October 2015, 2-month intervention. | Intervention Group: 2x Cooking classes by registered dietitians, a general physician and a nephrologist, and it consisted of a practical course for evaluating the amount of salt in a meal and instruction on salt-reduced cooking. Control group: participants attended lectures about healthy living. The lecture contents did not include information related to salt reduction. | Spot urine, 1 urine collection at 2 different times (baseline and 2 months after intervention) BP measured only in the housewife’s subgroup (baseline and 2 months after intervention | 0.57 | −1.16 | SBP: −3.6 (p = 0.371) in IG×CG. DBP: −1.68 (p = 0.606) in IG×CG |
| Ipjian [36] (2017), USA | 30 Healthy adults (34 mean years; n = 23 women). MyFitnessPal app group, n = 15. Journal group, n = 15. | Randomized parallel trial | August to December 2014, 4-week intervention. | Participants were instructed to reduce their sodium intake to ≤2300 mg/d by using the MyFitnessPal app to receive feedback on sodium content of foods or by paper tallying of estimated sodium intake. | 2 first morning spot urine collection at 2 different times (baseline and after intervention). BP (baseline and after intervention) | 2.1 | NI | NI |
| Takada [20] (2018), Japan | 158 Participants from 105 families. IG, n = 79 (61 mean years, 68.4% women). CG, n = 79 (64 mean years, 64.6% women). | Single blinded, family-based, cluster randomized controlled trial | September 2016 to April 2017. 4-week intervention | Participants in both the intervention and control groups attended lectures about salt reduction by a general physician and a registered dietitian. In the intervention group, participants used the self- monitoring device to estimate their daily salt intake, and they recorded their results for 4 weeks. | Spot urine, 1 urine collection at 2 different times (baseline, week 4) BP (baseline, week 4). | 0.77 | −0.50 | SBP: −4.4 in IG×CG |
| Cashman [30] (2019), Republic of Ireland | 46 Adults with slightly to moderately elevated BP (47 mean years, 40 women) | Randomized crossover trial | January 2008 to July 2010. 5-week intervention. | Intervention: Combination of pragmatic dietary advice with the replacement of bread and a limited number of other foods with equivalent foods with a lower salt content. Control: normal diet, but were asked to consume an in-house bread, equivalent in composition to the low-salt version, but with its more typical salt content. | 24 h urinary Na excretion, 1 urine collection at 3 different times (baseline, week 5, week 10) BP (baseline, week 5, week 10) | 1.7 | NI | SBP: −3.3 in IG |
| Rahimdel [24] (2019), Iran | 140 Adults at risk of developing hypertension (43 mean years, 59.3% women). IG, n = 70. CG, n = 70. | Randomized clinical trial | February 2017 to December 2017 | Intervention: Education program based on the theory of planned behavior (TPB) for salt intake in individuals at risk of hypertension. Based on the results of the pretest, the educational content was prepared in the form of a booklet. Control: No educational program was conducted for the control group. | 24 h urinary Na excretion, 1 urine collection at 2 different times (baseline and 2 months after the intervention) BP (baseline and 2 months after the intervention). | 4.7 | NI | SBP: +1.1 (p = 0.2) in IG DBP: +1.26 (p = 0.22) in IG |
| Riis [31] (2020), Denmark | Family with at least one child. IG A, n = 41 (42 mean years). IG B, n = 63 (41 mean years). CG, n = 49 (41 mean years). | single-blinded, cluster randomized controlled trial with a parallel design | January 2018 to July 2018, 4-month intervention. | Intervention A: Families received sodium-reduced bread Intervention B: Families received sodium-reduced bread and dietary counseling Control: Families received regular sodium bread | 24 h urinary Na excretion, 3 urine collections at 2 different times (baseline and 4 months after the intervention). | 1 in IG A (p = 0.085) 1.8 in IG B (p < 0.001) | −0.5 (IG A x CG), p = 0.523 −1.0 (IG B x CG), p = 0.079 | NA |
| Yokokawa [29] (2020), Thailand | 753 Patients at high risk of CVD stratified by the Framingham general CVD risk scoring system (367 women). 8 clusters: n = 4 CG, n = 4 IG. | cluster randomized controlled trial | February 2012 to January 2013 | Intervention group: education program, visualization tools to inform the patients of their estimated 24-h salt intake and dietary salt content in daily food/ soup (analyzed by investigators) and special health education classes organized by the dietician. Control group: routine care services and a brief individual health education session, not focused on salt reduction. | Overnight urine collection, average of 3 successive days’ measurements at 3 different times (baseline, 6 and 12 months). BP (baseline, 6 and 12 months) | 0.86 at 6 months (p < 0.01) 0.22 at 12 months (p = 0.02) | −0.66 at 6 months (p = 0.03) −0.42 at 12 months (p = 0.16) | SBP At 6 months in IG: −12.34 IG×CG: −7.55 SBP |
| Study Author (Year), Country | Participants | Study Design | Enrolment Start and End Dates; Length of Participant Follow-Up | Intervention | Method of Assessment | Results | ||
|---|---|---|---|---|---|---|---|---|
| Reduction in Salt Intake (g/day) in the IG | Difference in Salt Intake (g/day) between IG and CG | Blood Pressure (mmHg) | ||||||
| Yasutake [23] (2011), Japan | 30 Healthy adult volunteers (15 women, 43 mean years). | Quasi-experimental | March to April 2009, 4-week intervention. | Measurement of daily salt excretion at home for 4 weeks using the self-monitoring device for educating healthy adults regarding their levels of salt intake and the dangers of excessive salt use. | Overnight urine sample, 4 weeks using the self-monitoring device. BP (baseline and 8 weeks later). | 0.4 | NA | SBP: −3.4 |
| Jafari [26] (2016), Iran | Two cities. Intervention, n = 346 (61% women, 49 mean years). Control, n = 310 (50.3% women, 48 mean years). | Community intervention trial | March to July 2014, 4-week intervention. | Installation of educational banners and door-to-door distribution of pamphlets in the intervention city and in the control city. In the intervention city, they reduced the bread salt by 40% | Urine sample collection from 8:00 to 9:00 am after discarding the first urine, 1 urine collection at 2 different times (baseline and after 12 weeks). BP (baseline and after 12 weeks). | 0.9 | NA | SBP: −7.4 in IG |
| Land [39] (2016), Australia | 419 individuals at baseline and 572 at follow-up (56 mean years, 58% women). | Interventional (Clinical Trial)/Community-based intervention | March 2011 to May 2014, 18-month intervention. | A multi-faceted, community-based salt reduction program using the Communication for Behavioral Impact (COMBI) framework. | 24 h urinary Na excretion, 1 urine collection at 2 different times (baseline and at the end of the intervention) | 0.8 | NI | NA |
| Musso [33] (2018), Italy | 291 Patients on antihypertensive treatment (166 women, 63 mean years). Dietary protocol n = 240, control n = 51. | Intervention control Trial | 2-month intervention. | Low-sodium diet prescribed by the dietitian. | 24 h urinary Na excretion, 1 urine collection at 2 different times (baseline and after intervention). BP (baseline and after intervention). | 1.14 | NI | SBP: −7.66 in IG DBP: −4.69 in IG |
| Layeghiasl [25] (2020), Iran | 166 participants (50% women, 36 mean years). | Quasi-experimental pretest-posttest with control group design | 2-month intervention. | Intervention: Marketing mix components were determined for designing an intervention. An educational package focused on reducing salt intake and using alternatives was developed. Control: received routine interventions in healthcare centers. | Urine samples collected daily in the morning, 1 urine collection at 2 different times (baseline and at the end of the intervention). | 3.01 | NI | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva-Santos, T.; Moreira, P.; Rodrigues, M.; Padrão, P.; Pinho, O.; Norton, P.; Ndrio, A.; Gonçalves, C. Interventions That Successfully Reduced Adults Salt Intake—A Systematic Review. Nutrients 2022, 14, 6. https://doi.org/10.3390/nu14010006
Silva-Santos T, Moreira P, Rodrigues M, Padrão P, Pinho O, Norton P, Ndrio A, Gonçalves C. Interventions That Successfully Reduced Adults Salt Intake—A Systematic Review. Nutrients. 2022; 14(1):6. https://doi.org/10.3390/nu14010006
Chicago/Turabian StyleSilva-Santos, Tânia, Pedro Moreira, Micaela Rodrigues, Patrícia Padrão, Olívia Pinho, Pedro Norton, Altin Ndrio, and Carla Gonçalves. 2022. "Interventions That Successfully Reduced Adults Salt Intake—A Systematic Review" Nutrients 14, no. 1: 6. https://doi.org/10.3390/nu14010006
APA StyleSilva-Santos, T., Moreira, P., Rodrigues, M., Padrão, P., Pinho, O., Norton, P., Ndrio, A., & Gonçalves, C. (2022). Interventions That Successfully Reduced Adults Salt Intake—A Systematic Review. Nutrients, 14(1), 6. https://doi.org/10.3390/nu14010006