
Effectiveness and Usability of Digital Tools to Support Dietary Self-Management of Gestational Diabetes Mellitus: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Search Strategy
2.3. Inclusion Criteria
Pregnant Women with a Diagnosis or History of GDM Participated
2.4. Exclusion Criteria
2.5. Data Extraction
2.6. Quality Assessment
3. Results
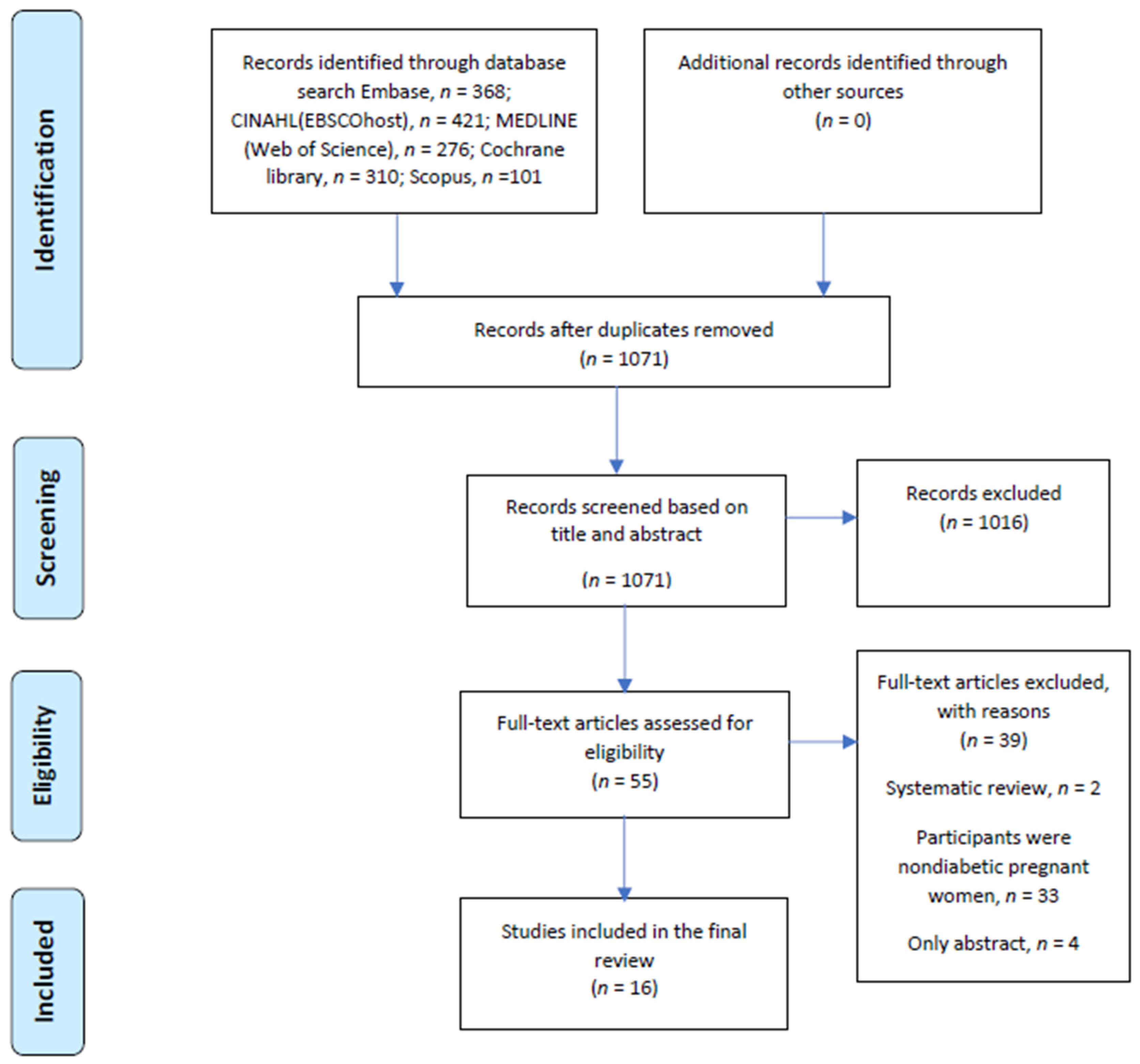
3.1. Study Selection
3.2. Study Quality Assessment
3.3. Study Characteristics
3.4. Findings
3.4.1. Effectiveness of Digital Tools to Support Dietary Self-Management of GDM
3.4.2. Acceptability of Digital Tools to Support Dietary Self-Management of Gestational Diabetes Mellitus
3.4.3. Feasibility of Digital Tools to Support Dietary Self-Management of Gestational Diabetes Mellitus
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chiefari, E.; Arcidiacono, B.; Foti, D.; Brunetti, A. Gestational diabetes mellitus: An updated overview. J. Endocrinol. Investig. 2017, 40, 899–909. [Google Scholar] [CrossRef] [PubMed]
- Farrar, D.; Duley, L.; Lawlor, A.D. Different strategies for diagnosing gestational diabetes to improve maternal and infant health. Cochrane Database Syst. Rev. 2011, 8, CD007122. [Google Scholar] [CrossRef] [Green Version]
- Parrettini, S.; Caroli, A.; Torlone, E. Nutrition and Metabolic Adaptations in Physiological and Complicated Pregnancy: Focus on Obesity and Gestational Diabetes. Front. Endocrinol. 2020, 11, 611929. [Google Scholar] [CrossRef] [PubMed]
- Muche, A.A.; Olayemi, O.O.; Gete, Y.K. Prevalence of gestational diabetes mellitus and associated factors among women attending antenatal care at Gondar town public health facilities, Northwest Ethiopia. BMC Pregnancy Childbirth 2019, 19, 334. [Google Scholar] [CrossRef] [PubMed]
- Ogurtsova, K.; Da Rocha Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.E.; Makaroff, L.E. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adu, M.D.; Malabu, U.H.; Malau-Aduli, A.E.O.; Malau-Aduli, B. Users’ preferences and design recommendations to promote engagements with mobile apps for diabetes self-management: Multi-national perspectives. PLoS ONE 2018, 13, e0208942. [Google Scholar] [CrossRef] [Green Version]
- Dirar, A.M.; Doupis, J. Gestational diabetes from A to Z. World J. Diabetes 2017, 8, 489. [Google Scholar] [CrossRef]
- Kretowicz, H.; Hundley, V.; Tsofliou, F. Exploring the Perceived Barriers to Following a Mediterranean Style Diet in Childbearing Age: A Qualitative Study. Nutrients 2018, 10, 1694. [Google Scholar] [CrossRef] [Green Version]
- Al Wattar, B.H.; Dodds, J.; Placzek, A.; Beresford, L.; Spyreli, E.; Moore, A.; Gonzalez Carreras, F.J.; Austin, F.; Murugesu, N.; Roseboom, T.J.; et al. Mediterranean-style diet in pregnant women with metabolic risk factors (ESTEEM): A pragmatic multicentre randomised trial. PLoS Med. 2019, 16, e1002857. [Google Scholar] [CrossRef]
- Horan, M.K.; Donnelly, J.; McGowan, C.A.; Gibney, E.R.; McAuliffe, F.M. The association between maternal nutrition and lifestyle during pregnancy and 2-year-old offspring adiposity: Analysis from the ROLO study. J. Public Health 2016, 24, 427–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kvedar, J.C. Evidence for the effectiveness of digital health. NPJ Digit. Med. 2020, 3, 34–41. [Google Scholar] [CrossRef]
- Wu, I.X.Y.; Kee, J.C.Y.; Threapleton, D.E.; Ma, R.C.W.; Lam, V.C.K.; Lee, E.K.P.; Wong, S.Y.S.; Chung, V.C.H. Effectiveness of smartphone technologies on glycaemic control in patients with type 2 diabetes: Systematic review with meta-analysis of 17 trials. Obes. Rev. 2018, 19, 825–838. [Google Scholar] [CrossRef] [PubMed]
- Jeffrey, B.; Bagala, M.; Creighton, A.; Leavey, T.; Nicholls, S.; Wood, C.; Longman, J.; Barker, J.; Pit, S. Mobile phone applications and their use in the self-management of Type 2 Diabetes Mellitus: A qualitative study among app users and non-app users. Diabetol. Metab. Syndr. 2019, 11, 84. [Google Scholar] [CrossRef]
- Overdijkink, S.B.; Velu, A.V.; Rosman, A.N.; Van Beukering, M.D.; Kok, M.; Steegers-Theunissen, R.P. The Usability and Effectiveness of Mobile Health Technology–Based Lifestyle and Medical Intervention Apps Supporting Health Care during Pregnancy: Systematic Review. JMIR mHealth uHealth 2018, 6, e109. [Google Scholar] [CrossRef] [Green Version]
- Bland, C.; Dalrymple, K.V.; White, S.L.; Moore, A.; Poston, L.; Flynn, A.C. Smartphone applications available to pregnant women in the United Kingdom: An assessment of nutritional information. Matern. Child Nutr. 2020, 16, e12918. [Google Scholar] [CrossRef] [Green Version]
- Wang, N.; Deng, Z.; Wen, L.M.; Ding, Y.; He, G. Understanding the Use of Smartphone Apps for Health Information Among Pregnant Chinese Women: Mixed Methods Study. JMIR mHealth uHealth 2019, 7, e12631. [Google Scholar] [CrossRef] [PubMed]
- Jo, S.; Park, H.-A. Development and Evaluation of a Smartphone Application for Managing Gestational Diabetes Mellitus. Health Inform. Res. 2016, 22, 11–21. [Google Scholar] [CrossRef] [Green Version]
- Garnweidner-Holme, L.M.; Borgen, I.; Garitano, I.; Noll, J.; Lukasse, M. Designing and Developing a Mobile Smartphone Application for Women with Gestational Diabetes Mellitus Followed-Up at Diabetes Outpatient Clinics in Norway. Health 2015, 3, 310–323. [Google Scholar] [CrossRef] [Green Version]
- Tassone, C.; Keshavjee, K.; Paglialonga, A.; Moreira, N.; Pinto, J.; Quintana, Y. Evaluation of mobile apps for treatment of patients at risk of developing gestational diabetes. Health Inform. J. 2020, 26, 1983–1994. [Google Scholar] [CrossRef] [Green Version]
- Anderson, K.; Burford, O.; Emmerton, L. Mobile Health Apps to Facilitate Self-Care: A Qualitative Study of User Experiences. PLoS ONE 2016, 11, e0156164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giles, E.L.; Robalino, S.; Sniehotta, F.F.; Adams, J.; McColl, E. Acceptability of financial incentives for encouraging uptake of healthy behaviours: A critical review using systematic methods. Prev. Med. 2015, 73, 145–158. [Google Scholar] [CrossRef] [Green Version]
- Booth, A.M.; Wright, K.E.; Outhwaite, H. Centre for Reviews and Dissemination databases: Value, content, and developments. Int. J. Technol. Assess. Heal. Care 2010, 26, 470–472. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tielemans, M.J.; Garcia, A.H.; Peralta-Santos, A.; Bramer, W.; Luksa, N.; Luvizotto, M.J.; Moreira, E.; Topi, G.; Al De Jonge, E.; Visser, T.L.; et al. Macronutrient composition and gestational weight gain: A systematic review. Am. J. Clin. Nutr. 2016, 103, 83–99. [Google Scholar] [CrossRef] [Green Version]
- Thomas, B.; Ciliska, D.; Dobbins, M.; Micucci, S. A Process for Systematically Reviewing the Literature: Providing the Research Evidence for Public Health Nursing Interventions. Worldviews Evid.-Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Skar, J.B.; Garnweidner-Holme, L.M.; Lukasse, M.; Terragni, L. Women’s experiences with using a smartphone app (the Pregnant+ app) to manage gestational diabetes mellitus in a randomised controlled trial. Midwifery 2018, 58, 102–108. [Google Scholar] [CrossRef]
- Sayakhot, P.; Carolan-Olah, M.; Steele, C. Use of a web-based educational intervention to improve knowledge of healthy diet and lifestyle in women with Gestational Diabetes Mellitus compared to standard clinic-based education. BMC Pregnancy Childbirth 2016, 16, 208. [Google Scholar] [CrossRef] [Green Version]
- Roozbahani, R.K.; Geranmayeh, M.; Hantoushzadeh, S.; Mehran, A. Effects of telephone follow-up on blood glucose levels and postpartum screening in mothers with Gestational Diabetes Mellitus. Med. J. Islam. Repub. Iran 2015, 29, 249. [Google Scholar]
- Rigla, M.; Martínez-Sarriegui, I.; García-Sáez, G.; Pons, B.; Hernando, M.E. Gestational Diabetes Management Using Smart Mobile Telemedicine. J. Diabetes Sci. Technol. 2017, 12, 260–264. [Google Scholar] [CrossRef]
- Miremberg, H.; Ben-Ari, T.; Betzer, T.; Raphaeli, H.; Gasnier, R.; Barda, G.; Bar, J.; Weiner, E. The impact of a daily smartphone-based feedback system among women with gestational diabetes on compliance, glycemic control, satisfaction, and pregnancy outcome: A randomized controlled trial. Am. J. Obstet. Gynecol. 2018, 218, 453.e1–453.e7. [Google Scholar] [CrossRef]
- Kennelly, M.A.; Ainscough, K.; Lindsay, K.L.; O’Sullivan, E.; Gibney, E.R.; McCarthy, M.; Segurado, R.; DeVito, G.; Maguire, O.; Smith, T.; et al. Pregnancy exercise and nutrition with smartphone application support: A randomized controlled trial. Obstet. Gynecol. 2018, 131, 818–826. [Google Scholar] [CrossRef] [PubMed]
- Hirst, J.E.; MacKillop, L.; Loerup, L.; Kevat, D.A.; Bartlett, K.; Gibson, O.; Kenworthy, Y.; Levy, J.C.; Tarassenko, L.; Farmer, A. Acceptability and User Satisfaction of a Smartphone-Based, Interactive Blood Glucose Management System in Women with Gestational Diabetes Mellitus. J. Diabetes Sci. Technol. 2014, 9, 111–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hewage, S.; Audimulam, J.; Sullivan, E.; Chi, C.; Yew, T.W.; Yoong, J. Barriers to Gestational Diabetes Management and Preferred Interventions for Women with Gestational Diabetes in Singapore: Mixed Methods Study. JMIR Form. Res. 2020, 4, e14486. [Google Scholar] [CrossRef]
- Guo, H.; Zhang, Y.; Li, P.; Zhou, P.; Chen, L.-M.; Li, S.-Y. Evaluating the effects of mobile health intervention on weight management, glycemic control and pregnancy outcomes in patients with gestational diabetes mellitus. J. Endocrinol. Investig. 2018, 42, 709–714. [Google Scholar] [CrossRef]
- Given, J.E.; Bunting, B.P.; O’Kane, M.J.; Dunne, F.; Coates, V.E. Tele-Mum: A Feasibility Study for a Randomized Controlled Trial Exploring the Potential for Telemedicine in the Diabetes Care of Those with Gestational Diabetes. Diabetes Technol. Ther. 2015, 17, 880–888. [Google Scholar] [CrossRef]
- Gianfrancesco, C.; Darwin, Z.; McGowan, L.; Smith, D.M.; Haddrill, R.; Carter, M.; Scott, E.M.; Alwan, N.A.; Morris, M.A.; Albar, S.A.; et al. Exploring the Feasibility of Use of An Online Dietary Assessment Tool (myfood24) in Women with Gestational Diabetes. Nutrients 2018, 10, 1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalfrà, M.G.; Nicolucci, A.; Lapolla, A. The effect of telemedicine on outcome and quality of life in pregnant women with diabetes. J. Telemed. Telecare 2009, 15, 238–242. [Google Scholar] [CrossRef]
- Carral, F.; Ayala, M.D.C.; Fernández, J.J.; González, C.; Piñero, A.; Garcia, G.; Cañavate, C.; Jiménez, A.I.; García, C. Web-Based Telemedicine System Is Useful for Monitoring Glucose Control in Pregnant Women with Diabetes. Diabetes Technol. Ther. 2015, 17, 349–354. [Google Scholar] [CrossRef]
- Carolan-Olah, M.; Sayakhot, P. A randomized controlled trial of a web-based education intervention for women with gestational diabetes mellitus. Midwifery 2019, 68, 39–47. [Google Scholar] [CrossRef]
- Caballero-Ruiz, E.; García-Sáez, G.; Rigla, M.; Villaplana, M.; Pons, B.; Hernando, M.E. A web-based clinical decision support system for gestational diabetes: Automatic diet prescription and detection of insulin needs. Int. J. Med. Inform. 2017, 102, 35–49. [Google Scholar] [CrossRef] [Green Version]
- Borgen, I.; Garnweidner-Holme, L.M.; Jacobsen, A.F.; Bjerkan, K.; Fayyad, S.; Joranger, P.; Lilleengen, A.M.; Mosdøl, A.; Noll, J.; Småstuen, M.C.; et al. Smartphone application for women with gestational diabetes mellitus: A study protocol for a multicentre randomised controlled trial. BMJ Open 2017, 7, e013117. [Google Scholar] [CrossRef] [PubMed]
- Krebs, P.; Duncan, D.T. Health app use among US mobile phone owners: A national survey. JMIR mHealth uHealth 2015, 3, e4924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wani, R.T. Lifestyle medicine and use of technology in current healthcare. BMJ Innov. 2019, 5, 135. [Google Scholar] [CrossRef]
- Kuwabara, A.; Su, S.; Krauss, J. Utilizing Digital Health Technologies for Patient Education in Lifestyle Medicine. Am. J. Lifestyle Med. 2020, 14, 137–142. [Google Scholar] [CrossRef]
- Dunleavy, G.; Nikolaou, C.K.; Nifakos, S.; Atun, R.; Law, G.C.Y.; Car, L.T. Mobile Digital Education for Health Professions: Systematic Review and Meta-Analysis by the Digital Health Education Collaboration. J. Med. Internet Res. 2019, 21, e12937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, S.; Tan, A.; Madden, S.; Hill, B. Health professionals’ and postpartum women’s perspectives on digital health interventions for lifestyle management in the postpartum period: A systematic review of qualitative studies. Front. Endocrinol. 2019, 10, 767. [Google Scholar] [CrossRef] [Green Version]
- Ossebaard, H.C.; Van Gemert-Pijnen, L. eHealth and quality in health care: Implementation time. Int. J. Qual. Heal. Care 2016, 28, 415–419. [Google Scholar] [CrossRef] [Green Version]
- Immanuel, J.; Simmons, D. Apps and the Woman with Gestational Diabetes Mellitus. Diabetes Care 2021, 44, 313–315. [Google Scholar] [CrossRef]
- Yew, T.W.; Chi, C.; Chan, S.-Y.; van Dam, R.M.; Whitton, C.; Lim, C.S.; Foong, P.S.; Fransisca, W.; Teoh, C.L.; Chen, J.; et al. A Randomized Controlled Trial to Evaluate the Effects of a Smartphone Application–Based Lifestyle Coaching Program on Gestational Weight Gain, Glycemic Control, and Maternal and Neonatal Outcomes in Women with Gestational Diabetes Mellitus: The SMART-GDM Study. Diabetes Care 2020, 44, 456–463. [Google Scholar] [CrossRef]
- Rasekaba, T.M.; Furler, J.; Young, D.; Liew, D.; Gray, K.; Blackberry, I.; Lim, W.K. Using technology to support care in gestational diabetes mellitus: Quantitative outcomes of an exploratory randomised control trial of adjunct telemedicine for gestational diabetes mellitus (TeleGDM). Diabetes Res. Clin. Pr. 2018, 142, 276–285. [Google Scholar] [CrossRef]
- Badawy, S.M.; Kuhns, L.M. Texting and Mobile Phone App Interventions for Improving Adherence to Preventive Behavior in Adolescents: A Systematic Review. JMIR mHealth uHealth 2017, 5, e50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Opie, R.S.; Neff, M.; Tierney, A.C. A behavioural nutrition intervention for obese pregnant women: Effects on diet quality, weight gain and the incidence of gestational diabetes. Aust. N. Z. J. Obstet. Gynaecol. 2016, 56, 364–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawkins, M.; Hosker, M.; Marcus, B.H.; Rosal, M.C.; Braun, B.; Stanek, E.J.; Markenson, G.; Chasan-Taber, L. A pregnancy lifestyle intervention to prevent gestational diabetes risk factors in overweight Hispanic women: A feasibility randomized controlled trial. Diabet. Med. 2014, 32, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Kallan, M.J.; Allison, K.C.; Sammel, M.D.; Wisch, S.; Elovitz, M.; Parry, S.; Durnwald, C.P. A Randomized Clinical Trial of an Intensive Behavior Education Program in Gestational Diabetes Mellitus Women Designed to Improve Glucose Levels on the 2-Hour Oral Glucose Tolerance Test. Am. J. Perinatol. 2016, 33, 1145–1151. [Google Scholar] [CrossRef] [PubMed]
- Vickery, M.; Van Teijlingen, E.; Hundley, V.; Smith, G.B.; Way, S.; Westwood, G. Midwives’ views towards women using mHealth and eHealth to self-monitor their pregnancy: A systematic review of the literature. Eur. J. Midwifery 2020, 4, 36. [Google Scholar] [CrossRef]
- Garabedian, L.F.; Ross-Degnan, D.; Wharam, J.F. Mobile Phone and Smartphone Technologies for Diabetes Care and Self-Management. Curr. Diabetes Rep. 2015, 15, 109. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2019. [Google Scholar]


{kind=link}
| Author | Design | Size | Exposure | Outcome | Adjustment | Total | Quality |
|---|---|---|---|---|---|---|---|
| Borgen et al. [41] | 2 | 2 | 1 | 2 | 1 | 8 | High |
| Guo et al. [34] | 2 | 2 | 0 | 2 | 0 | 6 | High |
| Given et al. [35] | 2 | 1 | 0 | 2 | 1 | 6 | High |
| Caballero-Ruiz et al. [40] | 2 | 1 | 0 | 2 | 1 | 7 | High |
| Dalfrà et al. [37] | 2 | 2 | 0 | 2 | 0 | 6 | High |
| Miremberg et al. [30] | 2 | 2 | 0 | 2 | 0 | 6 | High |
| Carolan-Olah and Sayakhot [39] | 2 | 2 | 0 | 1 | 0 | 5 | Moderate |
| Rigla et al. [29] | 2 | 2 | 0 | 2 | 0 | 6 | High |
| Kennelly et al. [31] | 2 | 2 | 0 | 2 | 0 | 6 | High |
| Carral et al. [38] | 2 | 2 | 0 | 2 | 0 | 6 | High |
| Sayakhot et al. [27] | 2 | 2 | 0 | 2 | 0 | 6 | High |
| Roozbahani et al. [28] | 2 | 1 | 0 | 2 | 0 | 5 | Moderate |
| Author | Study Design | Score | ||
|---|---|---|---|---|
| Qualitative | Quantitative | MM | ||
| Hewage et al. [33] | ** | ** | ** | 50% |
| Gianfrancesco et al. [36] | ** | ** | ** | 50% |
| Hirst et al. [32] | ** | 50% | ||
| Skar et al. [26] | ** | 50% | ||
| Author (Country) | Aim of the Study | Participants, Setting | Study Intervention | Key Findings |
|---|---|---|---|---|
| Borgen et al. [41] (Norway) | To assess the effectiveness of a “pregnancy+ “app on Glu levels | 238 women, 5 diabetes clinics | Intervention (N = 115): pregnancy+ app and usual care Control (N = 123): usual care | NS difference in Glu levels [6.7 mmol/L (95% CI 6.2 to 7.1) vs. 6.0 mmol/L (95% CI 5.6 to 6.3)] intervention vs. control |
| Caballero-Ruiz et al. [40] (Spain) | To evaluate the effectiveness of a web-based support system (Sinedie) on diabetes clinic visits | 90 pregnant women with GDM, diabetes clinic | Intervention (N = 60): Web-based support system and standard care Control (N = 30): Standard care | Diabetes clinic visits reduced by 88.6% |
| Carral et al. [38] (Spain) | To assess the effects of a web-based telemedicine system on diabetes clinic visits, monitoring Glu control, maternal, and neonatal outcomes | 104 pregnant women, diabetes clinic | (GDM = 77, T1DM = 16, T2DM = 11). Intervention (N = 40): Telemedicine and standard care Control (N = 64): Standard care | Diabetes clinic visits reduced (3.2 ± 2.3 vs. 5.9 ± 2.3 visits; p < 0.001) intervention vs. Control NS difference in maternal outcomes: CS prevalence (30% vs. 40%; p = 0.164), MWG (8.4 kg ± 6.5 kg vs. 9.0 kg ± 6.6 kg; p = 0.644) intervention vs. control NS difference in neonatal outcomes: LGA prevalence hypoglycaemia (2.5% vs. 3.1%) intervention vs. control |
| Carolan-Olah and Sayakhot [39] (Australia) | To investigate the effects of an online educational programme on maternal BMI, blood pressure, glycaemic index, and infant birthweight | 110 women with GDM, diabetes clinic | Intervention (N = 52): Web-based education and standard care Control group (N = 58): Standard car | 44.2% women in intervention group maintained normal BMI (18.5–24.9 kg/m2 post intervention (vs 31%, p < 0.001) intervention vs. control Maternal BP * (107/64 mm Hg vs. 109/66 mm Hg), ** (108/68 mm Hg vs. 112/68 mm Hg)] intervention vs. control, NS difference Maternal Glu [(8.8 mmol/L * and 7.3 mmol/L **) vs. (4.9 mmol/L * and 4.7 mmol/L **)] intervention vs. control NBW 2.5 kg−4 kg, NS (92.3% vs. 94.8%) intervention vs. control |
| Dalfrà et al. [37] (Italy) | To assess the effect of a telemedicine system on maternal and foetal outcome in women with GDM | 276 pregnant women attending a diabetes clinic (GDM = 240, T1DM = 36) | Pregnant women with GDM -Intervention (N = 88) (Standard care and Telemedicine) -Control (N = 115): Standard care Pregnant women with TIDM -Intervention (N = 17): Telemedicine and standard care -Control (N = 15): Standard care | NS difference in CS and FM (p = 0.02) |
| Guo et al. [34] (China) | To explore the effects of mobile health (mHealth) intervention on pregnancy weight management, blood Glu control, and pregnancy outcomes | 124 women with GDM, diabetes clinic | Intervention (N = 64): Mobile medical management and standard care Control (N = 60): standard care | Significant effect on blood Glu control (4.7 ± 0.2 vs. 5.3 ± 0.3 p < 0.001) and MWG, (3.2 ± 0.8 vs. 4.8 ± 0.7, p < 0.001) Intervention vs. control NS on pregnancy outcomes: CS (33.3% vs. 25.0%, p = 0.325), FM (10% vs. 65.3%, p = 0.295) intervention vs. control |
| Kennelly et al. [31] (Ireland) | To investigate the effect of a smartphone-supported behavioural intervention on the incidence of GDM in overweight and obese women | 565 obese women with GDM, diabetes clinic | Intervention (N = 278): Smartphone-supported intervention and standard care Control (N = 287l): standard care | NS difference in incidence of GDM (15.4% vs. 14.1%, p = 0.71) intervention vs. control |
| Roozbahani et al. [28] (Iran) | To investigate the effects of telephone follow-up on blood glucose level during pregnancy and postpartum screening in women with GDM | 80 women with GDM, diabetes clinic | Intervention (N = 40): 10 weeks telephone follow-up Control (N = 40): 3 weeks telephone follow-up | NS in Glu level at 28 weeks of pregnancy (122.5 ± 19.7 mg/dL vs. 113.2 ± 15.8 mg/dL, p = 0.06) intervention vs. control |
| Miremberg et al. [30] (Israel) | To explore the impact of a smartphone-supported intervention, on patient compliance, glycaemic control, pregnancy outcome, and patient satisfaction | 120 newly diagnosed women with GDM, diabetic clinic | Intervention (N = 60): Smartphone-supported intervention and standard care Control (N = 60): Standard care | NS difference in LC (84 ± 0.16% vs. 66 ± 0.28%, p < 0.001) and Mean Glu (105.1 ± 8.6 mg/dL vs. 112.6 ± 7.4 mg/dL, p < 0.001) intervention vs. control, |
| Author (Country) | Stated Aim of the Study | Participants, Setting | Study Type-Acceptability Assessment | Key Findings |
|---|---|---|---|---|
| Given et al. [35] (UK) | To investigate acceptability of using telemedicine in diabetes care of women with GDM | 50 pregnant women, diabetes clinic | RCT-user satisfaction, recommendation to others Intervention (N = 24): Telemedicine and standard care Control (N = 26): Standard care | 89% of the participants satisfied and intend to recommend Telemedicine to other women with GDM |
| Hirst et al. [32] (UK) | To explore women ‘satisfaction with GDM-health system and their attitudes towards their diabetes care | 52 pregnant women with GDM, diabetes clinic | Quantitative-user satisfaction, appreciation, recommendation to others | 92% of the participants satisfied about using GDM-health system towards diabetes care |
| Rigla et al. [29] (Spain) | To explore the acceptance of a mobile decision support system for GDM | 20 women with GDM | RCT-user satisfaction Intervention (N = 20): Mobile technology and standard care Control (N = 0) | 100% of the participants satisfied to use mobile decision support system for GDM |
| Author (Country) | Stated Aim of the Study | Participants, Setting | Study Type | Key Findings |
|---|---|---|---|---|
| Gianfrancesco et al. [36] (UK) | To explore the feasibility of an online ‘myfood24’ dietary assessment tool in women with GDM | 199 women with GDM, diabetes clinic | Mixed method Quantitative (N = 216): Questionnaire- actual use, intention to use Qualitative (N = 15): Semi-structured interview-perceived appropriateness | ‘myfood24′ is feasible (mean 70.9, 95% CI 67.1, 74.6) |
| Hewage et al. [33] (Singapore) | To investigate perception of patient and health care providers on barriers and preferred intervention to manage GDM. | 216 pregnant women with GDM, diabetes clinic | Mixed method Quantitative (N = 216): Questionnaire-intention to use, actual use Qualitative (N = 15): Semi-structured interview-perceived appropriateness | Web-based support perceived to be feasible in 80.9% of the participants |
| Sayakhot et al. [27] (Australia) | To explore the feasibility of using a web-based intervention to support on healthy diet and other lifestyle management in women with GDM | 116 pregnant women with GDM, diabetes clinic | RCT-Actual use, perceived appropriateness Intervention (N = 56): Web-based intervention and standard care Control (N = 60): Standard care | Feasible to improve GDM knowledge about GDM (48.2% vs. 46.7%) and high GI carbohydrate (62.5% vs.58.3%) |
| Skar et al. 2018 [26] (Norway) | To explore the experiences of women with GDM while using pregnancy+ app for health and nutrition information to control blood Glu | 17 pregnant women with GDM, 5 diabetic clinics | Qualitative (Semi-structured interview)-perceived appropriateness | The pregnancy+ was perceived to be appropriate in providing easily accessible dietary advice on blood Glu, health, and nutrition in 88.3% of the participants. DA and Glu values in the app not always in agreement with the recommendation from midwives. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adesina, N.; Dogan, H.; Green, S.; Tsofliou, F. Effectiveness and Usability of Digital Tools to Support Dietary Self-Management of Gestational Diabetes Mellitus: A Systematic Review. Nutrients 2022, 14, 10. https://doi.org/10.3390/nu14010010
Adesina N, Dogan H, Green S, Tsofliou F. Effectiveness and Usability of Digital Tools to Support Dietary Self-Management of Gestational Diabetes Mellitus: A Systematic Review. Nutrients. 2022; 14(1):10. https://doi.org/10.3390/nu14010010
Chicago/Turabian StyleAdesina, Nurudeen, Huseyin Dogan, Sue Green, and Fotini Tsofliou. 2022. "Effectiveness and Usability of Digital Tools to Support Dietary Self-Management of Gestational Diabetes Mellitus: A Systematic Review" Nutrients 14, no. 1: 10. https://doi.org/10.3390/nu14010010
APA StyleAdesina, N., Dogan, H., Green, S., & Tsofliou, F. (2022). Effectiveness and Usability of Digital Tools to Support Dietary Self-Management of Gestational Diabetes Mellitus: A Systematic Review. Nutrients, 14(1), 10. https://doi.org/10.3390/nu14010010