
The Role of Vitamin D Supplementation in Children with Autism Spectrum Disorder: A Narrative Review



Abstract
:1. Introduction
2. Materials and Methods
3. Effectiveness of Vitamin D Supplementation in Children with ASD
3.1. Vitamin D Status and Association with ASD Severity
3.2. Effectiveness of Vitamin D Supplementation on ASD Severity
3.3. Vitamin D Supplementation and Age for Intervention
3.4. Effectiveness of Vitamin D Supplementation on Secondary Outcomes
3.5. Safety and Tolerability of Vitamin D Supplementation
4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Cannell, J.J. Vitamin D and autism, what’s new? Rev. Endocr. Metab. Disord. 2017, 18, 183–193. [Google Scholar] [CrossRef]
- CDC Diagnostic Criteria. Autism Spectrum Disorder (ASD). NCBDDD. CDC. Available online: https://www.cdc.gov/ncbddd/autism/hcp-dsm.html (accessed on 22 April 2021).
- WHO. Autism Spectrum Disorders. Available online: https://www.who.int/news-room/fact-sheets/detail/autism-spectrum-disorders (accessed on 23 April 2021).
- Centers for Disease Control and Prevention. Data & Statistics on Autism Spectrum Disorder. Available online: https://www.cdc.gov/ncbddd/autism/data.html (accessed on 23 April 2021).
- Salhia, H.O.; Al-Nasser, L.A.; Taher, L.S.; Al-Khathaami, A.M.; El-Metwally, A.A. Systemic review of the epidemiology of autism in Arab Gulf countries. Neurosciences 2014, 19, 291–296. [Google Scholar] [PubMed]
- Abrahams, B.S.; Geschwind, D.H. Advances in autism genetics: On the threshold of a new neurobiology. Nat. Rev. Genet. 2008, 9, 341–355. [Google Scholar] [CrossRef] [Green Version]
- Hisle-Gorman, E.; Susi, A.; Stokes, T.; Gorman, G.; Erdie-Lalena, C.; Nylund, C.M. Prenatal, perinatal, and neonatal risk factors of autism spectrum disorder. Pediatr. Res. 2018, 84, 190–198. [Google Scholar] [CrossRef]
- Kim, J.Y.; Son, M.J.; Son, C.Y.; Radua, J.; Eisenhut, M.; Gressier, F.; Koyanagi, A.; Carvalho, A.F.; Stubbs, B.; Solmi, M.; et al. Environmental risk factors and biomarkers for autism spectrum disorder: An umbrella review of the evidence. Lancet Psychiatry 2019, 6, 590–600. [Google Scholar] [CrossRef] [Green Version]
- Modabbernia, A.; Velthorst, E.; Reichenberg, A. Environmental risk factors for autism: An evidence-based review of systematic reviews and meta-analyses. Mol. Autism 2017, 8, 13. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Environmental Health Sciences Autism. Available online: https://www.niehs.nih.gov/health/topics/conditions/autism/index.cfm (accessed on 23 April 2021).
- Krebs, N.F.; Lozoff, B.; Georgieff, M.K. Neurodevelopment: The Impact of Nutrition and Inflammation during Infancy in Low-Resource Settings. Pediatrics 2017, 139, S50–S58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, B.K.; Eyles, D.W.; Magnusson, C.; Newschaffer, C.J.; McGrath, J.J.; Kvaskoff, D.; Ko, P.; Dalman, C.; Karlsson, H.; Gardner, R.M. Developmental vitamin D and autism spectrum disorders: Findings from the Stockholm Youth Cohort. Mol. Psychiatry 2019, 26, 1578–1588. [Google Scholar] [CrossRef] [Green Version]
- Anjos, T.; The NUTRIMENTHE Research Group; Altmäe, S.; Emmett, P.; Tiemeier, H.; Closa-Monasterolo, R.; Luque, V.; Wiseman, S.; Pérez-García, M.; Lattka, E.; et al. Nutrition and neurodevelopment in children: Focus on NUTRIMENTHE project. Eur. J. Nutr. 2013, 52, 1825–1842. [Google Scholar] [CrossRef]
- Schwarzenberg, S.J.; Georgieff, M.K.; Committee on Nutrition. Advocacy for improving nutrition in the first 1000 days to support childhood development and adult health. Pediatrics 2018, 141, e20173716. [Google Scholar] [CrossRef] [Green Version]
- Gil, Á.; Plaza-Diaz, J.; Mesa, M.D. Vitamin D: Classic and Novel Actions. Ann. Nutr. Metab. 2018, 72, 87–95. [Google Scholar] [CrossRef]
- Siracusano, M.; Riccioni, A.; Abate, R.; Benvenuto, A.; Curatolo, P.; Mazzone, L. Vitamin D Deficiency and Autism Spectrum Disorder. Curr. Pharm. Des. 2020, 26, 2460–2474. [Google Scholar] [CrossRef] [PubMed]
- Şengenç, E.; Kiykim, E.; Saltık, S. Vitamin D levels in children and adolescents with autism. J. Int. Med. Res. 2020, 48, 0300060520934638. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Zhang, L.; Xu, H.-J.; Li, Y.; Hu, C.-M.; Yang, J.-Y.; Sun, M.-Y. The Anti-Inflammatory Effects of Vitamin D in Tumorigenesis. Int. J. Mol. Sci. 2018, 19, 2736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masi, A.; Quintana, D.S.; Glozier, N.; Lloyd, A.R.; Hickie, I.; Guastella, A.J. Cytokine aberrations in autism spectrum disorder: A systematic review and meta-analysis. Mol. Psychiatry 2015, 20, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.-J.; Tan, H.-P.; Yang, F.-Y.; Liu, C.-L.; Sang, B.; Zhu, X.-M.; Du, Y.-J. The roles of cortisol and pro-inflammatory cytokines in assisting the diagnosis of autism spectrum disorder. Res. Autism Spectr. Disord. 2015, 9, 174–181. [Google Scholar] [CrossRef]
- Xu, N.; Li, X.; Zhong, Y. Inflammatory Cytokines: Potential Biomarkers of Immunologic Dysfunction in Autism Spectrum Disorders. Mediat. Inflamm. 2015, 2015, 531518. [Google Scholar] [CrossRef] [Green Version]
- Filgueiras, M.S.; Rocha, N.P.; Novaes, J.F.; Bressan, J. Vitamin D status, oxidative stress, and inflammation in children and adolescents: A systematic review. Crit. Rev. Food Sci. Nutr. 2020, 60, 660–669. [Google Scholar] [CrossRef]
- Calton, E.K.; Keane, K.N.; Newsholme, P.; Soares, M.J. The Impact of Vitamin D Levels on Inflammatory Status: A Systematic Review of Immune Cell Studies. PLoS ONE 2015, 10, e0141770. [Google Scholar] [CrossRef]
- Patrick, R.P.; Ames, B.N. Vitamin D hormone regulates serotonin synthesis. Part 1: Relevance for autism. FASEB J. 2014, 28, 2398–2413. [Google Scholar] [CrossRef] [Green Version]
- Berridge, M.J. Vitamin D deficiency: Infertility and neurodevelopmental diseases (attention deficit hyperactivity disorder, autism, and schizophrenia). Am. J. Physiol. Physiol. 2018, 314, C135–C151. [Google Scholar] [CrossRef] [Green Version]
- Patrick, R.P.; Ames, B.N. Vitamin D and the omega-3 fatty acids control serotonin synthesis and action, part 2: Relevance for ADHD, bipolar disorder, schizophrenia, and impulsive behavior. FASEB J. 2015, 29, 2207–2222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, S.Y.; Yoo, H.J.; Cho, I.H.; Park, M.; Kim, S.A. Association with tryptophan hydroxylase 2 gene polymorphisms and autism spectrum disorders in Korean families. Neurosci. Res. 2012, 73, 333–336. [Google Scholar] [CrossRef] [PubMed]
- Seyedi, M.; Gholami, F.; Samadi, M.; Djalali, M.; Effatpanah, M.; Yekaninejad, M.S.; Hashemi, R.; Abdolahi, M.; Chamari, M.; Honarvar, N.M. The Effect of Vitamin D3 Supplementation on Serum BDNF, Dopamine, and Serotonin in Children with Attention-Deficit/Hyperactivity Disorder. CNS Neurol. Disord. Drug Targets 2019, 18, 496–501. [Google Scholar] [CrossRef]
- Sabir, M.S.; Haussler, M.R.; Mallick, S.; Kaneko, I.; Lucas, D.A.; Haussler, C.A.; Whitfield, G.K.; Jurutka, P.W. Optimal vitamin D spurs serotonin: 1,25-dihydroxyvitamin D represses serotonin reuptake transport (SERT) and degradation (MAO-A) gene expression in cultured rat serotonergic neuronal cell lines. Genes Nutr. 2018, 13, 19. [Google Scholar] [CrossRef] [PubMed]
- Alfawaz, H.A.; Bhat, R.S.; Al-Ayadhi, L.; El-Ansary, A.K. Protective and restorative potency of Vitamin D on persistent biochemical autistic features induced in propionic acid-intoxicated rat pups. BMC Complement. Altern. Med. 2014, 14, 416. [Google Scholar] [CrossRef] [Green Version]
- Ansari, M.G.A.; Sabico, S.; Clerici, M.; Khattak, M.N.K.; Wani, K.; Al-Musharaf, S.; Amer, O.E.; Alokail, M.S.; Al-Daghri, N.M. Vitamin D Supplementation is Associated with Increased Glutathione Peroxidase-1 Levels in Arab Adults with Prediabetes. Antioxidants 2020, 9, 118. [Google Scholar] [CrossRef] [Green Version]
- Bjørklund, G.; Tinkov, A.A.; Hosnedlová, B.; Kizek, R.; Ajsuvakova, O.P.; Chirumbolo, S.; Skalnaya, M.G.; Peana, M.; Dadar, M.; El-Ansary, A.; et al. The role of glutathione redox imbalance in autism spectrum disorder: A review. Free Radic. Biol. Med. 2020, 160, 149–162. [Google Scholar] [CrossRef]
- Gezen-AK, D.; Dursun, E.; Yilmazer, S. The Effect of Vitamin D Treatment on Nerve Growth Factor (NGF) Release from Hippocampal Neurons. Noro Psikiyatr. Ars. 2014, 51, 157–162. [Google Scholar] [CrossRef] [Green Version]
- Naveilhan, P.; Neveu, I.; Wion, D.; Brachet, P. 1,25-Dihydroxyvitamin D3, an inducer of glial cell line-derived neurotrophic factor. NeuroReport 1996, 7, 2171–2175. [Google Scholar] [CrossRef]
- Huang, E.J.; Reichardt, L.F. Neurotrophins: Roles in Neuronal Development and Function. Annu. Rev. Neurosci. 2001, 24, 677–736. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.; Bianco, J.I.; McGrath, J.J.; Eyles, D.W. 1,25-Dihydroxyvitamin D3 induces nerve growth factor, promotes neurite outgrowth and inhibits mitosis in embryonic rat hippocampal neurons. Neurosci. Lett. 2003, 343, 139–143. [Google Scholar] [CrossRef]
- Pozzi, F.; Aloe, L.; Frajese, G.V.; Frajese, G. Vitamin D (Calcifediol) Supplementation Modulates NGF and BDNF and Improves Memory Function in Postmenopausal Women: A Pilot Study. Res. Endocrinol. 2013, 2013, 552758. [Google Scholar] [CrossRef] [Green Version]
- Moradi, H.; Sohrabi, M.; Taheri, H.; Khodashenas, E.; Movahedi, A. The effects of different combinations of perceptual-motor exercises, music, and vitamin D supplementation on the nerve growth factor in children with high-functioning autism. Complement. Ther. Clin. Pract. 2018, 31, 139–145. [Google Scholar] [CrossRef]
- Liu, S.-H.; Shi, X.-J.; Fan, F.-C.; Cheng, Y. Peripheral blood neurotrophic factor levels in children with autism spectrum disorder: A meta-analysis. Sci. Rep. 2021, 11, 15. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, G.A.; Meguid, N.A.; Shehab, A.A.S.; Elsaeid, A.; Maher, M. Plasma levels of nerve growth factor in Egyptian autistic children: Relation to hyperserotonemia and autoimmunity. J. Neuroimmunol. 2021, 358, 577638. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, D.H.; Rocha, N.P.; da Cunha Sousa, L.F.; Barbosa, I.G.; Kummer, A.; Teixeira, A.L. Circulating levels of neurotrophic factors in autism spectrum disorders. Neuro Endocrinol. Lett. 2014, 35, 380–384. [Google Scholar]
- Cannell, J.; Grant, W.B. What is the role of vitamin D in autism? Derm. Endocrinol. 2013, 5, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Orme, R.P.; Bhangal, M.S.; Fricker, R.A. Calcitriol Imparts Neuroprotection In Vitro to Midbrain Dopaminergic Neurons by Upregulating GDNF Expression. PLoS ONE 2013, 8, e62040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kočovská, E.; Fernell, E.; Billstedt, E.; Minnis, H.; Gillberg, C. Vitamin D and autism: Clinical review. Res. Dev. Disabil. 2012, 33, 1541–1550. [Google Scholar] [CrossRef]
- Bauman, M.L. Medical comorbidities in autism: Challenges to diagnosis and treatment. Neurotherapeutics 2010, 7, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Frye, R.E.; Casanova, M.F.; Fatemi, S.H.; Folsom, T.D.; Reutiman, T.J.; Brown, G.L.; Edelson, S.M.; Slattery, J.C.; Adams, J.B. Neuropathological Mechanisms of Seizures in Autism Spectrum Disorder. Front. Neurosci. 2016, 10, 192. [Google Scholar] [CrossRef] [Green Version]
- Jazayeri, M.; Moradi, Y.; Rasti, A.; Nakhjavani, M.; Kamali, M.; Baradaran, H.R. Prevalence of vitamin D deficiency in healthy Iranian children: A systematic review and meta-analysis. Med. J. Islam. Repub. Iran 2018, 32, 83. [Google Scholar] [CrossRef] [Green Version]
- Mogire, R.M.; Mutua, A.; Kimita, W.; Kamau, A.; Bejon, P.; Pettifor, J.; Adeyemo, A.; Williams, T.N.; Atkinson, S.H. Prevalence of vitamin D deficiency in Africa: A systematic review and meta-analysis. Lancet Glob. Health 2020, 8, e134–e142. [Google Scholar] [CrossRef] [Green Version]
- Alzghoul, L.; Al-Eitan, L.N.; Aladawi, M.; Odeh, M.; Hantash, O.A. The Association between Serum Vitamin D3 Levels and Autism among Jordanian Boys. J. Autism Dev. Disord. 2020, 50, 3149–3154. [Google Scholar] [CrossRef] [PubMed]
- Arastoo, A.A.; Khojastehkia, H.; Rahimi, Z.; Khafaie, M.A.; Hosseini, S.A.; Mansouri, M.T.; Yosefyshad, S.; Abshirini, M.; Karimimalekabadi, N.; Cheraghi, M. Evaluation of serum 25-Hydroxy vitamin D levels in children with autism Spectrum disorder. Ital. J. Pediatr. 2018, 44, 150. [Google Scholar] [CrossRef] [PubMed]
- Bener, A.; Khattab, A.O.; Al-Dabbagh, M.M. Is high prevalence of Vitamin D deficiency evidence for autism disorder? In a highly endogamous population. J. Pediatr. Neurosci. 2014, 9, 227–233. [Google Scholar] [CrossRef] [Green Version]
- Desoky, T.; Hassan, M.H.; Fayed, H.; Sakhr, H.M. Biochemical assessments of thyroid profile, serum 25-hydroxycholecalciferol and cluster of differentiation 5 expression levels among children with autism. Neuropsychiatr. Dis. Treat. 2017, 13, 2397–2403. [Google Scholar] [CrossRef] [Green Version]
- El-Ansary, A.; Cannell, J.J.; Bjørklund, G.; Bhat, R.S.; Al Dbass, A.M.; Alfawaz, H.A.; Chirumbolo, S.; Al-Ayadhi, L. In the search for reliable biomarkers for the early diagnosis of autism spectrum disorder: The role of vitamin D. Metab. Brain Dis. 2018, 33, 917–931. [Google Scholar] [CrossRef]
- Fahmy, F.; Sabri, N.; El Hamamsy, M.; El Sawi, M.; Zaki, O. Vitamin D Intake and Sun Exposure in Autistic Children. Int. J. Pharm. Sci. Res. 2016, 7, 1043–1049. [Google Scholar]
- Saad, K.; Abdel-Rahman, A.A.; Elserogy, Y.M.; Al-Atram, A.A.; Cannell, J.J.; Bjørklund, G.; Abdel-Reheim, M.K.; Othman, H.A.K.; Houfey, A.A.E.; El-Aziz, N.H.R.A.; et al. Vitamin D status in autism spectrum disorders and the efficacy of vitamin D supplementation in autistic children. Nutr. Neurosci. 2016, 19, 346–351. [Google Scholar] [CrossRef]
- Mostafa, G.A.; Al-Ayadhi, L.Y. Reduced serum concentrations of 25-hydroxy vitamin D in children with autism: Relation to autoimmunity. J. Neuroinflamm. 2012, 9, 201. [Google Scholar] [CrossRef] [Green Version]
- Zachor, D.; Ben-Itzchak, E.; Rabinovich, A.-L.; Lahat, E. Change in autism core symptoms with intervention. Res. Autism Spectr. Disord. 2007, 1, 304–317. [Google Scholar] [CrossRef]
- Javadfar, Z.; Abdollahzad, H.; Moludi, J.; Rezaeian, S.; Amirian, H.; Foroughi, A.A.; Nachvak, S.M.; Goharmehr, N.; Mostafai, R. Effects of vitamin D supplementation on core symptoms, serum serotonin, and interleukin-6 in children with autism spectrum disorders: A randomized clinical trial. Nutrition 2020, 79–80, 110986. [Google Scholar] [CrossRef] [PubMed]
- Ucuz, I.I.; Dursun, O.B.; Esin, I.S.; Özgeriş, F.B.; Kurt, N.; Kiziltunç, A.; Orbak, Z. The relationship between Vitamin D, autistic spectrum disorders, and cognitive development: Do glial cell line-derived neurotrophic factor and nerve growth factor play a role in this relationship? Int. J. Dev. Disabil. 2014, 61, 222–230. [Google Scholar] [CrossRef]
- Feng, J.; Shan, L.; Du, L.; Wang, B.; Li, H.; Wang, W.; Wang, T.; Dong, H.; Yue, X.; Xu, Z.; et al. Clinical improvement following vitamin D3 supplementation in Autism Spectrum Disorder. Nutr. Neurosci. 2017, 20, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Olmos-Ortiz, A.; Avila, E.; Durand-Carbajal, M.; Díaz, L. Regulation of Calcitriol Biosynthesis and Activity: Focus on Gestational Vitamin D Deficiency and Adverse Pregnancy Outcomes. Nutrients 2015, 7, 443–480. [Google Scholar] [CrossRef] [Green Version]
- Azzam, H.M.; Sayyah, H.; Youssef, S.; Lotfy, H.; Abdelhamid, I.A.; Elhamed, H.A.A.; Maher, S. Autism and vitamin D: An Intervention Study. Middle East Curr. Psychiatry 2015, 22, 9–14. [Google Scholar] [CrossRef]
- Kerley, C.P.; Power, C.; Gallagher, L.; Coghlan, D. Lack of effect of vitamin D3 supplementation in autism: A 20-week, placebo-controlled RCT. Arch. Dis. Child. 2017, 102, 1030–1036. [Google Scholar] [CrossRef] [Green Version]
- Jia, F.; Wang, B.; Shan, L.; Xu, Z.; Staal, W.G.; Du, L. Core Symptoms of Autism Improved after Vitamin D Supplementation. Pediatrics 2015, 135, e196–e198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, F.; Shan, L.; Wang, B.; Li, H.; Feng, J.; Xu, Z.; Saad, K. Fluctuations in clinical symptoms with changes in serum 25(OH) vitamin D levels in autistic children: Three cases report. Nutr. Neurosci. 2019, 22, 863–866. [Google Scholar] [CrossRef]
- Moradi, H.; Sohrabi, M.; Taheri, H.; Khodashenas, E.; Movahedi, A. Comparison of the effects of perceptual-motor exercises, vitamin D supplementation and the combination of these interventions on decreasing stereotypical behavior in children with autism disorder. Int. J. Dev. Disabil. 2020, 66, 122–132. [Google Scholar] [CrossRef]
- Bent, S.; Ailarov, A.; Dang, K.T.; Widjaja, F.; Lawton, B.L.; Hendren, R.L. Open-Label Trial of Vitamin D3 Supplementation in Children with Autism Spectrum Disorder. J. Altern. Complement. Med. 2017, 23, 394–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazahery, H.; Conlon, C.A.; Beck, K.L.; Mugridge, O.; Kruger, M.C.; Stonehouse, W.; Camargo, C.A.; Meyer, B.J.; Tsang, B.; Jones, B.; et al. A Randomised-Controlled Trial of Vitamin D and Omega-3 Long Chain Polyunsaturated Fatty Acids in the Treatment of Core Symptoms of Autism Spectrum Disorder in Children. J. Autism Dev. Disord. 2019, 49, 1778–1794. [Google Scholar] [CrossRef]
- Mazahery, H.; Conlon, C.A.; Beck, K.L.; Mugridge, O.; Kruger, M.C.; Stonehouse, W.; Camargo, C.A.; Meyer, B.J.; Jones, B.; von Hurst, P.R. A randomised controlled trial of vitamin D and omega-3 long chain polyunsaturated fatty acids in the treatment of irritability and hyperactivity among children with autism spectrum disorder. J. Steroid Biochem. Mol. Biol. 2019, 187, 9–16. [Google Scholar] [CrossRef]
- Datta, S.; Pal, M.; De, A. The Dependency of Vitamin D Status on Anthropometric Data. Malays. J. Med. Sci. 2014, 21, 54–61. [Google Scholar]
- Nouri-Vaskeh, M.; Ouladsahebmadarek, E. Role of Confounding Factors in the Evaluation of Vitamin D Deficiency. Crescent J. Med. Biol. Sci. 2019, 6, 555–556. [Google Scholar]
- Ekwaru, J.P.; Zwicker, J.D.; Holick, M.F.; Giovannucci, E.; Veugelers, P.J. The Importance of Body Weight for the Dose Response Relationship of Oral Vitamin D Supplementation and Serum 25-Hydroxyvitamin D in Healthy Volunteers. PLoS ONE 2014, 9, e111265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institutes of Health Vitamin D—Fact Sheet for Health Professionals. Available online: https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/ (accessed on 12 August 2021).
- Grégoire-Pelchat, P.; Pastore, Y.; Robitaille, N.; Lemay, S.; Khamessan, A.; Kleiber, N.; Nyalendo, C.; Gagné, N.; Alos, N.; Mailhot, G. Comparison of two vitamin D supplementation strategies in children with sickle cell disease: A randomized controlled trial. Br. J. Haematol. 2021, 192, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Kojecky, V.; Matous, J.; Kianicka, B.; Dite, P.; Zadorova, Z.; Kubovy, J.; Hlostova, M.; Uher, M. Vitamin D levels in IBD: A randomised trial of weight-based versus fixed dose vitamin D supplementation. Scand. J. Gastroenterol. 2020, 55, 671–676. [Google Scholar] [CrossRef] [PubMed]
- Krol, A.; Feng, G. Windows of opportunity: Timing in neurodevelopmental disorders. Curr. Opin. Neurobiol. 2018, 48, 59–63. [Google Scholar] [CrossRef]
- Vinkhuyzen, A.A.E.; Eyles, D.; Burne, T.; Blanken, L.M.E.; Kruithof, C.J.; Verhulst, F.; White, T.; Jaddoe, V.W.; Tiemeier, H.; McGrath, J.J. Gestational vitamin D deficiency and autism spectrum disorder. BJPsych Open 2017, 3, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Ding, R.; Wang, J. The Association between Vitamin D Status and Autism Spectrum Disorder (ASD): A Systematic Review and Meta-Analysis. Nutrients 2020, 13, 86. [Google Scholar] [CrossRef]
- Stubbs, G.; Henley, K.; Green, J. Autism: Will vitamin D supplementation during pregnancy and early childhood reduce the recurrence rate of autism in newborn siblings? Med. Hypotheses 2016, 88, 74–78. [Google Scholar] [CrossRef]
- Khakzad, M.R.; Javanbakht, M.; Shayegan, M.R.; Kianoush, S.; Omid, F.; Hojati, M.; Meshkat, M. The complementary role of high sensitivity C-reactive protein in the diagnosis and severity assessment of autism. Res. Autism Spectr. Disord. 2012, 6, 1032–1037. [Google Scholar] [CrossRef]
- Kruit, A.; Zanen, P. The association between vitamin D and C-reactive protein levels in patients with inflammatory and non-inflammatory diseases. Clin. Biochem. 2016, 49, 534–537. [Google Scholar] [CrossRef]
- Ngo, D.T.; Sverdlov, A.; McNeil, J.; Horowitz, J. Does Vitamin D Modulate Asymmetric Dimethylarginine and C-Reactive Protein Concentrations? Am. J. Med. 2010, 123, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Mazidi, M.; Rezaie, P.; Vatanparast, H. Impact of vitamin D supplementation on C-reactive protein; a systematic review and meta-analysis of randomized controlled trials. BMC Nutr. 2018, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, N.; Wan, Z.; Han, S.-F.; Li, B.-Y.; Zhang, Z.-L.; Qin, L.-Q. Effect of Vitamin D Supplementation on the Level of Circulating High-Sensitivity C-Reactive Protein: A Meta-Analysis of Randomized Controlled Trials. Nutrients 2014, 6, 2206–2216. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in Inflammation, Immunity, and Disease. Cold Spring Harb. Perspect. Biol. 2014, 6, a016295. [Google Scholar] [CrossRef]
- Rostkowska-Nadolska, B.; Sliupkas-Dyrda, E.; Potyka, J.; Kusmierz, D.; Fraczek, M.; Krecicki, T.; Kubik, P.; Zatonski, M.; Latocha, M. Vitamin D derivatives: Calcitriol and tacalcitol inhibits interleukin-6 and interleukin-8 expression in human nasal polyp fibroblast cultures. Adv. Med. Sci. 2010, 55, 86–92. [Google Scholar] [CrossRef]
- Khoo, A.-L.; Chai, L.Y.A.; Koenen, H.J.P.M.; Sweep, F.C.G.J.; Joosten, I.; Netea, M.G.; van der Ven, A.J.A.M. Regulation of cytokine responses by seasonality of vitamin D status in healthy individuals. Clin. Exp. Immunol. 2011, 164, 72–79. [Google Scholar] [CrossRef]
- Hashemi, R.; Morshedi, M.; Jafarabadi, M.A.; Altafi, D.; Hosseini-Asl, S.S.; Rafie-Arefhosseini, S. Anti-inflammatory effects of dietary vitamin D3 in patients with multiple sclerosis. Neurol. Genet. 2018, 4, e278. [Google Scholar] [CrossRef] [Green Version]
- Miroliaee, A.E.; Salamzadeh, J.; Shokouhi, S.; Sahraei, Z. The study of vitamin D administration effect on CRP and Interleukin-6 as prognostic biomarkers of ventilator associated pneumonia. J. Crit. Care 2018, 44, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Tian, L.; Xiao, Y.; Huang, G.; Zhang, M. Effect of Vitamin D Supplementation on Some Inflammatory Biomarkers in Type 2 Diabetes Mellitus Subjects: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Ann. Nutr. Metab. 2018, 73, 62–73. [Google Scholar] [CrossRef]
- Jamka, M.; Wozniewicz, M.; Walkowiak, J.; Bogdański, P.; Jeszka, J.; Stelmach-Mardas, M. The effect of vitamin D supplementation on selected inflammatory biomarkers in obese and overweight subjects: A systematic review with meta-analysis. Eur. J. Nutr. 2016, 55, 2163–2176. [Google Scholar] [CrossRef]
- Weissmiller, A.M.; Wu, C. Current advances in using neurotrophic factors to treat neurodegenerative disorders. Transl. Neurodegener. 2012, 1, 14. [Google Scholar] [CrossRef] [Green Version]
- Vuillermot, S.; Luan, W.; Meyer, U.; Eyles, D. Vitamin D treatment during pregnancy prevents autism-related phenotypes in a mouse model of maternal immune activation. Mol. Autism 2017, 8, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maalouf, J.; Nabulsi, M.; Vieth, R.; Kimball, S.; El Rassi, R.; Mahfoud, Z.; Fuleihan, G.E.-H. Short- and Long-Term Safety of Weekly High-Dose Vitamin D3 Supplementation in School Children. J. Clin. Endocrinol. Metab. 2008, 93, 2693–2701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stallings, V.A.; Schall, J.I.; Hediger, M.L.; Zemel, B.S.; Tuluc, F.; Dougherty, K.A.; Samuel, J.L.; Rutstein, R.M. High-dose Vitamin D3 Supplementation in Children and Young Adults with HIV: A Randomized, Placebo-Controlled Trial. Pediatr. Infect. Dis. J. 2015, 34, e32–e40. [Google Scholar] [CrossRef] [Green Version]
- Balvers, M.; Brouwer-Brolsma, E.M.; Endenburg, S.; de Groot, L.C.P.G.M.; Kok, F.J.; Gunnewiek, J.K. Recommended intakes of vitamin D to optimise health, associated circulating 25-hydroxyvitamin D concentrations, and dosing regimens to treat deficiency: Workshop report and overview of current literature. J. Nutr. Sci. 2015, 4, e23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerini, F.R.; Bolognesi, E.; Chiappedi, M.; Mensi, M.M.; Fumagalli, O.; Rogantini, C.; Zanzottera, M.; Ghezzo, A.; Zanette, M.; Agliardi, C.; et al. Vitamin D Receptor Polymorphisms Associated with Autism Spectrum Disorder. Autism Res. 2020, 13, 680–690. [Google Scholar] [CrossRef]
- Barry, E.L.; Peacock, J.L.; Rees, J.R.; Bostick, R.M.; Robertson, D.J.; Bresalier, R.; Baron, J.A. Vitamin D Receptor Genotype, Vitamin D3 Supplementation, and Risk of Colorectal Adenomas: A Randomized Clinical Trial. JAMA Oncol. 2017, 3, 628–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carpenter, T.O.; Zhang, J.H.; Parra, E.J.; Ellis, B.K.; Simpson, C.; Lee, W.M.; Balko, J.; Fu, L.; Wong, B.Y.-L.; Cole, D.E.C. Vitamin D binding protein is a key determinant of 25-hydroxyvitamin D levels in infants and toddlers. J. Bone Miner. Res. 2013, 28, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.J.; Hansen, R.L.; Hartiala, J.; Allayee, H.; Sconberg, J.L.; Schmidt, L.C.; Volk, H.E.; Tassone, F. Selected vitamin D metabolic gene variants and risk for autism spectrum disorder in the CHARGE Study. Early Hum. Dev. 2015, 91, 483–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
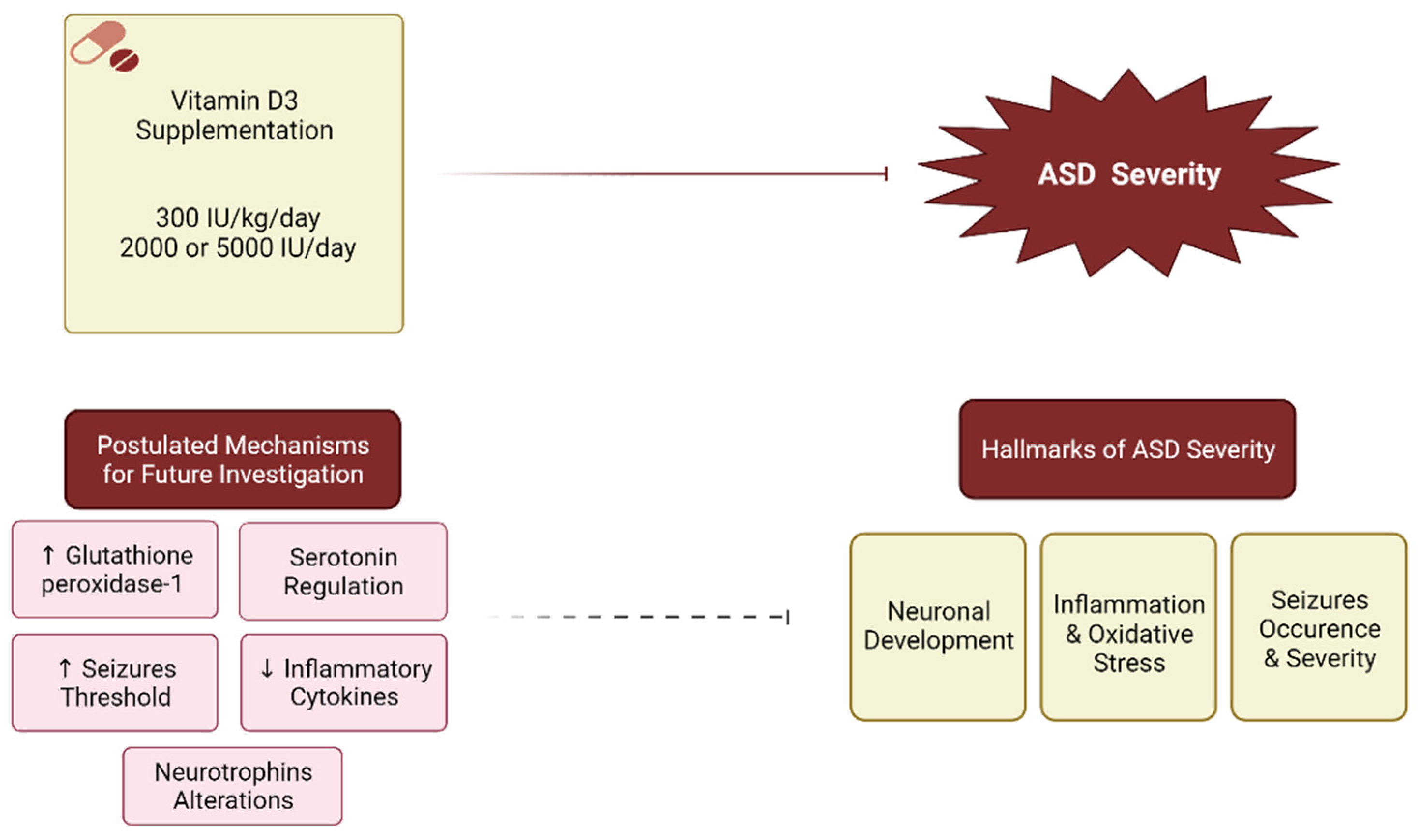
 , Postulated inhibition:
, Postulated inhibition:  .
, Postulated inhibition: .
.
, Postulated inhibition: .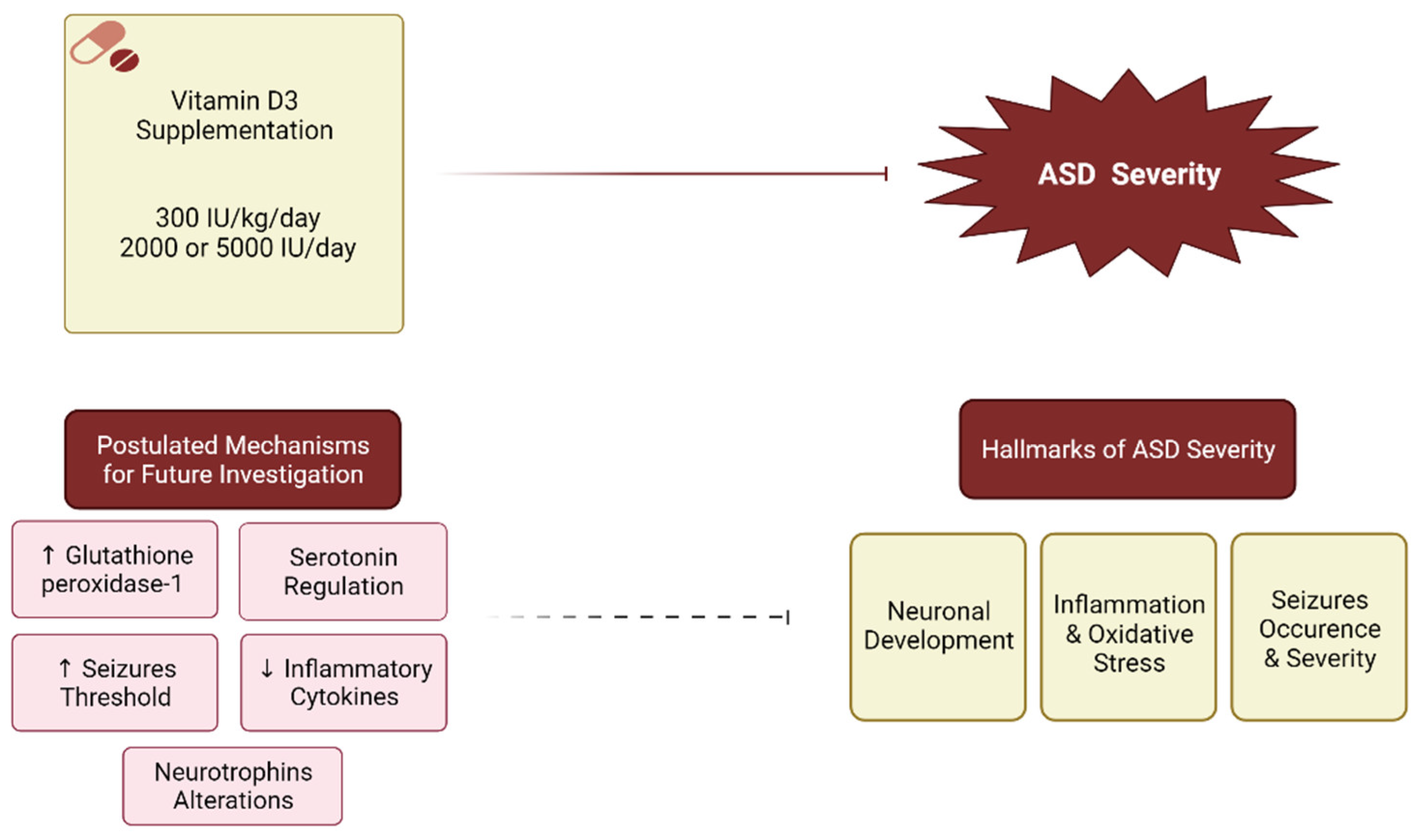

{kind=link}
| # | First Author (Year) | Study Design | Total Participants Analyzed, Age, and Gender | Treatment Details and Total Participants | Control Group/s and Total Participants | Duration | 25(OH)D Change in Cases (ng/mL) | 25(OH)D Change in Controls (ng/mL) | ASD Severity Measure | Before-after Change (Mean Trend) | Between Groups Comparison (p-Value) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Azzam (2015) [62] | Prospective, randomized, controlled study | n = 21 Age: 2–12 y. M:F: 16:5 | 2000 IU/day of vitamin D3 (n = 10) |
| 6 months | 47 ± 20 to 71 ± 35 (nmol/L) | 69 ± 41 to 70 ± 36 (nmol/L) | CARS | Decrease † | NS * |
| VABS | Increase † | NS * | |||||||||
| ATEC | Decrease † | NS * | |||||||||
| 2 | Javadfar (2020) [58] | Randomized, double-blind, placebo-controlled, parallel-group trial | n = 43 Age: 3–13 y. M:F: 36:7 | 300 IU/kg/day (Max. 6000 IU/day) of vitamin D3 (n = 22) | Placebo (n = 21) | 15 weeks | 8.19 ± 6.78 to 39.10 ± 33.71 † | 10.84 ± 16.80 to 8.94 ± 8.03 | CARS | Decrease † | S |
| ATEC | Decrease † | S | |||||||||
| ABC-C subscales |
| NS | |||||||||
| 3 | Kerley (2017) [63] | double-blind, randomized, placebo-controlled trial. | n = 38. Age: <18 y. M:F: 33:5 | 2000 IU vitamin D3 (n = 18) | Placebo (n = 20) | 20 weeks. | 58.4 ± 17.9 to 86.1 † (nmol/L) | 51.7 ± 19.8 to 50.6 (nmol/L) | ABC | Decrease | NS |
| SRS | Decrease | NS | |||||||||
| DD-CGAS | Increase in all subscales | Self-care subscale: S, other: NS | |||||||||
| 4 | Mazahery (2019) [69] | Randomized placebo controlled double-blind study | n = 73 Age: 2.5–8 y. M:F: 60:13 | 2000 IU/day vitamin D3 (n = 19) |
| 12 months | 68 ± 21 to an increase by 27 ± 14 (nmol/L) | 55 ± 27 to an increase by 38% (nmol/L) | ABC domains | Irritability and hyperactivity: Decrease † Other: Decrease | Irritability and hyper-activity: S * Others: NS * |
| 5 | Mazahery (2019) [68] | Randomized placebo controlled double-blind study | n = 73 Age: 2.5–8 y. M:F: 60:13 | 2000 IU/day vitamin D3 (n = 19) |
| 12 months | 68 ± 21 to an increase by 27 ± 14 (nmol/L) | 55 ± 27 to an increase by 38% (nmol/L) | SRS | Decrease | NS * |
| SPM | Decrease | NS * | |||||||||
| 6 | Moradi (2020) [66] | Randomized Controlled Trial | n = 100 Age: 6–9 y. M:F: 100:0 | 300 IU/kg/day (max. 5000 IU/day) of vitamin D3 (n = 25) |
| 3 months. | 4.61 ± 12.60 to 6.48 ± 24.36 † | 4.87 ± 11.52 to 3.95 ± 11.08 | SS-GARS-2 | Decrease † | S * |
| 7 | Ucuz (2014) [59] | Before-and-after study | n = 21 Age: 2–5 y. | Vitamin D3 dose (n = 11)
| No supplementation (n = 10) | 4 months. Follow-up at 6 months | <20 (exact before-after values NR) | ≥20 (exact before-after values NR) | ABC * | Decrease † | NS |
| Denver II: | Increase † | NS |
| # | First Author (Year) | Study Design | Total Participants Analyzed, Age, and Gender | Treatment Details and Total Participants | Duration | 25(OH)D Levels (ng/mL) Cases | ASD Severity Measure | Before-after Change (Mean Trend) |
|---|---|---|---|---|---|---|---|---|
| 1 | Bent (2017) [67] | Open-Label Trial | n = 3 Age: 3–8 y. M:F: 0:3 | 6000 IU/day of vitamin D3 oil drops for the first 10 days followed by 300 IU/kg/day | 3 months | 28 ± 2 to 82 ± 50 | SRS | Decrease † |
| ABC | Decrease | |||||||
| 2 | Feng (2017) [60] | Before-and-after study design | n = 37 Mean age: NR ** M:F: NR | 150,000 IU/month IM, and 400 IU/day orally of vitamin D3 | 3 months | Significant increase (values could not be interpreted from figure) | ABC * | Decrease † |
| CARS | Decrease † | |||||||
| ATEC | Decrease † | |||||||
| ABC-C subscales | Irritability: Decrease † Lethargy: Decrease † Others: Decrease | |||||||
| 3 | Jia (2014) [64] | Case Report | n = 1 Age: 32 m. M:F: 1:0 | 150,000 IU/month IM and 400 IU/day orally of vitamin D3 | 2 months | 12.5 to 81.2 | ABC * | Decrease |
| CARS | Decrease | |||||||
| CGI | Decrease | |||||||
| 4 | Jia (2019) [65] | Case Series | n = 3 Age: 19–48 m. M:F: 3:0 | Patients 1: 150,000 IU/month IM and 800 IU/day orally of vitamin D3. Patients 2 and 3: NR | 1 month (repeated twice) | 1st: 14.50 ± 5.39 to 46.70 ± 6.78 2nd: 28.10 ± 0.78 to 45.17 ± 3.04 • | ABC * | Decrease |
| CARS | Decrease | |||||||
| 5 | Saad (2016) [55] | Open label trial | n = 83 Age: 3–9 y. M:F: 83:0 | 300 IU/kg/day (max.: 5000 IU/day) of vitamin D3 | 3 months | NR | CARS | Decrease † |
| ABC subscales | Irritiability, lethargy, hyperactivity, stereotypic behavior: Decrease † Inappropriate speech: Decrease |
| First Author (Year) | ASD Severity Measure | Subscales/Items | Before-after Change (Mean Trend) | Between Groups Comparison (p-Value) |
|---|---|---|---|---|
| Feng (2017) [60] | ABC * | Sensory | Decrease | N/A |
| Social skills | Decrease † | N/A | ||
| Body and object use | Decrease † | N/A | ||
| Language | Decrease † | N/A | ||
| Social or self-help | Decrease † | N/A | ||
| Javadfar (2020) [58] | ABC-C subscales | Irritability | Decrease † | NS |
| Lethargy/social withdrawal | Decrease | NS | ||
| Hyperactivity | Decrease † | NS | ||
| Inappropriate speech | Decrease | NS | ||
| Stereotypic behavior | Decrease | NS | ||
| Jia (2019) [65] | ABC * | Sensory | Mostly Decrease * | N/A |
| Social skills | Mostly Decrease * | N/A | ||
| Body and object use | Mostly Decrease * | N/A | ||
| Language | Always Decrease * | N/A | ||
| Social or self-help | Mostly Decrease * | N/A | ||
| Kerley (2017) [63] | ABC subscales | Irritability | Decrease | NS |
| Lethargy/social withdrawal | Decrease | NS | ||
| Hyperactivity | Decrease | NS | ||
| Inappropriate speech | Decrease | NS | ||
| Stereotypic behavior | Decrease | NS | ||
| DD-CGAS | Self-care | Increase | Increase † | |
| Communication | Increase | NS | ||
| Social behaviour | Increase | NS | ||
| School/academic | Increase | NS | ||
| Mazahery (2019) [69] | ABC domains | Irritability | Decrease | Decrease † |
| Lethargy/social withdrawal | Decrease | NS | ||
| Hyperactivity | Decrease | Decrease † | ||
| Inappropriate speech | Decrease | NS | ||
| Stereotypic behavior | Decrease | NS | ||
| Mazahery (2019) [68] | SRS | Social-communicative functioning | Decrease | NS |
| Social awareness | Decrease | NS | ||
| Social cognition | Decrease | NS | ||
| Social communication | Decrease | NS | ||
| Social motivation | Decrease | NS | ||
| repetitive/stereotypic interests and behaviours | Decrease | NS | ||
| SPM | Vision | Decrease | NS | |
| Hearing | Decrease | NS | ||
| Touch | Decrease | NS | ||
| Taste and smell | Decrease | NS | ||
| Body awareness | Decrease | NS | ||
| Balance and motion | Decrease | NS | ||
| Social participation | Decrease | NS | ||
| Saad (2016) [55] | CARS | Relating to people | Decrease † | N/A |
| Emotional response | Decrease † | N/A | ||
| Imitation | Decrease † | N/A | ||
| Body use | Decrease † | N/A | ||
| Object use | Decrease † | N/A | ||
| Adaptation to change | Decrease † | N/A | ||
| Listening response | Decrease † | N/A | ||
| Taste, smell, touch | Increase | N/A | ||
| Visual response | Decrease † | N/A | ||
| Fear | Decrease | N/A | ||
| Verbal communication | Decrease | N/A | ||
| Activity level | Decrease | N/A | ||
| Non-verbal communication | Increase | N/A | ||
| Level and consistency of intellectual response | Decrease | N/A | ||
| General impression | Decrease † | N/A | ||
| ABC subscales | Irritability | Decrease † | N/A | |
| Lethargy/social withdrawal | Decrease † | N/A | ||
| Hyperactivity | Decrease † | N/A | ||
| Inappropriate speech | NS | N/A | ||
| Stereotypic behavior | Decrease † | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kittana, M.; Ahmadani, A.; Stojanovska, L.; Attlee, A. The Role of Vitamin D Supplementation in Children with Autism Spectrum Disorder: A Narrative Review. Nutrients 2022, 14, 26. https://doi.org/10.3390/nu14010026
Kittana M, Ahmadani A, Stojanovska L, Attlee A. The Role of Vitamin D Supplementation in Children with Autism Spectrum Disorder: A Narrative Review. Nutrients. 2022; 14(1):26. https://doi.org/10.3390/nu14010026
Chicago/Turabian StyleKittana, Monia, Asma Ahmadani, Lily Stojanovska, and Amita Attlee. 2022. "The Role of Vitamin D Supplementation in Children with Autism Spectrum Disorder: A Narrative Review" Nutrients 14, no. 1: 26. https://doi.org/10.3390/nu14010026
APA StyleKittana, M., Ahmadani, A., Stojanovska, L., & Attlee, A. (2022). The Role of Vitamin D Supplementation in Children with Autism Spectrum Disorder: A Narrative Review. Nutrients, 14(1), 26. https://doi.org/10.3390/nu14010026