
Can Feeding a Millet-Based Diet Improve the Growth of Children?—A Systematic Review and Meta-Analysis

 , ,
, ,  , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
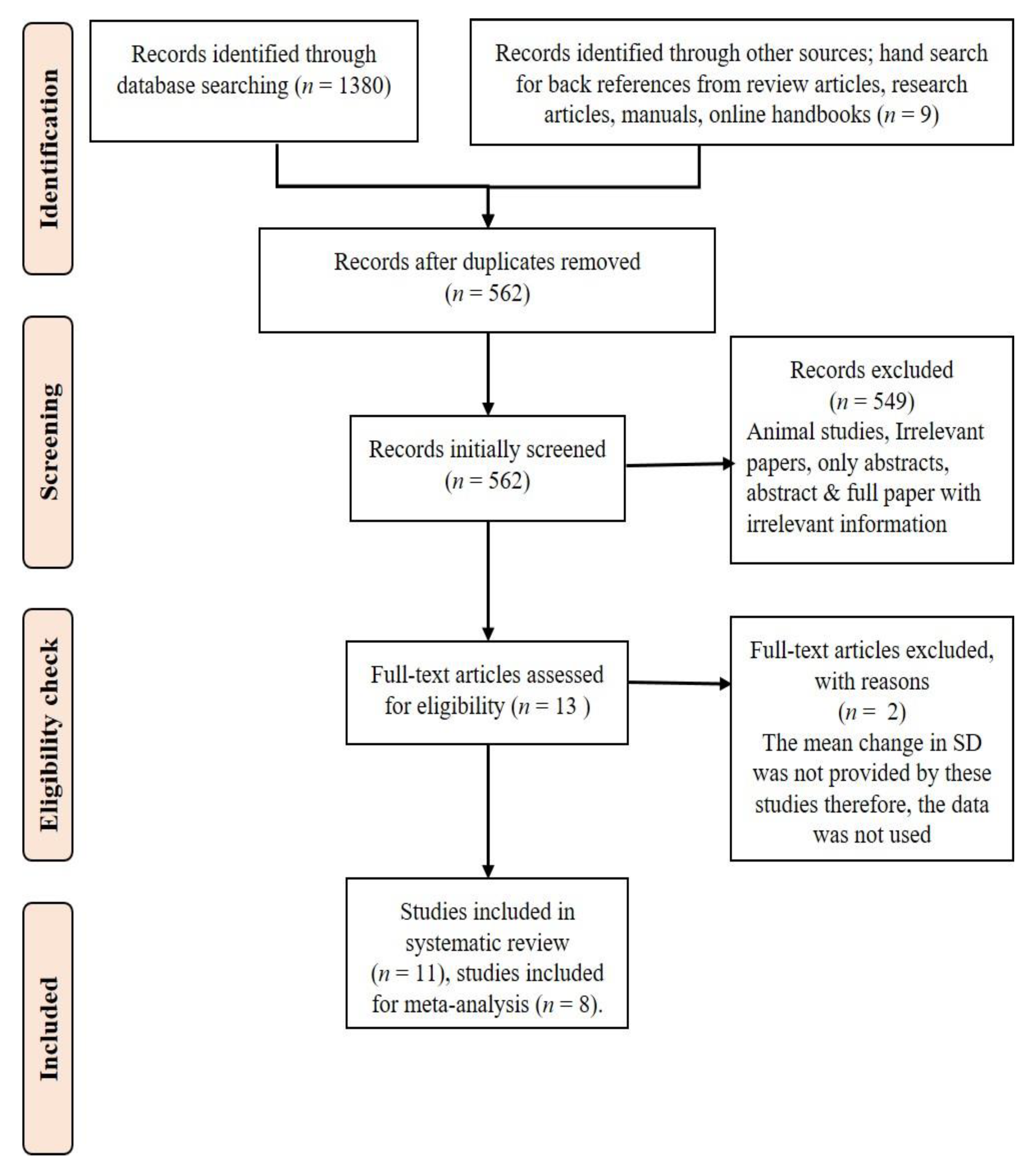
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection and Data Extraction
2.4. Risk of Bias Assessment
2.5. GRADE to Assess the Quality of the Evidence
2.6. Summary Measures and Result Synthesis
3. Results
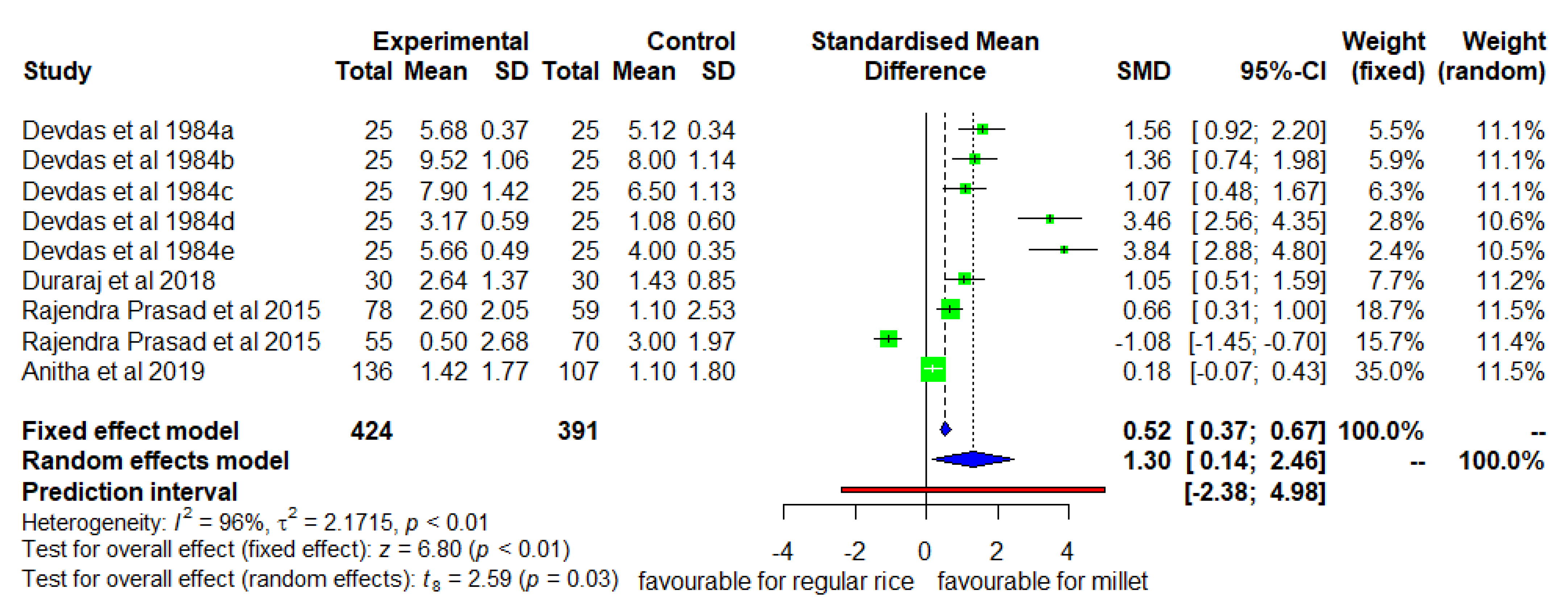
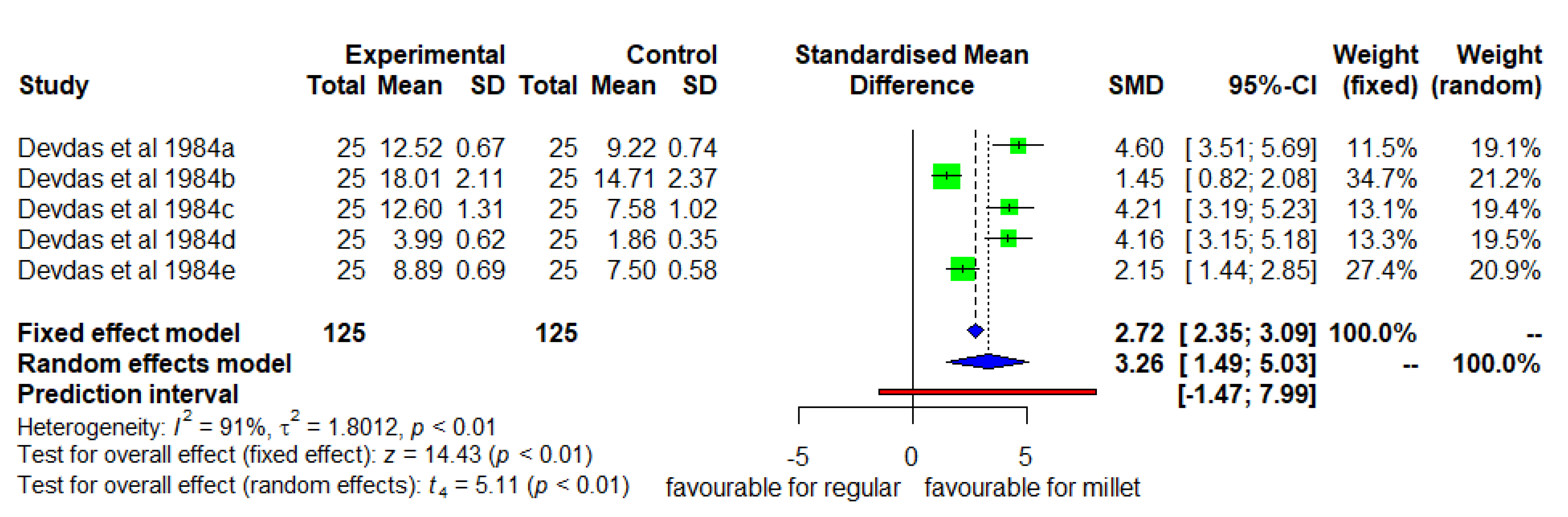
3.1. Mean Change in Height (Millet Diet vs. Regular Rice Based Diet)
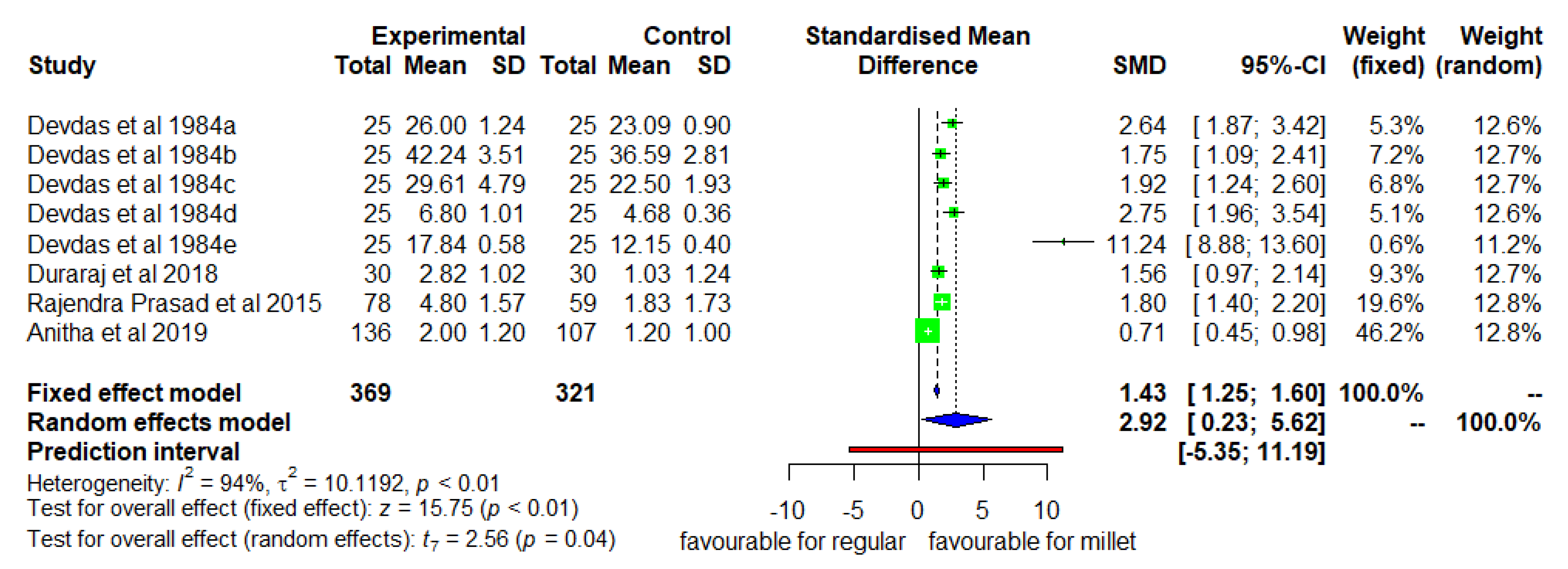
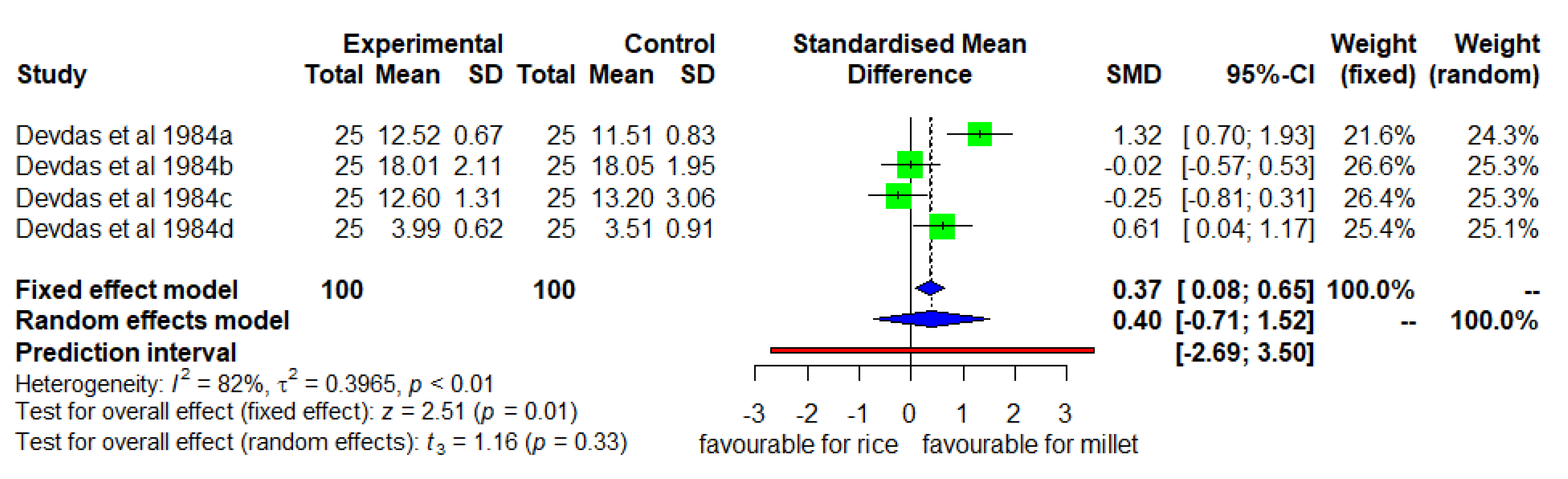
3.2. Mean Changes in Weight (Millet Diet vs. Regular Rice-Based Diet)
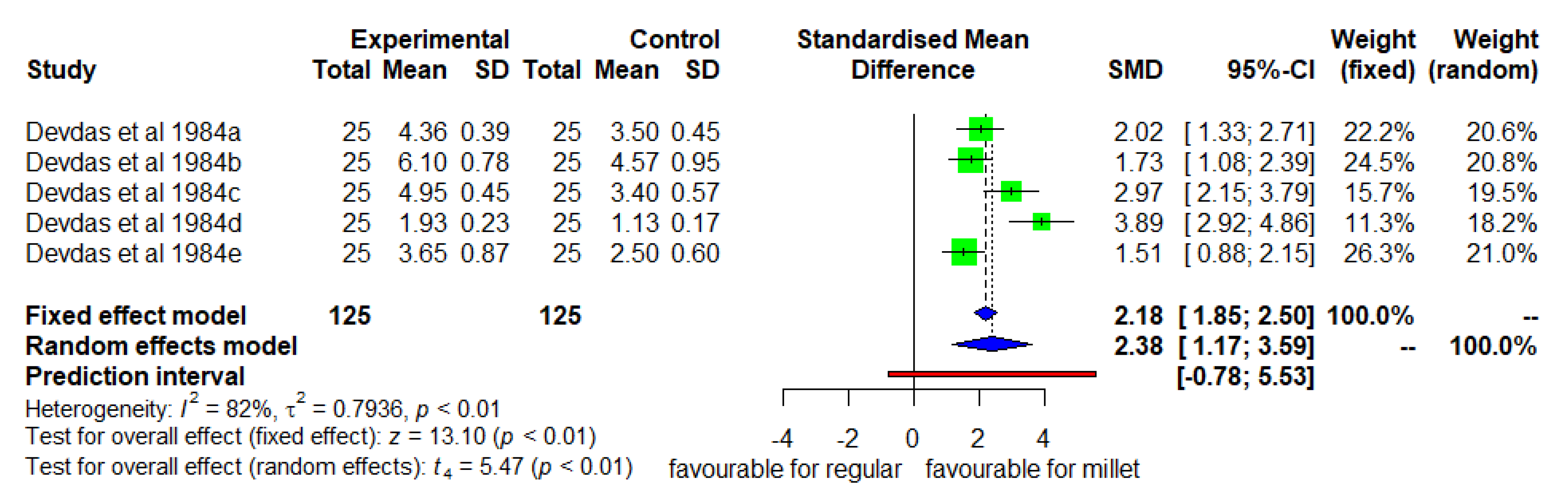
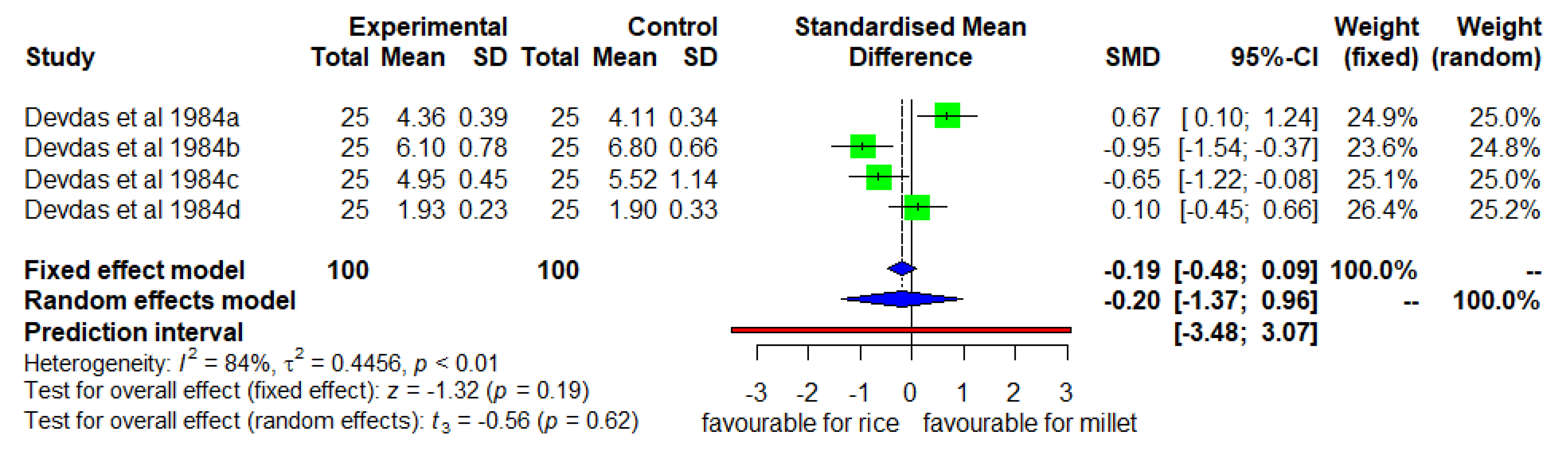
3.3. Mean Changes in MUAC (Millet Diet vs. Regular Rice Based Diet)
3.4. Mean Changes in CHEST Circumference (Millet Diet vs. Regular Rice-Based Diet)
3.5. Mean Changes in Height (Enhanced Diverse Millet Diet vs. Enhanced Diverse Rice Diet)
3.6. Mean Changes in Weight (Enhanced Diverse Millet Diet vs. Enhanced Diverse Rice Diet)
3.7. Mean Changes in MUAC (Enhanced Diverse Millet Diet vs. Enhanced Diverse Rice Diet)
3.8. Mean Changes in Chest Circumference (Enhanced Diverse Millet Diet vs. Enhanced Diverse Rice Diet)
3.9. Publication Bias and Risk of Bias
3.10. Effect of Interventions
4. Discussion
4.1. Publication Bias, Risk of Bias, and Quality of Evidence
4.2. Limitations and Future Research Recommendations
4.3. Policy Recommendations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Fact Sheets-Malnutrition–WHO. 2021. Available online: https://www.who.int›Newsroom›Factsheets›Detail (accessed on 1 July 2021).
- WHO. Fact Sheets. 2018. Available online: https://www.who.int›Newsroom›Factsheets›Detail (accessed on 1 July 2021).
- Pem, D. Factors affecting early childhood growth and development: Golden 1000 days. Adv. Pract. Nur. 2015, 1. [Google Scholar] [CrossRef]
- NHFS-5. Ministry of Health and Family Welfare. National Health Family Survey 5 (2015–2020). 2020. Available online: http://www.rchiips.org/nfhs/pdf/NFHS5/India.pdf (accessed on 3 July 2021).
- Awika, J.M. Major cereal grains production and use around the world. In Implications to Food Processing and Health Promotion, Advances in Cereal Science; Awika, J.M., Piironen, V., Bean, S., Eds.; American Chemical Society: Washington, DC, USA, 2011; pp. 1–13. [Google Scholar]
- Anitha, S.; Kane-Potaka, J.; Tsusaka, T.W.; Tripathi, D.; Upadhyay, S.; Kavishwar, A.; Jalagam, A.; Sharma, N.; Nedumaran, S. Acceptance and Impact of Millet-Based Mid-Day Meal on the Nutritional Status of Adolescent School Going Children in a Peri Urban Region of Karnataka State in India. Nutrients 2019, 11, 2077. [Google Scholar] [CrossRef] [Green Version]
- Longvah, T.; Ananthan, R.; Bhaskarachary, K.; Venkaiah, K. Indian Food Composition Table, National Institute of Nutrition; Indian Council of Medical Research: Hyderabad, India, 2017; pp. 1–578. [Google Scholar]
- Prentice, A.; Schoenmakers, I.; Laskey, M.A.; De Bono, S.; Ginty, F.; Goldberg, G.R. Symposium on ‘Nutrition and health in children and adolescents’ Session 1: Nutrition in growth and development: Nutrition and bone growth and development. Proc. Nutr. Soc. 2006, 65, 348–360. [Google Scholar] [CrossRef]
- Kumar, A.; Tomer, V.; Kaur, A.; Kumar, V.; Gupta, K. Millets: A solution to agrarian and nutritional challenges. Agric. Food Secur. 2018, 7, 31. [Google Scholar] [CrossRef]
- Poole, N.; Kane-Potaka, J. The smart food triple bottom line—Starting with diversifying staples. (Including summary of latest. smart food studies at ICRISAT). Agric. Dev. J. 2020, 41, 21–23. Available online: http://www.Ag4Dev41_Winter_2020_WEB.pdf(taa.org.uk) (accessed on 3 March 2021).
- Devdas, R.P.; Chandrasekhar, U.; Bhooma, N. Nutritional outcomes of a rural diet supplemented with low cost locally available foods—II. Impact on nursing mothers. Indian J. Nutr. Diet. 1983, 20, 71–78. [Google Scholar]
- Anitha, S.; Kane-Potaka, J.; Tsusaka, T.W.; Botha, R.; Rajendran, A.; Givens, D.I.; Parasannanavar, D.J.; Subramaniam, K.; Kanaka, P.; Mani, V.; et al. A systematic review and meta-analysis of the potential of millets and sorghum for managing and preventing diabetes mellitus. Front. Nutr. 2021. [Google Scholar] [CrossRef] [PubMed]
- Anitha, S.; Botha, R.; Kane-Potaka, J.; Givens, D.I.; Rajendran, A.; Tsusaka, T.W.; Bhandari, R. Can millet consumption help to manage hyperlipidaemia and obesity—A systematic review and meta-analysis. Front. Nutr. 2021, 8, 700778. [Google Scholar] [CrossRef]
- Anitha, S.; Kane-Potaka, J.; Botha, R.; Givens, D.I.; Binti Sulaiman, N.L.; Upadhyay, S.; Longvah, T.; Rajendran, A.; Tsusaka, T.W.; Subramaniam, K.; et al. Millets can have a major impact on improving iron status, haemoglobin level and in reducing iron deficiency anaemia—A systematic review and meta-analysis. Front. Nutr. 2021. [Google Scholar] [CrossRef] [PubMed]
- Anitha, S.; Ian Givens, D.; Botha, R.; Kane-Potaka, J.; Binti Sulaiman, N.L.; Tsusaka, T.W.; Subramaniam, K.; Rajendran, A.; Parasannanavar, D.J.; Bhandari, R.K. Calcium from finger millet—A systematic review and meta-analysis on calcium retention, and in-vitro bioavailability. Sustainability 2021, 13, 8677. [Google Scholar] [CrossRef]
- Mohar, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analysis: The PRISMA statement. Open Med. 2009, 3, 123–130. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D.D. Doing Meta-Analysis in R: A Hands-On Guide; CRC press: Raton, FL, USA, 2019; Available online: https://bookdown.org/MathiasHarrer/Doing_Meta_Analysis_in_R/ (accessed on 28 February 2021). [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, version 6.2 (updated February 2021); Cochrane: London, UK, 2021; Available online: www.training.cochrane.org/handbook (accessed on 13 April 2021).
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial? Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, A.; Fairbrother, M.; Jones, K. Fixed and random effects models: Making an informed choice. Qual. Quant. 2019, 53, 1051–1074. [Google Scholar] [CrossRef] [Green Version]
- Ahn, E.; Kang, H. Introduction to systematic review and meta-analysis. Korean J. Anaesthesiol. 2019, 71, 103–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hak, T.; Van Rhee, H.J.; Suurmond, R. How to Interpret Results of Meta-Analysis; (Version 1.3); Erasmus Rotterdam Institute of Management: Rotterdam, The Netherlands, 2016; pp. 1–2. Available online: https://www.erim.eur.nl/research-support/meta-essentials/downloads (accessed on 26 April 2021).
- Isreal, H.; Richter, R.P. A guide to understanding meta-analysis. J. Orthop. SportsPhys. Ther. 2011, 41, 496–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devdas, R.P.; Chandrasekhar, U.; Bhooma, N. Nutritional outcomes of a rural diet supplemented with low cost locally available foods—I. Impact on expectant women. Indian J. Nutr. Dietet. 1982, 19, 111–116. [Google Scholar]
- Devdas, R.P.; Chandrasekhar, U.; Bhooma, N. Nutritional outcomes of a rural diet supplemented with low cost locally available foods—III. Development and introduction of weaning foods for infants. Indian J. Nutr. Dietet. 1984, 21, 82–88. [Google Scholar]
- Devdas, R.P.; Chandrasekhar, U.; Bhooma, N. Nutritional outcomes of a rural diet supplemented with low cost locally available foods—IV. Impact on children studied from birth to pre-school age. Indian J. Nutr. Dietet. 1984, 21, 115–123. [Google Scholar]
- Devdas, R.P.; Chandrasekhar, U.; Bhooma, N. Nutritional outcomes of a rural diet supplemented with low cost locally available foods—V. Impact on pre-schoolers followed over a period of four and a half years. Indian J. Nutr. Dietet. 1984, 21, 153–164. [Google Scholar]
- Devdas, R.P.; Chandrasekhar, U.; Bhooma, N. Nutritional outcomes of a rural diet supplemented with low cost locally available foods—VI. Impact on school children. Indian J. Nutr. Dietet. 1984, 21, 187–193. [Google Scholar]
- Devdas, R.P.; Chandrasekhar, U.; Bhooma, N. Nutritional outcomes of a rural diet supplemented with low cost locally available foods—VII. Comparision of the nutritional profiles of children at different cut-off points. Indian J. Nutr. Dietet. 1984, 21, 218–224. [Google Scholar]
- Devdas, R.P.; Chandrasekhar, U.; Bhooma, N. Nutritional outcomes of a rural diet supplemented with low cost locally available foods—VIII. Impact on preschool children from a tribal community. Indian J. Nutr. Dietet. 1984, 21, 315–321. [Google Scholar]
- Durairaj, M.; Gurumurthy, G.; Nachimuthu, V.; Muniappan, K.; Balasubramanian, S. Dehulled small millets: The promising nutricereals for improving the nutrition of children. Matern. Child Nutr. 2019, 15 (Suppl. 3), e12791. [Google Scholar] [CrossRef]
- Rajendra Prasad, M.P.; Benhur, D.; Kommi, K.; Madhari, R.; Vishnuvardhan Rao, M.; Patil, J.V. Impact of sorghum supplementation on growth and micronutrient status of school going children in southern India—A randomized trial. Indian J. Pediatr. 2015, 83, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Corkins, M.R.; Daniels, S.R.; De Ferranti, S.D.; Golden, N.H.; Kim, J.H.; Magge, S.N.; Schwarzenberg, S.R. Nutrition in children and adolescents. Med. Clin. N. Am. 2016, 100, 1217–1235. [Google Scholar] [CrossRef]
- Sen, A.K. Development as Freedom; Oxford University Press: New York, NY, USA, 1999. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Keywords |
|---|---|
| 1 | Boolean logic such as “AND”, “OR”, “NOT” were used |
| 2 | Millets efficacy on child growth |
| 3 | Effect of millet supplementation on growth of the “children” OR “adolescents” OR ”pregnant women” |
| 4 | Effect of “millet” OR “finger millet” OR “pearl millet” OR “sorghum” OR “little millet” OR “barnyard millet” OR “Job’s tears” supplementation on growth of the children AND adolescent AND infant AND pregnant women |
| Author | Country | Type of Millet | Form Consumed | Study Participants | Duration | Sample Size | Parameters Studied | Study Design and Remarks |
|---|---|---|---|---|---|---|---|---|
| Devdas et al. (1982) [25] | India | Finger millet | Meal | Pregnant women | 9 months | 25 interventions (finger millet-based diet), 25 control | Weight, haemoglobin | Controlled feeding trial. This study was not included for meta-analysis as it focused on pregnant women. |
| Devdas et al. (1983) [11] | India | Finger millet | Meal | Nursing mother | 0–18 months | 25 interventions (finger millet-based diet), 25 control | Weight, haemoglobin | Controlled feeding trial. This study was not included in meta-analysis as it focused on lactating mother. |
| Devdas et al. (1984a) [26] | India | Finger millet | Finger millet malted, finger millet porridge, cooked with pulses, Idly, adai | Infants | 0–18 months | 25 interventions (finger millet-based diet), 25 control | Weight, height, chest circumference, mid upper arm circumference | Controlled feeding trial by feeding a millet-based diet to one group, enhanced rice-based diet to another group and the third group is a control which consumed a regular rice-based diet. |
| Devdas et al. (1984b) [27] | India | Finger millet | Meal | Preschool children | 0–4 years | 25 interventions (finger millet-based diet), 25 control | Weight, height, chest circumference, mid upper arm circumference | Controlled feeding trial by feeding millet-based diet to one group, enhanced rice-based diet for another group and third group is a control which was consuming a regular rice-based diet. |
| Devdas et al. (1984c) [28] | India | Finger millet | Meal | School children | 2.5 to 4.5 years | 25 interventions (finger millet-based diet), 25 control | Height, weight, chest circumference, haemoglobin, serum protein level | As described above [27] |
| Devdas et al. (1984d) [29] | India | Finger millet | Meal | School children | 6 to 7.5 years | 25 interventions (finger millet-based diet), 25 control | Height, weight, chest circumference, haemoglobin | As described above [27] |
| Devdas et al. (1984e) [30] | India | Finger millet | Meal | Preschool children | 0 to 3 years | 25 interventions (finger millet-based diet), 25 control | Weight, height, chest circumference, arm circumference, haemoglobin level | As described above [27] |
| Devdas et al. (1984f) [31] | India | Finger millet | Meal | Preschool children | 3.5 to 6.5 years | 25 interventions (finger millet-based diet), 25 control | Height, weight, chest circumference, haemoglobin | Controlled feeding trial. This was not included in meta-analysis as baseline values were missing to calculate mean difference. |
| Durairaj et al. (2018) [32] | India | Kodo, little, foxtail | health drink | Primary school children | 6 months | 30 interventions, 30 control | Height and weight | Controlled feeding trial. SD changes were calculated using t statistics provided in the paper as per Cochrance handbook. |
| Rajendra Prasad et al. (2015) [33] | India | Sorghum | Sorghum roti (flat bread), cooked with water same as rice, Khichidi/upma | School going children | 8 months | 78 interventions | Height, weight, haemoglobin, BMI | Controlled feeding trial tested a sorghum-based diet in one group (intervention) and an enhanced rice-based diet in another group (control). This study was included for weight parameters. For the height parameter, the boy’s group value was excluded as it was presented in two papers in two different ways by the same authors, which influenced the entire study. |
| Anitha et al. (2019) [6] | India | Finger millet, pearl millet, little millet | Kchichidi, ragi idly, bisibelle bath, little millet cooked with water as a rice | Adolescents | 3 months | 136 interventions, 107 control | Height for age and BMI for age | Controlled feeding trial which fed a millet-based diet to an intervention group and an enhanced rice-based diet to a control group. Height and weight values were obtained from the authors. |
| Food Items (g/day) | Enhanced Finger Millet Based Diet | Enhanced Rice Based Diet | Control Diet (Regular Rice Based Diet) |
|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | |
| Millet/rice (g) | 245 ± 20.4 | 228.3 ± 26.3 | 168.7 ± 26.2 |
| Pulses (g) | 100 ± 8.6 | 115.3 ± 5.0 | 27.0 ± 11.2 |
| Milk & milk products (g) | 54.2 ± 6.7 | 54.0 ± 9.6 | 34.0 ± 6.4 |
| Roots and tubers (g) | 96.7 ± 25.7 | 113 ± 37.2 | 57.2 ± 9.3 |
| Green leafy vegetables (g) | 39.2 ± 6.1 | 47.6 ± 4.9 | 16.2 ± 4.7 |
| Oils and fats (g) | 8.5 ± 1.7 | 8.6 ± 2.3 | 6.5 ± 1.0 |
| Sugar (g) | 10 ± 0.0 | 10.6 ± 1.2 | 6.5 ± 1.7 |
| Nuts (g) | 51.9 ± 2.1 | 53.0 ± 5.6 | - |
| Fruits (g) | 8.7 ± 0.5 | 9 ± 0.0 | 5.3 ± 0.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anitha, S.; Givens, D.I.; Subramaniam, K.; Upadhyay, S.; Kane-Potaka, J.; Vogtschmidt, Y.D.; Botha, R.; Tsusaka, T.W.; Nedumaran, S.; Rajkumar, H.; et al. Can Feeding a Millet-Based Diet Improve the Growth of Children?—A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 225. https://doi.org/10.3390/nu14010225
Anitha S, Givens DI, Subramaniam K, Upadhyay S, Kane-Potaka J, Vogtschmidt YD, Botha R, Tsusaka TW, Nedumaran S, Rajkumar H, et al. Can Feeding a Millet-Based Diet Improve the Growth of Children?—A Systematic Review and Meta-Analysis. Nutrients. 2022; 14(1):225. https://doi.org/10.3390/nu14010225
Chicago/Turabian StyleAnitha, Seetha, David Ian Givens, Kowsalya Subramaniam, Shweta Upadhyay, Joanna Kane-Potaka, Yakima D. Vogtschmidt, Rosemary Botha, Takuji W. Tsusaka, Swamikannu Nedumaran, Hemalatha Rajkumar, and et al. 2022. "Can Feeding a Millet-Based Diet Improve the Growth of Children?—A Systematic Review and Meta-Analysis" Nutrients 14, no. 1: 225. https://doi.org/10.3390/nu14010225
APA StyleAnitha, S., Givens, D. I., Subramaniam, K., Upadhyay, S., Kane-Potaka, J., Vogtschmidt, Y. D., Botha, R., Tsusaka, T. W., Nedumaran, S., Rajkumar, H., Rajendran, A., Parasannanavar, D. J., Vetriventhan, M., & Bhandari, R. K. (2022). Can Feeding a Millet-Based Diet Improve the Growth of Children?—A Systematic Review and Meta-Analysis. Nutrients, 14(1), 225. https://doi.org/10.3390/nu14010225