
The Impact of Bisphenol A on Thyroid Function in Neonates and Children: A Systematic Review of the Literature

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Eligibility Criteria
2.3. Literature Search
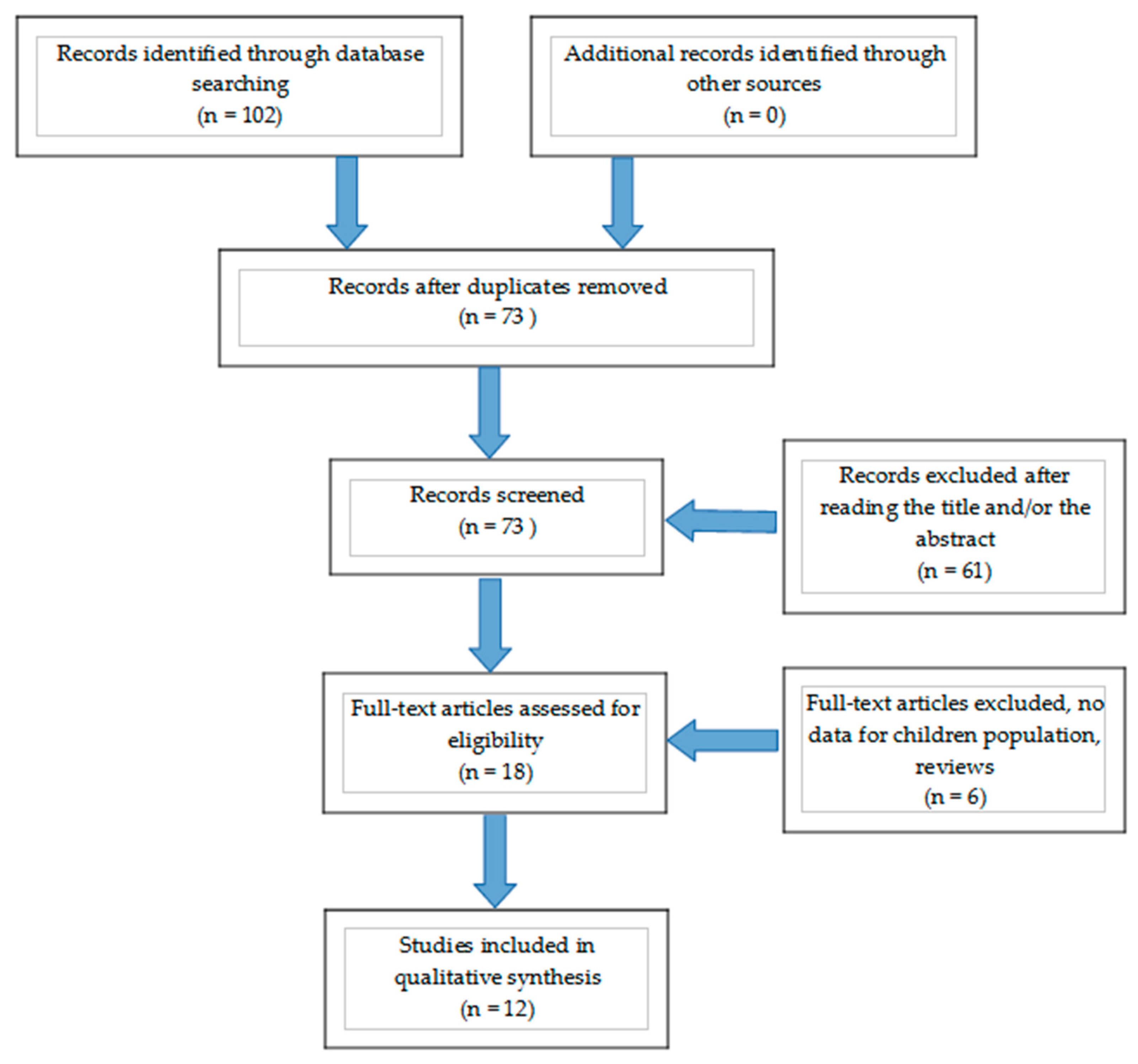
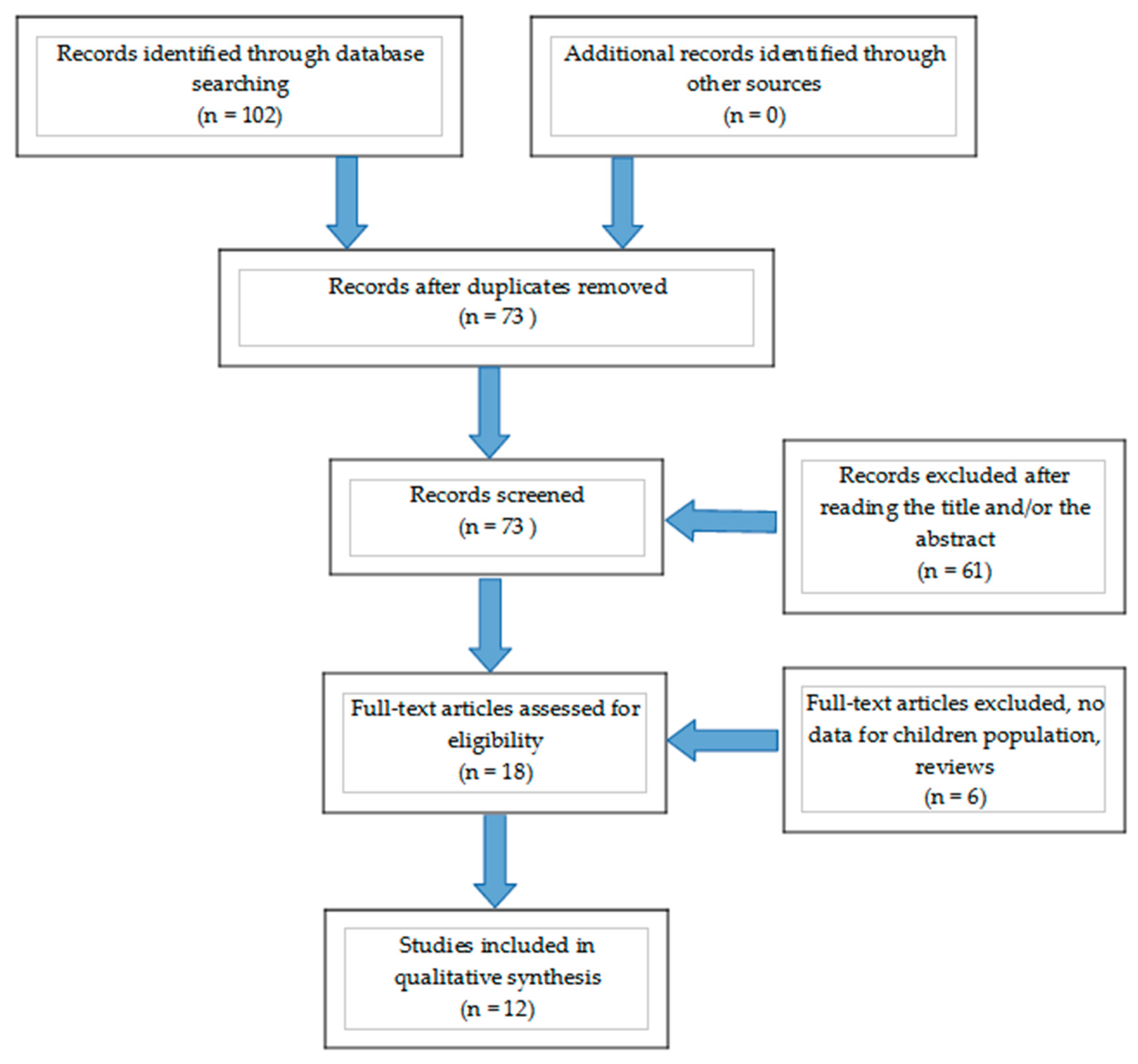
2.4. Study Selection
2.5. Data Extraction
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Diamanti-Kandarakis, E.; Bourguignon, J.-P.; Giudice, L.C.; Hauser, R.; Prins, G.S.; Soto, A.M.; Zoeller, R.T.; Gore, A.C. Endocrine-disrupting chemicals: An Endocrine Society scientific statement. Endocr. Rev. 2009, 30, 293–342. [Google Scholar] [CrossRef]
- Solecki, R.; Kortenkamp, A.; Bergman, Å.; Chahoud, I.; Degen, G.H.; Dietrich, D.; Greim, H.; Håkansson, H.; Hass, U.; Husoy, T.; et al. Scientific principles for the identification of endocrine-disrupting chemicals: A consensus statement. Arch. Toxicol. 2017, 91, 1001–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, J.-H.; Kondo, F.; Katayama, Y. Human exposure to bisphenol A. Toxicology 2006, 226, 79–89. [Google Scholar] [CrossRef]
- Ali, M.; Jaghbir, M.; Salam, M.; Al-Kadamany, G.; Damsees, R.; Al-Rawashdeh, N. Testing baby bottles for the presence of residual and migrated bisphenol A. Environ. Monit. Assess. 2018, 191, 7. [Google Scholar] [CrossRef] [PubMed]
- Michałowicz, J. Bisphenol A-sources, toxicity and biotransformation. Environ. Toxicol. Pharmacol. 2014, 37, 738–758. [Google Scholar] [CrossRef]
- Frankowski, R.; Zgoła-Grześkowiak, A.; Grześkowiak, T.; Sójka, K. The presence of bisphenol A in the thermal paper in the face of changing European regulations—A comparative global research. Environ. Pollut. 2020, 265, 114879. [Google Scholar] [CrossRef] [PubMed]
- Rudel, R.A.; Brody, J.G.; Spengler, J.D.; Vallarino, J.; Geno, P.W.; Sun, G.; Yau, A. Identification of selected hormonally active agents and animal mammary carcinogens in commercial and residential air and dust samples. J. Air Waste Manag. Assoc. 2001, 51, 499–513. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.; Wang, H.; Zhou, W.; He, Y.; Zhou, Y.; Chen, Y.; Jiang, Q. Exposure to bisphenol A among school children in eastern China: A multicenter cross-sectional study. J. Expo. Sci. Environ. Epidemiol. 2014, 24, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Calafat, A.M.; Ye, X.; Wong, L.-Y.; Reidy, J.A.; Needham, L.L. Exposure of the U.S. Population to Bisphenol A and 4-tertiary-Octylphenol: 2003–2004. Environ. Health Perspect. 2008, 116, 39–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manzan-Martins, C.; Paulesu, L. Impact of bisphenol A (BPA) on cells and tissues at the human materno-fetal interface. Tissue Cell 2021, 73, 101662. [Google Scholar] [CrossRef] [PubMed]
- Braun, J.M.; Kalkbrenner, A.E.; Calafat, A.M.; Yolton, K.; Ye, X.; Dietrich, K.N.; Lanphear, B.P. Impact of Early-Life Bisphenol A Exposure on Behavior and Executive Function in Children. Pediatrics 2011, 128, 873–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trasande, L.; Attina, T.M.; Blustein, J. Association between Urinary Bisphenol A Concentration and Obesity Prevalence in Children and Adolescents. JAMA 2012, 308, 1113–1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pergialiotis, V.; Kotrogianni, P.; Christopoulos-Timogiannakis, E.; Koutaki, D.; Daskalakis, G.; Papantoniou, N. Bisphenol A and adverse pregnancy outcomes: A systematic review of the literature. J. Matern. Fetal Neonatal Med. 2018, 31, 3320–3327. [Google Scholar] [CrossRef] [PubMed]
- Rochester, J.R. Bisphenol A and human health: A review of the literature. Reprod. Toxicol. 2013, 42, 132–155. [Google Scholar] [CrossRef]
- Wetherill, Y.B.; Akingbemi, B.T.; Kanno, J.; McLachlan, J.A.; Nadal, A.; Sonnenschein, C.; Watson, C.S.; Zoeller, R.T.; Belcher, S.M. In vitro molecular mechanisms of bisphenol A action. Reprod. Toxicol. 2007, 101, 59–67. [Google Scholar] [CrossRef] [PubMed]
- MacKay, H.; Abizaid, A. A plurality of molecular targets: The receptor ecosystem for bisphenol-A (BPA). Horm. Behav. 2018, 101, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Cimmino, I.; Fiory, F.; Perruolo, G.; Miele, C.; Beguinot, F.; Formisano, P. Potential Mechanisms of Bisphenol A (BPA) Contributing to Human Disease. Int. J. Mol. Sci. 2020, 21, 5761. [Google Scholar] [CrossRef]
- Pennie, W.D.; Aldridge, T.C.; Brooks, A.N. Differential activation by xenoestrogens of ER alpha and ER beta when linked to different response elements. J. Endocrinol. 1998, 158, 11–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takayanagi, S.; Tokunaga, T.; Liu, X.; Okada, H.; Matsushima, A.; Shimohigashi, Y. Endocrine disruptor bisphenol A strongly binds to human estrogen-related receptor gamma (ERRgamma) with high constitutive activity. Toxicol. Lett. 2006, 167, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Kuiper, G.G.; Lemmen, J.G.; Carlsson, B.O.; Corton, J.C.; Safe, S.H.; Van Der Saag, P.T.; Van Der Burg, B.; Gustafsson, J.A. Interaction of estrogenic chemicals and phytoestrogens with estrogen receptor beta. Endocrinology 1998, 139, 4252–4263. [Google Scholar] [CrossRef]
- Lee, H.J.; Chattopadhyay, S.; Gong, E.-Y.; Ahn, R.S.; Lee, K. Antiandrogenic effects of bisphenol A and nonylphenol on the function of androgen receptor. Toxicol. Sci. 2003, 75, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Richter, C.A.; Taylor, J.A.; Ruhlen, R.L.; Welshons, W.V.; vom Saal, F.S. Estradiol and Bisphenol A Stimulate Androgen Receptor and Estrogen Receptor Gene Expression in Fetal Mouse Prostate Mesenchyme Cells. Environ. Health Perspect. 2007, 115, 902–908. [Google Scholar] [CrossRef]
- Prasanth, G.K.; Divya, L.M.; Sadasivan, C. Bisphenol-A can bind to human glucocorticoid receptor as an agonist: An in silico study. J. Appl. Toxicol. 2010, 30, 769–774. [Google Scholar] [CrossRef]
- Atlas, E.; Pope, L.; Wade, M.G.; Kawata, A.; Boudreau, A.; Boucher, J.G. Bisphenol A increases aP2 expression in 3T3L1 by enhancing the transcriptional activity of nuclear receptors at the promoter. Adipocyte 2014, 3, 170–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biasiotto, G.; Zanella, I.; Masserdotti, A.; Pedrazzani, R.; Papa, M.; Caimi, L.; Di Lorenzo, D. Municipal wastewater affects adipose deposition in male mice and increases 3T3-L1 cell differentiation. Toxicol. Appl. Pharmacol. 2016, 297, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Singleton, D.W.; Feng, Y.; Yang, J.; Puga, A.; Lee, A.V.; Khan, S.A. Gene expression profiling reveals novel regulation by bisphenol-A in estrogen receptor-alpha-positive human cells. Environ. Res. 2006, 100, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Klinge, C.M. Estrogen Regulation of MicroRNA Expression. Curr. Genom. 2009, 10, 169–183. [Google Scholar] [CrossRef] [Green Version]
- Doherty, L.F.; Bromer, J.G.; Zhou, Y.; Aldad, T.S.; Taylor, H.S. In utero exposure to diethylstilbestrol (DES) or bisphenol-A (BPA) increases EZH2 expression in the mammary gland: An epigenetic mechanism linking endocrine disruptors to breast cancer. Horm. Cancer 2010, 1, 146–155. [Google Scholar] [CrossRef] [Green Version]
- Bromer, J.G.; Zhou, Y.; Taylor, M.B.; Doherty, L.; Taylor, H.S. Bisphenol-A exposure in utero leads to epigenetic alterations in the developmental programming of uterine estrogen response. FASEB J. 2010, 24, 2273–2280. [Google Scholar] [CrossRef] [Green Version]
- Moriyama, K.; Tagami, T.; Akamizu, T.; Usui, T.; Saijo, M.; Kanamoto, N.; Hataya, Y.; Shimatsu, A.; Kuzuya, H.; Nakao, K. Thyroid hormone action is disrupted by bisphenol A as an antagonist. J. Clin. Endocrinol. Metab. 2002, 87, 5185–5190. [Google Scholar] [CrossRef]
- Zoeller, R.T. Environmental chemicals as thyroid hormone analogues: New studies indicate that thyroid hormone receptors are targets of industrial chemicals? Mol. Cell. Endocrinol. 2005, 242, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Heimeier, R.A.; Das, B.; Buchholz, D.R.; Shi, Y.-B. The xenoestrogen bisphenol A inhibits postembryonic vertebrate development by antagonizing gene regulation by thyroid hormone. Endocrinology 2009, 150, 2964–2973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, H.; Shen, O.-X.; Wang, X.-R.; Zhou, L.; Zhen, S.-Q.; Chen, X.-D. Anti-thyroid hormone activity of bisphenol A, tetrabromobisphenol A and tetrachlorobisphenol A in an improved reporter gene assay. Toxicol. Vitro 2009, 23, 950–954. [Google Scholar] [CrossRef]
- Kudo, Y.; Yamauchi, K.; Fukazawa, H.; Terao, Y. In vitro and in vivo analysis of the thyroid system-disrupting activities of brominated phenolic and phenol compounds in Xenopus laevis. Toxicol. Sci. 2006, 92, 87–95. [Google Scholar] [CrossRef] [Green Version]
- Terasaki, M.; Kosaka, K.; Kunikane, S.; Makino, M.; Shiraishi, F. Assessment of thyroid hormone activity of halogenated bisphenol A using a yeast two-hybrid assay. Chemosphere 2011, 84, 1527–1530. [Google Scholar] [CrossRef]
- Sheng, Z.G.; Tang, Y.; Liu, Y.X.; Yuan, Y.; Zhao, B.Q.; Chao, X.J.; Zhu, B.Z. Low concentrations of bisphenol a suppress thyroid hormone receptor transcription through a nongenomic mechanism. Toxicol. Appl. Pharmacol. 2012, 259, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Guo, L.-H.; Wan, B.; Wei, Y. In vitro fluorescence displacement investigation of thyroxine transport disruption by bisphenol A. J. Environ. Sci. China 2011, 23, 315–321. [Google Scholar] [CrossRef]
- Yang, J.; Chan, K.M. Evaluation of the toxic effects of brominated compounds (BDE-47, 99, 209, TBBPA) and bisphenol A (BPA) using a zebrafish liver cell line, ZFL. Aquat. Toxicol. 2015, 159, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Beland, F.A.; Fang, J.-L. Effect of triclosan, triclocarban, 2,2′,4,4′-tetrabromodiphenyl ether, and bisphenol A on the iodide uptake, thyroid peroxidase activity, and expression of genes involved in thyroid hormone synthesis. Toxicol. Vitro 2016, 32, 310–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gentilcore, D.; Porreca, I.; Rizzo, F.; Ganbaatar, E.; Carchia, E.; Mallardo, M.; De Felice, M.; Ambrosino, C. Bisphenol A interferes with thyroid specific gene expression. Toxicology 2013, 304, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Kim, C.; Youn, H.; Choi, K. Thyroid hormone disrupting potentials of bisphenol A and its analogues—in vitro comparison study employing rat pituitary (GH3) and thyroid follicular (FRTL-5) cells. Toxicol. Vitro 2017, 40, 297–304. [Google Scholar] [CrossRef]
- Meeker, J.D.; Ferguson, K.K. Relationship between Urinary Phthalate and Bisphenol A Concentrations and Serum Thyroid Measures in U.S. Adults and Adolescents from the National Health and Nutrition Examination Survey (NHANES) 2007–2008. Environ. Health Perspect. 2011, 119, 1396–1402. [Google Scholar] [CrossRef]
- Batistuzzo, A.; Ribeiro, M.O. Clinical and subclinical maternal hypothyroidism and their effects on neurodevelopment, behavior and cognition. Arch. Endocrinol. Metab. 2020, 64, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Balakrishnan, B.; Henare, K.; Thorstensen, E.B.; Ponnampalam, A.P.; Mitchell, M.D. Transfer of bisphenol A across the human placenta. Am. J. Obstet. Gynecol. 2010, 202, 393.e1–393.e7. [Google Scholar] [CrossRef]
- Pop, V.J.; Brouwers, E.P.; Vader, H.L.; Vulsma, T.; van Baar, A.L.; de Vijlder, J.J. Maternal hypothyroxinaemia during early pregnancy and subsequent child development: A 3-year follow-up study. Clin. Endocrinol. 2003, 59, 282–288. [Google Scholar] [CrossRef] [Green Version]
- Berbel, P.; Mestre, J.L.; Santamaria, A.; Palazón, I.; Franco, A.; Graells, M.; González-Torga, A.; de Escobar, G.M. Delayed neurobehavioral development in children born to pregnant women with mild hypothyroxinemia during the first month of gestation: The importance of early iodine supplementation. Thyroid 2009, 19, 511–519. [Google Scholar] [CrossRef]
- Heindel, J.J.; Vandenberg, L.N. Developmental Origins of Health and Disease: A Paradigm for Understanding Disease Etiology and Prevention. Curr. Opin. Pediatr. 2015, 27, 248–253. [Google Scholar] [CrossRef] [Green Version]
- Wolstenholme, J.T.; Edwards, M.; Shetty, S.R.; Gatewood, J.D.; Taylor, J.A.; Rissman, E.F.; Connelly, J.J. Gestational exposure to bisphenol a produces transgenerational changes in behaviors and gene expression. Endocrinology 2012, 153, 3828–3838. [Google Scholar] [CrossRef] [Green Version]
- Manikkam, M.; Tracey, R.; Guerrero-Bosagna, C.; Skinner, M.K. Plastics derived endocrine disruptors (BPA, DEHP and DBP) induce epigenetic transgenerational inheritance of obesity, reproductive disease and sperm epimutations. PLoS ONE 2013, 8, e55387. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [Green Version]
- Chevrier, J.; Gunier, R.B.; Bradman, A.; Holland, N.T.; Calafat, A.M.; Eskenazi, B.; Harley, K.G. Maternal urinary bisphenol a during pregnancy and maternal and neonatal thyroid function in the CHAMACOS study. Environ. Health Perspect. 2013, 121, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Romano, M.E.; Webster, G.M.; Vuong, A.M.; Zoeller, R.T.; Chen, A.; Hoofnagle, A.N.; Calafat, A.M.; Karagas, M.R.; Yolton, K.; Lanphear, B.P.; et al. Gestational urinary bisphenol A and maternal and newborn thyroid hormone concentrations: The HOME Study. Environ. Res. 2015, 138, 453–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brucker-Davis, F.; Ferrari, P.; Boda-Buccino, M.; Wagner-Mahler, K.; Pacini, P.; Gal, J.; Azuar, P.; Fenichel, P. Cord blood thyroid tests in boys born with and without cryptorchidism: Correlations with birth parameters and in utero xenobiotics exposure. Thyroid 2011, 21, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Yang, F.; Li, D.K.; Tian, Y.; Miao, M.; Zhang, Y.; Ji, H.; Yuan, W.; Liang, H. Prenatal bisphenol A exposure, fetal thyroid hormones and neurobehavioral development in children at 2 and 4 years: A prospective cohort study. Sci. Total Environ. 2020, 722, 137887. [Google Scholar] [CrossRef]
- Guo, J.; Wu, C.; Zhang, J.; Li, W.; Lv, S.; Lu, D.; Qi, X.; Feng, C.; Liang, W.; Chang, X.; et al. Maternal and childhood urinary phenol concentrations, neonatal thyroid function, and behavioral problems at 10 years of age: The SMBCS study. Sci. Total Environ. 2020, 743, 140678. [Google Scholar] [CrossRef] [PubMed]
- Minatoya, M.; Sasaki, S.; Araki, A.; Miyashita, C.; Itoh, S.; Yamamoto, J.; Matsumura, T.; Mitsui, T.; Moriya, K.; Cho, K.; et al. Cord Blood Bisphenol A Levels and Reproductive and Thyroid Hormone Levels of Neonates: The Hokkaido Study on Environment and Children’s Health. Epidemiology 2017, 28, S3–S9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Tang, N.; Nakayama, S.F.; Fan, P.; Liu, Z.; Zhang, J.; Ouyang, F. Maternal urinary bisphenol A concentration and thyroid hormone levels of Chinese mothers and newborns by maternal body mass index. Environ. Sci. Pollut. Res. Int. 2020, 27, 10939–10949. [Google Scholar] [CrossRef]
- Sanlidag, B.; Dalkan, C.; Yetkin, O.; Bahçeciler, N.N. Evaluation of Dose Dependent Maternal Exposure to Bisphenol A on Thyroid Functions in Newborns. J. Clin. Med. 2018, 7, 119. [Google Scholar] [CrossRef] [Green Version]
- Jang, Y.; Choi, Y.J.; Lim, Y.H.; Lee, K.S.; Kim, B.N.; Shin, C.H.; Lee, Y.A.; Kim, J.I.; Hong, Y.C. Associations Between Thyroid Hormone Levels and Urinary Concentrations of Bisphenol A, F, and S in 6-Year-old Children in Korea. J. Prev. Med. Public Health 2021, 54, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Derakhshan, A.; Philips, E.M.; Ghassabian, A.; Santos, S.; Asimakopoulos, A.G.; Kannan, K.; Kortenkamp, A.; Jaddoe, V.W.; Trasande, L.; Peeters, R.P.; et al. Association of urinary bisphenols during pregnancy with maternal, cord blood and childhood thyroid function. Environ. Int. 2021, 146, 106160. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Zhou, Y.; Fu, C.; Wang, H.; Huang, P.; Wang, B.; Su, M.; Jiang, F.; Fang, H.; Zhao, Q.; et al. Influence of Bisphenol A on Thyroid Volume and Structure Independent of Iodine in School Children. PLoS ONE 2015, 10, e0141248. [Google Scholar] [CrossRef] [Green Version]
- Sur, U.; Erkekoglu, P.; Bulus, A.D.; Andiran, N.; Kocer-Gumusel, B. Oxidative stress markers, trace elements, and endocrine disrupting chemicals in children with Hashimoto’s thyroiditis. Toxicol. Mech. Methods. 2019, 29, 633–643. [Google Scholar] [CrossRef]
- Vandenberg, L.N.; Hauser, R.; Marcus, M.; Olea, N.; Welshons, W.V. Human exposure to bisphenol A (BPA). Reprod. Toxicol. 2007, 24, 139–177. [Google Scholar] [CrossRef] [PubMed]
- Yuan, N.; Wang, L.; Zhang, X.; Li, W. Bisphenol A and thyroid hormones: Bibliometric analysis of scientific publications. Medicine 2020, 99, e23067. [Google Scholar] [CrossRef]
- Wang, T.; Lu, J.; Xu, M.; Xu, Y.; Li, M.; Liu, Y.; Tian, X.; Chen, Y.; Dai, M.; Wang, W.; et al. Urinary bisphenol a concentration and thyroid function in Chinese adults. Epidemiology 2013, 24, 295–302. [Google Scholar] [CrossRef]
- Aung, M.T.; Johns, L.E.; Ferguson, K.K.; Mukherjee, B.; McElrath, T.F.; Meeker, J.D. Thyroid hormone parameters during pregnancy in relation to urinary bisphenol A concentrations: A repeated measures study. Environ. Int. 2017, 104, 33–40. [Google Scholar] [CrossRef]
- Kaneko, M.; Okada, R.; Yamamoto, K.; Nakamura, M.; Mosconi, G.; Polzonetti-Magni, A.M.; Kikuyama, S. Bisphenol A acts differently from and independently of thyroid hormone in suppressing thyrotropin release from the bullfrog pituitary. Gen. Comp. Endocrinol. 2008, 155, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Pirahanchi, Y.; Tariq, M.A.; Jialal, I. Physiology, Thyroid. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: http://www.ncbi.nlm.nih.gov/books/NBK519566/ (accessed on 31 October 2021).
- Kratzsch, J.; Pulzer, F. Thyroid gland development and defects. Best Pract. Res. Clin. Endocrinol. Metab. 2008, 22, 57–75. [Google Scholar] [CrossRef] [PubMed]
- Kauschansky, A.; Genel, M.; Smith, G.J. Congenital hypopituitarism in female infants: Its association with hypoglycemia and hypothyroidism. Am. J. Dis. Child 1960, 133, 165–169. [Google Scholar] [CrossRef]
- Zoeller, R.T.; Bansal, R.; Parris, C. Bisphenol-A, an environmental contaminant that acts as a thyroid hormone receptor antagonist in vitro, increases serum thyroxine, and alters RC3/neurogranin expression in the developing rat brain. Endocrinology 2005, 146, 607–612. [Google Scholar] [CrossRef]
- Xu, X.; Liu, Y.; Sadamatsu, M.E.; Tsutsumi, S.; Akaike, M.; Ushijima, H.; Kato, N. Perinatal bisphenol A affects the behavior and SRC-1 expression of male pups but does not influence on the thyroid hormone receptors and its responsive gene. Neurosci. Res. 2007, 58, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Vyas, A.K.; Veiga-Lopez, A.; Ye, W.; Abi Salloum, B.; Abbott, D.H.; Yang, S.; Liao, C.; Kannan, K.; Padmanabhan, V. Developmental programming: Sex-specific programming of growth upon prenatal bisphenol A exposure. J. Appl. Toxicol. 2019, 39, 1516–1531. [Google Scholar] [CrossRef]
- Ikezuki, Y.; Tsutsumi, O.; Takai, Y.; Kamei, Y.; Taketani, Y. Determination of bisphenol A concentrations in human biological fluids reveals significant early prenatal exposure. Hum. Reprod. 2002, 17, 2839–2841. [Google Scholar] [CrossRef] [Green Version]
- Pop, V.J.; Kuijpens, J.L.; van Baar, A.L.; Verkerk, G.; van Son, M.M.; de Vijlder, J.J.; Vulsma, T.; Wiersinga, W.M.; Drexhage, H.A.; Vader, H.L. Low maternal free thyroxine concentrations during early pregnancy are associated with impaired psychomotor development in infancy. Clin. Endocrinol. 1999, 50, 149–155. [Google Scholar] [CrossRef] [Green Version]
- Coughtrie, M.W.; Burchell, B.; Leakey, J.E.; Hume, R. The inadequacy of perinatal glucuronidation: Immunoblot analysis of the developmental expression of individual UDP-glucuronosyltransferase isoenzymes in rat and human liver microsomes. Mol. Pharmacol. 1988, 34, 729–735. [Google Scholar]
- Eng, L.; Lam, L. Thyroid Function during the Fetal and Neonatal Periods. NeoReviews 2020, 21, e30–e36. [Google Scholar] [CrossRef]
- Shapira, Y.; Agmon-Levin, N.; Shoenfeld, Y. Defining and analyzing geoepidemiology and human autoimmunity. J. Autoimmun. 2010, 34, J168–J177. [Google Scholar] [CrossRef]
- Kharrazian, D. The Potential Roles of Bisphenol A (BPA) Pathogenesis in Autoimmunity. Autoimmune Dis. 2014, 2014, 743616. [Google Scholar] [CrossRef] [Green Version]
- Midoro-Horiuti, T.; Tiwari, R.; Watson, C.S.; Goldblum, R.M. Maternal Bisphenol A Exposure Promotes the Development of Experimental Asthma in Mouse Pups. Environ. Health Perspect. 2010, 118, 273–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanley, P.; Lord, K.; Bauer, A.J. Thyroid Disorders in Children and Adolescents: A Review. JAMA Pediatr. 2016, 170, 1008–1019. [Google Scholar] [CrossRef] [PubMed]
- Chailurkit, L.; Aekplakorn, W.; Ongphiphadhanakul, B. The Association of Serum Bisphenol A with Thyroid Autoimmunity. Int. J. Environ. Res. Public Health 2016, 13, 1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ejaredar, M.; Lee, Y.; Roberts, D.J.; Sauve, R.; Dewey, D. Bisphenol A exposure and children’s behavior: A systematic review. J. Expo. Sci. Environ. Epidemiol. 2017, 27, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Seiwa, C.; Nakahara, J.; Komiyama, T.; Katsu, Y.; Iguchi, T.; Asou, H. Bisphenol A exerts thyroid-hormone-like effects on mouse oligodendrocyte precursor cells. Neuroendocrinology 2004, 80, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Xie, L.; Hong, X.; Ruan, Q.; Lu, H.; Zhang, Q.; Zhang, G.; Liu, X. Perinatal exposure to bisphenol-A inhibits synaptogenesis and affects the synaptic morphological development in offspring male mice. Chemosphere 2013, 91, 1073–1081. [Google Scholar] [CrossRef]
- Niu, Y.; Zhu, M.; Dong, M.; Li, J.; Li, Y.; Xiong, Y.; Liu, P.; Qin, Z. Bisphenols disrupt thyroid hormone (TH) signaling in the brain and affect TH-dependent brain development in Xenopus laevis. Aquat. Toxicol 2021, 237, 105902. [Google Scholar] [CrossRef]
- Grohs, M.N.; Reynolds, J.E.; Liu, J.; Martin, J.W.; Pollock, T.; Lebel, C.; Dewey, D. Prenatal maternal and childhood bisphenol a exposure and brain structure and behavior of young children. Environ. Health 2019, 18, 85. [Google Scholar] [CrossRef] [Green Version]
- Walker, D.M.; Gore, A.C. Transgenerational neuroendocrine disruption of reproduction. Nat. Rev. Endocrinol. 2011, 7, 197–207. [Google Scholar] [CrossRef]
- Levie, D.; Korevaar, T.I.; Bath, S.C.; Dalmau-Bueno, A.; Murcia, M.; Espada, M.; Dineva, M.; Ibarluzea, J.M.; Sunyer, J.; Tiemeier, H.; et al. Thyroid Function in Early Pregnancy, Child IQ, and Autistic Traits: A Meta-Analysis of Individual Participant Data. J. Clin. Endocrinol. Metab. 2018, 103, 2967–2979. [Google Scholar] [CrossRef]
- Pottenger, L.H.; Domoradzki, J.Y.; Markham, D.A.; Hansen, S.C.; Cagen, S.Z.; Waechter, J.M. The relative bioavailability and metabolism of bisphenol A in rats is dependent upon the route of administration. Toxicol. Sci. 2000, 54, 3–18. [Google Scholar] [CrossRef]

{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Authors | Number of Children | Method of BPA Measurement | BPA Sample | TSH Sample | Study Characteristics | Time of BPA Measurement |
|---|---|---|---|---|---|---|
| Brucker-Davis et al. (2011) [53] | 53 (only boys) | Chromatography coupled with mass spectrometry | Cord blood | Cord blood | Prospective–Cohort | At birth |
| Chevrier et al. (2013) [51] | 364 | Online solid-phase extraction coupled with isotope dilution–high-performance liquid chromatography–negative ion–atmospheric pressure chemical ionization tandem mass spectrometry | Urine | Blood spots | Cohort | 12.4 ± 3.8 and 26.2 ± 2.2 weeks of gestation |
| Romano et al. (2015) [52] | 249 | Online solid-phase extraction coupled to high-performance liquid chromatography-isotope dilution tandem mass spectrometry | Urine | Cord blood | Prospective | 16 (13.0–20.9) and 26 (23.1–34.6) weeks of gestation |
| Wang et al. (2015) [61] | 718 | Ultra-performance liquid chromatography coupled with tandem mass spectrometry | Urine | Cross sectional | 9–11 years old | |
| Minatoya et al. (2017) [56] | 283 | Isotope dilution liquid chromatography-tandem mass spectrometry (ID-LC/MS/MS) | Cord blood | Heel-prick blood sample | Prospective–Cohort | At birth |
| Sanlidag et al. (2018) [58] | 88 | Sandwich enzyme—linked Immunosorbent assays (ELISAs) | Cord blood | Cord blood | Cross-sectional | At birth |
| Sur et al. (2019) [62] | 29 and 29 control group | High-pressure liquid chromatography (HPLC) | Urine | Case-control | 8–16 years old | |
| Wang et al. (2020) [57] | 398 | Liquid chromatography tandem mass spectrometry (HPLC-MS/MS) | Urine | Cord blood | Cohort | Late pregnancy (38.8 ± 1.1 weeks of gestation) |
| Fen Li et al. (2020) [54] | 348 | High-performance liquid chromatography (HPLC) | Urine | Cord blood | Prospective | 12–16 weeks of gestation |
| Guo et al. (2020) [55] | 386 | Gas chromatography tandem mass spectrometry | Urine | Cord blood | Prospective-Cohort | At birth |
| Derakhshan et al. (2020) [60] | 853 neonates | Liquid–liquid extraction (LLE) followed by enzymatic deconjugation of the glucuronidated bisphenols accompanied by high performance liquid chromatography electrospray ionization-tandem mass spectrometry (HPLC-ESI-MS/MS) | Urine | Cord blood | Prospective | <18, 18–25, >25 weeks of gestation |
| 882 children | Urine | Serum | ||||
| Jang et al., 2021 [59] | 574 | High-performance liquid chromatography-tandem mass spectrometry | Urine | Blood sample | Prospective–Cohort | 20 weeks of gestation and 6 years old children |
| Authors | TSH | T3 | T4 | BPA | Other |
|---|---|---|---|---|---|
| Brucker-Davis et al. (2011) [53] | Mean: 7.67 mIU/L (SD: 5.04) R = −0.25, p = 0.077 ↓ | Mean: FT3 = 2.04 pmol/L (SD: 0.44) (-) | Mean: FT4 = 13.04 (pmol/L) (SD: 1.54) (-) | Median: 0.9 ng/mL (Range: 0.2–3.3) | |
| Chevrier et al. (2013) [51] | GM: 5.6 mIU/L (GSD:1.8) ↓ (boys) | Median: 1.2 mg/g creatinine (IQR: 0.8–1.9) | |||
| Romano et al. (2015) [52] | Mean: 7.2 mIU/L (95%CI: 6.7, 7.8) ↓ (girls) | Mean ± SD FT3 = 1.7 ± 0.3 pg/mL TT3 = 52 ± 19 ng/dL ↑ | Mean ± SD FT4 = 1.0 ± 0.2 ng/dL TT4 = 9.6 ± 1.8 mg/dL (-) | Median BPA (mg/g Cr) = 2.2 (IQR:1.5–3.4) | |
| Wang et al. (2015) [61] | Median: 2.45 (IQR: 1.09–5.97) μg/g creatinine | Median thyroid volume: 3.14 mL (IQR: 2.44–4.11) | |||
| Minatoya et al. (2017) [56] | Median Boys (127): 2.2 (IQR: 1.2–4.0) Median Girls (156): 2.2 (IQR1.4–3.9) (μU/mL) (-) | Median Boys (127): FT4 = 2.0 (IQR: 1.9–2.3) (ng/dl) Median Girls (156): FT4 = 2.0 (IQR: 1.8–2.3) (ng/dl) (-) | Mean ± SD: 0.057 ± 0.036 ng/ml | ||
| Sanlidag et al. (2018) [58] | Mean ± SD: 4.85 ± 1.73 uIu/mL (-) | Mean ± SD: FT4 = 0.95 ± 0.2 ng/dL (-) | Mean ± SD: 4.934 ± 2.33 ng/mL | SPINA-GT sTSHI | |
| Sur et al. (2019) [62] | Mean ± SEM: 7.72 ± 1.74 in control group and Mean ± SEM:7.31 ± 1.46 in HT group (μg/g creatinine) (-) | Hashimoto | |||
| Wang et al. (2020) [57] | GM: 5.48 (95%CI: 5.22, 5.77) mIU/L (-) | FT3 (pmol/L) Mean ± SD: Low tertile: 1.87 ± 0.34 Medium tertile: 1.81 ± 0.32 High tertile: 1.85 ± 0.38 (-) | FT4 (pmol/L) Mean ± SD: Low tertile: 13.75 ± 1.45 Medium tertile: 13.84 ± 1.35 High tertile: 13.82 ± 1.38 (-) | GM: 1.32 ng/mL (95%CI: 1.17–1.49) | Positivity of TPO-AbMean ± SD: Low tertile: 11 (8.3) Medium tertile: 15 (11.4) High tertile: 8 (5.9) (-) |
| Fen Li et al. (2020) [54] | Median: 6.43 μIU/L ↓ | Median: TT3 = 0.85 nmol/L Median: FT3 = 1.78 pmol/L ↓ | Median: FT4 = 14.18 pmol/L Median: TT4 = 92.90 nmol/L | Maternal median: 1.30 μg/g Cr Children’s median: 0.51 μg/g Cr | Neuro-development |
| Guo et al. (2020) [55] | Median: 6.88 pmol/L (IQR: 4.93 −9.49) (-) | Median: FT3 = 2.5 (IQR:2.3–2.7) pmol/L Median: TT3 = 0.89 (IQR:0.78–1.00) nmol/L (-) | Median: FT4 = 16.0 (IQR: 14.8–17.2) pmol/L Median: TT4 = 126 (IQR: 110–140) nmol/L ↑ | Maternal Median: 1.75 μg/L (IQR: 0.60–16.1) Children Median: 1.29 μg/L (IQR:0.56–2.40) | Median: TPOAb = 14.7 (IQR: 12.5–17.4) IU/mL |
| Derakhshan et al. (2020) [60] | Median (95% range) Newborn: 9.57 mU/L (3.13–34.7) ↑ Child: 2.33 mU/L (0.92–4.87) | Median (95% range) Newborn FT4 = 20.6 pmol/L (14.8–31.0) Child FT4 = 16.8 pmol/L(13.7–20.9) ↓ | Median (95% range) Early pregnancy: 1.61(<LOD-21.0) ng/mL Middle pregnancy: 1.47(<LOD-21.2) ng/mL Late pregnancy: 1.65(<LOD-20.5) ng/ml | ||
| Jang et al. 2021 [59] | Mean ± SD: 2.55 ± 1.36 μIU/mL (-) | Mean ± SD: TT3 = 148.00 ± 18.47 ng/dL | Mean ± SD: FT4 = 1.15 ± 0.11 ng/dL (-) | Mean ± SD: Children 2.73 ± 7.15 μg/L Mean ± SD: Prenatal 2.15 ± 2.85 μg/g Cr |
| TSH | |
|---|---|
| Brucker-Davis et al. (2011) [53] | Negative correlation between BPA concentrations and TSH (r = −0.25, p = 0.077) |
| Chevrier et al. (2013) [51] | Inverse relationship between maternal BPA concentrations and TSH in boys (−9.9% per log2 unit; 95% CI: −15.9%, −3.5%) |
| Romano et al. (2015) [52] | Inverse relationship between maternal BPA concentrations and TSH in girls (percent change = −36.0%; 95%(CI): −58.4, −1.7%) |
| Fen Li et al. (2020) [54] | Significant inverse relationship between BPA and TSH concentrations Overall:(β highest = −1.91, 95% CI: −3.32, −0.50); for boys: (β highest = −1.89, 95%CI: −3.70, −0.50) and for girls: (β middle = −2.34, 95% CI: −4.61, −0.07) |
| Derakhshan et al. (2020) [60] | Positive association of BPA with TSH in newborns, especially in females [β [95% CI]: 0.04 (0.007)] |
| T4 | |
| Sur et al. (2019) [62] | Negative correlation between BPA level and FT4 concentrations (r = −0.483, p < 0.02) |
| Wang et al. (2020) [57] | In mothers with higher BMI and higher BPA exposure, cord serum FT4 was 2.96 (95% CI 0.12–5.80) pmol/L higher in male newborns and 2.22 (95% CI 0.67–3.78) pmol/L higher in female newborns compared to those in the low tertile of BPA levels. |
| Guo et al. (2020) [55] | Maternal BPA concentrations were positively correlated with 1.00% (95%CI: 0.20%, 1.92%) increases in cord serum FT4 concentrations |
| Derakhshan et al. (2020) [60] | Lower FT4 concentration in childhood (β (95% CI): −0.11 (−0.21 to −0.01)) |
| T3 | |
| Fen Li et al. (2020) [54] | Children with the middle or highest tertile of BPA concentration also had lower TT3 (β highest = −0.05, 95%CI: −0.10,−0.01), FT3 (βhighest = −0.12, 95%CI: −0.22, −0.02; βmiddle = −0.11, 95% CI: −0.21, −0.01). |
| Jang et al., 2021 [59] | Gender specific effect between prenatal BPA and T3 concentrations (Boys p = 0.025; Girls p = 0.028) |
| Thyroid volume and multiple nodules risk | |
| Wang et al. (2015) [61] | Inverse association between urinary BPA concentration and thyroid volume (β = −0.033, 95% CI: −0.053, −0.013) |
| Negative association with the risk of multiple nodules (OR = 0.78; 95% CI: 0.63, 0.97) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koutaki, D.; Paltoglou, G.; Vourdoumpa, A.; Charmandari, E. The Impact of Bisphenol A on Thyroid Function in Neonates and Children: A Systematic Review of the Literature. Nutrients 2022, 14, 168. https://doi.org/10.3390/nu14010168
Koutaki D, Paltoglou G, Vourdoumpa A, Charmandari E. The Impact of Bisphenol A on Thyroid Function in Neonates and Children: A Systematic Review of the Literature. Nutrients. 2022; 14(1):168. https://doi.org/10.3390/nu14010168
Chicago/Turabian StyleKoutaki, Diamanto, George Paltoglou, Aikaterini Vourdoumpa, and Evangelia Charmandari. 2022. "The Impact of Bisphenol A on Thyroid Function in Neonates and Children: A Systematic Review of the Literature" Nutrients 14, no. 1: 168. https://doi.org/10.3390/nu14010168
APA StyleKoutaki, D., Paltoglou, G., Vourdoumpa, A., & Charmandari, E. (2022). The Impact of Bisphenol A on Thyroid Function in Neonates and Children: A Systematic Review of the Literature. Nutrients, 14(1), 168. https://doi.org/10.3390/nu14010168