
Protein Intake and Physical Activity in Newly Diagnosed Patients with Acute Coronary Syndrome: A 5-Year Longitudinal Study

 , ,
, ,  , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures
2.2.1. Protein Consumption
2.2.2. Physical Activity
2.2.3. Anxious and Depressive Symptoms
2.3. Data Analysis
3. Results
3.1. Study Population
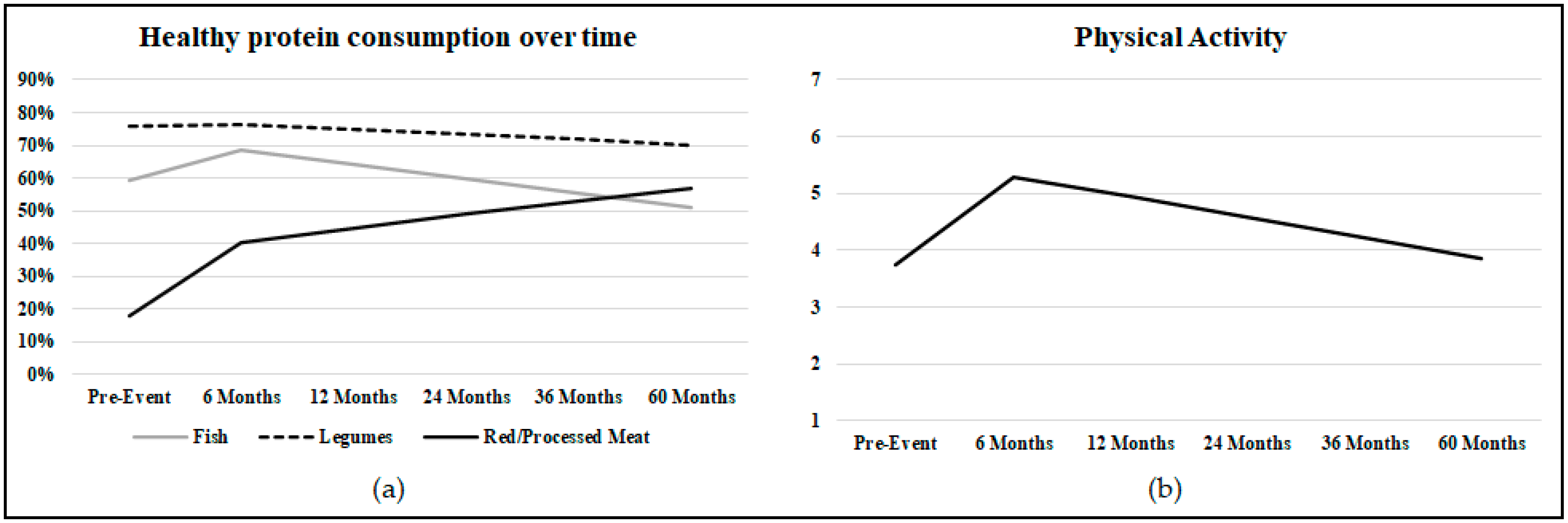
3.2. Longitudinal Changes in Protein Intake
3.3. Longitudinal Changes in Physical Activity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary. J. Am. Coll. Cardiol. 2019, 74, 1376–1414. [Google Scholar] [CrossRef] [PubMed]
- Timmis, A.; Townsend, N.; Gale, C.P.; Torbica, A.; Lettino, M.; Petersen, S.E.; Mossialos, E.A.; Maggioni, A.P.; Kazakiewicz, D.; May, H.T.; et al. European Society of Cardiology: Cardiovascular Disease Statistics 2019. Eur. Heart J. 2019, 41, 12–85. [Google Scholar] [CrossRef]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of Potentially Modifiable Risk Factors Associated with Myocardial Infarction in 52 Countries (the INTERHEART Study): Case-Control Study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Hamer, M.; O’Donovan, G.; Murphy, M. Physical Inactivity and the Economic and Health Burdens Due to Cardiovascular Disease: Exercise as Medicine. Adv. Exp. Med. Biol. 2017, 999, 3–18. [Google Scholar] [CrossRef]
- Hu, F.B. Protein, Body Weight, and Cardiovascular Health. Am. J. Clin. Nutr. 2005, 82, 242S–247S. [Google Scholar] [CrossRef]
- Zhang, B.; Xiong, K.; Cai, J.; Ma, A. Fish Consumption and Coronary Heart Disease: A Meta-Analysis. Nutrients 2020, 12, 2278. [Google Scholar] [CrossRef]
- Cui, K.; Liu, Y.; Zhu, L.; Mei, X.; Jin, P.; Luo, Y. Association between Intake of Red and Processed Meat and the Risk of Heart Failure: A Meta-Analysis. BMC Public Health 2019, 19, 1–8. [Google Scholar] [CrossRef]
- Widmer, R.J.; Flammer, A.J.; Lerman, L.O.; Lerman, A. The Mediterranean Diet, Its Components, and Cardiovascular Disease. Am. J. Med. 2015, 128, 229–238. [Google Scholar] [CrossRef]
- Bechthold, A.; Boeing, H.; Schwedhelm, C.; Hoffmann, G.; Knüppel, S.; Iqbal, K.; De Henauw, S.; Michels, N.; Devleesschauwer, B.; Schlesinger, S.; et al. Food Groups and Risk of Coronary Heart Disease, Stroke and Heart Failure: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Crit. Rev. Food Sci. Nutr. 2019, 59, 1071–1090. [Google Scholar] [CrossRef] [PubMed]
- Kotseva, K.; De Backer, G.; De Bacquer, D.; Rydén, L.; Hoes, A.; Grobbee, D.; Maggioni, A.; Marques-Vidal, P.; Jennings, C.; Abreu, A.; et al. Lifestyle and Impact on Cardiovascular Risk Factor Control in Coronary Patients across 27 Countries: Results from the European Society of Cardiology ESC-EORP EUROASPIRE V Registry. Eur. J. Prev. Cardiol. 2019, 26, 824–835. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Patao, C.; Chuang, J.; Wong, N.D. Cardiovascular Risk Factor Control and Adherence to Recommended Lifestyle and Medical Therapies in Persons with Coronary Heart Disease (from the National Health and Nutrition Examination Survey 2007–2010). Am. J. Cardiol. 2013, 112, 1126–1132. [Google Scholar] [CrossRef]
- Greco, A.; Brugnera, A.; D’Addario, M.; Compare, A.; Franzelli, C.; Maloberti, A.; Giannattasio, C.; Fattirolli, F.; Steca, P. A Three-Year Longitudinal Study of Healthy Lifestyle Behaviors and Adherence to Pharmacological Treatments in Newly Diagnosed Patients with Acute Coronary Syndrome: Hierarchical Linear Modeling Analyses. J. Public Health (Bangkok) 2020, 1–12. [Google Scholar] [CrossRef]
- Grace, S.L.; Abbey, S.E.; Shnek, Z.M.; Irvine, J.; Franche, R.-L.; Stewart, D.E. Cardiac Rehabilitation II: Referral and Participation. Gen. Hosp. Psychiatry 2002, 24, 127–134. [Google Scholar] [CrossRef]
- Jensen, M.T.; Marott, J.L.; Holtermann, A.; Gyntelberg, F. Living Alone Is Associated with All-Cause and Cardiovascular Mortality: 32 Years of Follow-up in the Copenhagen Male Study. Eur. Heart J. Qual. Care Clin. Outcomes 2019, 5, 208–217. [Google Scholar] [CrossRef]
- May, H.T.; Horne, B.D.; Knight, S.; Knowlton, K.U.; Bair, T.L.; Lappé, D.L.; Le, V.T.; Muhlestein, J.B. The Association of Depression at Any Time to the Risk of Death Following Coronary Artery Disease Diagnosis. Eur. Heart. J. Qual. Care Clin. Outcomes 2017, 3, 296–302. [Google Scholar] [CrossRef]
- Monzani, D.; D’Addario, M.; Fattirolli, F.; Giannattasio, C.; Greco, A.; Quarenghi, F.; Steca, P. Clustering of Lifestyle Risk Factors in Acute Coronary Syndrome: Prevalence and Change after the First Event. Appl. Psychol. Health Well-Being 2018, 10, 434–456. [Google Scholar] [CrossRef] [PubMed]
- Kuhl, E.A.; Fauerbach, J.A.; Bush, D.E.; Ziegelstein, R.C. Relation of Anxiety and Adherence to Risk-Reducing Recommendations Following Myocardial Infarction. Am. J. Cardiol. 2009, 103, 1629–1634. [Google Scholar] [CrossRef]
- Steca, P.; Monzani, D.; Greco, A.; Franzelli, C.; Magrin, M.E.; Miglioretti, M.; Sarini, M.; Scrignaro, M.; Vecchio, L.; Fattirolli, F.; et al. Stability and Change of Lifestyle Profiles in Cardiovascular Patients after Their First Acute Coronary Event. PLoS ONE 2017, 12, e0183905. [Google Scholar] [CrossRef]
- Ma, Y.; Olendzki, B.C.; Li, W.; Hafner, A.R.; Chiriboga, D.; Hebert, J.R.; Campbell, M.; Sarnie, M.; Ockene, I.S. Seasonal Variation in Food Intake, Physical Activity, and Body Weight in a Predominantly Overweight Population. Eur. J. Clin. Nutr. 2006, 60, 519–528. [Google Scholar] [CrossRef]
- Stelmach-Mardas, M.; Kleiser, C.; Uzhova, I.; Peñalvo, J.L.; La Torre, G.; Palys, W.; Lojko, D.; Nimptsch, K.; Suwalska, A.; Linseisen, J.; et al. Seasonality of Food Groups and Total Energy Intake: A Systematic Review and Meta-Analysis. Eur. J. Clin. Nutr. 2016, 70, 700–708. [Google Scholar] [CrossRef]
- van der Toorn, J.E.; Cepeda, M. Seasonal Variation of Diet Quality in a Large Middle-Aged and Elderly Dutch Population-Based Cohort. Eur. J. Nutr. 2020, 59, 493–504. [Google Scholar] [CrossRef]
- Bhatnagar, A. Environmental Determinants of Cardiovascular Disease. Circ. Res. 2017, 121, 162–180. [Google Scholar] [CrossRef] [PubMed]
- Izawa, K.P.; Watanabe, S.; Oka, K.; Brubaker, P.H.; Hirano, Y.; Omori, Y.; Kida, K.; Suzuki, K.; Osada, N.; Omiya, K.; et al. Leisure-Time Physical Activity over Four Seasons in Chronic Heart Failure Patients. Int. J. Cardiol. 2014, 177, 651–653. [Google Scholar] [CrossRef] [PubMed]
- Klompstra, L.; Jaarsma, T.; Strömberg, A.; van der Wal, M.H.L. Seasonal Variation in Physical Activity in Patients with Heart Failure. Heart Lung 2019, 48, 381–385. [Google Scholar] [CrossRef]
- Steca, P.; Pancani, L.; Greco, A.; D’Addario, M.; Magrin, M.E.; Miglioretti, M.; Sarini, M.; Scrignaro, M.; Vecchio, L.; Cesana, F.; et al. Changes in Dietary Behavior among Coronary and Hypertensive Patients: A Longitudinal Investigation Using the Health Action Process Approach. Appl. Psychol. Health Well Being 2015, 7, 316–339. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Topolski, T.D.; LoGerfo, J.; Patrick, D.L.; Williams, B.; Walwick, J.; Patrick, M.B. The Rapid Assessment of Physical Activity (RAPA) among Older Adults. Prev. Chronic Dis. 2006, 3, A118. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Costantini, M.; Musso, M.; Viterbori, P.; Bonci, F.; Del Mastro, L.; Garrone, O.; Venturini, M.; Morasso, G. Detecting Psychological Distress in Cancer Patients: Validity of the Italian Version of the Hospital Anxiety and Depression Scale. Support. Care Cancer 1999, 7, 121–127. [Google Scholar] [CrossRef]
- Raudenbush, S.W.; Bryk, A.S. Hierarchical Linear Models: Applications and Data Analysis Methods, 2nd ed.; Sage: Thousand Oaks, CA, USA, 2002; Volume 1. [Google Scholar]
- Gallop, R.; Tasca, G.A. Multilevel Modeling of Longitudinal Data for Psychotherapy Researchers: II. The Complexities. Psychother. Res. 2009, 19, 438–452. [Google Scholar] [CrossRef]
- Willet, J.; Singer, J. Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence; Oxford University Press: New York, NY, USA, 2003. [Google Scholar]
- Calabrò, P.; Gragnano, F.; Di Maio, M.; Patti, G.; Antonucci, E.; Cirillo, P.; Gresele, P.; Palareti, G.; Pengo, V.; Pignatelli, P.; et al. Epidemiology and Management of Patients With Acute Coronary Syndromes in Contemporary Real-World Practice: Evolving Trends from the EYESHOT Study to the START-ANTIPLATELET Registry. Angiology 2018, 69, 795–802. [Google Scholar] [CrossRef]
- Munyombwe, T.; Hall, M.; Dondo, T.B.; Alabas, O.A.; Gerard, O.; West, R.M.; Pujades-Rodriguez, M.; Hall, A.; Gale, C.P. Quality of Life Trajectories in Survivors of Acute Myocardial Infarction: A National Longitudinal Study. Heart 2020, 106, 33–39. [Google Scholar] [CrossRef]
- Peersen, K.; Munkhaugen, J.; Gullestad, L.; Liodden, T.; Moum, T.; Dammen, T.; Perk, J.; Otterstad, J.E. The Role of Cardiac Rehabilitation in Secondary Prevention after Coronary Events. Eur. J. Prev. Cardiol. 2017, 24, 1360–1368. [Google Scholar] [CrossRef]
- Urbinati, S.; Olivari, Z.; Gonzini, L.; Savonitto, S.; Farina, R.; Del Pinto, M.; Valbusa, A.; Fantini, G.; Mazzoni, A.; Maggioni, A.P. Secondary Prevention after Acute Myocardial Infarction: Drug Adherence, Treatment Goals, and Predictors of Health Lifestyle Habits. The BLITZ-4 Registry. Eur. J. Prev. Cardiol. 2015, 22, 1548–1556. [Google Scholar] [CrossRef]
- Claassen, L.; Henneman, L.; Kindt, I.; Marteau, T.M.; Timmermans, D.R. Perceived Risk and Representations of Cardiovascular Disease and Preventive Behaviour in People Diagnosed with Familial Hypercholesterolemia: A Cross-Sectional Questionnaire Study. J. Health Psychol. 2010, 15, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Alwan, H.; William, J.; Viswanathan, B.; Paccaud, F.; Bovet, P. Perception of Cardiovascular Risk and Comparison with Actual Cardiovascular Risk. Eur. J. Cardiovasc. Prev. Rehabil. 2009, 16, 556–561. [Google Scholar] [CrossRef]
- Laursen, U.B.; Johansen, M.N.; Joensen, A.M.; Overvad, K.; Larsen, M.L. Is Cardiac Rehabilitation Equally Effective in Improving Dietary Intake in All Patients with Ischemic Heart Disease? J. Am. Coll. Nutr. 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Grace, S.L.; Abbey, S.E.; Shnek, Z.M.; Irvine, J.; Franche, R.-L.; Stewart, D.E. Cardiac Rehabilitation I: Review of Psychosocial Factors. Gen. Hosp. Psychiatry 2002, 24, 121–126. [Google Scholar] [CrossRef]
- Tully, P.J.; Cosh, S.M.; Baune, B.T. A review of the affects of worry and generalized anxiety disorder upon cardiovascular health and coronary heart disease. Psychol. Health Med. 2013, 18, 627–644. [Google Scholar] [CrossRef]
- Beckie, T.M.; Beckstead, J.W. Predicting Cardiac Rehabilitation Attendance in a Gender-Tailored Randomized Clinical Trial. J. Cardiopulm. Rehabil. Prev. 2010, 30, 147–156. [Google Scholar] [CrossRef]
- Parker, G.; Hyett, M.; Hadzi-Pavlovic, D.; Brotchie, H.; Walsh, W. GAD is good? Generalized anxiety disorder predicts a superior five-year outcome following an acute coronary syndrome. Psychiatry Res. 2011, 188, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.J.; Cameron, L.D.; Wünsche, B.; Stevens, C. A randomized trial of computer-based communications using imagery and text information to alter representations of heart disease risk and motivate protective behaviour. Br. J. Health Psychol. 2011, 16, 72–91. [Google Scholar] [CrossRef] [PubMed]
- Conraads, V.M.; Deaton, C.; Piotrowicz, E.; Santaularia, N.; Tierney, S.; Piepoli, M.F.; Pieske, B.; Schmid, J.P.; Dickstein, K.; Ponikowski, P.P.; et al. Adherence of Heart Failure Patients to Exercise: Barriers and Possible Solutions: A Position Statement of the Study Group on Exercise Training in Heart Failure of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2012, 14, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Greco, A.; Steca, P.; Pozzi, R.; Monzani, D.; D’Addario, M.; Villani, A.; Rella, V.; Giglio, A.; Malfatto, G.; Parati, G. Predicting Depression from Illness Severity in Cardiovascular Disease Patients: Self-Efficacy Beliefs, Illness Perception, and Perceived Social Support as Mediators. Int. J. Behav. Med. 2014, 21, 221–229. [Google Scholar] [CrossRef]
- Vellone, E.; Pancani, L.; Greco, A.; Steca, P.; Riegel, B. Self-Care Confidence May Be More Important than Cognition to Influence Self-Care Behaviors in Adults with Heart Failure: Testing a Mediation Model. Int. J. Nurs. Stud. 2016, 60, 191–199. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: Toward a Unifying Theory of Behavioral Change. Psychol. Rev. 1977, 84, 191. [Google Scholar] [CrossRef]
- Schwarzer, R. Social-Cognitive Factors in Changing Health-Related Behaviors. Curr. Dir. Psychol. Sci. 2001, 10, 47–51. [Google Scholar] [CrossRef]
- Sol, B.G.M.; van der Graaf, Y.; van Petersen, R.; Visseren, F.L.J. The Effect of Self-Efficacy on Cardiovascular Lifestyle. Eur. J. Cardiovasc. Nurs. 2011, 10, 180–186. [Google Scholar] [CrossRef]
- Baretta, D.; Sartori, F.; Greco, A.; D’Addario, M.; Melen, R.; Steca, P. Improving Physical Activity MHealth Interventions: Development of a Computational Model of Self-Efficacy Theory to Define Adaptive Goals for Exercise Promotion. Adv. Hum. Comput. Interact. 2019, 2019, 3068748. [Google Scholar] [CrossRef]
- Schwarzer, R. Modeling health behavior change: How to predict and modify the adoption and maintenance of health behaviors. Appl. Psychol. 2008, 57, 1–29. [Google Scholar] [CrossRef]
- Sharman, J.E.; La Gerche, A.; Coombes, J.S. Exercise and Cardiovascular Risk in Patients with Hypertension. Am. J. Hypertens. 2015, 28, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Aaby, A.; Friis, K.; Christensen, B.; Rowlands, G.; Maindal, H.T. Health Literacy Is Associated with Health Behaviour and Self-Reported Health: A Large Population-Based Study in Individuals with Cardiovascular Disease. Eur. J. Prev. Cardiol. 2017, 24, 1880–1888. [Google Scholar] [CrossRef] [PubMed]
- Veronesi, G.; Ferrario, M.M.; Kuulasmaa, K.; Bobak, M.; Chambless, L.E.; Salomaa, V.; Soderberg, S.; Pajak, A.; Jørgensen, T.; Amouyel, P.; et al. Educational Class Inequalities in the Incidence of Coronary Heart Disease in Europe. Heart 2016, 102, 958–965. [Google Scholar] [CrossRef] [PubMed]
- Magrin, M.E.; D’addario, M.; Greco, A.; Miglioretti, M.; Sarini, M.; Scrignaro, M.; Steca, P.; Vecchio, L.; Crocetti, E. Social Support and Adherence to Treatment in Hypertensive Patients: A Meta-Analysis. Ann. Behav. Med. 2015, 49, 307–318. [Google Scholar] [CrossRef]
- Warehime, S.; Dinkel, D.; Alonso, W.; Pozehl, B. Long-term exercise adherence in patients with heart failure: A qualitative study. Heart Lung 2020, 49, 696–701. [Google Scholar] [CrossRef] [PubMed]
- Prince, S.A.; Adamo, K.B.; Hamel, M.E.; Hardt, J.; Gorber, S.C.; Tremblay, M. A Comparison of Direct versus Self-Report Measures for Assessing Physical Activity in Adults: A Systematic Review. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 1–24. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sociodemographic Variables | ACS Patients |
|---|---|
| Age, mean (SD) | 57.1 (7.87) |
| Gender, n (%) | |
| Male | 231 (84%) |
| Female | 44 (16%) |
| Working status, n (%) | |
| working | 111 (40.4%) |
| not working | 163 (59.3%) |
| Educational level, n (%) | |
| less than high school | 141 (51.3%) |
| high school or higher | 134 (48.7%) |
| Marital status, n (%) | |
| single\widowed\divorced | 78 (28.4%) |
| married | 197 (71.6%) |
| Clinical Variables | ACS Patients |
|---|---|
| Clinical Presentation, n (%) | |
| Non-ST elevation myocardial infarction (NSTEMI) | 54 (19.8) |
| ST-elevation myocardial infarction (STEMI) | 196 (71.8) |
| Unstable Angina | 23 (8.5) |
| Percutaneous coronary intervention, n (%) | 258 (94.5) |
| Patients with at least one stent, n (%) | 263 (96) |
| Risk factors, n (%) | |
| Hypertension | 127 (46.5) |
| Dyslipidemia | 143 (52.4) |
| Smoking History | 180 (66.4) |
| Diabetes | 47 (17.2) |
| Obesity | 43 (15.8) |
| Family History of CVD | 108 (39.3) |
| Physical Inactivity | 20 (7.3) |
| Body Mass Index, mean (SD) | 27.2 (4.1) |
| Systolic Blood Pressure (SBP), mean (SD) | 115.9 (13.9) |
| Diastolic Blood Pressure (DBP), mean (SD) | 72.9 (8.5) |
| Baseline | 6 Months | 1 Year | 2 Years | 3 Years | 5 Years | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N (%) | Mean (SD) | N (%) | Mean (SD) | N (%) | Mean (SD) | N (%) | Mean (SD) | N (%) | Mean (SD) | N (%) | Mean (SD) | |
| Anxiety | 274 39% | 6.85 (3.88) | 241 33% | 6.23 (3.35) | 233 26% | 5.70 (3.45) | 218 28% | 5.99 (3.37) | 183 26% | 5.68 (3.34) | 175 14% | 4.21 (3.19) |
| Depression | 274 21% | 4.73 (3.42) | 241 19% | 4.45 (3.18) | 233 11% | 3.84 (2.98) | 218 17% | 4.45 (3.14) | 183 15% | 4.25 (3.29) | 175 14% | 2.90 (2.94) |
| Pre | 6 Months | 1 Year | 2 Years | 3 Years | 5 Years | |||||||
| N | n (%) | N | n (%) | N | n (%) | N | n (%) | N | n (%) | N | n (%) | |
| Fish | 274 | 182 (66.4) | 239 | 185 (77.4) | 233 | 186 (67.6) | 216 | 124 (57.4) | 183 | 105 (57.4) | 176 | 109 (61.9) |
| Legumes | 273 | 216 (79.1) | 238 | 195 (81.9) | 231 | 190 (82.3) | 218 | 151 (69.3) | 183 | 124 (67.8) | 175 | 131 (74.9) |
| Red/processed meat | 274 | 23 (8.4) | 239 | 80 (33.5) | 233 | 75 (32.2) | 218 | 105 (48.2) | 184 | 85 (46.2) | 176 | 107 (60.8) |
| N | Mean (SD) | N | Mean (SD) | N | Mean (SD) | N | Mean (SD) | N | Mean (SD) | N | Mean (SD) | |
| Physical Activity | 275 | 4.20 (2.02) | 240 | 5.48 (1.79) | 234 | 5.36 (1.80) | 217 | 5.17 (1.89) | 183 | 5.12 (1.94) | 176 | 3.86 (1.96) |
| Variables | Fixed Effects | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| β1 | SE | t Values | DF | p | β2 | SE | t Values | DF | p | R2 | |
| Fish intake | 0.902 | 0.324 | 2.783 | 1006 | 0.005 | −0.213 | 0.040 | −5.341 | 1006 | <0.001 | \ |
| Legume intake | −0.035 | 0.339 | −0.103 | 1003 | 0.918 | −0.085 | 0.038 | −2.240 | 1003 | 0.025 | \ |
| Red/processed meat intake | 4.011 | 0.508 | 7.895 | 749 | <0.001 | 0.276 | 0.044 | 6.351 | 260 | <0.001 | \ |
| Physical Activity | 2.334 | 0.229 | 10.217 | 260 | <0.001 | −0.240 | 0.025 | −9.623 | 260 | <0.001 | 34.4% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Greco, A.; Brugnera, A.; Adorni, R.; D’Addario, M.; Fattirolli, F.; Franzelli, C.; Giannattasio, C.; Maloberti, A.; Zanatta, F.; Steca, P. Protein Intake and Physical Activity in Newly Diagnosed Patients with Acute Coronary Syndrome: A 5-Year Longitudinal Study. Nutrients 2021, 13, 634. https://doi.org/10.3390/nu13020634
Greco A, Brugnera A, Adorni R, D’Addario M, Fattirolli F, Franzelli C, Giannattasio C, Maloberti A, Zanatta F, Steca P. Protein Intake and Physical Activity in Newly Diagnosed Patients with Acute Coronary Syndrome: A 5-Year Longitudinal Study. Nutrients. 2021; 13(2):634. https://doi.org/10.3390/nu13020634
Chicago/Turabian StyleGreco, Andrea, Agostino Brugnera, Roberta Adorni, Marco D’Addario, Francesco Fattirolli, Cristina Franzelli, Cristina Giannattasio, Alessandro Maloberti, Francesco Zanatta, and Patrizia Steca. 2021. "Protein Intake and Physical Activity in Newly Diagnosed Patients with Acute Coronary Syndrome: A 5-Year Longitudinal Study" Nutrients 13, no. 2: 634. https://doi.org/10.3390/nu13020634
APA StyleGreco, A., Brugnera, A., Adorni, R., D’Addario, M., Fattirolli, F., Franzelli, C., Giannattasio, C., Maloberti, A., Zanatta, F., & Steca, P. (2021). Protein Intake and Physical Activity in Newly Diagnosed Patients with Acute Coronary Syndrome: A 5-Year Longitudinal Study. Nutrients, 13(2), 634. https://doi.org/10.3390/nu13020634