
Does the Minerals Content and Osmolarity of the Fluids Taken during Exercise by Female Field Hockey Players Influence on the Indicators of Water-Electrolyte and Acid-Basic Balance?


Abstract
1. Introduction
2. Materials and Methods
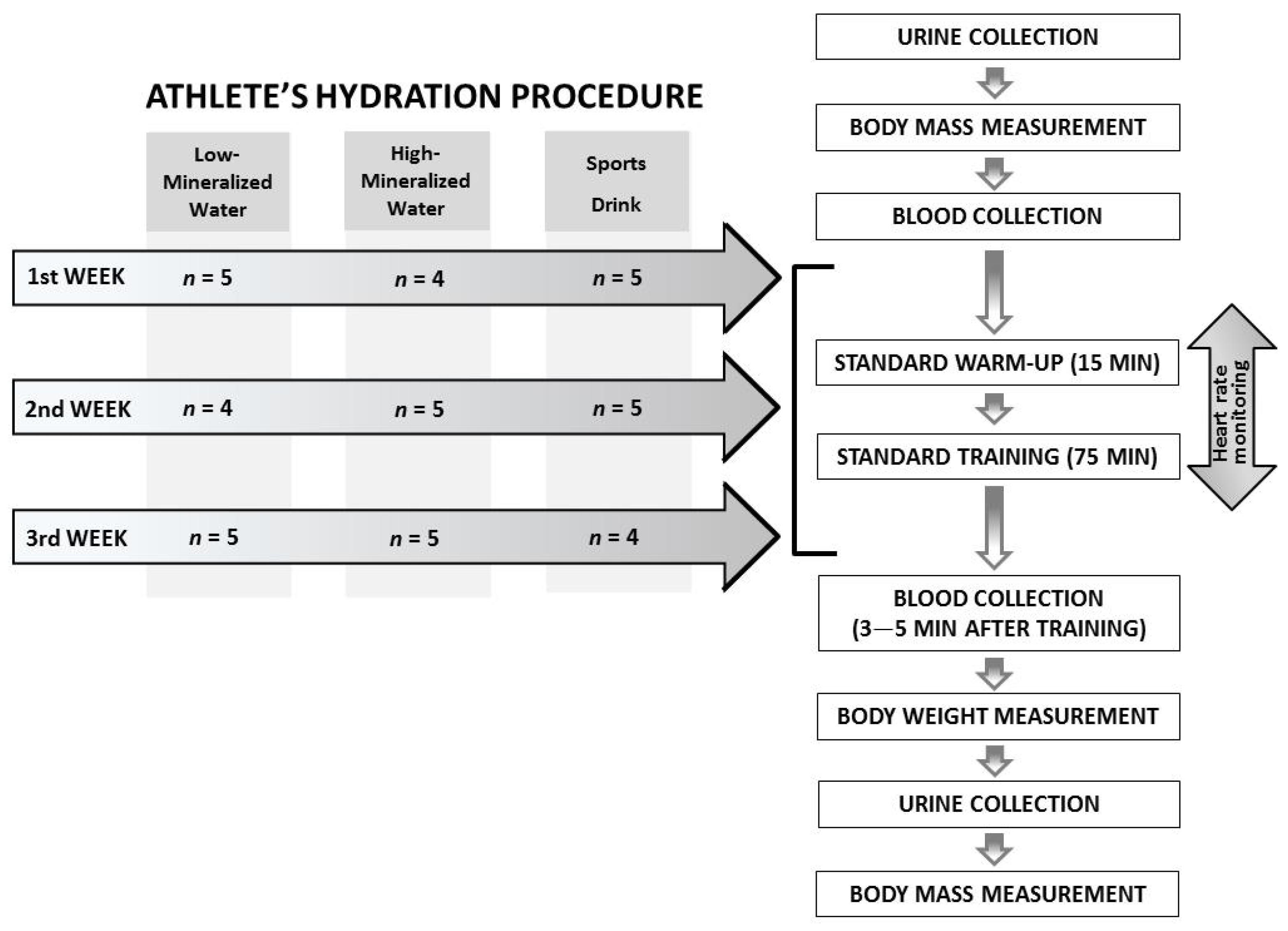
2.1. Experimental Approach
2.2. Participants
- Monday—active recovery training + static stretching
- Tuesday—technical/tactical training session + interval run
- Wednesday—technical/tactical training session (research measurements)
- Thursday—training game/small side games
- Friday—individual gym session
- Saturday—free/passive recovery
- Sunday—Polish League competition
2.3. Ethics Approval
2.4. Biochemical Analyses
2.5. Specialized Training
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barboza, S.D.; Joseph, C.; Nauta, J.; van Mechelen, W.; Verhagen, E. Injuries in Field Hockey Players: A Systematic Review. Sports Med. 2018, 48, 849–866. [Google Scholar] [CrossRef]
- MacLeod, H.; Sunderland, C. Fluid balance and hydration habits of elite female field hockey players during consecutive international matches. J. Strength Cond. Res. 2009, 23, 1245–1251. [Google Scholar] [CrossRef]
- Gabbett, T.J. GPS analysis of elite women’s field hockey training and competition. J. Strength Cond. Res. 2010, 24, 1321–1324. [Google Scholar] [CrossRef] [PubMed]
- Macutkiewicz, D.; Sunderland, C. The use of GPS to evaluate activity profiles of elite women hockey players during match-play. J. Sports Sci. 2011, 29, 967–973. [Google Scholar] [CrossRef] [PubMed]
- González-Alonso, J.; Mora-Rodríguez, R.; Below, P.R.; Coyle, E.F. Dehydration markedly impairs cardiovascular function in hyperthermic endurance athletes during exercise. J. Appl. Physiol. 1997, 82, 1229–1236. [Google Scholar] [CrossRef] [PubMed]
- Leiper, J.B.; Broad, N.P.; Maughan, R.J. Effect of intermittent high-intensity exercise on gastric emptying in man. Med. Sci. Sports Exerc. 2001, 33, 1270–1278. [Google Scholar] [CrossRef]
- Shirreffs, S.M.; Maughan, R.J. Whole body sweat collection in humans: An improved method with preliminary data on electrolyte content. J. Appl. Physiol. 1997, 82, 336–341. [Google Scholar] [CrossRef]
- Wiecek, M.; Maciejczyk, M.; Szymura, J.; Szygula, Z. Changes in oxidative stress and acid-base balance in men and women following maximal-intensity physical exercise. Physiol. Res. 2015, 64, 93–102. [Google Scholar] [CrossRef]
- Hanon, C.; Bernard, O.; Rabate, M.; Claire, T. Effect of two different long-sprint training regimens on sprint performance and associated metabolic responses. J. Strength Cond. Res. 2012, 26, 1551–1557. [Google Scholar] [CrossRef]
- Cunniffe, B.; Fallan, C.; Yau, A.; Evans, G.H.; Cardinale, M. Assessment of physical demands and fluid balance in elite female handball players during a 6-day competitive tournament. Int. J. Sport Nutr. Exerc. Metab. 2015, 25, 78–88. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific opinion on dietary reference values for water. EFSA J. 2010, 8, 1459. [Google Scholar]
- Maughan, R.J.; Leiper, J.B. Limitations to fluid replacement during exercise. Can. J. Appl. Physiol. 1999, 24, 173–187. [Google Scholar] [CrossRef]
- Nose, H.; Mack, G.W.; Shi, X.R.; Nadel, E.R. Role of osmolality and plasma volume during rehydration in humans. J. Appl. Physiol. 1988, 65, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Shirreffs, S.M.; Aragon-Vargas, L.F.; Keil, M.; Love, T.D.; Phillips, S. Rehydration after exercise in the heat: A comparison of 4 commonly used drinks. Int. J. Sport Nutr. Exerc. Metab. 2007, 17, 244–258. [Google Scholar] [CrossRef] [PubMed]
- Yamauchi, T.; Harada, T.; Kurono, M.; Matsui, N. Effect of exercise-induced acidosis on aldosterone secretion in men. Eur. J. Appl. Physiol. Occup. Physiol. 1998, 77, 409–412. [Google Scholar] [CrossRef] [PubMed]
- Passe, D.H. Physiological and psychological determinants of fluid intake. In Sports Drinks: Basic Science and Practical Aspects; Maughan, R.J., Murray, R., Eds.; CRC Press: Boca Raton, FL, USA, 2001; pp. 45–87. [Google Scholar]
- Ersoy, N.; Ersoy, G. Sports drinks for hydration and alternative drinks review. Turk. Klin. J. Sports Sci. 2013, 5, 96–100. [Google Scholar]
- Sadowska, A.; Świderski, F.; Rakowska, R.; Waszkiewicz-Robak, B.; Żebrowska-Krasuska, M.; Dybkowska, E. Beverage osmolality as a marker for maintaining appropriate body hydration. Rocz. Panstw. Zakl. Hig. 2017, 68, 167–173. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Zetou, E.; Giatsis, G.; Mountaki, F.; Komninakidou, A. Body weight changes and voluntary fluid intakes of beach volleyball players during an official tournament. J. Sci. Med. Sport 2008, 11, 139–145. [Google Scholar] [CrossRef]
- Jones, B.; Till, K.; King, R.; Gray, M.; O’Hara, J. Are Habitual Hydration Strategies of Female Rugby League Players Sufficient to Maintain Fluid Balance and Blood Sodium Concentration During Training and Match-Play? A Research Note from the Field. J. Strength Cond. Res. 2016, 30, 875–880. [Google Scholar] [CrossRef]
- O’Connell, S.M.; Woodman, R.J.; Brown, I.L.; Vincent, D.J.; Binder, H.J.; Ramakrishna, B.S.; Young, G.P. Comparison of a sports-hydration drink containing high amylose starch with usual hydration practice in Australian rules footballers during intense summer training. J. Int. Soc. Sports Nutr. 2018, 15, 1–10. [Google Scholar] [CrossRef]
- Bargh, M.J.; King, R.F.; Gray, M.P.; Jones, B. Why do team-sport athletes drink fluid in excess when exercising in cool conditions? Appl. Physiol. Nutr. Metab. 2017, 42, 271–277. [Google Scholar] [CrossRef]
- Karakoc, Y.; Duzova, H.; Polat, A.; Emre, M.H.; Arabaci, I. Effects of training period on haemorheological variables in regularly trained footballers. Br. J. Sports Med. 2005, 39, e4. [Google Scholar] [CrossRef][Green Version]
- Wang, L.; Zhang, J.; Wang, J.; He, W.; Huang, H. Effects of high-intensity training and resumed training on macroelement and microelement of elite basketball athletes. Biol. Trace Elem. Res. 2012, 149, 148–154. [Google Scholar] [CrossRef]
- Laires, M.J.; Alves, F. Changes in plasma, erythrocyte, and urinary magnesium with prolonged swimming exercise. Magnes. Res. 1991, 4, 119–122. [Google Scholar] [PubMed]
- Couderc, A.; Thomas, C.; Lacome, M.; Piscione, J.; Robineau, J.; Delfour-Peyrethon, R.; Borne, R.; Hanon, C. Movement Patterns and Metabolic Responses During an International Rugby Sevens Tournament. Int. J. Sports Physiol. Perform. 2017, 12, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Macutkiewicz, D.; Sunderland, C. Sodium bicarbonate supplementation does not improve elite women’s team sport running or field hockey skill performance. Physiol. Rep. 2018, 6, e13818. [Google Scholar] [CrossRef]
- Wiacek, M.; Andrzejewski, M.; Chmura, J.; Zubrzycki, I.Z. The changes of the specific physiological parameters in response to 12-week individualized training of young soccer players. J. Strength Cond. Res. 2011, 25, 1514–1521. [Google Scholar] [CrossRef]
- Osterberg, K.L.; Horswill, C.A.; Baker, L.B. Pregame urine specific gravity and fluid intake by National Basketball Association players during competition. J. Athl. Train. 2009, 44, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Wolf, J.P.; Nguyen, N.U.; Dumoulin, G.; Berthelay, S. Plasma renin and aldosterone changes during twenty minutes’ moderate exercise. Influence of posture. Eur. J. Appl. Physiol. Occup. Physiol. 1986, 54, 602–607. [Google Scholar] [CrossRef]
- Mannix, E.T.; Palange, P.; Aronoff, G.R.; Manfredi, F.; Farber, M.O. Atrial natriuretic peptide and the renin-aldosterone axis during exercise in man. Med. Sci. Sports Exerc. 1990, 22, 785–789. [Google Scholar] [CrossRef] [PubMed]
- Pence, J.; Bloomer, R.J. Impact of Nuun Electrolyte Tablets on Fluid Balance in Active Men and Women. Nutrients 2020, 12, 3030. [Google Scholar] [CrossRef] [PubMed]
- Boone, C.H.; Hoffman, J.R.; Gonzalez, A.M.; Jajtner, A.R.; Townsend, J.R.; Baker, K.M.; Fukuda, D.H.; Stout, J.R. Changes in Plasma Aldosterone and Electrolytes Following High-Volume and High-Intensity Resistance Exercise Protocols in Trained Men. J. Strength Cond. Res. 2016, 30, 1917–1923. [Google Scholar] [CrossRef] [PubMed]
- Morgan, R.M.; Patterson, M.J.; Nimmo, M.A. Acute effects of dehydration on sweat composition in men during prolonged exercise in the heat. Acta Physiol. Scand. 2004, 182, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Powers, S.K.; Lawler, J.; Dodd, S.; Tulley, R.; Landry, G.; Wheeler, K. Fluid replacement drinks during high intensity exercise: Effects on minimizing exercise-induced disturbances in homeostasis. Eur. J. Appl. Physiol. Occup. Physiol. 1990, 60, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Gisolfi, C.V.; Summers, R.W.; Lambert, G.P.; Xia, T. Effect of beverage osmolality on intestinal fluid absorption during exercise. J. Appl. Physiol. 1998, 85, 1941–1948. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Hashimoto, H.; Oh, T.; Ishijima, T.; Mitsuda, H.; Peake, J.M.; Sakamoto, S.; Muraoka, I.; Higuchi, M. The effects of sports drink osmolality on fluid intake and immunoendocrine responses to cycling in hot conditions. J. Nutr. Sci. Vitam. 2013, 59, 206–212. [Google Scholar] [CrossRef][Green Version]
- Łagowska, K.; Podgórski, T.; Celińska, E.; Kryściak, J. A comparison of the effectiveness of commercial and natural carbohydrate–electrolyte drinks. Sci. Sports 2017, 32, 160–164. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Low-Mineralized Water | High-Mineralized Water | Isotonic Drink | p Value | |||
|---|---|---|---|---|---|---|---|
| ± SD | 95% CI | ± SD | 95% CI | ± SD | 95% CI | ||
| Age (years) | 21.9 ± 2.3 | (20.6–23.2) | 21.9 ± 2.3 | (20.6–23.2) | 21.9 ± 2.3 | (20.6–23.2) | 1.000 |
| Body height (m) | 1.70 ± 0.06 | (1.67–1.74) | 1.70 ± 0.06 | (1.67–1.74) | 1.70 ± 0.06 | (1.67–1.74) | 1.000 |
| Body mass (kg) | 65.3 ± 5.4 | (62.2–68.4) | 65.4 ± 5.4 | (62.2–68.5) | 65.2 ± 5.0 | (62.3–68.1) | 0.712 |
| WHtR | 42.9 ± 1.4 | (42.1–43.7) | 43.0 ± 1.4 | (42.1–43.8) | 42.9 ± 1.4 | (42.1–43.7) | 0.906 |
| HR mean (bpm) | 151.7 ± 3.0 | (149.9–153.4) | 152.0 ± 4.3 | (149.5–154.5) | 151.6 ± 2.1 | (150.4–152.9) | 0.962 |
| Fluid intake (ml) | 543.9 ± 270.0 | (388.0–699.8) | 535.7 ± 180.2 | (431.7–639.8) | 503.6 ± 224.7 | (373.9–633.3) | 0.800 |
| Urine mass excreted after training (g) | 157.1 ± 70.4 | (116.5–197.8) | 135.0 ± 104.6 | (74.6–195.4) | 115.7 ± 72.8 | (73.7–157.8) | 0.404 |
| Training Group | Women’s National Team and Women’s Junior Team |
|---|---|
| Training duration | 90 min |
| Venue | Indoor Hall 40 m × 20 m |
| Training objective | Preparation for indoor championship events according to the calendar of the European Field Hockey Federation |
| Warm-up | Warm-up incl. dynamic stretching + acceleration and speed drills—15 min Hockey-specific warm-up: various forms of passing and receiving the ball in motion (without the participation of a defender); shorter and longer passes, also with the use of a boards—5 min Scoring exercises (different zones of the shooting circle)—5 min |
| Training | Numerical advantage training—2 vs. 1 and 3 vs. 2/defensive organization in the numerical superiority of the opponent; cooperation with the goalkeeper—20 min Tactical cooperation in even numbers situation—3 vs. 3 on the side sector of the pitch (left and right board) with an emphasis on the transition phase (transition from defending to attacking)—15 min Build-up in 5 vs 4 superiority—4 × 3 min + 1 min break after every 3 min 5 vs. 4 game—2 × 5 min (change of teams after 5 min) |
| Mineral | Low-Mineralized Water | High-Mineralized Water | Isotonic Drink + Low-Mineralized Water |
|---|---|---|---|
| (mg/L) | |||
| Ca2+ | 48.10 | 319.00 | 288.10 |
| Na+ | 2.10 | 111.00 | 702.10 |
| Mg2+ | 6.68 | 47.90 | 126.68 |
| K+ | 1.20 | 49.50 | 261.20 |
| HCO3− | 166.30 | 1639.00 | 166.30 |
| SO42− | 10.29 | 30.00 | 10.29 |
| Cl− | 5.60 | 2.70 | 245.60 |
| F− | 0.06 | 0.30 | 0.06 |
| Total minerals | 240.33 | 2199.40 | 1800.33 |
| Glucose | 0.00 | 0.00 | 52,600.00 |
| Indicator | Beverages | Pre-Exercise | Post-Exercise | p Value (Pre vs. Post) | Effect Size | p Value for ANOVA (Post-Exercise Differences between Beverages) |
|---|---|---|---|---|---|---|
| Body mass (kg) | Low | 65.3 ± 5.4 | 65.1 ± 5.4 | 0.002 | 0.04 | 0.706 |
| High | 65.4 ± 5.4 | 65.2 ± 5.5 | 0.001 | 0.03 | ||
| Isotonic | 65.2 ± 5.0 | 65.0 ± 5.0 | <0.001 | 0.04 | ||
| Water Balance | ||||||
| Hematocrit (l/L) | Low | 0.377 ± 0.017 | 0.366 ± 0.021 | 0.048 | 0.56 | 0.212 |
| High | 0.372 ± 0.020 | 0.360 ± 0.023 | <0.001 | 0.59 | ||
| Isotonic | 0.367 ± 0.020 | 0.353 ± 0.021 | <0.001 | 0.71 | ||
| Urine specific gravity (g/L) | Low | 1.013 ± 0.006 | 1.019 ± 0.008 | 0.001 | 0.82 | 0.108 |
| High | 1.014 ± 0.006 | 1.023 ± 0.009 | 0.006 | 1.15 | ||
| Isotonic | 1.016 ± 0.009 | 1.019 ± 0.007 | 0.068 | |||
| Plasma osmolality (mOsm/kg) | Low | 291.5 ± 2.1 | 290.1 ± 3.6 | 0.155 | <0.001 a | |
| High | 291.6 ± 2.5 | 290.1 ± 3.6 | 0.077 | |||
| Isotonic | 290.1 ± 2.9 | 285.3 ± 2.6 | 0.001 | 1.73 | ||
| Electrolyte Balance | ||||||
| Sodium ions (mmol/L) | Low | 143 ± 1 | 142 ± 2 | 0.111 | 0.005 a | |
| High | 143 ± 1 | 142 ± 2 | 0.179 | |||
| Isotonic | 142 ± 2 | 140 ± 1 | <0.001 | 1.51 | ||
| Potassium ions (mmol/L) | Low | 4.4 ± 0.4 | 4.1 ± 0.4 | 0.024 | 0.66 | 0.022 b |
| High | 4.3 ± 0.3 | 3.9 ± 0.3 | <0.001 | 1.39 | ||
| Isotonic | 4.5 ± 0.4 | 4.3 ± 0.3 | 0.075 | |||
| Calcium ions (mmol/L) | Low | 1.21 ± 0.03 | 1.19 ± 0.03 | 0.031 | 0.76 | 0.624 |
| High | 1.20 ± 0.02 | 1.18 ± 0.04 | 0.030 | 0.60 | ||
| Isotonic | 1.22 ± 0.03 | 1.19 ± 0.03 | <0.001 | 1.06 | ||
| Chloride ions (mmol/L) | Low | 109 ± 1 | 108 ± 2 | 0.418 | 0.357 | |
| High | 108 ± 2 | 107 ± 2 | 0.292 | |||
| Isotonic | 109 ± 2 | 107 ± 2 | <0.001 | 0.80 | ||
| Magnesium (mmol/L) | Low | 0.89 ± 0.01 | 0.89 ± 0.03 | 0.730 | 0.789 | |
| High | 0.89 ± 0.01 | 0.89 ± 0.02 | 0.431 | |||
| Isotonic | 0.89 ± 0.02 | 0.90 ± 0.02 | 0.272 | |||
| Aldosterone (pmol/L) | Low | 125.8 ± 45.4 | 411.8 ± 184.0 | 0.001 | 2.13 | 0.005 a |
| High | 117.0 ± 53.9 | 424.2 ± 107.5 | <0.001 | 3.61 | ||
| Isotonic | 112.2 ± 28.4 | 270.2 ± 104.6 | <0.001 | 2.06 | ||
| Acid–Base Balance | ||||||
| Bicarbonate ions (mmol/L) | Low | 24.1 ± 1.6 | 22.4 ± 1.3 | <0.001 | 1.13 | 0.683 |
| High | 24.7 ± 2.1 | 22.8 ± 1.5 | 0.005 | 1.05 | ||
| Isotonic | 24.3 ± 1.4 | 22.3 ± 2.0 | <0.001 | 1.16 | ||
| Standard base excess (mmol/L) | Low | −0.1 ± 1.3 | −2.6 ± 1.8 | <0.001 | 1.63 | 0.645 |
| High | 0.9 ± 1.7 | −2.1 ± 2.0 | <0.001 | 1.61 | ||
| Isotonic | 0.1 ± 1.7 | −2.8 ± 2.8 | <0.001 | 1.26 | ||
| Blood pH | Low | 7.40 ± 0.03 | 7.39 ± 0.03 | 0.024 | 0.45 | 0.926 |
| High | 7.41 ± 0.02 | 7.39 ± 0.03 | 0.012 | 0.82 | ||
| Isotonic | 7.40 ± 0.03 | 7.39 ± 0.03 | 0.102 | |||
| Urine pH | Low | 6.2 ± 0.7 | 5.4 ± 0.6 | 0.002 | 1.31 | 0.313 |
| High | 6.2 ± 0.7 | 5.6 ± 0.6 | 0.005 | 0.89 | ||
| Isotonic | 6.0 ± 0.7 | 5.5 ± 0.6 | 0.018 | 0.81 | ||
| Lactate (mmol/L) | Low | 1.3 ± 0.4 | 5.8 ± 1.7 | 0.001 | 3.64 | 0.807 |
| High | 1.3 ± 0.3 | 5.9 ± 2.6 | 0.001 | 2.54 | ||
| Isotonic | 1.4 ± 0.4 | 5.9 ± 2.5 | 0.001 | 2.55 | ||
| Authors (Sport Discipline) (Kind of Effort) Sex | The Types of Beverages | Tested Biochemical Indicators | |
|---|---|---|---|
| No Significant Differences | Significant Differences | ||
| Powers et al. [36] (cyclists; n = 9) (exercises with a constant load on a bicycle ergometer until fatigue) Men | Non-electrolyte placebo (NEP) (31 mOsm/kg) | Heart rate, plasma osmolality, concentration of lactate, potassium, calcium, sodium, and chloride in blood | The concentration of hydrogen ions in the blood was significantly lower after 30 min of exercise while using GP and EP compared to NEP |
| Electrolyte placebo drink without carbohydrate (EP) (48 mOsm/kg) | |||
| Glucose polymer drink containing electrolytes (GP) (231 mOsm/kg) | |||
| Gisolfi et al. [37] (wytrenowani; n = 7) (85 min 60%–65% VO2ma xcycle ergometer) 5 Men, 2 Women | Water (1 ± 0.3 mOsm/kg) | Osmolarity, sodium and potassium ions in plasma | There are no statistically significant differences |
| Hypertonic (197 ± 2 mOsm/kg) | |||
| Isotonic (295 ± 6 mOsm/kg) | |||
| Hypotonic (414 ± 2 mOsm/kg) | |||
| Suzuki et al. [38] (cyclists; n = 6) (cycling at 60% VO2peak for 90 min in the hot conditions) Men | Plain water (no data) | Plasma osmolality, lactate concentration | There are no statistically significant differences |
| Hypotonic sports drink (193 mOsm/kg) | |||
| Isotonic sports drink (317 mOsm/kg) | |||
| Łagowska et al. [39] (rowers; n = 11) (80 min of exercises on a rowing ergometer) Men | Commercially available sports drink (258 mOsm/kg) | Lactate concentration, hematocrit | There are no statistically significant differences |
| Natural carbohydrate electrolyte drink (402 mOsm/kg) | |||
| Our work (field hockey; n = 14) (90-min training unit) Women | Low-mineralized water (~20 mOsm/kg) | HR, hematocrit, concentration of lactate, calcium, chloride and bicarbonate ions, magnesium, standard base excess, blood and urine pH, and urine-specific gravity | Consumption of an isotonic drink caused the smallest increase in the concentration of aldosterone and potassium ions, and the greatest post-exercise reduction in sodium ions and blood osmolality |
| High-mineralized water (~88 mOsm/kg) | |||
| Isotonic drink (~279 mOsm/kg) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamińska, J.; Podgórski, T.; Rachwalski, K.; Pawlak, M. Does the Minerals Content and Osmolarity of the Fluids Taken during Exercise by Female Field Hockey Players Influence on the Indicators of Water-Electrolyte and Acid-Basic Balance? Nutrients 2021, 13, 505. https://doi.org/10.3390/nu13020505
Kamińska J, Podgórski T, Rachwalski K, Pawlak M. Does the Minerals Content and Osmolarity of the Fluids Taken during Exercise by Female Field Hockey Players Influence on the Indicators of Water-Electrolyte and Acid-Basic Balance? Nutrients. 2021; 13(2):505. https://doi.org/10.3390/nu13020505
Chicago/Turabian StyleKamińska, Joanna, Tomasz Podgórski, Krzysztof Rachwalski, and Maciej Pawlak. 2021. "Does the Minerals Content and Osmolarity of the Fluids Taken during Exercise by Female Field Hockey Players Influence on the Indicators of Water-Electrolyte and Acid-Basic Balance?" Nutrients 13, no. 2: 505. https://doi.org/10.3390/nu13020505
APA StyleKamińska, J., Podgórski, T., Rachwalski, K., & Pawlak, M. (2021). Does the Minerals Content and Osmolarity of the Fluids Taken during Exercise by Female Field Hockey Players Influence on the Indicators of Water-Electrolyte and Acid-Basic Balance? Nutrients, 13(2), 505. https://doi.org/10.3390/nu13020505