
Most Short Children with Cystic Fibrosis Do Not Catch Up by Adulthood

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
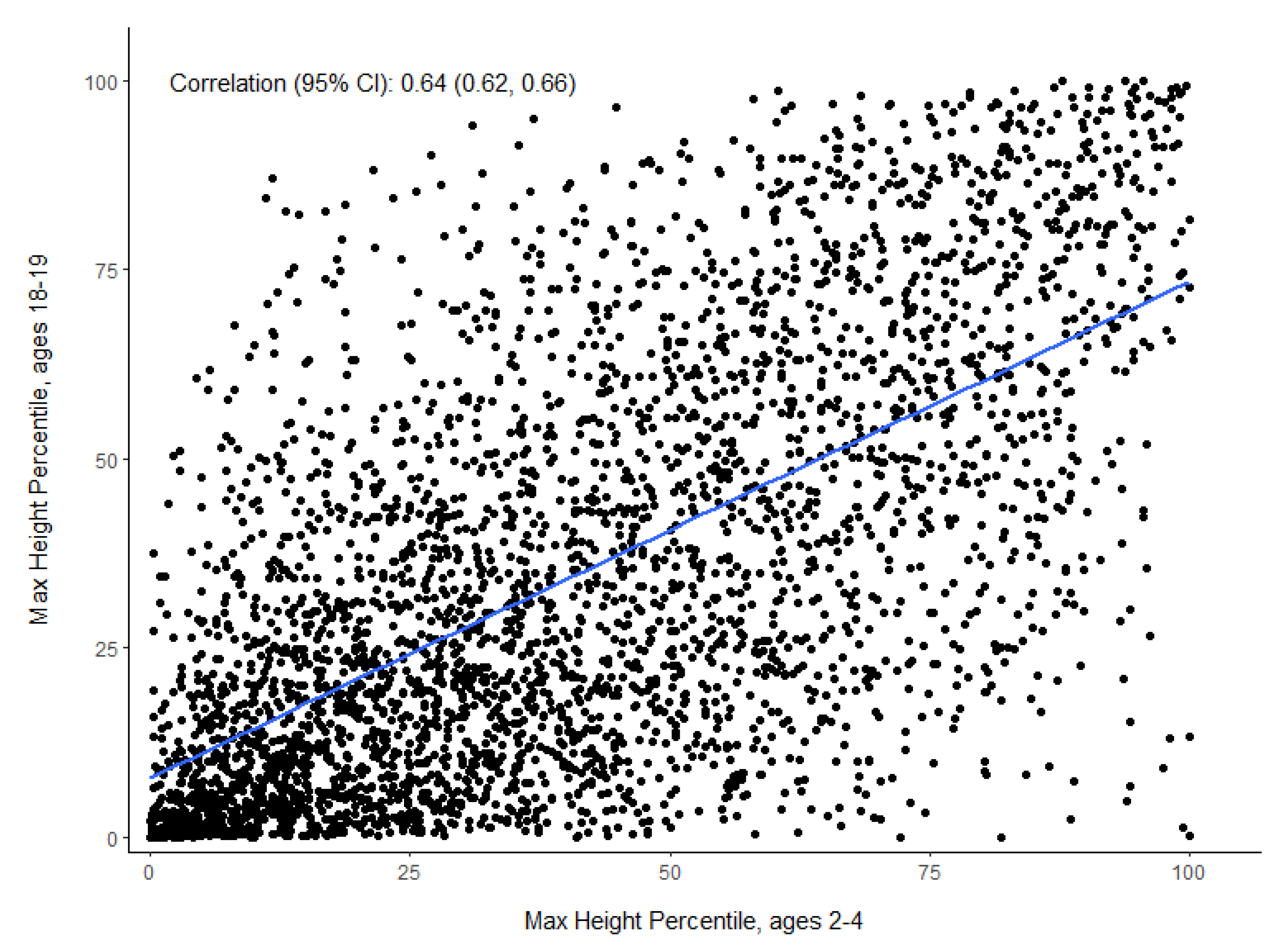
Early Childhood Height for Age Is Associated with Adult Height
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rommens, J.M.; Iannuzzi, M.C.; Kerem, B.; Drumm, M.L.; Melmer, G.; Dean, M.; Rozmahel, R.; Cole, J.; Kennedy, D.; Hidaka, N.; et al. Identification of the cystic fibrosis gene: Chromosome walking and jumping. Science 1989, 245, 1059–1065. [Google Scholar] [CrossRef] [PubMed]
- VanDevanter, D.R.; Kahle, J.; O’Sullivan, A.K.; Sikirica, S.; Hodgkins, P.S. Cystic fibrosis in young children: A review of disease manifestation, progression, and response to early treatment. J. Cyst. Fibros. 2016, 15, 147–157. [Google Scholar] [CrossRef] [Green Version]
- Sanders, D.B.; Fink, A.; Mayer-Hamblett, N.; Schechter, M.S.; Sawicki, G.S.; Rosenfeld, M.; Flume, P.A.; Morgan, W.J. Early Life Growth Trajectories in Cystic Fibrosis are Associated with Pulmonary Function at Age 6 Years. J. Pediatr. 2015, 167, 1081–1088.e1. [Google Scholar] [CrossRef] [Green Version]
- Stallings, V.A.; Stark, L.J.; Robinson, K.A.; Feranchak, A.P.; Quinton, H. Evidence-Based Practice Recommendations for Nutrition-Related Management of Children and Adults with Cystic Fibrosis and Pancreatic Insufficiency: Results of a Systematic Review. J. Am. Diet. Assoc. 2008, 108, 832–839. [Google Scholar] [CrossRef]
- Farrell, P.M.; Lai, H.J.; Li, Z.; Kosorok, M.R.; Laxova, A.; Green, C.G.; Collins, J.; Hoffman, G.; Laessig, R.; Rock, M.J.; et al. Evidence on improved outcomes with early diagnosis of cystic fibrosis through neonatal screening: Enough is enough! J. Pediatr. 2005, 147, S30–S36. [Google Scholar] [CrossRef] [PubMed]
- Konstan, M.W.; Butler, S.M.; Wohl, M.E.B.; Stoddard, M.; Matousek, R.; Wagener, J.S.; Johnson, C.A.; Morgan, W.J. Growth and nutritional indexes in early life predict pulmonary function in cystic fibrosis. J. Pediatr. 2003, 142, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Yen, E.H.; Quinton, H.; Borowitz, D. Better Nutritional Status in Early Childhood Is Associated with Improved Clinical Outcomes and Survival in Patients with Cystic Fibrosis. J. Pediatr. 2013, 162, 530–535.e1. [Google Scholar] [CrossRef]
- Assael, B.M.; Casazza, G.; Iansa, P.; Volpi, S.; Milani, S. Growth and long-term lung function in cystic fibrosis: A longitudinal study of patients diagnosed by neonatal screening. Pediatr. Pulmonol. 2009, 44, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Sanders, D.B.; E Slaven, J.; Maguiness, K.; Chmiel, J.F.; Ren, C.L. Early Life Height Attainment in Cystic Fibrosis Is Associated with Pulmonary Function at Age 6 Years. Ann. Am. Thorac. Soc. 2021, 18, 1335–1342. [Google Scholar] [CrossRef]
- Vieni, G.; Faraci, S.; Collura, M.; Lombardo, M.; Traverso, G.; Cristadoro, S.; Termini, L.; Lucanto, M.C.; Furnari, M.L.; Trimarchi, G.; et al. Stunting is an independent predictor of mortality in patients with cystic fibrosis. Clin. Nutr. 2013, 32, 382–385. [Google Scholar] [CrossRef]
- Foundation, C.F. Cystic Fibrosis Foundation Patient Registry 2019 Annual Data Report; Cystic Fibrosis Foundation: Bethesda, MD, USA, 2020. [Google Scholar]
- Centers for Disease Control and Prevention, National Center for Health Statistics: CDC Growth Charts: United States. 2000. Available online: http://www.cdc.gov/growthcharts/ (accessed on 15 September 2017).
- Konstan, M.W.; Pasta, D.J.; Wagener, J.S.; VanDevanter, D.R.; Morgan, W.J. BMI fails to identify poor nutritional status in stunted children with CF. J. Cyst. Fibros. 2017, 16, 158–160. [Google Scholar] [CrossRef] [Green Version]
- Leung, D.H.; Heltshe, S.L.; Borowitz, D.; Gelfond, D.; Kloster, M.; Heubi, J.E.; Stalvey, M.; Ramsey, B.W.; for the Baby Observational and Nutrition Study (BONUS) Investigators of the Cystic Fibrosis Foundation Therapeutics Development Network. Effects of Diagnosis by Newborn Screening for Cystic Fibrosis on Weight and Length in the First Year of Life. JAMA Pediatr. 2017, 171, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Lindstrom, M.J.; Lai, H.J. Pubertal Height Velocity and Associations with Prepubertal and Adult Heights in Cystic Fibrosis. J. Pediatr. 2013, 163, 376–382.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byard, P.J. The adolescent growth spurt in children with cystic fibrosis. Ann. Hum. Biol. 1994, 21, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Tanner, J.; Davies, P.S. Clinical longitudinal standards for height and height velocity for North American children. J. Pediatr. 1985, 107, 317–329. [Google Scholar] [CrossRef]
- Kelly, A.; Winer, K.K.; Kalkwarf, H.; Oberfield, S.E.; Lappe, J.; Gilsanz, V.; Zemel, B.S. Age-Based Reference Ranges for Annual Height Velocity in US Children. J. Clin. Endocrinol. Metab. 2014, 99, 2104–2112. [Google Scholar] [CrossRef] [PubMed]
- Zysman-Colman, Z.N.; Kilberg, M.J.; Harrison, V.S.; Chesi, A.; Grant, S.F.A.; Mitchell, J.; Sheikh, S.; Hadjiliadis, D.; Rickels, M.R.; Rubenstein, R.C.; et al. Genetic potential and height velocity during childhood and adolescence do not fully account for shorter stature in cystic fibrosis. Pediatr. Res. 2020, 89, 653–659. [Google Scholar] [CrossRef]
- A Rosenberg, L.; Schluchter, M.D.; Parlow, A.F.; Drumm, M.L. Mouse as a Model of Growth Retardation in Cystic Fibrosis. Pediatr. Res. 2006, 59, 191–195. [Google Scholar] [CrossRef] [Green Version]
- Darrah, R.; Bederman, I.; Vitko, M.; Valerio, D.M.; Drumm, M.L.; Hodges, C.A. Growth deficits in cystic fibrosis mice begin in utero prior to IGF-1 reduction. PLoS ONE 2017, 12, e0175467. [Google Scholar] [CrossRef] [PubMed]
- Stalvey, M.S.; Havasi, V.; Tuggle, K.L.; Wang, D.; Birket, S.; Rowe, S.M.; Sorscher, E.J. Reduced bone length, growth plate thickness, bone content, and IGF-I as a model for poor growth in the CFTR-deficient rat. PLoS ONE 2017, 12, e0188497. [Google Scholar] [CrossRef] [Green Version]
- Rogan, M.P.; Reznikov, L.; Pezzulo, A.; Gansemer, N.D.; Samuel, M.; Prather, R.; Zabner, J.; Fredericks, D.C.; McCray, P.; Welsh, M.J.; et al. Pigs and humans with cystic fibrosis have reduced insulin-like growth factor 1 (IGF1) levels at birth. Proc. Natl. Acad. Sci. USA 2010, 107, 20571–20575. [Google Scholar] [CrossRef] [Green Version]
- Gifford, A.; Nymon, A.; Ashare, A. Serum insulin-like growth factor-1 (IGF-1) during CF pulmonary exacerbation: Trends and biomarker correlations. Pediatr. Pulmonol. 2013, 49, 335–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terliesner, N.; Vogel, M.; Steighardt, A.; Gausche, R.; Henn, C.; Hentschel, J.; Kapellen, T.; Klamt, S.; Gebhardt, J.; Kiess, W.; et al. Cystic-fibrosis related-diabetes (CFRD) is preceded by and associated with growth failure and deteriorating lung function. J. Pediatr. Endocrinol. Metab. 2017, 30, 815–821. [Google Scholar] [CrossRef]
- Cheung, M.; Bridges, N.; Prasad, S.; Francis, J.; Carr, S.; Suri, R.; Balfour-Lynn, I. Growth in children with cystic fibrosis-related diabetes. Pediatr. Pulmonol. 2009, 44, 1223–1225. [Google Scholar] [CrossRef]
- Hardin, D.S.; Rice, J.; Ahn, C.; Ferkol, T.; Howenstine, M.; Spears, S.; Prestidge, C.; Seilheimer, D.K.; Shepherd, R. Growth hormone treatment enhances nutrition and growth in children with cystic fibrosis receiving enteral nutrition. J. Pediatr. 2005, 146, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Stalvey, M.S.; Pace, J.; Niknian, M.; Higgins, M.N.; Tarn, V.; Davis, J.; Heltshe, S.L.; Rowe, S.M. Growth in Prepubertal Children With Cystic Fibrosis Treated With Ivacaftor. Pediatrics 2017, 139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell-Heggs, P.; Mearns, M.; Batten, J.C. Cystic Fibrosis in Adolescents and Adults. QJM Int. J. Med. 1976, 45. [Google Scholar] [CrossRef] [Green Version]
- Reiter, E.O.; Stern, R.C.; Root, A.W. The Reproductive Endocrine System in Cystic Fibrosis. Am. J. Dis. Child. 1981, 135, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Buntain, H.M.; Greer, R.M.; Wong, J.C.; Schluter, P.J.; Batch, J.; Lewindon, P.; Bell, S.C.; E Wainwright, C. Pubertal development and its influences on bone mineral density in Australian children and adolescents with cystic fibrosis. J. Paediatr. Child Health 2005, 41, 317–322. [Google Scholar] [CrossRef]

{kind=link}
| Age 2–4 Height Percentile | Age 18–19 Height Percentile n % of Row | Total n % of Column | |||
|---|---|---|---|---|---|
| <10th | 10th–25th | 25th–50th | ≥50th | ||
| <10th | 563 54.4% | 283 27.4% | 150 14.5% | 38 3.7% | 1034 28.3% |
| 10th–25th | 231 23.8% | 327 33.7% | 285 29.4% | 126 13% | 969 26.5% |
| 25th–50th | 97 10.8% | 207 22.9% | 323 35.8% | 275 30.5% | 902 24.7% |
| ≥50th | 24 3.2% | 63 8.4% | 163 21.7% | 500 66.7% | 750 20.5% |
| Total | 915 25% | 880 24.1% | 921 25.2% | 939 25.7% | 3655 100% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marks, M.P.; Heltshe, S.L.; Baines, A.; Ramsey, B.W.; Hoffman, L.R.; Stalvey, M.S. Most Short Children with Cystic Fibrosis Do Not Catch Up by Adulthood. Nutrients 2021, 13, 4414. https://doi.org/10.3390/nu13124414
Marks MP, Heltshe SL, Baines A, Ramsey BW, Hoffman LR, Stalvey MS. Most Short Children with Cystic Fibrosis Do Not Catch Up by Adulthood. Nutrients. 2021; 13(12):4414. https://doi.org/10.3390/nu13124414
Chicago/Turabian StyleMarks, Margaret P., Sonya L. Heltshe, Arthur Baines, Bonnie W. Ramsey, Lucas R. Hoffman, and Michael S. Stalvey. 2021. "Most Short Children with Cystic Fibrosis Do Not Catch Up by Adulthood" Nutrients 13, no. 12: 4414. https://doi.org/10.3390/nu13124414
APA StyleMarks, M. P., Heltshe, S. L., Baines, A., Ramsey, B. W., Hoffman, L. R., & Stalvey, M. S. (2021). Most Short Children with Cystic Fibrosis Do Not Catch Up by Adulthood. Nutrients, 13(12), 4414. https://doi.org/10.3390/nu13124414