
A Systematic Review of the Cardiometabolic Benefits of Plant Products Containing Mixed Phenolics and Polyphenols in Postmenopausal Women: Insufficient Evidence for Recommendations to This Specific Population

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Question, PICO and Study Protocol
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction and Management
2.5. Assessment of the Risk of Bias
3. Results
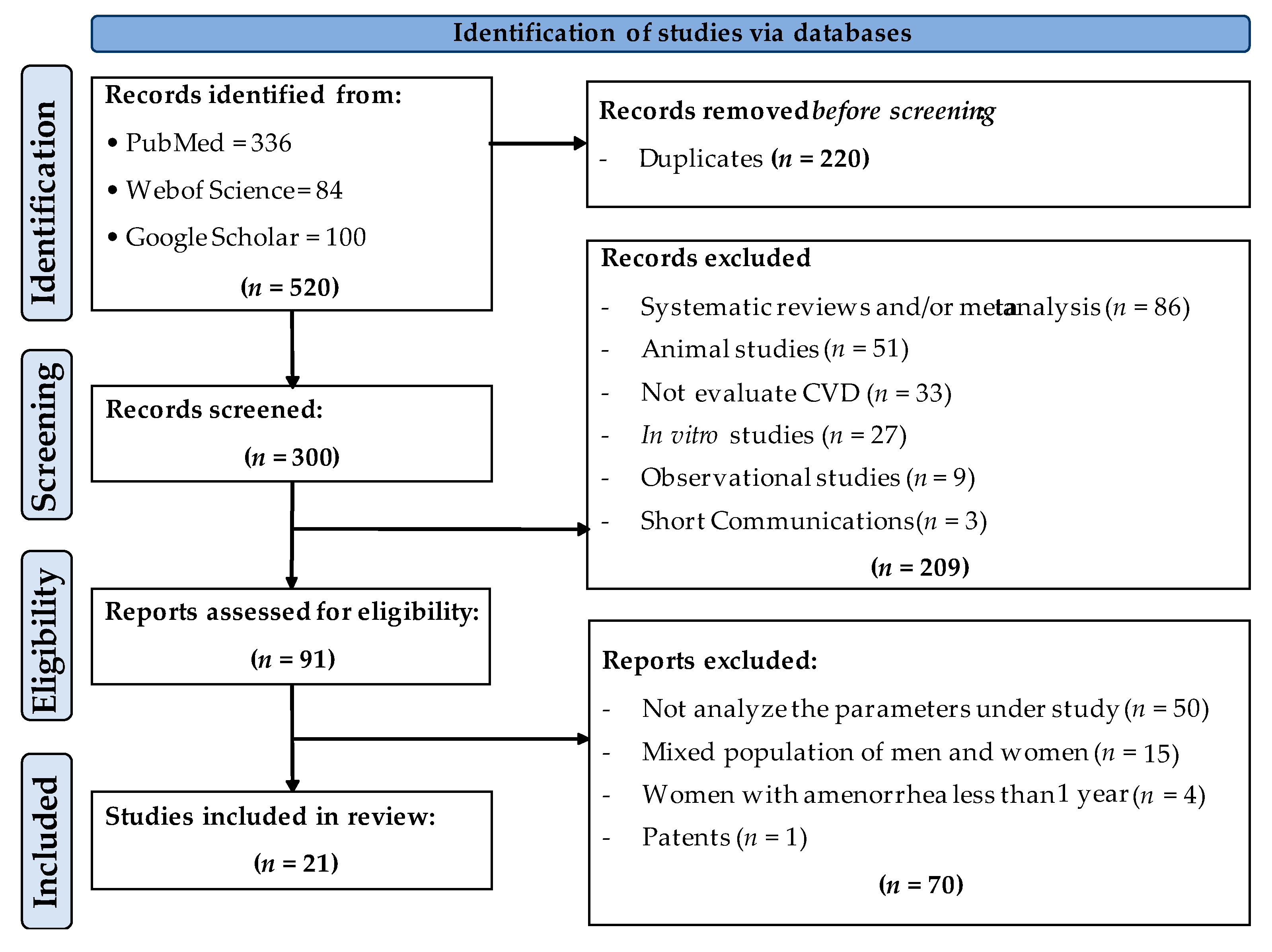
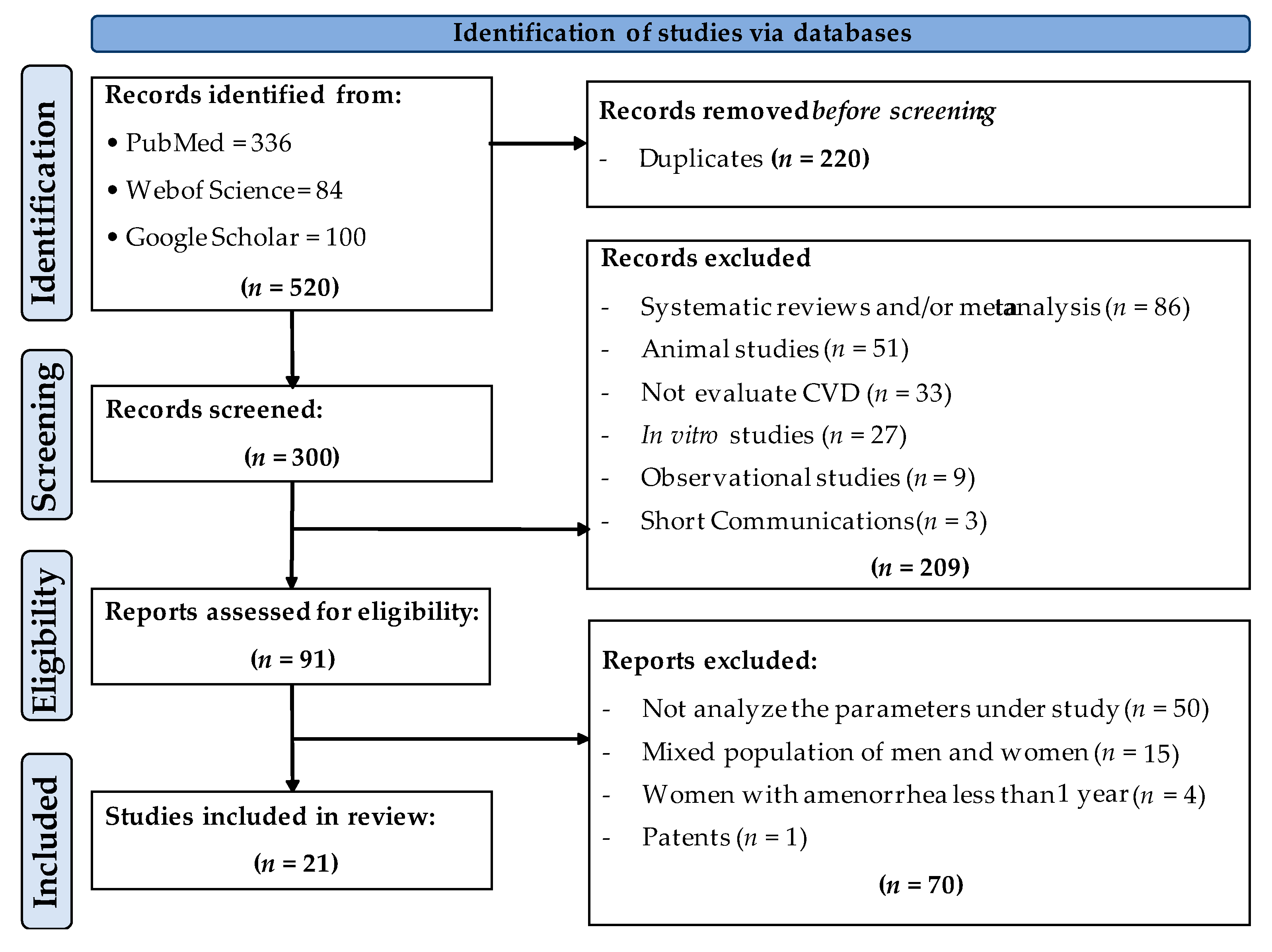
3.1. Study Selection
3.2. Description of the Characteristics of the Studies Finally Included in This Review

{kind=link}
| References | Study Design | Reported Health Status/ BMI (kg/m2) | Mean Age (Years) | Treatment/Supplementation/ Dose (poly)Phenols/Duration | Risk of Bias (Score) * |
|---|---|---|---|---|---|
| Cheng et al., 2004 [36] | Double-blind parallel P (n = 11); T (n = 17) | Healthy BMI P: 23 ± 2.0; T: 22 ± 2.6 | P: 58 ± 6.0; T: 61 ± 8.9 | P: Estrogen capsules 0.625 mg T: Isoflavone capsules (primrose oil, daidzein and genistein (w/w/w ratio 1:1:3) Dose (poly)phenols: 100 mg/day; Duration: 180 days | 7.0 |
| Sathyapalan et al., 2018 [37] | Double-blind parallel P (n = 60); T (n = 60) | Healthy BMI P: 27 ± 7.0; T: 27 ± 4.6 | P: 52; T: 52 | P: Soy protein free of isoflavones T: Soy protein with isoflavones Dose (poly)phenols: 66 mg/day; Duration: 180 days | 7.0 |
| Myasoedova et al., 2016 [35] | Double-blind parallel P (n = 71); T (n = 56) | Healthy (mixed population of asymptomatic women with hypertension, and high cholesterol were included) BMI P: 27 ± 3.8; T: 27 ± 4.0 | P: 65 ± 6.0; T: 65 ± 7.0 | P: Placebo capsules T: Mixed herbal preparation rich in isoflavonoids, containing tannins from grape seeds, green tea leaves, hop cone powder and garlic powder Dose(poly)phenols: 283 mg/day; Duration: 365 days | 6.0 |
| Wu et al., 2012 [38] | Double blind parallel, with three arms P (n = 32); T1 (n = 37); T2 (n = 34) | Healthy BMI P: 29 ± NI; T1: 30 ± NI; T2: 29 ± NI | P: 58 ± 6.3; T1: 60 ± 6.4; T2: 62 ± 9.4 | P: Placebo capsules T: EGCG and other catechins included EC, EGC, ECG, and GCG Doses (poly)phenols: T1: Low dose (400 mg/day); T2: High dose (800 mg/day); Duration: 160 days | 5.0 |
| Curtis et al., 2009 [39] | Double-blind parallel P (n = 26); T (n = 26) | Healthy BMI P: 24 ± 3.4; T: 25 ± 3.8 | P: 58 ± 5.8; T: 58 ± 5.5 | P: Placebo capsules T: Elderberry extract (anthocyanins) Dose (poly)phenols: 500 mg/day; Duration: 84 days | 5.5 |
| Zern et al., 2005 [40] | Single blind crossover P (n = 20); T (n = 20) | Healthy BMI P/T: 31 ± 4.6 | P: 40 ± 8.5; T: 59 ± 7.5 | P: Placebo capsules T: Lyophilized grape powder (flavanols, anthocyanins, quercetin, myricetin, kaempferol, and resveratrol) Dose (poly)phenols: 210 mg/day; Duration: 84 days | 4.0 |
| Chai et al., 2012 [41] | Single blinded to researcher, parallel T1 (n = 55); T2 (n = 45) | Healthy BMI T1: 25 ± 4.1; T2: 25 ± 4.6 | T1: 56 ± 5.0; T2: 58 ± 4.0 | T1: Dried apples (75 g) T2: Dried plums (100 g) Dose (poly)phenols: NI; Duration: 180 days | 6.5 |
| Al-Dashti et al., 2019 [34] | Open-label crossover T1 (n = 27); T2 (n = 27) | Healthy BMI T1: 25 ± 6.1; T2: 24 ± 6.8 | T1: 59 ± 5.2; T2: 59 ± 5.2 | Prunes (Prunus domestica L) T1: Low dose (14 g of dried prunes) T2: High dose (42 g of dried prunes) Dose (poly)phenols: NI; Duration: 14 days | 4.5 |
| García-Yu et al., 2020 [42] | Single blinded to researchers, parallel C (n = 66); T (n = 71) | Healthy BMI C: 27 ± 3.1; T: 26 ± 3.8 | C: 58 ± 3.8; T: 57 ± 3.5 | C: Not receiving any interventionT: Dark chocolate, 99% cocoa (10 g). (Poly)phenols: protocatechuic acid, catechins, procyanidins, quercetin Dose(poly)phenols: 65.4 mg/day; Duration: 180 days | 6.5 |
| García-Yu et al., 2021 [43] | Single blinded to researchers, parallel C (n = 61); T (n = 67) | Healthy BMI C: 25 ± 3.1; T: 26 ± 3.8 | C: 57 ± 3.8; T: 57 ± 3.6 | C: Not receiving any intervention T: Dark chocolate, 99% cocoa (10 g). (Poly)phenols: protocatechuic acid, catechins, procyanidins, quercetin Dose (poly)phenols: 65.4 mg/day; Duration: 180 days | 6.5 |
| Estévez-Santiago et al., 2019 [44] | Open label, parallel, with three arms T1 (n = 26); T2 (n = 23); T3 (n = 23) | Healthy BMI T1: 25 ± 2.8; T2: 25 ± 3.3; T3: 25 ± 2.7 | T1: 60 ± 6; T2: 58 ± 6; T3: 60 ± 5 | T1: Xanthophylls (6 mg lutein + 2 mg zeaxanthin/day) T2: Anthocyanins (60 mg/day) T3: Anthocyanins (60 mg/day) and xanthophylls (6 mg lutein + 2 mg zeaxanthin/day); Doses (poly)phenols: 60 mg/day; Duration: 240 days | 4.0 |
| Trius-Soler et al., 2021 [32] | Open label, controlled parallel, with three arms C (n = 14); T1 (n = 16); T2 (n = 7) | Healthy BMI C: 27 ± 4.4; T1: 25 ± 3.7; T2: 30 ± 9.0 | C, T1, T2: 45–70 | C: Not receiving any intervention T1: Beer with alcohol (330 mL/day with 14 g of etanol) T2: Beer without alcohol (660 mL/day) Doses (poly)phenols: T1: 0.359 mg/day of prenylflavonoids; T2: 0.259 mg/day of prenylflavonoids; Duration: 180 days | 4.5 |
| Filip et al., 2015 [28] | Double blind parallel P (n = 21); T (n = 27) | Osteopenia (mix cholesterol levels) BMI P: 28 ± 4.0; T: 26 ± 4.3 | P: 59 ± 5.6; T: 60 ± 4.4 | P: Placebo capsules T: Calcium supplement (1000 mg Ca) and olive extract (250 mg/day) Dose: >100 mg oleuropein; Duration: 365 days | 7.5 |
| Wang-Polagruto et al., 2006 [25] | Double-blind parallel T1 (n = 16); T2 (n = 16) | Dyslipidaemia (high cholesterol) BMI T1: 25 ± 3.2; T2: 25 ± 4.0 | T1: 55 ± 6.8; T2: 58 ± 8.8 | Flavanol cocoa beverage T1: Low flavanol dose T2: High flavanol dose Doses (poly)phenols: T1: 43 mg/day; T2: 446 mg/day; Duration: 42 days | 5.5 |
| Naissides et al., 2006ab [26,27] | Open label, parallel, with three arms C (n = 16); T1 (n = 15); T2 (n = 14) | Dyslipidaemia (high cholesterol) BMI C: 27 ± 4.8; T1: 26 ± 6.0; T2: 26 ± 3.5 | C: 59 ± 5.6; T1: 58 ± 4.9; T2: 58 ± 5.0 | C: Water (400 mL) T1: Non-alcoholic red wine (400 mL) T2: Alcoholic red wine (400 mL) Doses (poly)phenols: 1000 mg/day red wine (poly) phenols, each treatment group; Duration: 42 days | 6.0 /5.0 |
| Aubertin-Leheudre et al., 2008 [45] | Double-blind parallel P (n = 18); T (n = 21) | Obese BMI P: 31 ± 4.5; T: 33 ± 4.8 | P: 57 ± 5.6; T: 58 ± 5.2 | P: Placebo capsules T: Isoflavone capsules containing 70 mg isoflavones extracted from natural soy (44 mg daidzein, 16 mg glycitein, and 10 mg genistein) Dose (poly)phenols: 70 mg/day; Duration: 180 days | 5.5 |
| Dostal et al., 2016 [33] | Double-blind parallel P (n = 120); T (n = 117) | Obese and overweight BMI P: 28 ± 2.7; T: 29 ± 3.0 | P: 61 ± 5.2; T: 61 ± 4.9 | P: Placebo capsules T: Decaffeinated green tea extract Dose (poly)phenols: 1315 mg catechins/day; Duration: 365 days | 7.5 |
| Johnson et al., 2015 [29] | Double-blind, parallel with two arms P (n = 20); T (n = 20) | Seated blood pressure ≥125/85 mm Hg but ≤160/90 mm Hg BMI P: 33 ± 6.5; T: 30 ± 5.9 | P: 57 ± 4.8; T: 60 ± 4.6 | P: Placebo powder T: Blueberry powder (22 g) Dose (poly)phenols: Phenolics (845 mg/day) and anthocyanins (469 mg/days); Duration: 56 days | 7.0 |
| Johnson et al., 2017 [30] | Double-blind parallel with two arms P (n = 20); T (n = 20) | Pre- and stage 1-hypertension BMI NI | P, T: 45–65 | P: Placebo capsules T: Blueberry powder (22 g) Dose (poly)phenols: Phenolics (845 mg/day) and anthocyanins (469 mg/days); Duration: 56 days | 7.5 |
| D’Anna et al., 2014 [31] | Open parallel P (n = 21); T (n = 22) | MetS BMI P: 34 ± 3.9; T: 32 ± 3.8 | P: 56 ± 4.8; T: 56 ± 3.8 | P: Placebo powder T: Cocoa (poly)phenols (30 mg), soy isoflavones (80 mg) and myoinositol Dose (poly)phenols: 110 mg/day; Duration: 180 days | 5.5 |
3.3. Analysis of the Results of the Selected Studies
3.4. Changes in the Glucose Homeostasis Indicators
3.5. Changes in the Lipid Profile
3.6. Changes in Blood Pressure (BP)
3.7. Changes in the Inflammatory, Endothelial Function and Oxidative Stress Biomarkers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Cardiovascular Diseases (CVDs). Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 11 October 2021).
- Santoro, N.; Randolph, J.F., Jr. Reproductive Hormones and the Menopause Transition. Obstet. Gynecol. Clin. N. Am. 2011, 38, 455–466. [Google Scholar] [CrossRef] [Green Version]
- Maas, A.H.E.M.; Rosano, G.; Cifkova, R.; Chieffo, A.; van Dijken, D.; Hamoda, H.; Kunadian, V.; Laan, E.; Lambrinoudaki, I.; Maclaran, K.; et al. Cardiovascular health after menopause transition, pregnancy disorders, and other gynaecologic conditions: A consensus document from European cardiologists, gynaecologists, and endocrinologists. Eur. Heart J. 2021, 42, 967–984. [Google Scholar] [CrossRef]
- Hallajzadeh, J.; Khoramdad, M.; Izadi, N.; Karamzad, N.; Almasi-Hashiani, A.; Ayubi, E.; Qorbani, M.; Pakzad, R.; Hasanzadeh, A.; Sullman, M.J.M.; et al. Metabolic syndrome and its components in premenopausal and postmenopausal women: A comprehensive systematic review and meta-analysis on observational studies. Menopause 2018, 25, 1155–1164. [Google Scholar] [CrossRef]
- Chopra, S.; Sharma, K.A.; Ranjan, P.; Malhotra, A.; Vikram, N.K.; Kumari, A. Ight Management Module for Perimenopausal Women: A Practical Guide for Gynecologists. J. Mid-Life Health 2019, 10, 165. [Google Scholar]
- Farias, D.D.P.; Fernandez de Araújo, F.; Neri-Numa, I.A.; Pastore, G.M. Antidiabetic potential of dietary polyphenols: A mechanistic review. Food Res. Int. 2021, 145, 110383. [Google Scholar] [CrossRef]
- Swarup, S.; Goyal, A.; Grigorova, Y.; Zeltser, R. Metabolic Syndrome. Available online: https://www.ncbi.nlm.nih.gov/books/NBK459248/?report=classic (accessed on 1 November 2020).
- Fernández-Sánchez, A.; Madrigal-Santillán, E.; Bautista, M.; Esquivel-Soto, J.; Morales-González, Á.; Esquivel-Chirino, C.; Durante-Montiel, I.; Sánchez-Rivera, G.; Valadez-Vega, C.; Morales-González, J.A. Inflammation, Oxidative Stress, and Obesity. Int. J. Mol. Sci. 2011, 12, 3117–3132. [Google Scholar] [CrossRef] [Green Version]
- Silva, T.R.; Oppermann, K.; Reis, F.M.; Spritzer, P.M. Nutrition in Menopausal Women: A Narrative Review. Nutrients 2021, 13, 2149. [Google Scholar] [CrossRef] [PubMed]
- Rossouw, J.E.; Anderson, G.L.; Prentice, R.L.; LaCroix, A.Z.; Kooperberg, C.; Stefanick, M.L.; Jackson, R.D.; Beresford, S.A.; Howard, B.V.; Johnson, K.C.; et al. Risks and Benefits of Estrogen Plus Progestin in Healthy Postmenopausal Women. JAMA 2002, 288, 321–333. [Google Scholar] [CrossRef] [PubMed]
- Hemler, E.C.; Hu, F.B. Plant-Based Diets for Personal, Population, and Planetary Health. Adv. Nutr. 2019, 10, S275–S283. [Google Scholar] [CrossRef]
- Koes, R.E.; Quattrocchio, F.; Mol, J.N.M. The Flavonoid Biosynthetic Pathway in Plants: Function and Evolution. Plant Metab. Biotechnol. 1994, 16, 123–132. [Google Scholar] [CrossRef]
- Del Rio, D.; Rodriguez-Mateos, A.; Spencer, J.P.E.; Tognolini, M.; Borges, G.; Crozier, A. Dietary (Poly)phenolics in Human Health: Structures, Bioavailability, and Evidence of Protective Effects Against Chronic Diseases. Antioxid. Redox Signal. 2013, 18, 1818–1892. [Google Scholar] [CrossRef] [Green Version]
- Frank, J.; Fukagawa, N.F.; Bilia, A.R.; Johnson, E.J.; Kwon, O.; Prakash, V.; Miyazawa, T.; Clifford, M.N.; Kay, C.D.; Crozier, A.; et al. Terms and nomenclature used for plant-derived components in nutrition and related research: Efforts toward harmonization. Nutr. Rev. 2020, 78, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Vetrani, C.; Costabile, G.; Vitale, M.; Giacco, R. (Poly)phenols and cardiovascular diseases: Looking in to move forward. J. Funct. Foods 2020, 71, 104013. [Google Scholar] [CrossRef]
- Weaver, S.R.; Rendeiro, C.; McGettrick, H.M.; Philp, A.; Lucas, S.J.E. Fine wine or sour grapes? A systematic review and meta-analysis of the impact of red wine polyphenols on vascular health. Eur. J. Nutr. 2020, 60, 1–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Sarrías, A.; Combet, E.; Pinto, P.; Mena, P.; Dall’Asta, M.; Garcia-Aloy, M.; Rodríguez-Mateos, A.; Gibney, E.R.; Dumont, J.; Massaro, M.; et al. A Systematic Review and Meta-Analysis of the Effects of Flavanol-Containing Tea, Cocoa and Apple Products on Body Composition and Blood Lipids: Exploring the Factors Responsible for Variability in Their Efficacy. Nutrients 2017, 9, 746. [Google Scholar] [CrossRef]
- García-Conesa, M.T.; Larrosa, M. Polyphenol-Rich foods for Human Health and Disease. Nutrients 2020, 12, 400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Conesa, M.-T.; Chambers, K.; Combet, E.; Pinto, P.; Garcia-Aloy, M.; Andrés-Lacueva, C.; de Pascual-Teresa, S.; Pedro, M.; Ristic, A.K.; Hollands, W.J.; et al. Meta-Analysis of the Effects of Foods and DerivedProducts Containing Ellagitannins and Anthocyaninson Cardiometabolic Biomarkers: Analysis of FactorsInfluencing Variability of the Individual Responses. Int. J. Mol. Sci. 2018, 19, 694. [Google Scholar] [CrossRef] [Green Version]
- Raimundo, A.F.; Félix, F.; Andrade, R.; García-Conesa, M.-T.; González-Sarrías, A.; Gilsa-Lopes, J.; do Ó, D.; Ribeiro, R.; Rodriguez-Mateos, A.; Santos, C.N.; et al. Combined effect of interventions with pure or enriched mixtures of (poly)phenols and anti-diabetic medication in type 2 diabetes management: A meta-analysis of randomized controlled human trials. Eur. J. Nutr. 2020, 59, 1329–1343. [Google Scholar] [CrossRef] [PubMed]
- Morand, C.; De Roos, B.; Garcia-Conesa, M.T.; Gibney, E.R.; Landberg, R.; Manach, C.; Milenkovic, D.; Rodriguez-Mateos, A.; Van de Wiele, T.; Tomas-Barberan, F. Why interindividual variation in response to consumption of plant food bioactives matters for future personalised nutrition. Proc. Nutr. Soc. 2020, 79, 225–235. [Google Scholar] [CrossRef]
- De Roos, B.; Aura, A.-M.; Bronze, M.; Cassidy, A.; Conesa, M.-T.G.; Gibney, E.R.; Greyling, A.; Kaput, J.; Kerem, Z.; Knežević, N.; et al. Targeting the delivery of dietary plant bioactives to those who would benefit most: From science to practical applications. Eur. J. Nutr. 2019, 58, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; E Brennan, S.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; Updated March 2011; The Cochrane Collaboration: London, UK, 2011; Available online: www.handbook.cochrane.org (accessed on 1 April 2016).
- Wang-Polagruto, J.F.; Villablanca, A.C.; Polagruto, J.A.; Lee, L.; Holt, R.R.; Schrader, H.R.; Ensunsa, J.L.; Steinberg, F.M.; Schmitz, H.H.; Keen, C.L. Chronic Consumption of Flavanol-rich Cocoa Improves Endothelial Function and Decreases Vascular Cell Adhesion Molecule in Hypercholesterolemic Postmenopausal Women. J. Cardiovasc. Pharmacol. 2006, 47, S177–S186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naissides, M.; Pal, S.; Mamo, J.; James, A.P.; Dhaliwal, S. The effect of chronic consumption of red wine polyphenols on vascular function in postmenopausal women. Eur. J. Clin. Nutr. 2006, 60, 740–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naissides, M.; Mamo, J.C.L.; James, A.P.; Pal, S. The effect of chronic consumption of red wine on cardiovascular disease risk factors in postmenopausal women. Atherosclerosis 2006, 185, 438–445. [Google Scholar] [CrossRef]
- Filip, R.; Possemiers, S.; Heyerick, A.; Pinheiro, I.; Raszewski, G.; Davicco, M.-J.; Coxam, V. Twelve-month consumption of a polyphenol extract from olive (Olea europaea) in a double blind, randomized trial increases serum total osteocalcin levels and improves serum lipid profiles in postmenopausal women with osteopenia. J. Nutr. Health Aging 2015, 19, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.A.; Figueroa, A.; Navaei, N.; Wong, A.; Kalfon, R.; Ormsbee, L.T.; Feresin, R.G.; Elam, M.L.; Hooshmand, S.; Payton, M.E.; et al. Daily Blueberry Consumption Improves Blood Pressure and Arterial Stiffness in Postmenopausal Women with Pre- and Stage 1-Hypertension: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. J. Acad. Nutr. Diet. 2015, 115, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.A.; Feresin, R.G.; Navaei, N.; Figueroa, A.; Elam, M.L.; Akhavan, N.S.; Hooshmand, S.; Pourafshar, S.; Payton, M.E.; Arjmandi, B.H. Effects of daily blueberry consumption on circulating biomarkers of oxidative stress, inflammation, and antioxidant defense in postmenopausal women with pre- and stage 1-hypertension: A randomized controlled trial. Food Funct. 2017, 8, 372–380. [Google Scholar] [CrossRef] [PubMed]
- D’Anna, R.; Santamaria, A.; Cannata, M.L.; Interdonato, M.L.; Giorgianni, G.M.; Granese, R.; Corrado, F.; Bitto, A. Effects of a New Flavonoid and Myo-Inositol Supplement on Some Biomarkers of Cardiovascular Risk in Postmenopausal Women: A Randomized Trial. Int. J. Endocrinol. 2014, 2014, 653561. [Google Scholar] [CrossRef]
- Trius-Soler, M.; Marhuenda-Muñoz, M.; Laveriano-Santos, E.P.; Martínez-Huélamo, M.; Sasot, G.; Storniolo, C.E.; Estruch, R.M.; Lamuela-Raventós, R.; Tresserra-Rimbau, A. Moderate Consumption of Beer (with and without Ethanol) and Menopausal Symptoms: Results from a Parallel Clinical Trial in Postmenopausal Women. Nutrients 2021, 13, 2278. [Google Scholar] [CrossRef]
- Dostal, A.M.; Samavat, H.; Espejo, L.; Arikawa, A.Y.; Stendell-Hollis, N.R.; Kurzer, M.S. Green Tea Extract and Catechol-O-Methyltransferase Genotype Modify Fasting Serum Insulin and Plasma Adiponectin Concentrations in a Randomized Controlled Trial of Overweight and Obese Postmenopausal Women. J. Nutr. 2016, 146, 38–45. [Google Scholar] [CrossRef] [Green Version]
- Al-Dashti, Y.A.; Holt, R.R.; Carson, J.G.; Keen, C.L.; Hackman, R.M. Effects of Short-Term Dried Plum (Prune) Intake on Markers of Bone Resorption and Vascular Function in Healthy Postmenopausal Women: A Randomized Crossover Trial. J. Med. Food 2019, 22, 982–992. [Google Scholar] [CrossRef]
- Myasoedova, V.A.; Kirichenko, T.V.; Melnichenko, A.A.; Orekhova, V.A.; Ravani, A.; Poggio, P.; Sobenin, I.A.; Bobryshev, Y.V.; Orekhov, A.N. Anti-Atherosclerotic Effects of a Phytoestrogen-Rich Herbal Preparation in Postmenopausal Women. Int. J. Mol. Sci. 2016, 17, 1318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, S.-Y.; Shaw, N.-S.; Tsai, K.-S.; Chen, C.-Y. The Hypoglycemic Effects of Soy Isoflavones on Postmenopausal Women. J. Women’s Health 2004, 13, 1080–1086. [Google Scholar] [CrossRef] [PubMed]
- Sathyapalan, T.; Aye, M.; Rigby, A.S.; Thatcher, N.J.; Dargham, S.R.; Kilpatrick, E.S.; Atkin, S.L. Soy isoflavones improve cardiovascular disease risk markers in women during the early menopause. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 691–697. [Google Scholar] [CrossRef]
- Wu, A.H.; Spicer, D.; Stanczyk, F.Z.; Tseng, C.-C.; Yang, C.S.; Pike, M.C. Effect of 2-Month Controlled Green Tea Intervention on Lipoprotein Cholesterol, Glucose, and Hormone Levels in Healthy Postmenopausal Women. Cancer Prev. Res. 2012, 5, 393–402. [Google Scholar] [CrossRef] [Green Version]
- Curtis, P.J.; Kroon, P.A.; Hollands, W.J.; Walls, R.; Jenkins, G.; Kay, C.D.; Cassidy, A. Cardiovascular Disease Risk Biomarkers and Liver and Kidney Function Are Not Altered in Postmenopausal Women after Ingesting an Elderberry Extract Rich in Anthocyanins for 12 Weeks. J. Nutr. 2009, 139, 2266–2271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zern, T.L.; Wood, R.J.; Greene, C.; West, K.L.; Liu, Y.; Aggarwal, D.; Shachter, N.S.; Fernandez, M.L. Grape Polyphenols Exert a Cardioprotective Effect in Pre- and Postmenopausal Women by Lowering Plasma Lipids and Reducing Oxidative Stress. J. Nutr. 2005, 135, 1911–1917. [Google Scholar] [CrossRef] [Green Version]
- Chai, S.C.; Hooshmand, S.; Saadat, R.L.; Payton, M.E.; Brummel-Smith, K.; Arjmandi, B.H. Daily Apple versus Dried Plum: Impact on Cardiovascular Disease Risk Factors in Postmenopausal Women. J. Acad. Nutr. Diet. 2012, 112, 1158–1168. [Google Scholar] [CrossRef]
- Garcia-Yu, I.A.; Garcia-Ortiz, L.; Gomez-Marcos, M.A.; Rodriguez-Sanchez, E.; Agudo-Conde, C.; Gonzalez-Sanchez, J.; Maderuelo-Fernandez, J.A.; Recio-Rodriguez, J.I. Effects of Cocoa-Rich Chocolate on Blood Pressure, Cardiovascular Risk Factors, and Arterial Stiffness in Postmenopausal Women: A Randomized Clinical Trial. Nutrients 2020, 12, 1758. [Google Scholar] [CrossRef]
- Garcia-Yu, I.A.; Garcia-Ortiz, L.; Gomez-Marcos, M.A.; Rodriguez-Sanchez, E.; Lugones-Sanchez, C.; Maderuelo-Fernandez, J.A.; Recio-Rodriguez, J.I. Cocoa-rich chocolate and body composition in postmenopausal women: A randomised clinical trial. Br. J. Nutr. 2020, 125, 548–556. [Google Scholar] [CrossRef]
- Estévez-Santiago, R.; Silván, J.M.; Can-Cauich, C.A.; Veses, A.M.; Alvarez-Acero, I.; Martinez-Bartolome, M.A.; San-Román, R.; Cámara, M.; Olmedilla-Alonso, B.; De Pascual-Teresa, S. Lack of a Synergistic Effect on Cardiometabolic and Redox Markers in a Dietary Supplementation with Anthocyanins and Xanthophylls in Postmenopausal Women. Nutrients 2019, 11, 1533. [Google Scholar] [CrossRef] [Green Version]
- Aubertin-Leheudre, M.; Lord, C.; Khalil, A.; Dionne, I.J. Isoflavones and Clinical Cardiovascular Risk Factors in Obese Postmenopausal Women: A Randomized Double-Blind Placebo-Controlled Trial. J. Women’s Health 2008, 17, 1363–1369. [Google Scholar] [CrossRef]
- Stachowiak, G.; Pertyński, T.; Pertyńska-Marczewska, M. Metabolic disorders in menopause. Prz. Menopauzalny Menopause Rev. 2015, 14, 59–64. [Google Scholar] [CrossRef]
- El Khoudary, S.R.; Ceponiene, I.; Samargandy, S.; Stein, J.H.; Li, D.; Tattersall, M.C.; Budoff, M. HDL (High-Density Lipoprotein) Metrics and Atherosclerotic Risk in Women: Do Menopause Characteristics Matter? MESA. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 2236–2244. [Google Scholar] [CrossRef] [PubMed]
- Ko, S.-H.; Hyun-Sook, K. Menopause-Associated Lipid Metabolic Disorders and Foods Beneficial for Postmenopausal Women. Nutr. Hosp. 2020, 12, 202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Conesa, M.T. Dietary Polyphenols against Metabolic Disorders: How Far Have We Progressed in the Understanding of the Molecular Mechanisms of Action of These Compounds? Crit. Rev. Food Sci. Nutr. 2017, 57, 1769–1786. [Google Scholar] [CrossRef] [PubMed]
- Zamora-Ros, R.; Rabassa, M.; Cherubini, A.; Urpi-Sarda, M.; Bandinelli, S.; Ferrucci, L.; Andres-Lacueva, C. High Concentrations of a Urinary Biomarker of Polyphenol Intake Are Associated with Decreased Mortality in Older Adults. J. Nutr. 2013, 143, 1445–1450. [Google Scholar] [CrossRef] [Green Version]
- Tresserra-Rimbau, A.; Rimm, E.B.; Medina-Remón, A.; Martínez-González, M.A.; de la Torre, R.; Corella, D.; Salas-Salvadó, J.; Gómez-Gracia, E.; Lapetra, J.; Arós, F.; et al. Inverse association between habitual polyphenol intake and incidence of cardiovascular events in the PREDIMED study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 639–647. [Google Scholar] [CrossRef]
- Rangel-Huerta, O.D.; Pastor-Villaescusa, B.; Aguilera, C.M.; Gil, A. A Systematic Review of the Efficacy of Bioactive Compounds in Cardiovascular Disease: Phenolic Compounds. Nutrients 2015, 7, 5177–5216. [Google Scholar] [CrossRef] [Green Version]
- Menezes, R.; Rodriguez-Mateos, A.; Kaltsatou, A.; González-Sarrías, A.; Greyling, A.; Giannaki, C.; Andres-Lacueva, C.; Milenkovic, D.; Gibney, E.R.; Dumont, J.; et al. Impact of Flavonols on Cardiometabolic Biomarkers: A Meta-Analysis of Randomized Controlled Human Trials to Explore the Role of Inter-Individual Variability. Nutrients 2017, 9, 117. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Zhang, Y.; Li, H.; Deng, Z.; Tsao, R. A review on insoluble-bound phenolics in plant-based food matrix and their contribution to human health with future perspectives. Trends Food Sci. Technol. 2020, 105, 347–362. [Google Scholar] [CrossRef]
- Kasprzak-Drozd, K.; Oniszczuk, T.; Stasiak, M.; Oniszczuk, A. Beneficial Effects of Phenolic Compounds on Gut Microbiota and Metabolic Syndrome. Int. J. Mol. Sci. 2021, 22, 3715. [Google Scholar] [CrossRef] [PubMed]
- Hills, R.K.; Daniels, J. Assessing new interventions in women’s health. Best Pract. Res. Clin. Obstet. Gynaecol. 2006, 20, 713–728. [Google Scholar] [CrossRef]
- Nikolic, M.; Ristic, A.K.; González-Sarrías, A.; Istas, G.; Urpi-Sarda, M.; Dall’Asta, M.; Monfoulet, L.-E.; Cloetens, L.; Bayram, B.; Tumolo, M.R.; et al. Improving the reporting quality of intervention trials addressing the inter-individual variability in response to the consumption of plant bioactives: Quality index and recommendations. Eur. J. Nutr. 2019, 58, 49–64. [Google Scholar] [CrossRef] [Green Version]
- Manach, C.; Milenkovic, D.; Van de Wiele, T.; Rodriguez-Mateos, A.; de Roos, B.; Garcia-Conesa, M.T.; Landberg, R.; Gibney, E.R.; Heinonen, M.; Tomás-Barberán, F.; et al. Addressing the Inter-Individual Variation in Response Toconsumption of Plant Food Bioactives: Towards a Betterunderstanding of Their Role in Healthy Aging Andcardiometabolic Risk Reduction. Mol. Nutr. Food Res. 2017, 61, 1600557. [Google Scholar] [CrossRef] [Green Version]
- Di Lorenzo, C.; Colombo, F.; Biella, S.; Stockley, C.; Restani, P. Polyphenols and Human Health: The Role of Bioavailability. Nutrients 2021, 13, 273. [Google Scholar] [CrossRef] [PubMed]
- Mathew, T.; Tadi, P. Blood Glucose Monitoring. Available online: https://www.ncbi.nlm.nih.gov/books/NBK555976/ (accessed on 11 August 2021).
- American College of Cardiology. Guidelines & Clinical Documents. Available online: https://www.acc.org/guidelines (accessed on 23 September 2021).
- Hardy, S.T.; Loehr, L.R.; Butler, K.R.; Chakladar, S.; Chang, P.P.; Folsom, A.R.; Heiss, G.; MacLehose, R.F.; Matsushita, K.; Avery, C.L. Reducing the Blood Pressure–Related Burden of Cardiovascular Disease: Impact of Achievable Improvements in Blood Pressure Prevention and Control. J. Am. Heart Assoc. 2015, 4, e002276. [Google Scholar] [CrossRef] [Green Version]
- Carr, S.S.; Hooper, A.J.; Sullivan, D.R.; Burnett, J.R. Non-HDL-cholesterol and apolipoprotein B compared with LDL-cholesterol in atherosclerotic cardiovascular disease risk assessment. Pathology 2019, 51, 148–154. [Google Scholar] [CrossRef]
- Whelton, P.; He, J.; Appel, L.J.; Cutler, J.A.; Havas, S.; Kotchen, T.; Roccella, E.J.; Stout, R.; Vallbona, C.; Winston, M.C.; et al. Primary Prevention of Hypertension: Clinical and Public Health Advisory from the National High Blood Pressure Education Program. J. Am. Med. Assoc. 2002, 288, 1882–1888. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Wald, N.; Morris, J. Lowering blood pressure to prevent myocardial infarction and stroke: A new preventive strategy. Int. J. Technol. Assess. Health Care 2005, 21, 145. [Google Scholar] [CrossRef]
- American Heart Association. Guidelines & Statements. Available online: https://professional.heart.org/en/guidelines-and-statements (accessed on 23 September 2021).
- European Society of Hypertension. Blood Pressure Monitoring. Available online: https://www.eshonline.org/guidelines/blood-pressure-monitoring/ (accessed on 23 September 2021).
- European Society of Cardiology. Clinical Practice Guidelines. Available online: https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines (accessed on 23 September 2021).
- Pearson, T.A.; Mensah, G.A.; Alexander, R.W.; Anderson, J.L.; Cannon, R.O., III; Criqui, M.; Fadl, Y.Y.; Fortmann, S.P.; Hong, Y.; Myers, G.L.; et al. Markers of Inflammation and Cardiovascular Disease: Application to Clinical and Public Health Practice: A Statement for Healthcare Professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation 2003, 107, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, X.-M.T.; Lane, J.; Smith, B.R.; Nguyen, N.T. Changes in Inflammatory Biomarkers across Weight Classes in a Representative US Population: A Link between Obesity and Inflammation. J. Gastrointest. Surg. 2009, 13, 1205–1212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- C-reactive Protein Concentrations as a Marker of Inflammation or Infection for Interpreting Biomarkers of Micronutrient Status; Vitamin and Mineral Nutrition Information System; World Health Organization: Geneva, Switzerland, 2014; (WHO/NMH/NHD/EPG/14.7); Available online: http://apps.who.int/iris/bitstream/10665/133708/1/WHO_NMH_NHD_EPG_14.7_eng.pdf?ua=1 (accessed on 28 September 2021).
- Wyczalkowska-Tomasik, A.; Czarkowska-Paczek, B.; Zielenkiewicz, M.; Paczek, L. Inflammatory Markers Change with Age, but do not Fall Beyond Reported Normal Ranges. Arch. Immunol. Ther. Exp. 2015, 64, 249–254. [Google Scholar] [CrossRef] [Green Version]
- Marcos-Pérez, D.; Sánchez-Flores, M.; Maseda, A.; Lorenzo-López, L.; Millán-Calenti, J.C.; Gostner, J.M.; Fuchs, D.; Pasaro, E.; Laffon, B.; Valdiglesias, V. Frailty in Older Adults Is Associated with Plasma Concentrations of Inflammatory Mediators but Not With Lymphocyte Subpopulations. Front. Immunol. 2018, 9, 1056. [Google Scholar] [CrossRef] [Green Version]
- Jabłońska, A.; Zagrapan, B.; Neumayer, C.; Eilenberg, W.; Scheuba, A.; Brostjan, C.; Demyanets, S.; Klinger, M.; Nanobachvili, J.; Huk, I. Polymorphisms in the IL-6 and TNF-α gene are associated with an increased risk of abdominal aortic aneurysm. Int. J. Cardiol. 2020, 329, 192–197. [Google Scholar] [CrossRef]
- Pahwa, R.; Goyal, A.; Bansal, P.; Jialal, I. Chronic Inflammation. Available online: https://europepmc.org/article/nbk/nbk493173#free-full-text (accessed on 11 August 2021).
- Mulhem, A.; Moulla, Y.; Klöting, N.; Ebert, T.; Tönjes, A.; Fasshauer, M.; Dietrich, A.; Schön, M.R.; Stumvoll, M.; Richter, V.; et al. Circulating cell adhesion molecules in metabolically healthy obesity. Int. J. Obes. 2020, 45, 331–336. [Google Scholar] [CrossRef]
- Ridker, P.M.; Buring, J.E.; Cook, N.R.; Rifai, N. C-Reactive Protein, the Metabolic Syndrome, and Risk of Incident Cardiovascular Events: An 8-Year Follow-Up of 14 719 Initially Healthy American Women. Circulation 2003, 107, 391–397. [Google Scholar] [CrossRef]
- Monserrat-Mesquida, M.; Quetglas-Llabrés, M.; Bouzas, C.; Capó, X.; Mateos, D.; Ugarriza, L.; Tur, J.A.; Sureda, A. Peripheral Blood Mononuclear Cells Oxidative Stress and Plasma Inflammatory Biomarkers in Adults with Normal Weight, Overweight and Obesity. Antioxidants 2021, 10, 813. [Google Scholar] [CrossRef]
- Todd, J.; Simpson, P.; Estis, J.; Torres, V.; Wub, A.H.B. Reference range and short- and long-term biological variation of interleukin (IL)-6, IL-17A and tissue necrosis factor-alpha using high sensitivity assays. Cytokine 2013, 64, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Ashcheulova, T.; Gerasimchuk, N.; Kovalyova, O.; Honchar, O. Beneficial effects of combined therapy with lacidipine and candesartan in obese hypertensive patients. Rom. J. Intern. Med. 2018, 56, 257–264. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, R.S.; Sharif, D.A.; Jaf, M.Y.; Hussain, A.H. Tumor Necrosis Factor Alpha (TNF- α), as a Biomarker for Disease Activity among Iraqi Patients with Generalized Vitiligo, Independent on Disease Duration and Extent of Skin Involvement. Med. Sci. 2020, 24, 4295–4302. [Google Scholar] [CrossRef]
- Bulló, M.; Garcia-Lorda, P.; Salas-Salvadó, J. Plasma soluble tumor necrosis factor alpha receptors and leptin levels in normal-weight and obese women: Effect of adiposity and diabetes. Eur. J. Endocrinol. 2002, 146, 325–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olszanecka-Glinianowicz, M.; Zahorska-Markiewicz, B.; Janowska, J.; Zurakowski, A. Serum concentrations of nitric oxide, tumor necrosis factor (TNF)-α and TNF soluble receptors in women with overweight and obesity. Metabolism 2004, 53, 1268–1273. [Google Scholar] [CrossRef]
- Marques-Vidal, P.; Bochud, M.; Bastardot, F.; Lüscher, T.; Ferrero, F.; Gaspoz, J.-M.; Paccaud, F.; Urwyler, A.; Von Känel, R.; Hock, C.; et al. Levels and Determinants of Inflammatory Biomarkers in a Swiss Population-Based Sample (CoLaus Study). PLoS ONE 2011, 6, e21002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues, K.F.; Pietrani, N.T.; Bosco, A.A.; Campos, F.M.F.; Sandrim, V.C.; Gomes, K.B. IL-6, TNF-α, and IL-10 levels/polymorphisms and their association with type 2 diabetes mellitus and obesity in Brazilian individuals. Arch. Endocrinol. Metab. 2017, 61, 438–446. [Google Scholar] [CrossRef] [Green Version]
- Zafar, U.; Khaliq, S.; Ahmad, H.U.; Lone, K.P. Serum profile of cytokines and their genetic variants in metabolic syndrome and healthy subjects: A comparative study. Biosci. Rep. 2019, 39. [Google Scholar] [CrossRef] [Green Version]
- Mallard, A.R.; Hollekim-Strand, S.M.; Ingul, C.B.; Coombes, J.S. High day-to-day and diurnal variability of oxidative stress and inflammation biomarkers in people with type 2 diabetes mellitus and healthy individuals. Redox Rep. 2020, 25, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Emara, M.; El-Edel, R.; Fathy, W.M.; Aboelkhair, N.T.; Watany, M.M.; Abou-Elela, D.H. Study the Association of Tumor Necrosis Factor Promoter Polymorphism with Type 2 Diabetic Nephropathy. Mediat. Inflamm. 2020, 2020, 1–9. [Google Scholar] [CrossRef]
- Mohammadi, M.H.; Gozashti, M.; Aghadavood, M.; Mehdizadeh, M.R.; Hayatbakhsh, M.M. Clinical Significance of Serum IL-6 and TNF-α Levels in Patients with Metabolic Syndrome. Rep. Biochem. Mol. Biol. 2017, 6, 74–79. [Google Scholar] [PubMed]
- Hussain, T.; Tan, B.; Yin, Y.; Blachier, F.; Tossou, M.C.B.; Rahu, N. Oxidative Stress and Inflammation: What Polyphenols Can Do for Us? Oxidative Med. Cell. Longev. 2016, 2016, 7432797. [Google Scholar] [CrossRef] [Green Version]
- Holvoet, P.; Macy, E.; Landeloos, M.; Jones, D.; Nancy, J.S.; Van De Werf, F.; Tracy, R.P. Analytical Performance and Diagnostic Accuracy of Immunometric Assays for the Measurement of Circulating Oxidized LDL. Clin. Chem. 2006, 52, 760–764. [Google Scholar] [CrossRef]
- Couillard, C.; Ruel, G.; Archer, W.R.; Pomerleau, S.; Bergeron, J.; Couture, P.; Lamarche, B.; Bergeron, N. Circulating Levels of Oxidative Stress Markers and Endothelial Adhesion Molecules in Men with Abdominal Obesity. J. Clin. Endocrinol. Metab. 2005, 90, 6454–6459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chae, J.S.; Kim, O.Y.; Paik, J.K.; Kang, R.; Seo, W.J.; Jeong, T.-S.; Sweeney, G.; Lee, S.-H.; Lee, J.H. Association of Lp-PLA2 activity and LDL size with interleukin-6, an inflammatory cytokine and oxidized LDL, a marker of oxidative stress, in women with metabolic syndrome. Atherosclerosis 2011, 218, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Paik, J.K.; Chae, J.S.; Kang, R.; Kwon, N.; Lee, S.-H.; Lee, J.H. Effect of age on atherogenicity of LDL and inflammatory markers in healthy women. Nutr. Metab. Cardiovasc. Dis. 2012, 23, 967–972. [Google Scholar] [CrossRef]
- Gross, M.; Steffes, M.; Jacobs, D.R.; Yu, X.; Lewis, L.; Lewis, C.E.; Loria, C.M. Plasma F2-Isoprostanes and Coronary Artery Calcification: The CARDIA Study. Clin. Chem. 2005, 51, 125–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milne, G.L.; Sanchez, S.C.; Musiek, E.S.; Morrow, J.D. Quantification of F2-isoprostanes as a biomarker of oxidative stress. Nat. Protoc. 2007, 2, 221–226. [Google Scholar] [CrossRef]
- Gaskins, A.J.; Rovner, A.J.; Mumford, S.L.; Yeung, E.; Browne, R.W.; Trevisan, M.; Perkins, N.J.; Wactawski-Wende, J.; Schisterman, E.F.; for the BioCycle Study Group. Adherence to a Mediterranean diet and plasma concentrations of lipid peroxidation in premenopausal women. Am. J. Clin. Nutr. 2010, 92, 1461–1467. [Google Scholar] [CrossRef] [Green Version]
- Esterbauer, H.; Gebicki, J.; Puhl, H.; Jürgens, G. The role of lipid peroxidation and antioxidants in oxidative modification of LDL. Free Radic. Biol. Med. 1992, 13, 341–390. [Google Scholar] [CrossRef]
- Stojanov, M.; Stefanovic, A.; Dzingalasevic, G.; Ivanisevic, J.; Miljkovic, M.; Mandic-Radic, S.; Prostran, M. Total bilirubin in young men and women: Association with risk markers for cardiovascular diseases. Clin. Biochem. 2013, 46, 1516–1519. [Google Scholar] [CrossRef] [PubMed]
- Arab, K.; Steghens, J.-P. Plasma lipid hydroperoxides measurement by an automated xylenol orange method. Anal. Biochem. 2004, 325, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Hui, S.-P.; Murai, T.; Yoshimura, T.; Chiba, H.; Nagasaka, H.; Kurosawa, T. Improved HPLC assay for lipid peroxides in human plasma using the internal standard of hydroperoxide. Lipids 2005, 40, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Ide, T.; Tsutsui, H.; Ohashi, N.; Hayashidani, S.; Suematsu, N.; Tsuchihashi, M.; Tamai, H.; Takeshita, A. Greater Oxidative Stress in Healthy Young Men Compared With Premenopausal Women. Arter. Thromb. Vasc. Biol. 2002, 22, 438–442. [Google Scholar] [CrossRef] [Green Version]
- Manso, C.; Wróblewski, F. Glutathione Reductase Activity in Blood and Body Fluids. J. Clin. Investig. 1958, 37, 214–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnabel, R.; Lackner, K.J.; Rupprecht, H.J.; Espinola-Klein, C.; Torzewski, M.; Lubos, E.; Bickel, C.; Cambien, F.; Tiret, L.; Münzel, T.; et al. Glutathione Peroxidase-1 and Homocysteine for Cardiovascular Risk Prediction: Results from the AtheroGeneStudy. J. Am. Coll. Cardiol. 2005, 45, 1631–1637. [Google Scholar] [CrossRef] [Green Version]
- Califf, R.M. Biomarker definitions and their applications. Exp. Biol. Med. 2018, 243, 213–221. [Google Scholar] [CrossRef] [PubMed]
| PICO Components | Determinants |
|---|---|
| Population | Postmenopausal women with amenorrhea for at least 12 months and who did not follow HRT |
| Intervention | Supplementation with (poly)phenol-rich products |
| Comparison | Placebo or control or any other comparative group (i.e., high vs. low doses of (poly)phenol-rich product) |
| Outcome | Cardiometabolic biomarkers: blood glucose/insulin, and HOMA-IR, blood lipids, SBP and DBP, and blood inflammatory biomarkers, endothelial cell adhesion molecules and oxidative stress biomarkers. |
| Markers of Glucose Metabolism | Study Characteristics | Effect (Change) | ||||||
|---|---|---|---|---|---|---|---|---|
| Type of Population | Source of (poly)phenols/(poly)phenols | Doses (mg/day) | Duration (days) | Variability of the Results (CV%) | Effect Size Range | Consistency of the Change 1 | Consistency of the Statistical Significance 2 | |
| Glucose (mg/dL) (n = 12) [27,31,32,33,34,36,37,38,39,42,44,45] | Mix (healthy, obese, dyslipidaemia, MetS and overweight) | Snack bar (soy protein, mix isoflavones), chocolate 99% (procyanidins, epicatechins, quercetin glycosides), red wine and dealcoholized red wine (anthocyanins and resveratrol) and mix (poly)phenols (isoflavones, daidzein, genistein, anthocyanins, flavan-3-ols and procyanidins) | ~60–1315 | 14–365 | ~6–39 | (−17.0, +12.0) | No | No |
| Insulin (µIU/mL) (n = 10) [27,33,34,36,37,38,42,43,44,45] | 14–365 | ~11–>100 | (−3.3, +2.2) | No | No | |||
| HOMA- IR (n = 6) [27,33,37,42,43,45] | 42–365 | ~27–>100 | (−0.82, +0.24) | No | No | |||
| Lipid Profile | Study Characteristics | Effect (Change) | ||||||
|---|---|---|---|---|---|---|---|---|
| Type of Population | Source of (poly)phenols /Type of (poly)phenols | Doses (mg/day) | Duration (days) | Variability of the Results (CV%) | Effect Size Range | Consistency of the Change 1 | Consistency of the Statistical Significance 2 | |
| T-C (mg/dL) (n = 15) [25,27,28,32,34,35,36,37,38,39,40,41,42,44,45] | Mix (healthy, osteopenia, dyslipidaemia) | Snack bar (soy protein, mix isoflavones), dried apple (proanthocyanins, hydroxycinnamic and anthocyanins), dried prunes (chlorogenic, neochlorogenic acids), chocolate 99% (procyanidins, epicatechins, quercetin glycosides), red wine and dealcoholized red wine (anthocyanins and resveratrol), beer and dealcoholized beer (prenylflavonoids) and mix (poly)phenols (isoflavones, daidzein, genistein, procyanidin, flavones, resveratrol, anthocyanins, quercetin, myricetin, kaempferol) | ~43–1000 | 14–365 | ~10–48 | (−22.0, +11.6) | No | No |
| LDL-C (mg/dL) (n = 15) [25,27,28,32,34,35,36,37,38,39,40,41,42,44,45] | Mix (healthy, osteopenia, dyslipidaemia) | Snack bar (soy protein, mix isoflavones), dried apple (proanthocyanins, hydroxycinnamic and anthocyanins), dried prunes (chlorogenic, neochlorogenic acids), chocolate 99% (procyanidins, epicatechins, quercetin glycosides), red wine and dealcoholized red wine (anthocyanins and resveratrol), beer and dealcoholized beer (prenylflavonoids) and mix (poly)phenols (isoflavones, daidzein, genistein, procyanidin, flavones, resveratrol, anthocyanins, quercetin, myricetin, kaempferol) | ~43–1000 | 14–365 | ~13–92 | (−23.9, +18.1) | No | No |
| HDL-C (mg/dL) (n = 16) [25,27,28,31,32,34,35,36,37,38,39,40,41,42,44,45] | Mix (healthy, osteopenia, dyslipidaemia, metabolic syndrom) | Snack bar (soy protein, mix isoflavones), dried apple (proanthocyanins, hydroxycinnamic and anthocyanins), dried prunes (chlorogenic, neochlorogenic acids), chocolate 99% (procyanidins, epicatechins, quercetin glycosides), red wine and dealcoholized red wine (anthocyanins and resveratrol), beer and dealcoholized beer (prenylflavonoids) and mix (poly)phenols (isoflavones, daidzein, genistein, procyanidin, flavones, resveratrol, anthocyanins, quercetin, myricetin, kaempferol) | ~43–1000 | 14–365 | ~10–66 | (−11.9, +11.1) | No | No |
| TGs (mg/dL) (n = 16) [25,27,28,31,32,34,35,36,37,38,39,40,41,42,44,45] | Mix (healthy, osteopenia, dyslipidaemia, metabolic syndrom) | Snack bar (soy protein, mix isoflavones), dried apple (proanthocyanidins, hydroxycinnamics and anthocyanins), dried prunes (chlorogenic, neochlorogenic acids), chocolate 99% (procyanidins, epicatechins, quercetin glycosides), red wine and dealcoholized red wine (anthocyanins and resveratrol), beer and dealcoholized beer (prenylflavonoids) | ~43–1000 | 14–365 | ~10–80 | (−23.0 +13.0) | No | No |
| and mix (poly)phenols (isoflavones, daidzein, genistein, procyanidin, flavones, resveratrol, anthocyanins, quercetin, myricetin, kaempferol) | ||||||||
| Blood Pressure (Units) | Study Characteristics | Effect (Change) | ||||||
|---|---|---|---|---|---|---|---|---|
| Type of Population | Source of (poly)phenols/ Type of (poly)phenols | Doses (mg/day) | Duration (days) | Variability of the Results (CV%) | Effect Size Range | Consistency of the Change 1 | Consistency of the Statistical Significance 2 | |
| SBP (mmHg) (n = 12) [25,26,29,31,32,34,35,37,39,42,44,45] | Mix (healthy, metabolic syndrome, dyslipidaemia, hypertensive) | Snack bar (soy protein, mix isoflavones), dried prunes (chlorogenic, neochlorogenic acids), chocolate 99% (procyanidins, epicatechins, quercetin glycosides), beer and dealcoholized beer (prenylflavonoids), red wine and dealcoholized red wine (anthocyanins and resveratrol) and mix (poly)phenols (isoflavones, daidzein, genistein, procyanidin, flavones, resveratrol, anthocyanins, or flavanols) | ~43–1000 | 14–365 | ~7–29% | (−11.0, +16.0) | No | No |
| DBP (mmHg) (n = 12) [25,26,29,31,32,34,35,37,39,42,44,45] | ~8–19% | (−7.0, +5.0) | No | No | ||||
| Biomarkers (Units) | Study Characteristics | Effect (Change) | ||||||
|---|---|---|---|---|---|---|---|---|
| Type of Population | Source of (poly)phenols/ Type of (poly)phenols | Doses (mg/day) | Duration (days) | Variability of the Results (CV%) | Effect Size Range | Consistency of the Change 1 | Consistency of the Statistical Significance 2 | |
| Inflammatory and cell adhesion biomarkers | ||||||||
| TNF-α (pg/L) (n = 3) [30,39,40] | Mix (healthy, hypertensive) | Blueberry powder (anthocyanins), lyophilized grape powder (anthocyanins, quercetin, myricetin, kaempferol and resveratrol) and elderberry extracts capsules (mix anthocyanins, mostly cyanidin-3-glucoside) | ~200–845 | 28–84 | ~20–90% | (−3.0, +0.11) | No | No |
| IL-6 (pg/L) (n = 4) [28,39,40,44] | Mix (healthy, osteopenia) | Lyophilized grape powder (anthocyanins, quercetin, myricetin, kaempferol and resveratrol), elderberry extracts capsules (mix anthocyanins, mostly cyanidin-3-glucoside), olive leaf extract (mix (poly)phenols, >40% oleuropein) and anthocyanins capsules | ~100–500 | 28–365 | ~25–>100% | (−0.50, +0.50) | No | Yes (NS) |
| CRP (mg/L) (n = 8) [28,29,30,37,39,40,41,44] | Mix (healthy, hypertensive, osteopenia) | Blueberry powder (anthocyanins), lyophilized grape powder (anthocyanins, quercetin, myricetin, kaempferol and resveratrol), elderberry extracts capsules (mix anthocyanins, mostly cyanidin-3- glucoside), olive leaf extract (mix (poly)phenols, >40% oleuropein), dried prunes (chlorogenic, neochlorogenic acids), dried apple (mix (poly)phenols), dried plums (mix (poly)phenols), snack bar (soy protein, mix isoflavones), and anthocyanins capsules | ~66–845 | 28–365 | ~40–>100% | (−0.50, +1.0) | No | Yes (NS) |
| Adiponectin (µg/mL) (n = 3) [31,33,38] | Mix (healthy, hypertensive, overweight/ obese) | Green tea extract capsules (mostly EGCG plus EC, EGC, ECG, and GCG), cocoa (poly)phenols, soy isoflavones and catechins | ~100–1300 | 60–365 | ~20–50% | (−1.0, +5.0) | No | No |
| sVCAM-1 (ng/mL) (n = 2) [25,44] | Mix (overweight and dyslipidaemia) | Anthocyanins capsules and cocoa beverage (mix flavanols) | ~240–400 | 42–240 | ~20–40% | (−113.0, +16.0) | No | No |
| sICAM-1 (ng/mL) (n = 2) [25,44] | Mix (overweight and dyslipidaemia) | Anthocyanins capsules and cocoa beverage (mix flavanols) | ~240–400 | 42–240 | ~15–55% | (−6.0, +29.0) | No | No |
| sP-Selectin (ng/mL) (n = 1) [25] | Dyslipidaemia | Cocoa beverage (mix flavanols) | ~400 | 42 | ~30–55% | (+3.0) | NA | NA |
| sE-Selectin (ng/mL) (n = 1) [25] | Dyslipidaemia | Cocoa beverage (mix flavanols) | ~400 | 42 | ~40–45% | (−5.0) | NA | NA |
| Oxidative stress biomarkers | ||||||||
| Ox-LDL (ng/mL) | Pre- and 1-stage hypertension | Blueberry powder (mix (poly)phenols and anthocyanins) | 845 | 28, 56 | ~5–32% | (+32.4, +59.5) Ῡ | Yes | NA |
| Isoprostanes (pg/mL serum) | ~39–92% | (−3.6, +2.5) Ῡ | No | NA | ||||
| TBARS (µM) | ~21–68% | (+0.30, +0.40) Ῡ | Yes | NA | ||||
| 8-OHdG (ng/mL) | ~13–26% | (−0.08, −0.04) Ῡ | Yes | Yes | ||||
| GSR (nmol/min/mL) | ~24–>100% | (−1.4, +−0.10) Ῡ | No | NA | ||||
| GPx (nmol/min/mL) | ~8–100% | (+3.1, +15.1) Ῡ | Yes | NA | ||||
| SOD (U/mL) (n = 1) [30] | ~70–>100% | (−0.02, +0.03) Ῡ | No | NA | ||||
| Isoprostanes (ng/mg creatinine, urine) (n = 1) [30] | Healthy | Lyophilized grape powder (flavanols, anthocyanins, quercetin, myricetin, kaempferol, and resveratrol) | ~210 | 28 | ~75–95% | NA | NA | NA |
| LPO (µM) (n = 1) [41] | Healthy | Dried plum or dried apple (mix (poly)phenols) | NI | 90, 365 | ~42–>100% | (−7.7, +0.20) Ῡ | No | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Martínez, L.; Periago, M.-J.; García-Alonso, J.; García-Conesa, M.-T.; González-Barrio, R. A Systematic Review of the Cardiometabolic Benefits of Plant Products Containing Mixed Phenolics and Polyphenols in Postmenopausal Women: Insufficient Evidence for Recommendations to This Specific Population. Nutrients 2021, 13, 4276. https://doi.org/10.3390/nu13124276
Sánchez-Martínez L, Periago M-J, García-Alonso J, García-Conesa M-T, González-Barrio R. A Systematic Review of the Cardiometabolic Benefits of Plant Products Containing Mixed Phenolics and Polyphenols in Postmenopausal Women: Insufficient Evidence for Recommendations to This Specific Population. Nutrients. 2021; 13(12):4276. https://doi.org/10.3390/nu13124276
Chicago/Turabian StyleSánchez-Martínez, Lorena, María-Jesús Periago, Javier García-Alonso, María-Teresa García-Conesa, and Rocío González-Barrio. 2021. "A Systematic Review of the Cardiometabolic Benefits of Plant Products Containing Mixed Phenolics and Polyphenols in Postmenopausal Women: Insufficient Evidence for Recommendations to This Specific Population" Nutrients 13, no. 12: 4276. https://doi.org/10.3390/nu13124276
APA StyleSánchez-Martínez, L., Periago, M.-J., García-Alonso, J., García-Conesa, M.-T., & González-Barrio, R. (2021). A Systematic Review of the Cardiometabolic Benefits of Plant Products Containing Mixed Phenolics and Polyphenols in Postmenopausal Women: Insufficient Evidence for Recommendations to This Specific Population. Nutrients, 13(12), 4276. https://doi.org/10.3390/nu13124276