
Prognostic Role of Malnutrition Diagnosed by Bioelectrical Impedance Vector Analysis in Older Adults Hospitalized with COVID-19 Pneumonia: A Prospective Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
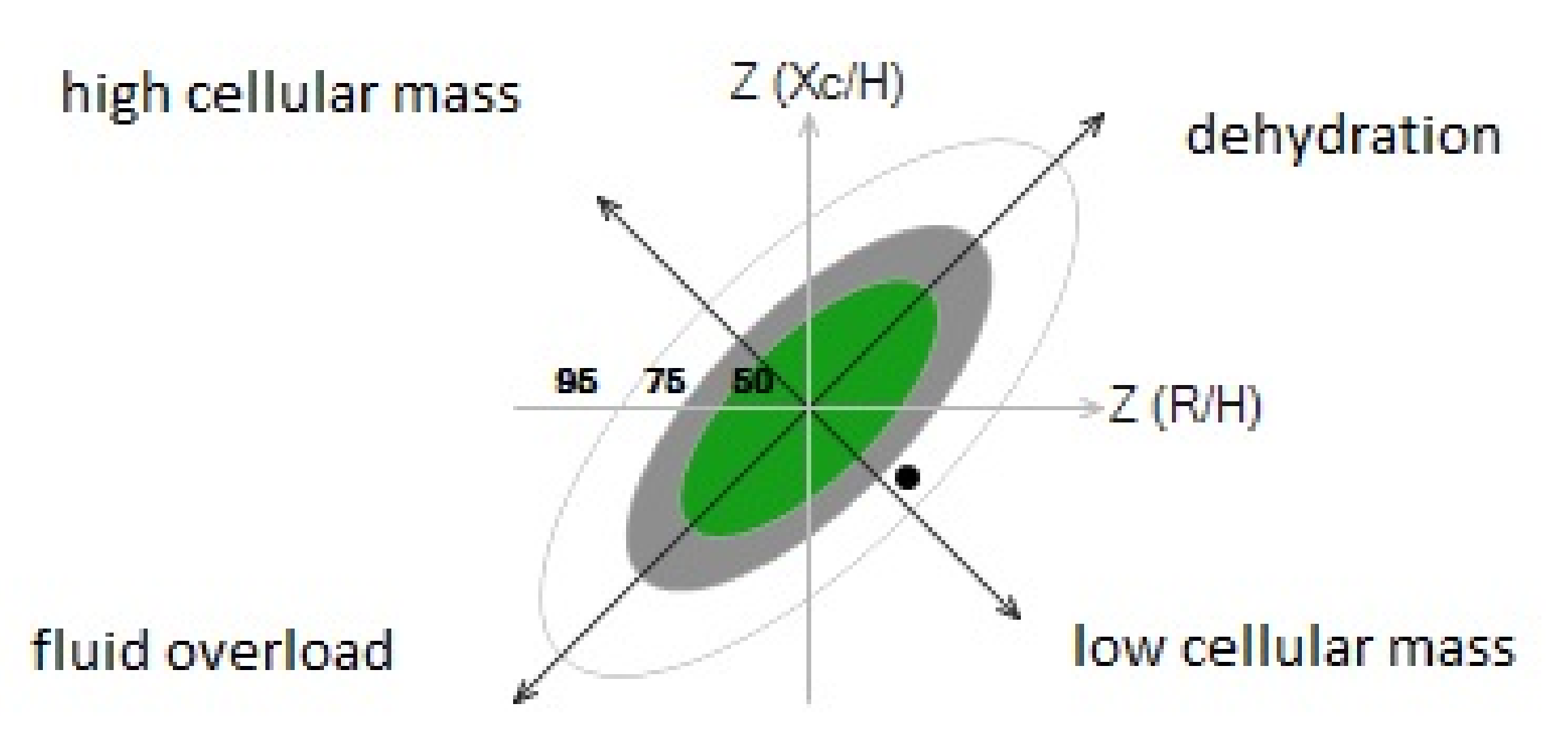
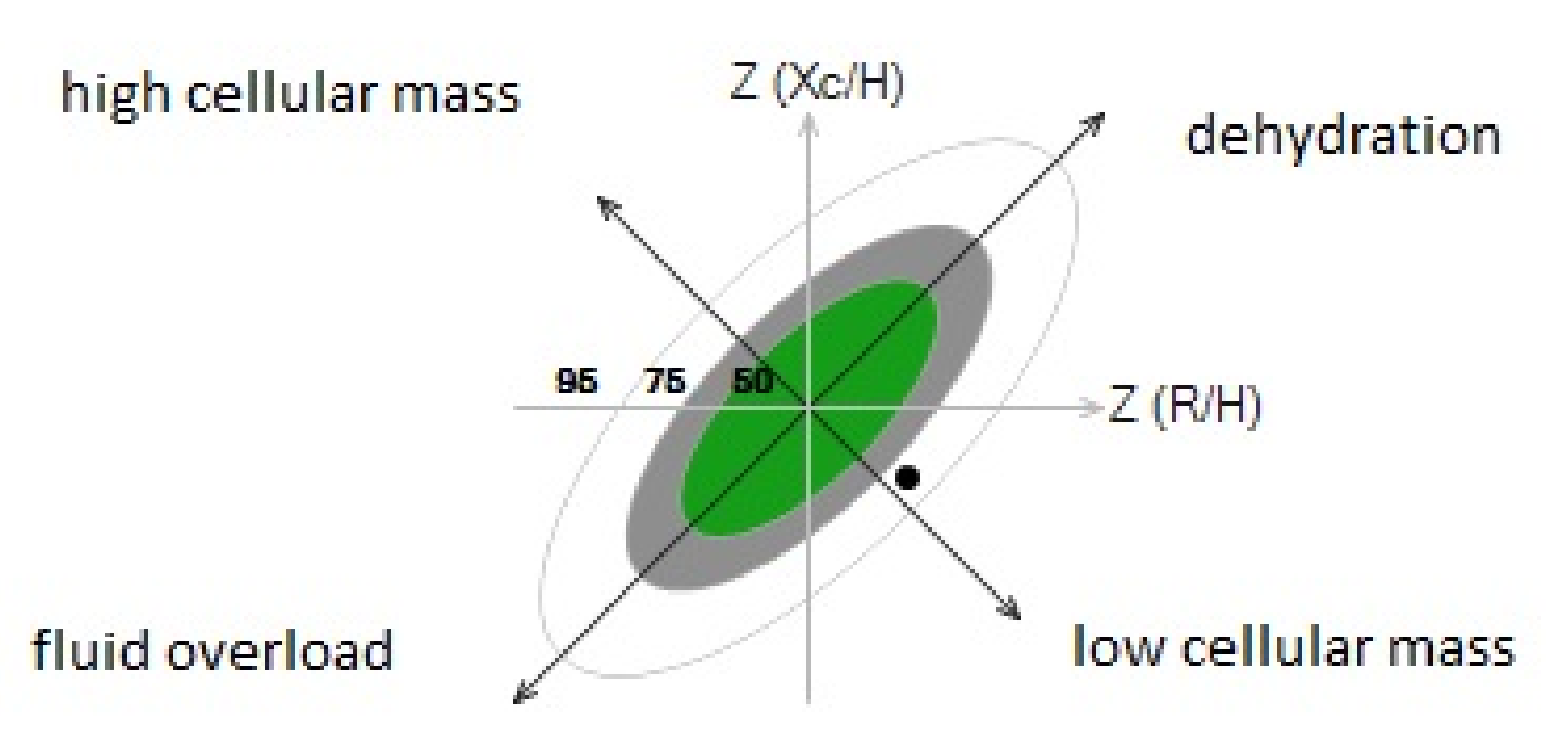
2.3. Nutritional Status: Bioelectrical Impedance Vector Analysis (BIVA)
2.4. Statistical Analysis
3. Results
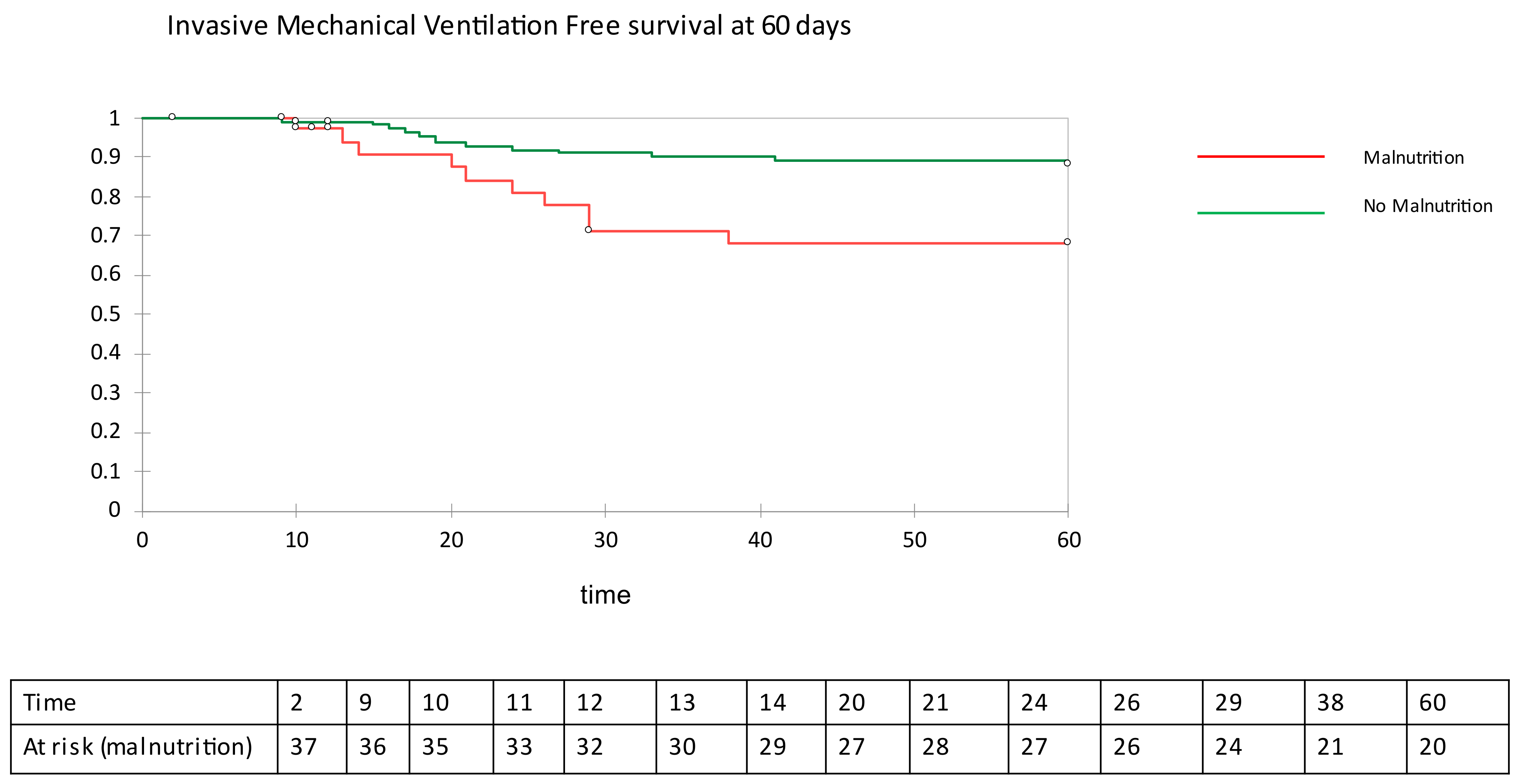
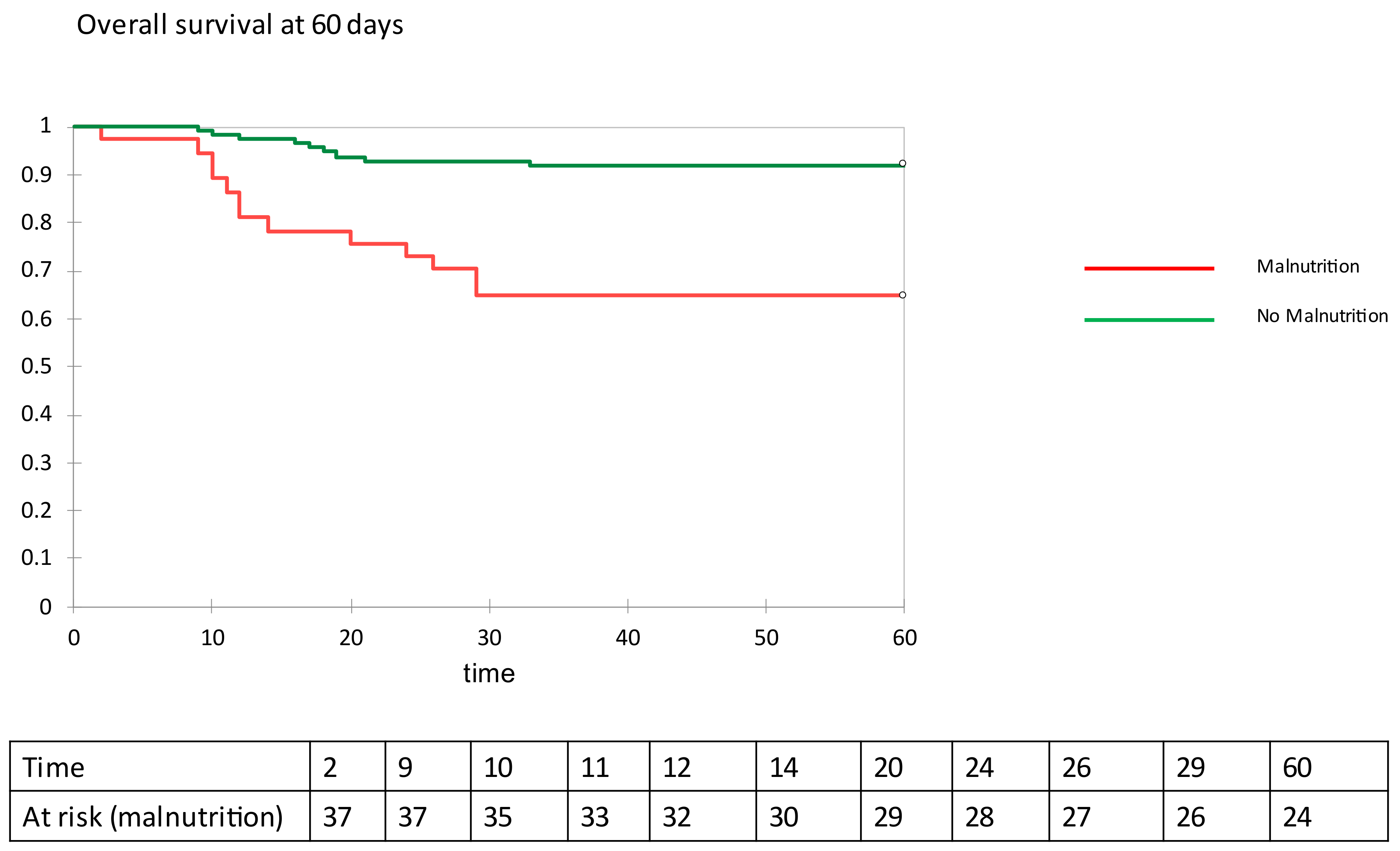
Outcome Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gallo Marin, B.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 severity: A literature review. Rev. Med. Virol. 2021, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Pirlich, M.; Schütz, T.; Kemps, M.; Luhman, N.; Minko, N.; Lübke, H.J.; Rossnagel, K.; Willich, S.N.; Lochs, H. Social risk factors for hospital malnutrition. Nutrition 2005, 21, 295–300. [Google Scholar] [CrossRef] [PubMed]
- White, J.V.; Guenter, P.; Jensen, G.; Malone, A.; Schofield, M.; Academy Malnutrition Work Group; A.S.P.E.N. Malnutrition Task Force; A.S.P.E.N. Board of Directors. Consensus statement: Academy of Nutrition and Dietetics and American Society for Parenteral and Enteral Nutrition: Characteristics recommended for the identification and documentation of adult malnutrition (undernutrition). J. Parenter. Enter. Nutr. 2012, 36, 275–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barker, L.A.; Gout, B.S.; Crowe, T.C. Hospital malnutrition: Prevalence, identification and impact on patients and the healthcare system. Int. J. Environ. Res. Public Health 2011, 8, 514–527. [Google Scholar] [CrossRef] [Green Version]
- Lew, C.C.H.; Yandell, R.; Fraser, R.J.L.; Chua, A.P.; Chong, M.F.F.; Miller, M. Association between malnutrition and clinical outcomes in the intensive care unit: A systematic review. J. Parenter. Enter. Nutr. 2017, 41, 744–758. [Google Scholar] [CrossRef]
- Wei, C.; Liu, Y.; Li, Y.; Zhang, Y.; Zhong, M.; Meng, X. Evaluation of the nutritional status in patients with COVID-19. J. Clin. Biochem. Nutr. 2020, 67, 116–121. [Google Scholar] [CrossRef]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.M.; et al. Diagnostic criteria for malnutrition An ESPEN Consensus Statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef]
- Earthman, C.P. Body Composition Tools for Assessment of Adult Malnutrition at the Bedside: A Tutorial on Research Considerations and Clinical Applications. JPEN J. Parenter. Enteral. Nutr. 2015, 39, 787–822. [Google Scholar] [CrossRef]
- Mulasi, U.; Kuchnia, A.J.; Cole, A.J.; Earthman, C.P. Bioimpedance at the bedside: Current applications, limitations, and opportunities. Nutr. Clin. Pract. 2015, 30, 180–193. [Google Scholar] [CrossRef] [Green Version]
- Dittmar, M. Reliability and variability of bioimpedance measures in normal adults: Effects of age, gender, and body mass. Am. J. Phys. Anthropol. 2003, 122, 361e70. [Google Scholar] [CrossRef]
- Piccoli, A.; Rossi, B.; Pillon, L.; Bucciante, G. A new method for monitoring body fluid variation by bioimpedance analysis: The RXc graph. Kidney. Int. 1994, 46, 534e9. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, M.C.; Barbosa-Silva, T.G.; Bielemann, R.M.; Gallagher, D.; Heymsfield, S.B. Phase angle and its determinants in healthy subjects: Influence of body composition. Am. J. Clin. Nutr. 2016, 103, 712–716. [Google Scholar] [CrossRef] [Green Version]
- Dehesa-López, E.; Martínez-Felix, J.I.; Ruiz-Ramos, A.; Atilano-Carsi, X. Discordance between bioelectrical impedance vector analysis and the new ESPEN definition of malnutrition for the diagnosis of hospital malnutrition. Clin. Nutr. ESPEN 2017, 18, 44–48. [Google Scholar] [CrossRef]
- Son, K.-B.; Lee, T.-J.; Hwang, S.-S. Disease severity classification and COVID-19 outcomes, Republic of Korea. Bull. World Health Organ. 2021, 99, 62–66. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection (SARI) when COVID-19 Disease Is Suspected: Interim Guidance. Available online: https://www.who.int/docs/default-source/coronaviruse/clinical-management-of-novel-cov.pdf. (accessed on 13 March 2021).
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Manuel Gómez, J.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.; Pirlich, M.; et al. Bioelectrical impedance analysis. Clin. Nutr. 2004, 23, 1430–1453. [Google Scholar] [CrossRef]
- Piccoli, A.; Nigrelli, S.; Caberlotto, A.; Bottazzo, S.; Rossi, B.; Pillon, L.; Maggiore, Q. Bivariate normal values of the bioelectrical impedance vector in adult and elderly populations. Am. J. Clin. Nutr. 1995, 61, 269–270. [Google Scholar] [CrossRef]
- Moonen, H.P.F.X.; van Zanten, F.J.L.; Driessen, L.; de Smet, V.; Slingerland-Boot, R.; Mensink, M.; van Zanten, A.R.H. Association of bioelectric impedance analysis body composition and disease severity in COVID-19 hospital ward and ICU patients: The BIAC-19 study. Clin. Nutr. 2021, 40, 2328–2336. [Google Scholar] [CrossRef]
- Cornejo-Pareja, I.; Vegas-Aguilar, I.M.; García-Almeida, J.M.; Bellido-Guerrero, D.; Talluri, A.; Lukaski, H.; Tinahones, F.J. Phase angle and standardized phase angle from bioelectrical impedance measurements as a prognostic factor for mortality at 90 days in patients with COVID-19: A longitudinal cohort study. Clin. Nutr. 2021, 17, S0261-5614(21)00091-1. [Google Scholar] [CrossRef]
- Del Giorno, R.; Quarenghi, M.; Stefanelli, K.; Capelli, S.; Giagulli, A.; Quarleri, L.; Stehrenberger, D.; Ossola, N.; Monotti, R.; Gabutti, L. Nutritional Risk Screening and Body Composition in COVID-19 Patients Hospitalized in an Internal Medicine Ward. Int. J. Gen. Med. 2020, 23, 1643–1651. [Google Scholar] [CrossRef]
- Norman, K.; Stobäus, N.; Pirlich, M.; Bosy-Westphal, A. Bioelectrical phase angle and impedance vector analysis-clinical relevance and applicability of impedance parameters. Clin. Nutr. 2012, 31, 854–861. [Google Scholar] [CrossRef]
- Lukaski, H.C.; Kyle, U.G.; Kondrup, J. Assessment of adult malnutrition and prognosis with bioelectrical impedance analysis: Phase angle and impedance ratio. Curr. Opin. Clin. Nutr. Metab. Care. 2017, 20, 330–339. [Google Scholar] [CrossRef]
- Piccoli, A.; Codognotto, M.; Piasentin, P.; Naso, A. Combined evaluation of nutrition and hydration in dialysis patients with bioelectrical impedance vector analysis (BIVA). Clin. Nutr. 2014, 33, 673–677. [Google Scholar] [CrossRef]
- Kammar-García, A.; Castillo-Martínez, L.; Villanueva-Juárez, J.L.; Pérez-Pérez, A.; Rocha-González, H.I.; Arrieta-Valencia, J.; Remolina-Schlig, M.; Hernández-Gilsoul, T. Comparison of Bioelectrical Impedance Analysis Parameters for the Detection of Fluid Overload in the Prediction of Mortality in Patients Admitted at the Emergency Department. JPEN J. Parenter. Enteral Nutr. 2021, 45, 414–422. [Google Scholar] [CrossRef]
- Zhao, X.; Li, Y.; Ge, Y.; Shi, Y.; Lv, P.; Zhang, J.; Fu, G.; Zhou, Y.; Jiang, K.; Lin, N.; et al. Evaluation of Nutrition Risk and Its Association With Mortality Risk in Severely and Critically Ill COVID-19 Patients. JPEN J. Parenter. Enteral Nutr. 2021, 45, 32–42. [Google Scholar] [CrossRef]
- Czapla, M.; Juárez-Vela, R.; Gea-Caballero, V.; Zieliński, S.; Zielińska, M. The Association between Nutritional Status and In-Hospital Mortality of COVID-19 in Critically-Ill Patients in the ICU. Nutrients 2021, 13, 3302. [Google Scholar] [CrossRef]
- Bedock, D.; Bel Lassen, P.; Mathian, A.; Moreau, P.; Couffignal, J.; Ciangura, C.; Poitou-Bernert, C.; Jeannin, A.C.; Mosbah, H.; Fadlallah, J.; et al. Prevalence and severity of malnutrition in hospitalized COVID-19 patients. Clin. Nutr. ESPEN. 2020, 40, 214–219. [Google Scholar] [CrossRef]
- Alwarawrah, Y.; Kiernan, K.; MacIver, N.J. Changes in Nutritional Status Impact Immune Cell Metabolism and Function. Front. Immunol. 2018, 16, 1055. [Google Scholar] [CrossRef] [Green Version]
- Christopher, E.T.; Carlos, A.C.J. Impact of micronutrients on respiratory infections. Nutr. Rev. 2011, 69, 259–269. [Google Scholar] [CrossRef]
- Liu, H.; Zhou, L.; Wang, H.; Wang, X.; Qu, G.; Cai, J.; Zhang, H. Malnutrition is associated with hyperinflammation and immunosuppression in COVID-19 patients: A prospective observational study. Nutr. Clin. Pract. 2021, 12, 863–871. [Google Scholar] [CrossRef]
- Sozio, E.; Tascini, C.; Fabris, M.; D′Aurizio, F.; De Carlo, C.; Graziano, E.; Bassi, F.; Sbrana, F.; Ripoli, A.; Pagotto, A.; et al. MR-proADM as prognostic factor of outcome in COVID-19 patients. Sci. Rep. 2021, 4, 5121. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients (n = 150) | No Malnutrition (n = 113) | Malnutrition (n = 37) | p-Value |
|---|---|---|---|---|
| Age (years) Median and IQR | 69 (58–78) | 66 (57–75) | 77 (71–83) | <0.001 |
| Male Sex (%) | 68.7% (103) | 69.1% (78) | 67.6% (25) | 0.860 |
| BMI (kg/m2) | 28.3 ± 4.9 | 29.3 ± 5.1 | 25.2 ± 3.4 | <0.001 |
| Waist Circ (cm) | 102 ± 16 | 104 ± 14 | 96 ± 11 | 0.001 |
| CRP (mg/dL) | 90.3 ± 71.4 | 86.7 ± 70.4 | 101.8 ± 74.4 | 0.145 |
| Current Smoker (%) | 3.4 | 2.7 | 3.6 | 0.237 |
| Dyslipidemia (%) | 26.2 | 26.8 | 24.3 | 0.957 |
| Hypertension (%) | 55.1 | 56.3 | 51.4 | 0.604 |
| Diabetes (%) | 28.8 | 27.7 | 32.4 | 0.570 |
| COPD (%) | 3.3 | 2.7 | 5.4 | 0.508 |
| CV disease (%) | 25.5 | 21.4 | 37.8 | 0.025 |
| CKD (%) | 12.6 | 10.7 | 16.6 | 0.126 |
| Malignancies (%) | 10.7 | 8 | 18 | 0.064 |
| Liver disease (%) | 6.7 | 6.3 | 8.3 | 0.187 |
| PCT (ng/mL) | 0.34 + 1.35 | 0.89 + 0.11 | 0.16 + 0.18 | 0.120 |
| IL-6 (ng/mL) | 66.5 ± 83.7 | 63.8 ± 63.9 | 72.2 ± 117.5 | 0.440 |
| Pro-ADM (ng/mL) | 1.22 ± 0.93 | 1.09 ± 0.45 | 1.61 ± 1.61 | 0.012 |
| D-Dimer (ng/mL) | 1584 ± 4025 | 1344.7 ± 3951.7 | 2309 ± 4217.2 | 0.025 |
| BUN (mg/dL) | 24.7 ± 10.1 | 22.6 ± 10.8 | 25.4 ± 10.8 | 0.712 |
| Creatinine (mg/dL) | 1.2 ± 1.8 | 1.1 ± 0,4 | 1.5 ± 2.3 | 0.667 |
| Sodium (mEq/L) | 138.2 ± 4.1 | 138.5 ± 3.7 | 137.2 ± 4.6 | 0.073 |
| Potassium (mEq/L) | 4.13 ± 0.5 | 4.12 ± 0.5 | 4.15 ± 0.5 | 0.853 |
| Chloride (mEq/L) | 100.4 ± 4.8 | 100.2 ± 4.2 | 101.2 ± 6.4 | 0.699 |
| AST (UI/L) | 41 ± 26.4 | 41.1 ± 26 | 37.6 ± 21.3 | 0.705 |
| ALT (UI/L) | 42.3 ± 36.3 | 44.7 ± 39.3 | 34.4 ± 23.9 | 0.156 |
| Bilirubin (mg/dL) | 0.568 ± 0.29 | 0.59 ± 0.31 | 0.48 ± 0.19 | 0.081 |
| LDH (UI/L) | 651.8 ± 241.9 | 640.4 ± 240.5 | 686.9 ± 246.5 | 0.328 |
| CPK (UI/L) | 155.3 ± 218.4 | 170.1 ± 230.2 | 110.2 ± 172.8 | 0.102 |
| Troponin (ng/mL) | 17.4 ± 16.2 | 16.7 ± 15.1 | 19.6 ± 9 | 0.133 |
| Albumin (g/L) | 34.4 ± 4.1 | 34.8 ± 4.1 | 33.1 ± 3.3 | 0.020 |
| Uric Acid (mg/dL) | 4.7 ± 1.8 | 4.8 ± 1.6 | 4.6 ± 2.2 | 0.457 |
| Cholesterol (mg/dL) | 150.2 ± 36.7 | 157.5 ± 30.7 | 147.6 ± 38.3 | 0.328 |
| HDL (mg/dL) | 33.4 ± 9.5 | 34.9 ± 8.9 | 32.8 ± 9.7 | 0.207 |
| LDL (mg/dL) | 84.8 ± 30.9 | 90.9 ± 25.8 | 82.7 ± 32.3 | 0.442 |
| TG (mg/dL) | 165.2 ± 58.8 | 165.9 ± 60.9 | 163.3 ± 53.4 | 0.729 |
| Glucose (mg/dL) | 130.9 ± 58.1 | 130.4 ± 57.5 | 132.4 ± 60.6 | 0.849 |
| HbA1c (DCCT) | 6.6 ± 1.1 | 6.5 ± 0.9 | 6.6 ± 1.2 | 0.950 |
| Variable | All Patients (n = 150) | No Malnutrition (n = 113) | Malnutrition (n = 37) | p-Value |
|---|---|---|---|---|
| Fat mass (kg/m2) | 28.8 ± 10.1 | 28.2 ± 10.6 | 30.5 ± 8.3 | 0.293 |
| Visceral adipose tissue (lt) | 3.4 ± 2.1 | 3.7 ± 2.2 | 2.8 ± 1.5 | 0.037 |
| Fat free mass (kg/m2) | 59.1 ± 13.3 | 62.1 ± 13.1 | 49.9 ± 9.3 | <0.001 |
| Skeletal muscle mass (kg/m2) | 27.1 ± 8.4 | 29.1 ± 8.2 | 20.9 ± 5.7 | <0.001 |
| TBW | 44.6 ± 10.1 | 46.3 ± 10 | 37.0 ± 6.6 | <0.001 |
| EBW | 12.2 ± 3.9 | 20.4 ± 3.9 | 17.3 ± 2.5 | <0.001 |
| EBW/TBW | 45.1 ± 3.3 | 44.4 ± 3.2 | 47 ± 2.7 | <0.001 |
| Phase angle (°) | 5.5 ± 1.5 | 5.9 ± 1.5 | 4.5 ± 0.7 | <0.001 |
| Variable | All Patients (n = 150) | No Malnutrition (n = 113) | Malnutrition (n = 37) | p-Value |
|---|---|---|---|---|
| WHO stage | ||||
| 0 | 13.3% (20) | 14.2% (16) | 10.8% (4) | 0.738 |
| 1 | 33.3% (50) | 36.3% (41) | 24.3% (9) | 0.229 |
| 2 | 38.6% (58) | 37.1% (42) | 43.2% (16) | 0.562 |
| 3 | 14.8% (22) | 12.4% (14) | 21.7% (8) | 0.185 |
| Lung CT Extension | ||||
| <25% | 9.6% (15) | 9.3% (11) | 10.8% (4) | 0.986 |
| 25–50% | 37.5% (56) | 42.7% (45) | 24.1% (9) | 0.114 |
| 50–75% | 49% (73) | 45.3% (51) | 58.5% (22) | 0.227 |
| >75% | 3.8% (6) | 2.7% (4) | 6.4% (2) | 0.310 |
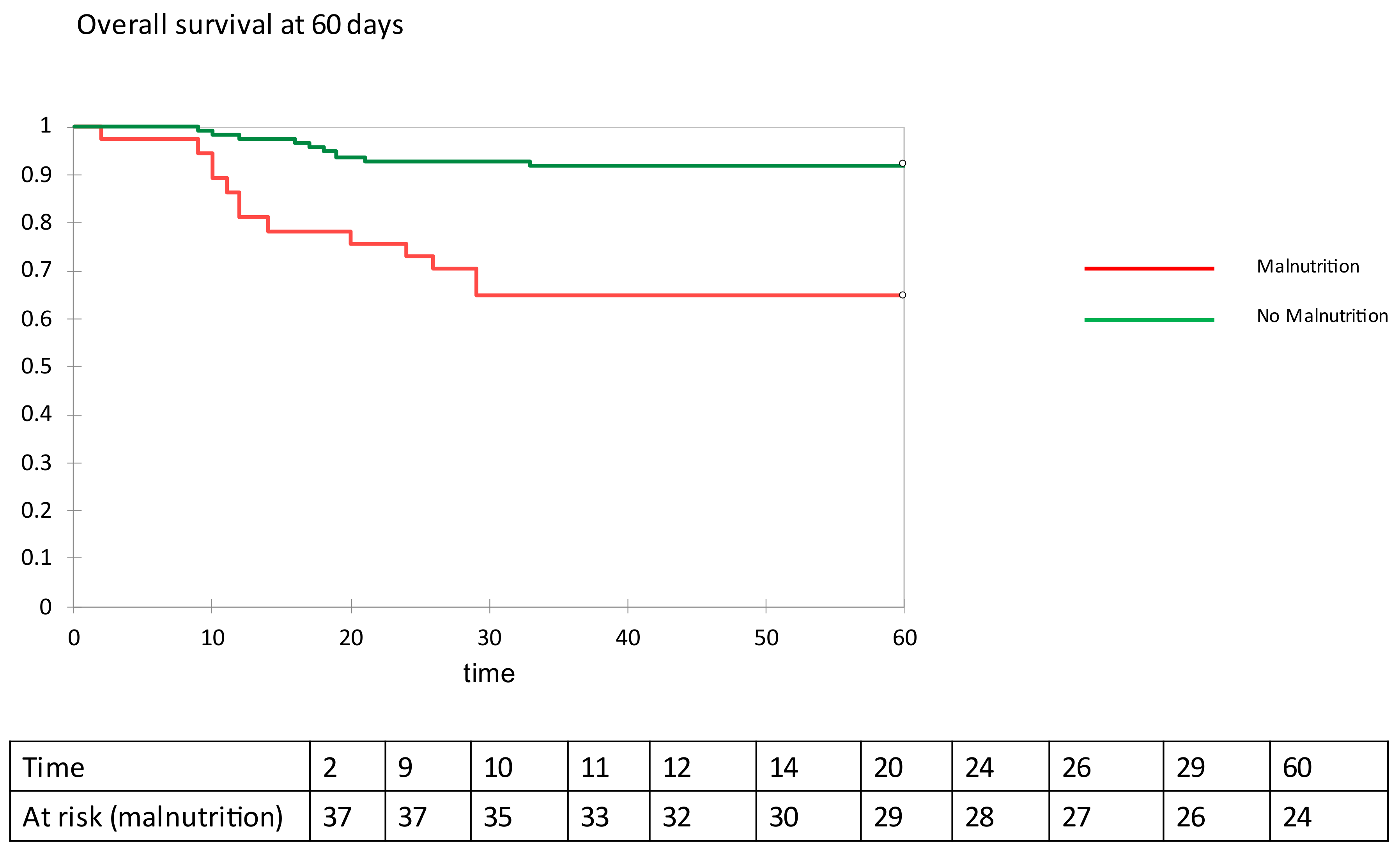
| Mortality (60 days) (%) | 14.7% (22) | 7.9% (9) | 35.1% (13) | 0.001 |
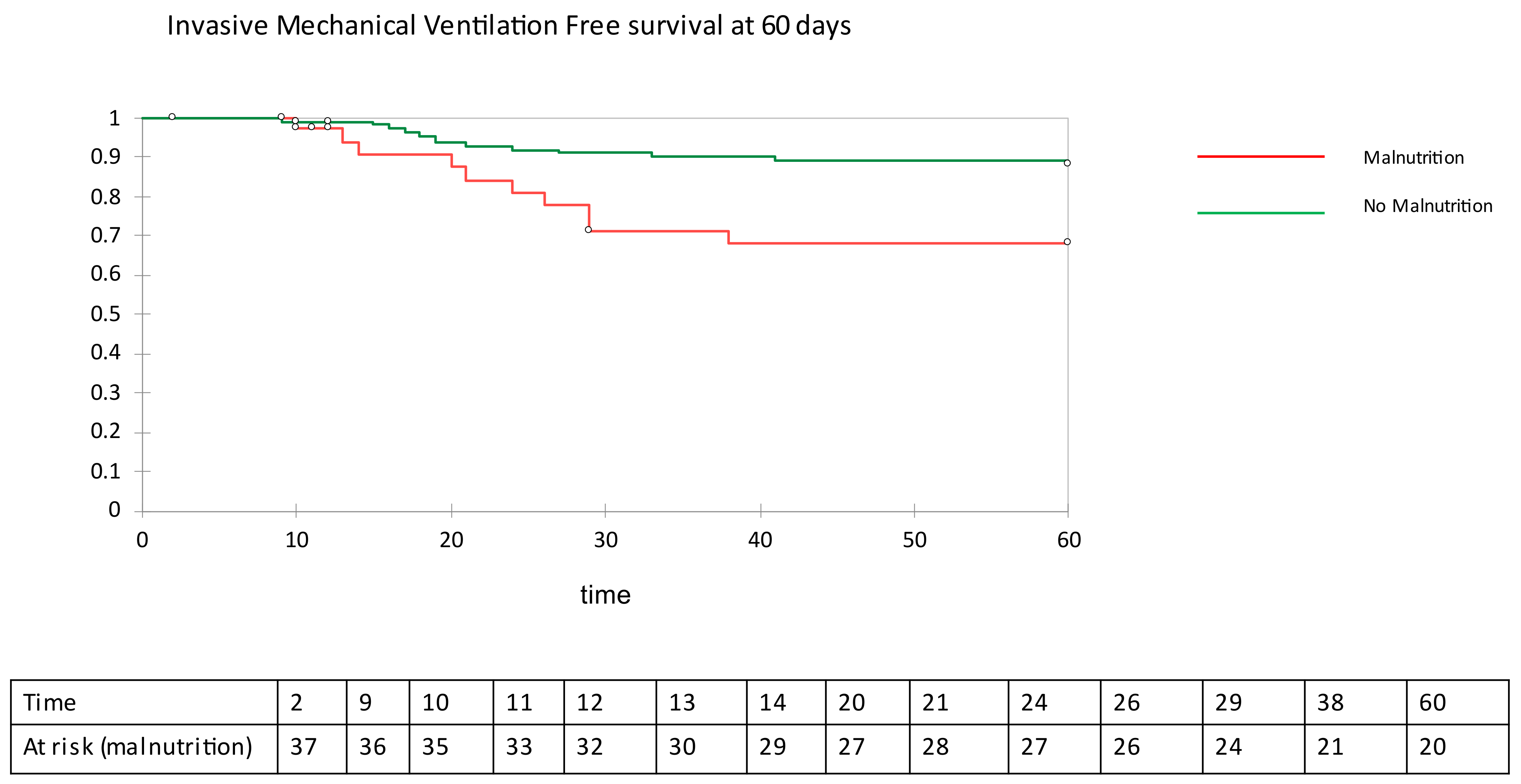
| IMV (%) | 15.3% (23) | 11.5% (13) | 27.1% (10) | 0.023 |
| Hospital stay (days) | 14.5 ± 15.1 | 13.2 ± 14.8 | 18.2 ± 15.7 | 0.003 |
| Variable | Value | Standard Error | Wald Chi-Square | Pr > Chi2 | Hazard Ratio | Lower Bound (95%) | Upper Bound (95%) |
|---|---|---|---|---|---|---|---|
| BIVA Malnutrition (crude) | 1.122 | 0.421 | 7.086 | 0.008 | 3.069 | 1.344 | 7.009 |
| BIVA Malnutrition (adjusted) * | 1.476 | 0.513 | 8.275 | 0.004 | 4.375 | 1.601 | 11.959 |
| Phase Angle value (adjusted) * | 0.007 | 0.176 | 0.002 | 0.967 | 1.007 | 0.714 | 1.422 |
| Variable | Value | Standard Error | Wald Chi-Square | Pr > Chi2 | Hazard Ratio | Lower Bound (95% | Upper Bound (95%) |
|---|---|---|---|---|---|---|---|
| BIVA Malnutrition (crude) | 1.641 | 0.434 | 14.287 | 0.000 | 5.159 | 2.203 | 12.081 |
| BIVA Malnutrition (adjused) * | 1.498 | 0.516 | 8.421 | 0.004 | 4.474 | 1.626 | 12.306 |
| Phase Angle value (adjused) * | 0.081 | 0.153 | 0.280 | 0.597 | 1.084 | 0.803 | 1.463 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Da Porto, A.; Tascini, C.; Peghin, M.; Sozio, E.; Colussi, G.; Casarsa, V.; Bulfone, L.; Graziano, E.; De Carlo, C.; Catena, C.; et al. Prognostic Role of Malnutrition Diagnosed by Bioelectrical Impedance Vector Analysis in Older Adults Hospitalized with COVID-19 Pneumonia: A Prospective Study. Nutrients 2021, 13, 4085. https://doi.org/10.3390/nu13114085
Da Porto A, Tascini C, Peghin M, Sozio E, Colussi G, Casarsa V, Bulfone L, Graziano E, De Carlo C, Catena C, et al. Prognostic Role of Malnutrition Diagnosed by Bioelectrical Impedance Vector Analysis in Older Adults Hospitalized with COVID-19 Pneumonia: A Prospective Study. Nutrients. 2021; 13(11):4085. https://doi.org/10.3390/nu13114085
Chicago/Turabian StyleDa Porto, Andrea, Carlo Tascini, Maddalena Peghin, Emanuela Sozio, Gianluca Colussi, Viviana Casarsa, Luca Bulfone, Elena Graziano, Chiara De Carlo, Cristiana Catena, and et al. 2021. "Prognostic Role of Malnutrition Diagnosed by Bioelectrical Impedance Vector Analysis in Older Adults Hospitalized with COVID-19 Pneumonia: A Prospective Study" Nutrients 13, no. 11: 4085. https://doi.org/10.3390/nu13114085
APA StyleDa Porto, A., Tascini, C., Peghin, M., Sozio, E., Colussi, G., Casarsa, V., Bulfone, L., Graziano, E., De Carlo, C., Catena, C., & Sechi, L. A. (2021). Prognostic Role of Malnutrition Diagnosed by Bioelectrical Impedance Vector Analysis in Older Adults Hospitalized with COVID-19 Pneumonia: A Prospective Study. Nutrients, 13(11), 4085. https://doi.org/10.3390/nu13114085