
Adherence to the Mediterranean Diet and Its Association with the Level of Physical Activity in Fitness Center Users: Croatian-Based Study

 ,
,  ,
,  , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Considerations
2.2. Participants
2.3. Questionnaires
- Walking MET-min/week = 3.3 × walking minutes × walking days
- Moderate MET-min/week = 4.0 × moderate activity minutes × moderate days
- Vigorous MET-min/week = 8.0 × vigorous activity minutes × vigorous days
- Total MET-min/week = walking + moderate + vigorous MET-min/week scores
2.4. Survey Pre-Testing
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics
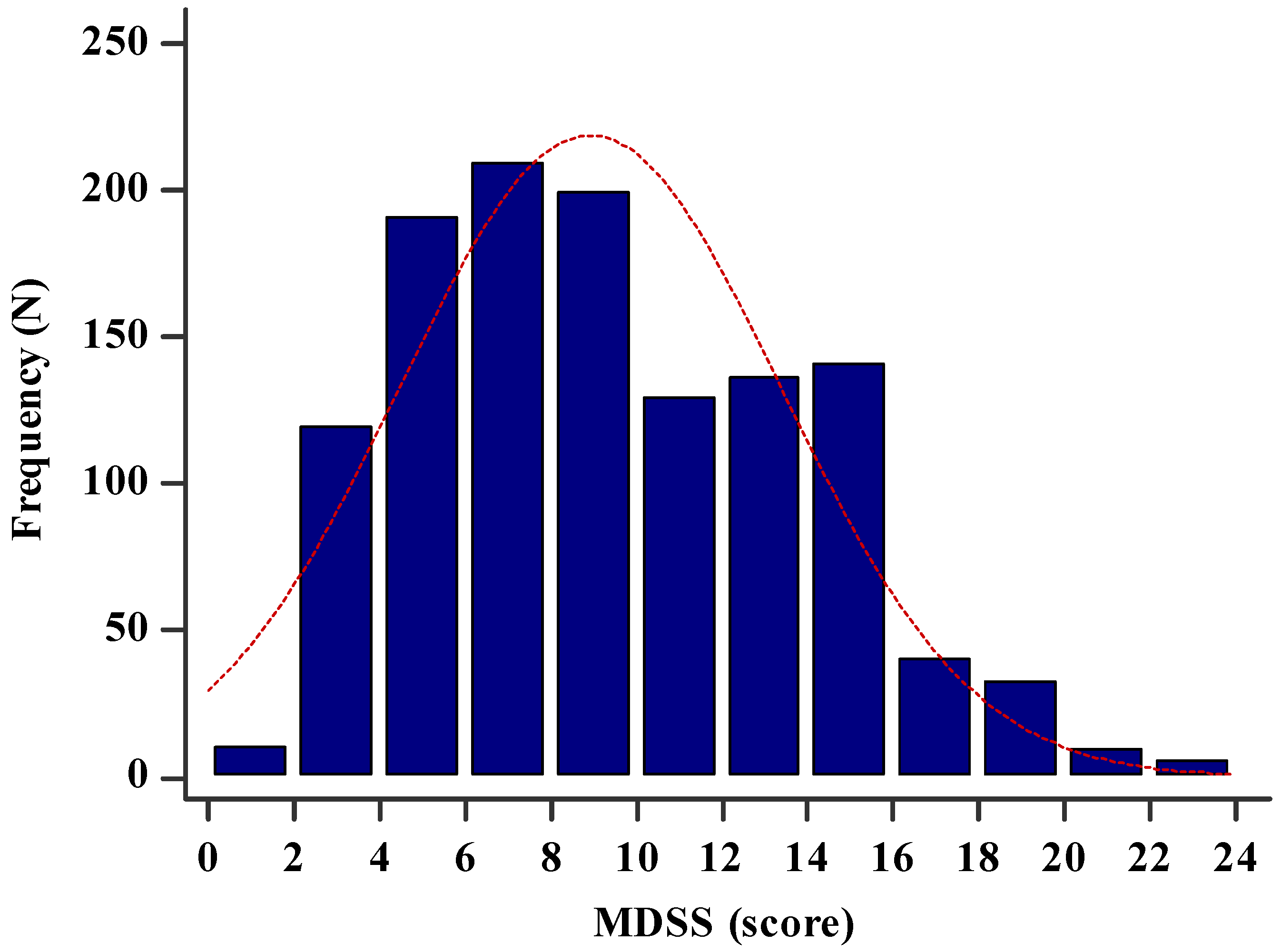
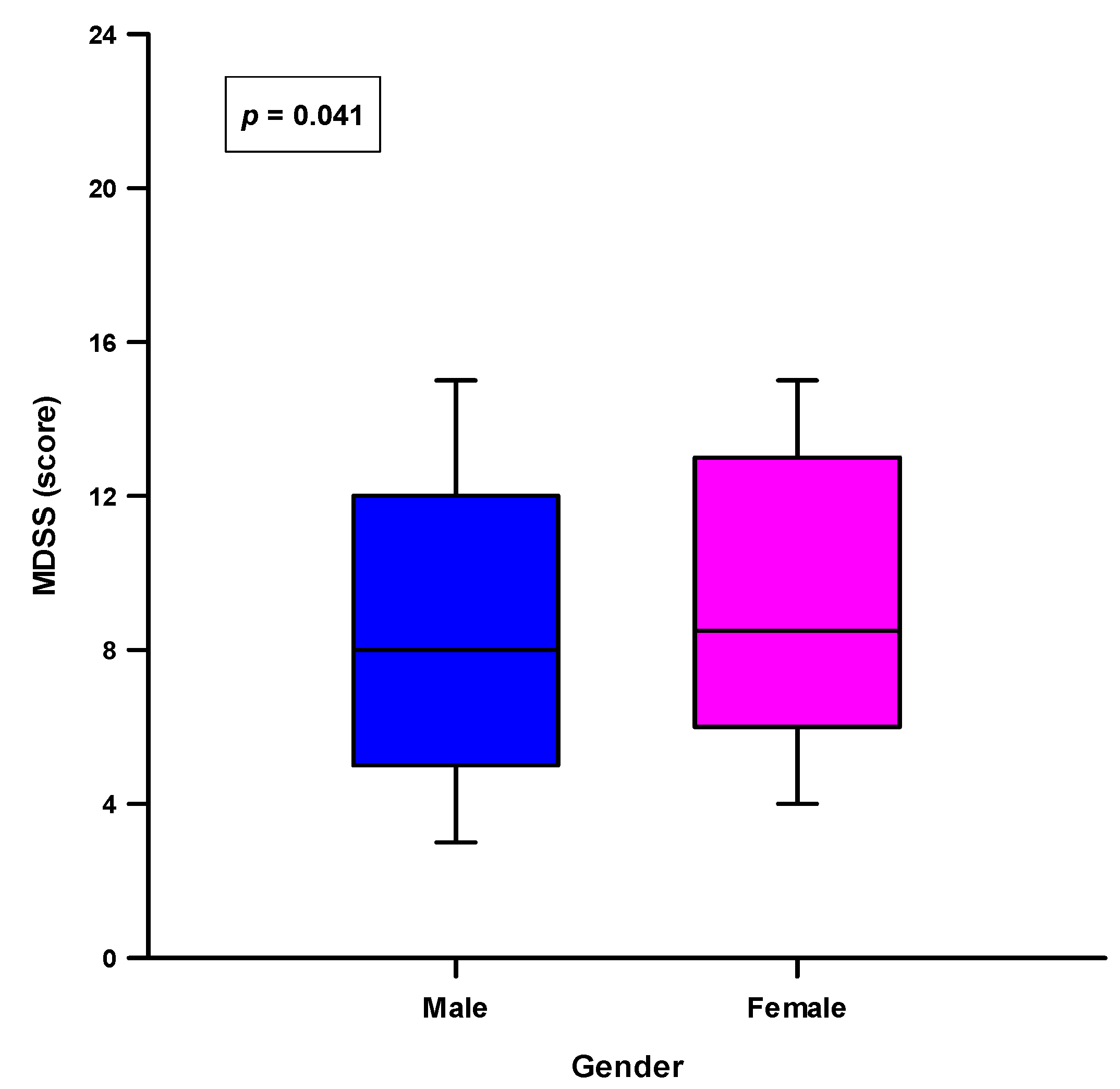
3.2. MDSS Results in the Study Sample
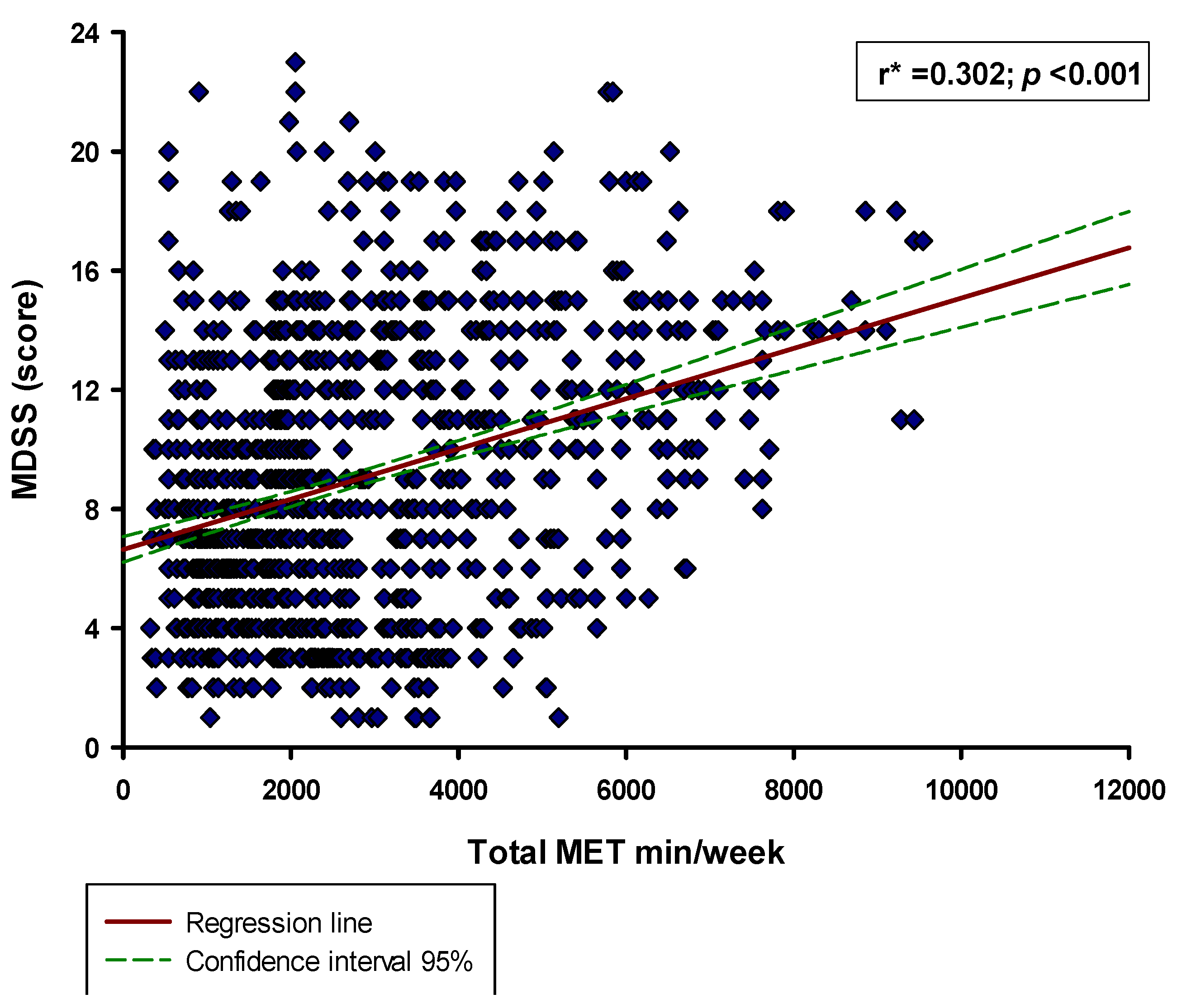
3.3. Regression Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ruegsegger, G.N.; Booth, F.W. Health Benefits of Exercise. Cold Spring Harb. Perspect. Med. 2018, 8, a029694. [Google Scholar] [CrossRef] [Green Version]
- Block, L.G.; Grier, S.A.; Childers, T.L.; Davis, B.; Ebert, J.E.J.; Kumanyika, S.; Laczniak, R.N.; Machin, J.E.; Motley, C.M.; Peracchio, L.; et al. From Nutrients to Nurturance: A Conceptual Introduction to Food Well-Being. J. Public Policy Mark. 2011, 30, 5–13. [Google Scholar] [CrossRef] [Green Version]
- Renner, B.; Sproesser, G.; Strohbach, S.; Schupp, H.T. Why we eat what we eat. The Eating Motivation Survey (TEMS). Appetite 2012, 59, 117–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.J. An Overview of Current Physical Activity Recommendations in Primary Care. Korean J. Fam. Med. 2019, 40, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of exercise is a major cause of chronic diseases. Compr. Physiol. 2012, 2, 1143–1211. [Google Scholar]
- Sharma, A.; Madaan, V.; Petty, F.D. Exercise for mental health. Prim. Care Companion J. Clin. Psychiatry 2006, 8, 106. [Google Scholar] [CrossRef] [PubMed]
- Martinovic, D.; Tokic, D.; Vilovic, M.; Rusic, D.; Bukic, J.; Bozic, J. Sport Dietary Supplements and Physical Activity in Biomedical Students. Int. J. Environ. Res. Public Health 2021, 18, 2046. [Google Scholar] [CrossRef]
- Gardiner, P.; Kemper, K.J.; Legedza, A.; Phillips, R.S. Factors associated with herb and dietary supplement use by young adults in the United States. BMC Complement. Altern. Med. 2007, 7, 39. [Google Scholar] [CrossRef] [Green Version]
- Cena, H.; Calder, P.C. Defining a Healthy Diet: Evidence for the Role of Contemporary Dietary Patterns in Health and Disease. Nutrients 2020, 12, 334. [Google Scholar] [CrossRef] [Green Version]
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet; A Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef]
- Augimeri, G.; Bonofiglio, D. The Mediterranean Diet as a Source of Natural Compounds: Does It Represent a Protective Choice against Cancer? Pharmaceuticals 2021, 14, 920. [Google Scholar] [CrossRef] [PubMed]
- Augimeri, G.; Montalto, F.I.; Giordano, C.; Barone, I.; Lanzino, M.; Catalano, S.; Andò, S.; De Amicis, F.; Bonofiglio, D. Nutraceuticals in the Mediterranean Diet: Potential Avenues for Breast Cancer Treatment. Nutrients 2021, 13, 2557. [Google Scholar] [CrossRef]
- Zappalà, G.; Buscemi, S.; Mulè, S.; La Verde, M.; D’Urso, M.; Corleo, D.; Marranzano, M. High adherence to Mediterranean diet, but not individual foods or nutrients, is associated with lower likelihood of being obese in a Mediterranean cohort. Eat. Weight Disord. 2018, 23, 605–614. [Google Scholar] [CrossRef] [PubMed]
- La Verde, M.; Mulè, S.; Zappalà, G.; Privitera, G.; Maugeri, G.; Pecora, F.; Marranzano, M. Higher adherence to the Mediterranean diet is inversely associated with having hypertension: Is low salt intake a mediating factor? Int. J. Food Sci. Nutr. 2018, 69, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Psaltopoulou, T.; Sergentanis, T.N.; Panagiotakos, D.B.; Sergentanis, I.N.; Kosti, R.; Scarmeas, N. Mediterranean diet, stroke, cognitive impairment, and depression: A meta-analysis. Ann. Neurol. 2013, 74, 580–591. [Google Scholar] [CrossRef]
- Loughrey, D.G.; Lavecchia, S.; Brennan, S.; Lawlor, B.A.; Kelly, M.E. The Impact of the Mediterranean Diet on the Cognitive Functioning of Healthy Older Adults: A Systematic Review and Meta-Analysis. Adv. Nutr. 2017, 8, 571–586. [Google Scholar] [CrossRef] [PubMed]
- Platania, A.; Zappala, G.; Mirabella, M.U.; Gullo, C.; Mellini, G.; Beneventano, G.; Maugeri, G.; Marranzano, M. Association between Mediterranean diet adherence and dyslipidaemia in a cohort of adults living in the Mediterranean area. Int. J. Food Sci. Nutr. 2018, 69, 608–618. [Google Scholar] [CrossRef]
- Guasch-Ferré, M.; Merino, J.; Sun, Q.; Fitó, M.; Salas-Salvadó, J. Dietary Polyphenols, Mediterranean Diet, Prediabetes, and Type 2 Diabetes: A Narrative Review of the Evidence. Oxid. Med. Cell. Longev. 2017, 2017, 6723931. [Google Scholar] [CrossRef]
- Bendinelli, B.; Masala, G.; Saieva, C.; Salvini, S.; Calonico, C.; Sacerdote, C.; Agnoli, C.; Grioni, S.; Frasca, G.; Mattiello, A.; et al. Fruit, vegetables, and olive oil and risk of coronary heart disease in Italian women: The EPICOR Study. Am. J. Clin. Nutr. 2011, 93, 275–283. [Google Scholar] [CrossRef] [Green Version]
- Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Ruiz-Gutiérrez, V.; Covas, M.I.; Fiol, M.; Gómez-Gracia, E.; López-Sabater, M.C.; Vinyoles, E.; et al. Effects of a Mediterranean-style diet on cardiovascular risk factors: A randomized trial. Ann. Intern. Med. 2006, 145, 1–11. [Google Scholar] [CrossRef]
- Buckland, G.; Travier, N.; Barricarte, A.; Ardanaz, E.; Moreno-Iribas, C.; Sánchez, M.J.; Molina-Montes, E.; Chirlaque, M.D.; Huerta, J.M.; Navarro, C.; et al. Olive oil intake and CHD in the European Prospective Investigation into Cancer and Nutrition Spanish cohort. Br. J. Nutr. 2012, 108, 2075–2082. [Google Scholar] [CrossRef] [Green Version]
- Samieri, C.; Féart, C.; Proust-Lima, C.; Peuchant, E.; Tzourio, C.; Stapf, C.; Berr, C.; Barberger-Gateau, P. Olive oil consumption, plasma oleic acid, and stroke incidence: The Three-City Study. Neurology 2011, 77, 418–425. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, 13. [Google Scholar] [CrossRef]
- Iaccarino Idelson, P.; Scalfi, L.; Valerio, G. Adherence to the Mediterranean Diet in children and adolescents: A systematic review. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 283–299. [Google Scholar] [CrossRef]
- Malakou, E.; Linardakis, M.; Armstrong, M.E.G.; Zannidi, D.; Foster, C.; Johnson, L.; Papadaki, A. The Combined Effect of Promoting the Mediterranean Diet and Physical Activity on Metabolic Risk Factors in Adults: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Nutrients 2018, 10, 1577. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Iglesias, R.; Álvarez-Pereira, S.; Tardón, A.; Fernández-García, B.; Iglesias-Gutiérrez, E. Adherence to the Mediterranean Diet in a School Population in the Principality of Asturias (Spain): Relationship with Physical Activity and Body Weight. Nutrients 2021, 13, 1507. [Google Scholar] [CrossRef] [PubMed]
- López-Gil, J.F.; Brazo-Sayavera, J.; García-Hermoso, A.; Yuste Lucas, J.L. Adherence to Mediterranean Diet Related with Physical Fitness and Physical Activity in Schoolchildren Aged 6–13. Nutrients 2020, 12, 567. [Google Scholar] [CrossRef] [Green Version]
- Galan-Lopez, P.; Sánchez-Oliver, A.J.; Ries, F.; González-Jurado, J.A. Mediterranean Diet, Physical Fitness and Body Composition in Sevillian Adolescents: A Healthy Lifestyle. Nutrients 2019, 11, 2009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Passariello, C.L.; Marchionni, S.; Carcuro, M.; Casali, G.; Della Pasqua, A.; Hrelia, S.; Malaguti, M.; Lorenzini, A. The Mediterranean Athlete’s Nutrition: Are Protein Supplements Necessary? Nutrients 2020, 12, 3681. [Google Scholar] [CrossRef] [PubMed]
- Monteagudo, C.; Mariscal-Arcas, M.; Rivas, A.; Lorenzo-Tovar, M.L.; Tur, J.A.; Olea-Serrano, F. Proposal of a Mediterranean Diet Serving Score. PLoS ONE 2015, 10, e0128594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marendić, M.; Polić, N.; Matek, H.; Oršulić, L.; Polašek, O.; Kolčić, I. Mediterranean diet assessment challenges: Validation of the Croatian Version of the 14-item Mediterranean Diet Serving Score (MDSS) Questionnaire. PLoS ONE 2021, 16, e0247269. [Google Scholar] [CrossRef]
- Sember, V.; Meh, K.; Sorić, M.; Starc, G.; Rocha, P.; Jurak, G. Validity and Reliability of International Physical Activity Questionnaires for Adults across EU Countries: Systematic Review and Meta Analysis. Int. J. Environ. Res. Public Health 2020, 17, 7161. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R., Jr.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32, S498–S504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Fauci, V.; Alessi, V.; Assefa, D.Z.; Lo Giudice, D.; Calimeri, S.; Ceccio, C.; Antonuccio, G.M.; Genovese, C.; Squeri, R. Mediterranean diet: Knowledge and adherence in Italian young people. Clin. Ter. 2020, 171, e437–e443. [Google Scholar] [PubMed]
- Dinu, M.; Lotti, S.; Pagliai, G.; Pisciotta, L.; Zavatarelli, M.; Borriello, M.; Solinas, R.; Galuffo, R.; Clavarino, A.; Acerra, E.; et al. Mediterranean Diet Adherence in a Sample of Italian Adolescents Attending Secondary School—The “#facciamoComunicAzione” Project. Nutrients 2021, 13, 2806. [Google Scholar] [CrossRef]
- Kyriacou, A.; Evans, J.M.; Economides, N. Adherence to the Mediterranean diet by the Greek and Cypriot population: A systematic review. Eur. J. Public Health 2015, 25, 1012–1018. [Google Scholar] [CrossRef] [Green Version]
- Chacón-Cuberos, R.; Badicu, G.; Zurita-Ortega, F.; Castro-Sánchez, M. Mediterranean Diet and Motivation in Sport: A Comparative Study Between University Students from Spain and Romania. Nutrients 2018, 11, 30. [Google Scholar] [CrossRef] [Green Version]
- Morelli, C.; Avolio, E.; Galluccio, A.; Caparello, G.; Manes, E.; Ferraro, S.; Caruso, A.; De Rose, D.; Barone, I.; Adornetto, C.; et al. Nutrition Education Program and Physical Activity Improve the Adherence to the Mediterranean Diet: Impact on Inflammatory Biomarker Levels in Healthy Adolescents From the DIMENU Longitudinal Studby. Front. Nutr. 2021, 8, 685247. [Google Scholar] [CrossRef]
- Ouyang, Y.; Wang, K.; Zhang, T.; Peng, L.; Song, G.; Luo, J. The Influence of Sports Participation on Body Image, Self-Efficacy, and Self-Esteem in College Students. Front. Psychol. 2020, 10, 3039. [Google Scholar] [CrossRef] [Green Version]
- Bonaccorsi, G.; Furlan, F.; Scocuzza, M.; Lorini, C. Adherence to Mediterranean Diet among Students from Primary and Middle School in the Province of Taranto, 2016–2018. Int. J. Environ. Res. Public Health 2020, 17, 5437. [Google Scholar] [CrossRef] [PubMed]
- Rosi, A.; Calestani, M.V.; Parrino, L.; Milioli, G.; Palla, L.; Volta, E.; Brighenti, F.; Scazzina, F. Weight Status Is Related with Gender and Sleep Duration but Not with Dietary Habits and Physical Activity in Primary School Italian Children. Nutrients 2017, 9, 579. [Google Scholar] [CrossRef]
- Andrade, V.; Jorge, R.; García-Conesa, M.-T.; Philippou, E.; Massaro, M.; Chervenkov, M.; Ivanova, T.; Maksimova, V.; Smilkov, K.; Ackova, D.G.; et al. Mediterranean Diet Adherence and Subjective Well-Being in a Sample of Portuguese Adults. Nutrients 2020, 12, 3837. [Google Scholar] [CrossRef] [PubMed]
- Biasini, B.; Rosi, A.; Menozzi, D.; Scazzina, F. Adherence to the Mediterranean Diet in Association with Self-Perception of Diet Sustainability, Anthropometric and Sociodemographic Factors: A Cross-Sectional Study in Italian Adults. Nutrients 2021, 13, 3282. [Google Scholar] [CrossRef] [PubMed]
- Gregório, M.J.; Rodrigues, A.M.; Graça, P.; de Sousa, R.D.; Dias, S.S.; Branco, J.C.; Canhão, H. Food Insecurity Is Associated with Low Adherence to the Mediterranean Diet and Adverse Health Conditions in Portuguese Adults. Front. Public Health 2018, 6, 38. [Google Scholar] [CrossRef]
- Joo, J.; Williamson, S.A.; Vazquez, A.I.; Fernandez, J.R.; Bray, M.S. The influence of 15-week exercise training on dietary patterns among young adults. Int. J. Obes. 2019, 43, 1681–1690. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Study Sample n = 1220 | Male n = 690 | Female n = 530 | p * |
|---|---|---|---|---|
| Age (years) | 29.1 ± 8.8 | 28.2 ± 7.8 | 30.3 ± 9.9 | 0.001 |
| Weight (kg) | 79.3 ± 15.6 | 87.2 ± 13.0 | 68.9 ± 12.1 | 0.001 |
| Height (cm) | 179.6 ± 9.5 | 184.8 ± 7.3 | 172.0 ± 7.4 | 0.001 |
| BMI (kg/m2) | 24.4 ± 3.4 | 25.4 ± 2.9 | 23.0 ± 3.6 | 0.001 |
| Education level | ||||
| Elementary school (n, %) | 7 (0.6) | 2 (0.3%) | 5 (0.9) | 0.334 |
| High school (n, %) | 315 (25.8) | 172 (24.9) | 143 (27.0) | |
| Bachelor’s degree (n, %) | 256 (21.0) | 143 (20.7) | 113 (21.3) | |
| Master’s degree (n, %) | 642 (52.6) | 373 (54.1) | 269 (50.8) | |
| Using dietary supplements (n, %) | ||||
| Yes (n, %) | 803 (65.8) | 493 (71.4) | 310 (58.5) | <0.001 |
| No (n, %) | 417 (34.2) | 197 (28.6) | 220 (41.5) | |
| Dietary supplements used | ||||
| Whey protein (n, %) | 617 (76.8) | 375 (76.0) | 242 (78.0) | 0.003 |
| BCAA (n, %) | 399 (49.6) | 232 (47.0) | 167 (53.8) | 0.472 |
| Creatine (n, %) | 243 (30.2) | 196 (39.7) | 47 (15.1) | <0.001 |
| Magnesium (n, %) | 472 (58.7) | 275 (55.7) | 197 (63.5) | 0.370 |
| Vitamin C (n, %) | 347 (43.2) | 205 (41.5) | 142 (45.8) | 0.291 |
| Vitamin B complex (n, %) | 170 (21.1) | 90 (18.2) | 80 (25.8) | 0.715 |
| Multivitamin (n, %) | 258 (32.1) | 139 (28.1) | 119 (38.3) | 0.364 |
| Duration of using a fitness center | ||||
| <1 year (n, %) | 337 (27.6) | 205 (29.7) | 132 (24.9) | 0.222 |
| 1–3 years (n, %) | 352 (28.9) | 187 (27.1) | 165 (31.1) | |
| 4–7 years (n, %) | 232 (19.0) | 128 (18.6) | 104 (19.3) | |
| >7 years (n, %) | 299 (24.5) | 170 (24.6) | 129 (24.3) |
| Parameter | First Tertile Group MET < 1750 min/Week n = 407 | Second Tertile Group MET 1750–3150 min/Week n = 406 | Third Tertile Group MET > 3150 min/Week n = 407 | p * |
|---|---|---|---|---|
| Age (years) | 29.0 ± 8.4 | 29.2 ± 9.3 | 29.1 ± 8.8 | 0.954 |
| Male gender (n, %) | 193 (47.4%) | 255 (62.8%) | 242 (59.5%) | <0.001 |
| Weight (kg) | 79.9 ± 15.8 | 77.7 ± 14.4 | 79.9 ± 16.2 | 0.095 |
| Height (cm) | 179.9 ± 9.7 | 179.0 ± 9.3 | 179.7 ± 9.5 | 0.473 |
| BMI (kg/m2) | 24.4 ± 3.3 | 24.0 ± 3.1 | 24.5 ± 3.8 | 0.114 |
| Education level | ||||
| Elementary school (n, %) | 2 (0.5) | 2 (0.5) | 3 (0.7) | <0.001 |
| High school (n, %) | 133 (32.7) | 88 (21.7) | 94 (23.1) | |
| Bachelor’s degree (n, %) | 69 (17.0) | 113 27.8) | 74 (18.2) | |
| Master’s degree (n, %) | 203 (49.9) | 203 (50.0) | 236 (58.0) | |
| Using dietary supplements (n, %) | ||||
| Yes (n, %) | 229 (56.3) | 274 (67.5) | 300 (73.7) | <0.001 |
| No (n, %) | 178 (43.7) | 132 (32.5) | 107 (26.3) | |
| Dietary supplements used | ||||
| Whey protein (n, %) | 115 (50.2) | 206 (89.9) | 296 (98.6) | <0.001 |
| BCAA (n, %) | 73 (31.8) | 154 (67.2) | 172 (57.3) | <0.001 |
| Creatine (n, %) | 22 (9.6) | 102 (44.5) | 119 (39.6) | <0.001 |
| Magnesium (n, %) | 144 (62.8) | 165 (72.0) | 163 (71.1) | 0.240 |
| Vitamin C (n, %) | 118 (51.5) | 112 (48.9) | 117 (51.0) | 0.893 |
| Vitamin B complex (n, %) | 59 (25.7) | 56 (24.4) | 55 (24.0) | 0.916 |
| Multivitamin (n, %) | 84 (36.6) | 90 (39.3) | 84 (36.6) | 0.827 |
| Duration of using a fitness center | ||||
| <1 year (n, %) | 98 (24.1) | 118 (29.1) | 121 (29.7) | <0.001 |
| 1–3 years (n, %) | 137 (33.7) | 115 (28.3) | 100 (24.6) | |
| 4–7 years (n, %) | 76 (18.7) | 94 (23.2) | 62 (15.2) | |
| >7 years (n, %) | 96 (23.6) | 79 (19.5) | 124 (30.5) |
| Parameter | First Tertile Group MET < 1750 min/Week n = 407 | Second Tertile Group MET 1750–3150 min/Week n = 406 | Third Tertile Group MET > 3150 min/Week n = 407 | p * |
|---|---|---|---|---|
| Cereals (n, %) | 87 (21.4) | 93 (23.0) | 156 (38.3) | <0.001 |
| Potatoes (n, %) | 367 (90.2) | 343 (84.7) | 318 (78.1) | <0.001 |
| Olive oil (n, %) | 59 (14.5) | 85 (21.0) | 119 (29.2) | <0.001 |
| Nuts (n, %) | 124 (30.5) | 174 (43.0) | 171 (42.0) | <0.001 |
| Fruits (n, %) | 70 (17.2) | 98 (24.1) | 158 (38.8) | <0.001 |
| Vegetables (n, %) | 91 (22.4) | 111 (27.3) | 178 (43.7) | <0.001 |
| Dairy (n, %) | 64 (15.7) | 118 (29.1) | 154 (37.8) | <0.001 |
| Legumes (n, %) | 313 (76.9) | 248 (61.2) | 270 (66.3) | <0.001 |
| Eggs (n, %) | 224 (55.0) | 186 (46.0) | 195 (47.9) | 0.025 |
| Fish (n, %) | 242 (59.5) | 217 (53.7) | 266 (65.4) | 0.003 |
| White meat (n, %) | 372 (91.4) | 304 (74.9) | 329 (80.8) | <0.001 |
| Red meat (n, %) | 73 (17.9) | 145 (35.8) | 187 (45.9) | <0.001 |
| Sweets (n, %) | 206 (50.6) | 265 (65.3) | 191 (46.9) | <0.001 |
| Wine (n, %) | 1 (0.2) | 59 (14.6) | 38 (9.3) | <0.001 |
| Variable. | β * | SE | t-Value | p |
|---|---|---|---|---|
| Age | −0.003 | 0.013 | −0.222 | 0.824 |
| BMI | 0.017 | 0.038 | 0.464 | 0.642 |
| Total MET min/week | 0.007 | 0.0006 | 11.509 | <0.001 |
| Duration of using a fitness center | 0.401 | 0.102 | 3.912 | 0.001 |
| Variable | aOR [95% CI] | p |
|---|---|---|
| Female sex 1 | 1.09 [0.77, 1.54] | 0.811 |
| Using the fitness center for 1–3 years 2 | 1.93 [1.24, 3.00] | 0.021 |
| Using the fitness center for 4–7 years 2 | 1.47 [0.97, 2.23] | 0.071 |
| Using the fitness center for >7 years 2 | 1.05 [0.68, 1.63] | 0.814 |
| Dietary supplements usage 3 | 1.52 [1.06, 2.17] | 0.023 |
| Older age | 1.00 [0.98, 1.02] | 0.874 |
| Total MET min/week 2nd quartile 4 | 1.61 [0.88, 2.96] | 0.126 |
| Total MET min/week 3rd quartile 4 | 3.94 [2.28, 6.80] | <0.001 |
| Total MET min/week 4th quartile 4 | 8.08 [4.78, 13.67] | <0.001 |
| BMI | 0.99 [0.95, 1.05] | 0.936 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinovic, D.; Tokic, D.; Martinovic, L.; Kumric, M.; Vilovic, M.; Rusic, D.; Vrdoljak, J.; Males, I.; Ticinovic Kurir, T.; Lupi-Ferandin, S.; et al. Adherence to the Mediterranean Diet and Its Association with the Level of Physical Activity in Fitness Center Users: Croatian-Based Study. Nutrients 2021, 13, 4038. https://doi.org/10.3390/nu13114038
Martinovic D, Tokic D, Martinovic L, Kumric M, Vilovic M, Rusic D, Vrdoljak J, Males I, Ticinovic Kurir T, Lupi-Ferandin S, et al. Adherence to the Mediterranean Diet and Its Association with the Level of Physical Activity in Fitness Center Users: Croatian-Based Study. Nutrients. 2021; 13(11):4038. https://doi.org/10.3390/nu13114038
Chicago/Turabian StyleMartinovic, Dinko, Daria Tokic, Lovre Martinovic, Marko Kumric, Marino Vilovic, Doris Rusic, Josip Vrdoljak, Ivan Males, Tina Ticinovic Kurir, Slaven Lupi-Ferandin, and et al. 2021. "Adherence to the Mediterranean Diet and Its Association with the Level of Physical Activity in Fitness Center Users: Croatian-Based Study" Nutrients 13, no. 11: 4038. https://doi.org/10.3390/nu13114038
APA StyleMartinovic, D., Tokic, D., Martinovic, L., Kumric, M., Vilovic, M., Rusic, D., Vrdoljak, J., Males, I., Ticinovic Kurir, T., Lupi-Ferandin, S., & Bozic, J. (2021). Adherence to the Mediterranean Diet and Its Association with the Level of Physical Activity in Fitness Center Users: Croatian-Based Study. Nutrients, 13(11), 4038. https://doi.org/10.3390/nu13114038