
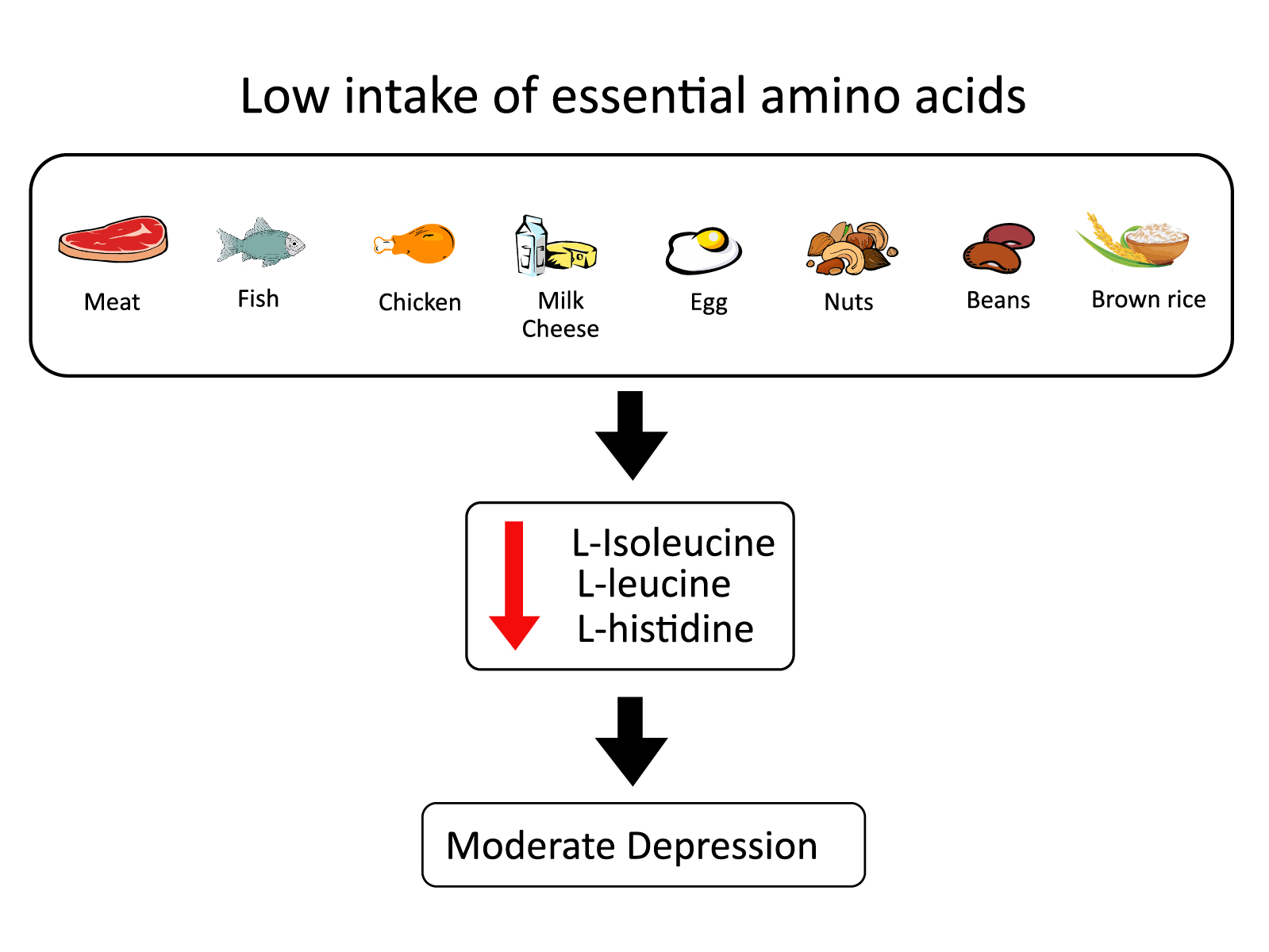
Deficiency in the Essential Amino Acids l-Isoleucine, l-Leucine and l-Histidine and Clinical Measures as Predictors of Moderate Depression in Elderly Women: A Discriminant Analysis Study

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Depression Questionnaires
2.3. Dementia and Global Cognition
2.4. Quantification of Amino Acids
2.5. Discriminant Analysis
2.6. Statistical Procedure
3. Results
3.1. Characteristics of the Participants and Depressive Symptoms
3.2. Amino Acid Profiles
3.3. Discriminant Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Depression 2020. Available online: http://who.int/mediacentre/factsheets/fs369/en/ (accessed on 30 January 2020).
- Agüera-Ortiz, L.; Claver-Martín, M.D.; Franco-Fernández, M.D.; López-Álvarez, J.; Martín-Carrasco, M.; Ramos-García, M.I.; Sánchez-Pérez, M. Depression in the Elderly. Consensus Statement of the Spanish Psychogeriatric Association. Front. Psychiatry 2020, 11. [Google Scholar] [CrossRef]
- Santos, P.V.D.L.; Valdés, S.E.C. Prevalencia de depresión en hombres y mujeres mayores en México y factores de riesgo. Poblac. Salud Mesoam. 2017, 15. [Google Scholar] [CrossRef] [Green Version]
- Gutsmiedl, K.; Krause, M.; Bighelli, I.; Schneider-Thoma, J.; Leucht, S. How well do elderly patients with major depressive disorder respond to antidepressants: A systematic review and single-group meta-analysis. BMC Psychiatry 2020, 20, 102. [Google Scholar] [CrossRef] [Green Version]
- Solís-Ortiz, S.; Pérez-Luque, E.; Pacheco-Zavala, M.D.P. Resting EEG Activity and Ovarian Hormones as Predictors of Depressive Symptoms in Postmenopausal Women without a Diagnosis of Major Depression. Psychology 2012, 03, 834–840. [Google Scholar] [CrossRef] [Green Version]
- Kang, H.-J.; Kim, S.-Y.; Bae, K.-Y.; Kim, S.-W.; Shin, I.-S.; Yoon, J.-S.; Kim, J.-M. Comorbidity of Depression with Physical Disorders: Research and Clinical Implications. Chonnam Med. J. 2015, 51, 8–18. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Aging. Health, Depression and Older Adults. 2020. Available online: www.nih.gob (accessed on 2 March 2020).
- Hakkarainen, R.; Partonen, T.; Haukka, J.; Virtamo, J.; Albanes, D.; Lönnqvist, J. Association of dietary amino acids with low mood. Depress. Anxiety 2003, 18, 89–94. [Google Scholar] [CrossRef]
- Aucoin, M.; LaChance, L.; Cooley, K.; Kidd, S. Diet and Psychosis: A Scoping Review. Neuropsychobiology 2018, 79, 20–42. [Google Scholar] [CrossRef]
- Loureiro, C.M.; Da Roza, D.L.; Corsi-Zuelli, F.; Shuhama, R.; Fachim, H.A.; Simões-Ambrosio, L.M.C.; Deminice, R.; Jordão, A.A.; Menezes, P.R.; Del-Ben, C.M.; et al. Plasma amino acids profile in first-episode psychosis, unaffected siblings and community-based controls. Sci. Rep. 2020, 10, 21423. [Google Scholar] [CrossRef]
- Leppik, L.; Kriisa, K.; Koido, K.; Koch, K.; Kajalaid, K.; Haring, L.; Vasar, E.; Zilmer, M. Profiling of Amino Acids and Their Derivatives Biogenic Amines Before and After Antipsychotic Treatment in First-Episode Psychosis. Front. Psychiatry 2018, 9, 155. [Google Scholar] [CrossRef] [Green Version]
- Van der Does, A. The effects of tryptophan depletion on mood and psychiatric symptoms. J. Affect. Disord. 2001, 64, 107–119. [Google Scholar] [CrossRef]
- Parker, G.; Brotchie, H. Mood effects of the amino acids tryptophan and tyrosine. Acta Psychiatr. Scand. 2011, 124, 417–426. [Google Scholar] [CrossRef]
- Baranyi, A.; Amouzadeh-Ghadikolai, O.; Von Lewinski, D.; Breitenecker, R.J.; Rothenhäusler, H.-B.; Robier, C.; Baranyi, M.; Theokas, S.; Meinitzer, A. Revisiting the tryptophan-serotonin deficiency and the inflammatory hypotheses of major depression in a biopsychosocial approach. PeerJ 2017, 5. [Google Scholar] [CrossRef] [Green Version]
- Pan, J.-X.; Xia, J.-J.; Deng, F.-L.; Liang, W.-W.; Wu, J.; Yin, B.-M.; Dong, M.-X.; Chen, J.-J.; Ye, F.; Wang, H.-Y.; et al. Diagnosis of major depressive disorder based on changes in multiple plasma neurotransmitters: A targeted metabolomics study. Transl. Psychiatry 2018, 8, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Fellendorf, F.; Platzer, M.; Pilz, R.; Rieger, A.; Kapfhammer, H.-P.; Mangge, H.; Dalkner, N.; Zelzer, S.; Meinitzer, A.; Birner, A.; et al. Branched-chain amino acids are associated with metabolic parameters in bipolar disorder. World J. Biol. Psychiatry 2018, 20, 821–826. [Google Scholar] [CrossRef]
- Baranyi, A.; Amouzadeh-Ghadikolai, O.; von Lewinski, D.; Rothenhäusler, H.B.; Theokas, S.; Robier, C.; Mangge, H.; Reicht, G.; Hlade, P.; Meinitzer, A. Branched-Chain amino acids as new biomarkers of major depression-A novel neurobiology of mood disorder. PLoS ONE 2016, 11, e0160542. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, A.F.; Solmi, M.; Sanches, M.; Machado, M.O.; Stubbs, B.; Ajnakina, O.; Sherman, C.; Sun, Y.R.; Liu, C.S.; Brunoni, A.R.; et al. Evidence-based umbrella review of 162 peripheral biomarkers for major mental disorders. Transl. Psychiatry 2020, 10, 1–13. [Google Scholar] [CrossRef]
- Fisher, R.A. The use of multiple measurements in taxonomic problems. Ann. Eugen. 1936, 7, 179–188. [Google Scholar] [CrossRef]
- Flury, B.; Reidwyl, H. Discriminant analysis. In Multivariate Statistics. A Practical Approach; Chapman and Hall: London, UK, 1988; pp. 181–233. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Beck, A.T.; Steer, R.A. Beck Depression Inventory; The Psychological Corporation: San Antonio, TX, USA, 1993. [Google Scholar]
- Kuehner, C. Why is depression more common among women than among men? Lancet Psychiatry 2017, 4, 146–158. [Google Scholar] [CrossRef]
- Jurado, S.; Villegas, M.E.; Méndez, L.; Rodríguez, F.; Loperena, V.; Varela, R. La estandarización del inventario de la depresión de Beck, para los residentes de la ciudad de México. Salud Ment. 1998, 21, 36–38. [Google Scholar]
- Yesavage, J.A.; Brink, T.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1983, 17, 37–49. [Google Scholar] [CrossRef]
- Martínez-de la Iglesia, J.; Onís-Vilches, M.C.; Dueñas-Herrero, R.; Albert-Colomer, C.; Aguado-Taberné, C.; Luque, D. Versiόn española del cuestionario de Yesavage abreviado (GDS) para el despistaje de depresiόn en mayores de 65 años: Adaptaciόn y validaciόn. MEDIFAM 2002, 12, 620–630. [Google Scholar] [CrossRef] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Lobo, A.; Saz, P.; Marcos, G.; Grupo de Trabajo ZARADEMP. MMSE: Examen Cognoscitivo Mini-Mental; TEA Ediciones: Madrid, Spain, 2002. [Google Scholar]
- Henderson, J.W.; Ricker, R.D.; Bidlingmeyer, B.A.; Woodward, C. Rapid, accurate, sensitive and reproducible HPLC analysis of amino acids. In Amino Acid Analysis using Zorbax Aclipse AAA Columns and the Agilent 1100 HPLC; Agilent Technologies: Santa Clara, CA, USA, 2000. [Google Scholar]
- Field, A. Multivariate Analysis of Variance. In Discovering Statistics Using SPSS; Sage Publications Ltd.: London, UK, 2009; pp. 587–623. [Google Scholar]
- Dowd, E.T. Depression: Theory, assessment, and new directions in practice. Int. J. Clin. Health Psychol. 2004, 4, 413–423. [Google Scholar]
- Steffen, A.; Nübel, J.; Jacobi, F.; Bätzing, J.; Holstiege, J. Mental and somatic comorbidity of depression: A comprehensive cross-sectional analysis of 202 diagnosis groups using German nationwide ambulatory claims data. BMC Psychiatry 2020, 20, 142. [Google Scholar] [CrossRef] [Green Version]
- Corrao, S.; Santalucia, P.; Argano, C.; Djade, C.; Barone, E.; Tettamanti, M.; Pasina, L.; Franchi, C.; Eldin, T.K.; Marengoni, A.; et al. Gender-differences in disease distribution and outcome in hospitalized elderly: Data from the REPOSI study. Eur. J. Intern. Med. 2014, 25, 617–623. [Google Scholar] [CrossRef] [Green Version]
- Marcucci, M.; Franchi, C.; Nobili, A.; Mannucci, P.M.; Ardoino, I. REPOSI Investigators Defining Aging Phenotypes and Related Outcomes: Clues to Recognize Frailty in Hospitalized Older Patients. J. Gerontol. Ser. A Boil. Sci. Med Sci. 2016, 72, 395–402. [Google Scholar] [CrossRef]
- Fiske, A.; Wetherell, J.L.; Gatz, M. Depression in Older Adults. Annu. Rev. Clin. Psychol. 2009, 5, 363–389. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, S.; Milani, S.A.; Wong, R. Is “Busy” Always Better? Time-Use Activities and Depressive Symptoms Among Older Mexican Adults. Innov. Aging 2020, 4, igaa030. [Google Scholar] [CrossRef]
- Pruchno, R.; Carr, D. Successful Aging 2.0: Resilience and Beyond. J. Gerontol. Ser. B 2017, 72, 201–203. [Google Scholar] [CrossRef]
- Wilson, R.S.; Mendes, D.; Bennett, D.; Bienias, J.L.; Evans, D. Depressive symptoms and cognitive decline in a community population of older persons. J. Neurol. Neurosurg. Psychiatry 2004, 75, 126–129. [Google Scholar]
- Perini, G.; Ramusino, M.C.; Sinforiani, E.; Bernini, S.; Petrachi, R.; Costa, A. Cognitive impairment in depression: Recent advances and novel treatments. Neuropsychiatr. Dis. Treat. 2019, 15, 1249–1258. [Google Scholar] [CrossRef] [Green Version]
- Yaffe, K.; Blackwell, T.; Gore, R.; Sands, L.; Reus, V.; Browner, W.S. Depressive Symptoms and Cognitive Decline in Nondemented Elderly Women. Arch. Gen. Psychiatry 1999, 56, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Aajami, Z.; Kazazi, L.; Troski, M.; Bahrami, M.; Borhaninejad, V. Relationship between Depression and Cognitive Impairment among Elderly: A Cross-sectional Study. J. Caring Sci. 2020, 9, 148–153. [Google Scholar] [CrossRef]
- HoleČek, M. Branched-chain amino acids in health and disease: Metabolism, alterations in blood plasma, and as supplements. Nutr. Metab. 2018, 15, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Blomstrand, E. A Role for Branched-Chain Amino Acids in Reducing Central Fatigue. J. Nutr. 2006, 136, 544S–547S. [Google Scholar] [CrossRef] [Green Version]
- Pedroso, J.A.; Zampieri, T.T.; Donato, J.J. Reviewing the Effects of l-Leucine Supplementation in the Regulation of Food Intake, Energy Balance, and Glucose Homeostasis. Nutrients 2015, 7, 3914–3937. [Google Scholar] [CrossRef] [Green Version]
- Murín, R.; Hamprecht, B. Metabolic and Regulatory Roles of Leucine in Neural Cells. Neurochem. Res. 2007, 33, 279–284. [Google Scholar] [CrossRef]
- García-Espinosa, M.A.; Wallin, R.; Hutson, S.M.; Sweatt, A.J. Widespread neuronal expression of branched-chain aminotransferase in the CNS: Implications for leucine/glutamate metabolism and for signaling by amino acids. J. Neurochem. 2007, 100, 1458–1468. [Google Scholar] [CrossRef]
- Sperringer, J.E.; Addington, A.; Hutson, S.M. Branched-Chain Amino Acids and Brain Metabolism. Neurochem. Res. 2017, 42, 1697–1709. [Google Scholar] [CrossRef]
- Haas, H.L.; Sergeeva, O.A.; Selbach, O. Histamine in the Nervous System. Physiol. Rev. 2008, 88, 1183–1241. [Google Scholar] [CrossRef]
- Kano, M.; Fukudo, S.; Tashiro, A.; Utsumi, A.; Tamura, D.; Itoh, M.; Iwata, R.; Tashiro, M.; Mochizuki, H.; Funaki, Y.; et al. Decreased histamine H1 receptor binding in the brain of depressed patients. Eur. J. Neurosci. 2004, 20, 803–810. [Google Scholar] [CrossRef]
- Sasahara, I.; Fujimura, N.; Nozawa, Y.; Furuhata, Y.; Sato, H. The effect of histidine on mental fatigue and cognitive performance in subjects with high fatigue and sleep disruption scores. Physiol. Behav. 2015, 147, 238–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, Y.-H.; Choi-Kwon, S.; Park, K.-A.; Suh, M.; Jung, Y. Nutrient deficiencies and depression in older adults according to sex: A cross sectional study. Nurs. Health Sci. 2016, 19, 88–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, J.; Yun, K.; Chae, J.-H.; Kim, T.-S. Association between Macronutrients Intake and Depression in the United States and South Korea. Front. Psychiatry 2020, 11, 207. [Google Scholar] [CrossRef] [Green Version]
- Nie, C.; He, T.; Zhang, W.; Zhang, G.; Ma, X. Branched Chain Amino Acids: Beyond Nutrition Metabolism. Int. J. Mol. Sci. 2018, 19, 954. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Features | Minimal Mean ± SD | Moderate Mean ± SD | Partial Wilks’ Lambda | F Value | p Value |
|---|---|---|---|---|---|
| Age (years) | 66 ± 6.0 | 67 ± 5.7 | 0.993 | 0.67 | 0.41 |
| Years of education | 8 ± 5.6 | 6 ± 4.0 | 0.976 | 2.35 | 0.12 |
| Age at Menarche | 12 ± 1.0 | 13 ± 1.0 | 0.992 | 0.958 | 0.35 |
| Age at Menopause | 48 ± 3.9 | 47 ± 4.0 | 0.998 | −1.022 | 0.25 |
| Weight (kg) | 72 ± 13.0 | 68 ± 7.0 | 0.981 | −0.426 | 0.10 |
| Size (m) | 1.5 ± 0.10 | 1.5 ± 0.10 | 0.978 | −0.805 | 0.92 |
| BMI (kg/m2) | 30 ± 5.0 | 28 ± 3.0 | 0.973 | 0.112 | 0.91 |
| TAS (mmHg) | 113 ± 11.0 | 127 ± 9.0 | 0.992 | 0.335 | 0.40 |
| TAD (mmHg) | 70 ± 6.0 | 75 ± 5.0 | 0.966 | 0.633 | 0.08 |
| Comorbidities | 2 ± 0.9 | 2 ± 1.0 | 0.998 | 0.22 | 0.64 |
| GDS depression scores | 3 ± 3.6 | 9 ± 5.7 | 0.715 | 38.20 | 0.0001 |
| BDI depression scores | 4.5 ± 2.6 | 18 ± 6.6 | 0.331 | 194.00 | 0.0001 |
| MMSE scores | 24.5 ± 4.3 | 26 ± 3.1 | 0.987 | 1.24 | 0.27 |
| Amino-Acids | Minimal Mean ± SD | Moderate Mean ± SD | Partial Wilks’ Lambda | F Value | p Value |
|---|---|---|---|---|---|
| l-Aspartate | 3.2 ± 4.2 | 4.2 ± 3.9 | 0.986 | 1.367 | 0.24 |
| l-Glutamate | 166.6 ± 153.2 | 173.6 ± 90.5 | 0.999 | 0.066 | 0.79 |
| l-Asparagine | 27.2 ± 7.0 | 26.6 ± 7.0 | 0.998 | 0.157 | 0.69 |
| l-Serine | 105.3 ± 24.8 | 110.2 ± 18.4 | 0.988 | 1.164 | 0.28 |
| l-Glutamine | 383.2 ± 139.2 | 361.8 ± 102.3 | 0.993 | 0.656 | 0.40 |
| l-Histidine | 62.0 ± 10.8 | 59.8 ± 8.3 | 0.988 | 1.158 | 0.28 |
| l-Glycine | 272.6 ± 74.2 | 251.9 ± 72.0 | 0.981 | 1.825 | 0.18 |
| l-Theonine | 104.9 ± 24.4 | 107.5 ± 28.8 | 0.998 | 0.237 | 0.62 |
| l-Cirtrulline | 23.8 ± 6.5 | 25.2 ± 7.1 | 0.990 | 1.007 | 0.31 |
| l-Arginine | 48.0 ± 21.3 | 50.7 ± 20.0 | 0.996 | 0.386 | 0.53 |
| l-Alanine + Taurine | 195.4 ± 45.3 | 192.8 ± 39.8 | 0.999 | 0.086 | 0.77 |
| GABA | 2.2 ± 2.0 | 2.6 ± 2.8 | 0.991 | 0.916 | 0.34 |
| l-Tyrosine | 58.6 ± 12.7 | 63.1 ± 16.9 | 0.979 | 2.009 | 0.16 |
| l-Valine | 182.8 ± 27.8 | 192.8 ± 32.3 | 0.973 | 2.635 | 0.10 |
| l-Methionine | 25.3 ± 8.0 | 28.7 ± 9.7 | 0.966 | 3.429 | 0.05 |
| l-Tryptophan | 32.7 ± 7.1 | 34.5 ± 9.7 | 0.984 | 1.552 | 0.21 |
| l-Phenylalanine | 51.5 ± 8.5 | 51.5 ± 8.1 | 1.000 | 0.002 | 0.96 |
| l-Isoleucine | 55.9 ± 14.5 | 49.3 ± 11.7 | 0.939 | 6.232 | 0.01 |
| l-Leucine | 123.0 ± 22.0 | 119.5 ± 20.2 | 0.993 | 0.651 | 0.42 |
| Predictor Variables | Standardized Coefficients | Structure Matrix | F Ratio | p Value |
|---|---|---|---|---|
| BDI depression scores | 0.961 | 0.827 | 194.00 | 0.0001 |
| MMSE scores | 0.386 | 0.066 | 102.35 | 0.0001 |
| Comorbidities | 0.396 | 0.028 | 74.60 | 0.0001 |
| l-Histidine | −0.196 | −0.064 | 58.87 | 0.0001 |
| GDS depression scores | 0.333 | 0.367 | 49.34 | 0.0001 |
| l-Isoleucine | 0.508 | 0.148 | 42.39 | 0.0001 |
| l-Leucine | −0.396 | 0.048 | 38.00 | 0.0001 |
| Canonical correlation | 0.864 | |||
| Effect size R2 | 0.74 | |||
| Eigenvalue | 2.956 | |||
| Wilks’ lambda | 0.253 | |||
| x2 | 127.20 | 0.0001 |
| Predictors | Moderate Symptoms | Minimal Symptoms |
|---|---|---|
| BDI depression scores GDS depression scores MMSE scores | 0.579 | −0.157 |
| 1.201 | 0.943 | |
| 2.243 | 1.903 | |
| Comorbidities l-histidine | 0.276 | 1.658 |
| 0.365 | 0.434 | |
| l-isoleucine l-leucine | 0.019 | −0.120 |
| 0.220 | 0.286 | |
| Fisher´s linear discrimination functions |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solís-Ortiz, S.; Arriaga-Avila, V.; Trejo-Bahena, A.; Guevara-Guzmán, R. Deficiency in the Essential Amino Acids l-Isoleucine, l-Leucine and l-Histidine and Clinical Measures as Predictors of Moderate Depression in Elderly Women: A Discriminant Analysis Study. Nutrients 2021, 13, 3875. https://doi.org/10.3390/nu13113875
Solís-Ortiz S, Arriaga-Avila V, Trejo-Bahena A, Guevara-Guzmán R. Deficiency in the Essential Amino Acids l-Isoleucine, l-Leucine and l-Histidine and Clinical Measures as Predictors of Moderate Depression in Elderly Women: A Discriminant Analysis Study. Nutrients. 2021; 13(11):3875. https://doi.org/10.3390/nu13113875
Chicago/Turabian StyleSolís-Ortiz, Silvia, Virginia Arriaga-Avila, Aurora Trejo-Bahena, and Rosalinda Guevara-Guzmán. 2021. "Deficiency in the Essential Amino Acids l-Isoleucine, l-Leucine and l-Histidine and Clinical Measures as Predictors of Moderate Depression in Elderly Women: A Discriminant Analysis Study" Nutrients 13, no. 11: 3875. https://doi.org/10.3390/nu13113875
APA StyleSolís-Ortiz, S., Arriaga-Avila, V., Trejo-Bahena, A., & Guevara-Guzmán, R. (2021). Deficiency in the Essential Amino Acids l-Isoleucine, l-Leucine and l-Histidine and Clinical Measures as Predictors of Moderate Depression in Elderly Women: A Discriminant Analysis Study. Nutrients, 13(11), 3875. https://doi.org/10.3390/nu13113875