
Two of a Kind? Mapping the Psychopathological Space between Obesity with and without Binge Eating Disorder


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Assessment of Eating-Related Symptomatology
2.4. Assessment of General Psychopathology
2.5. Assessment of Early Life Experiences
2.6. Data Aggregation and Analysis
3. Results
3.1. Participant Demographics
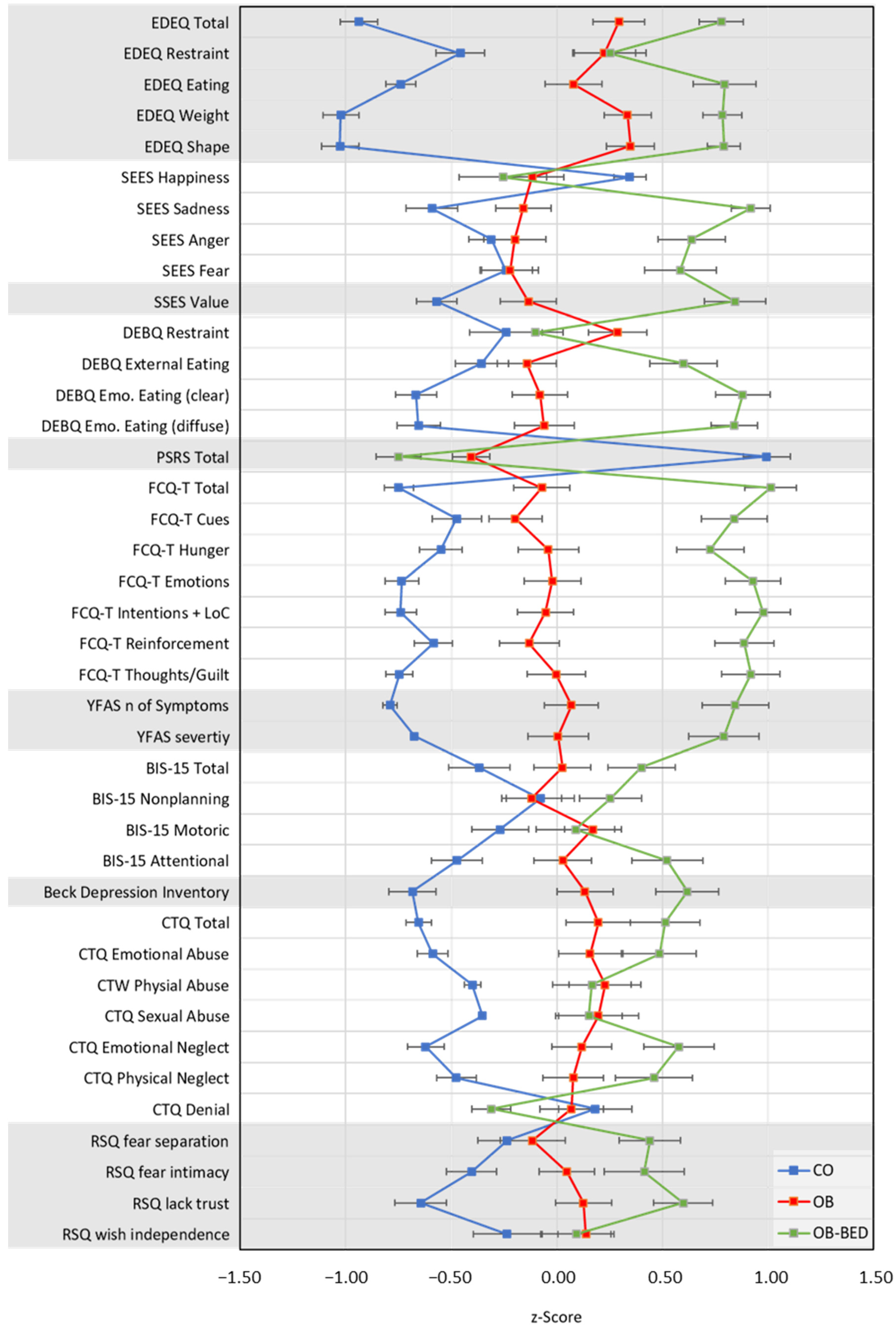
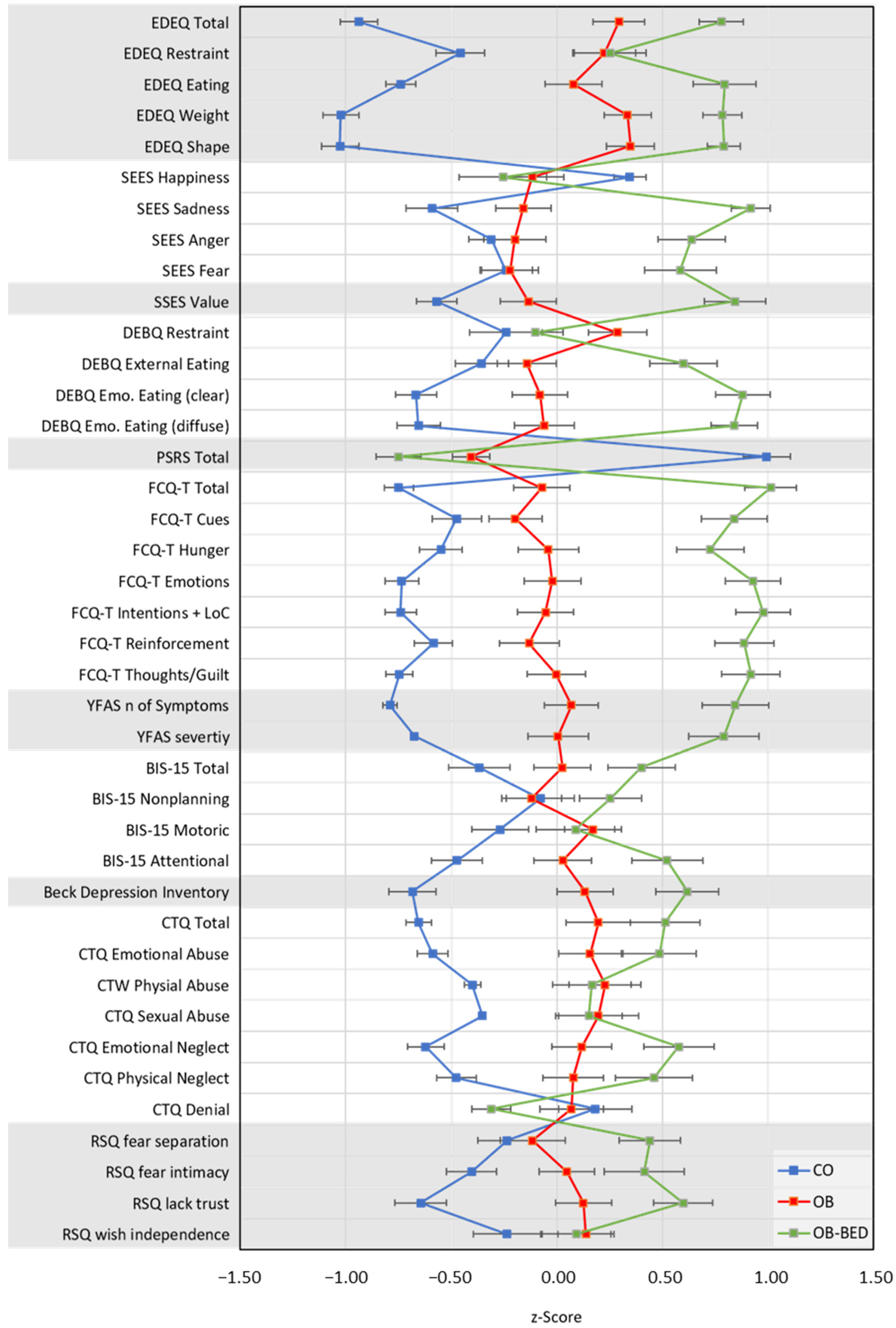
3.2. Eating-Related Symptomatology: EDEQ, SSES, SEES, DEBQ, PSRS, FCTQ, & YFAS 2.0
3.3. General Psychopathology: BIS-15 & BDI
3.4. Early Life Experiences: CTQ & RSQ
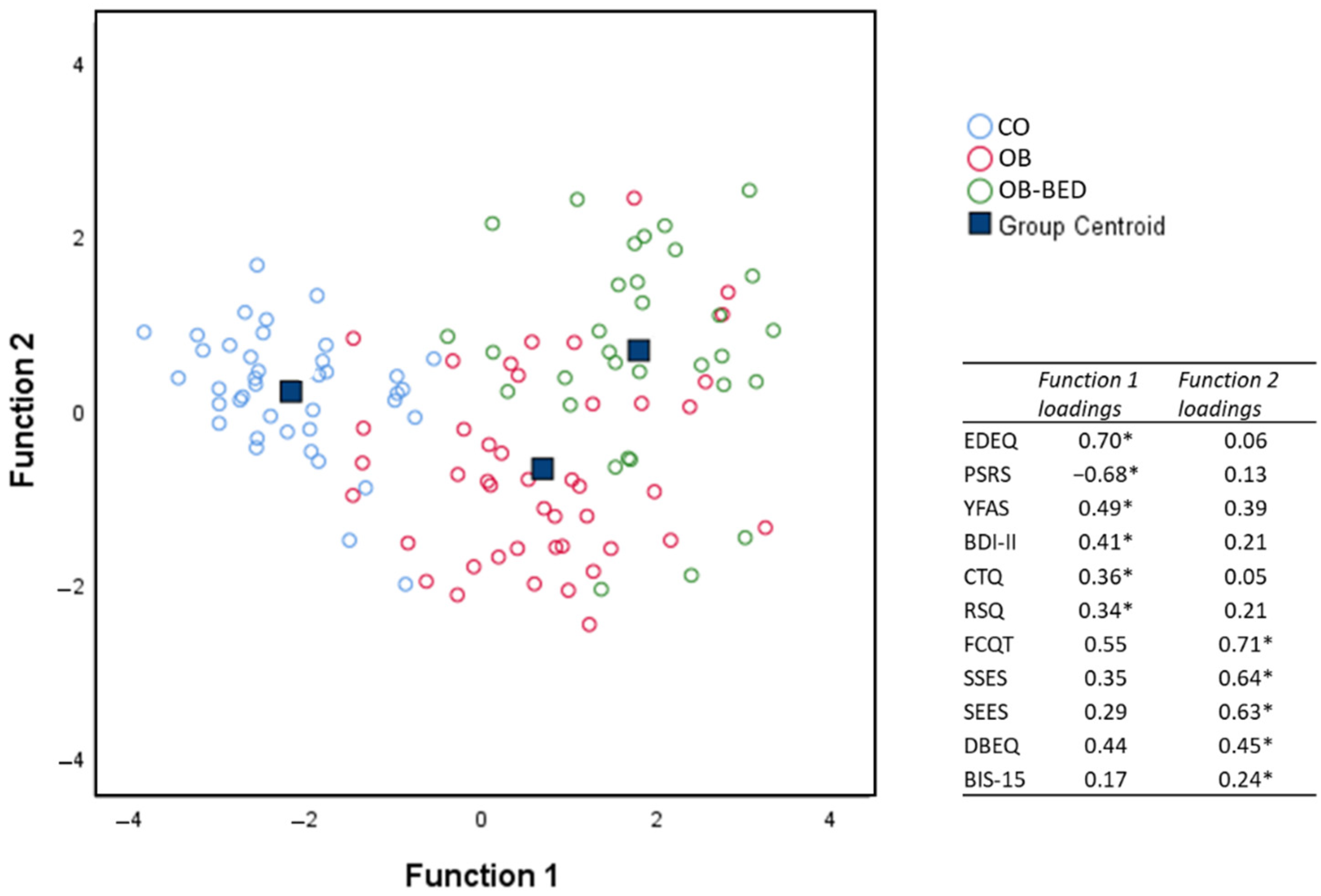
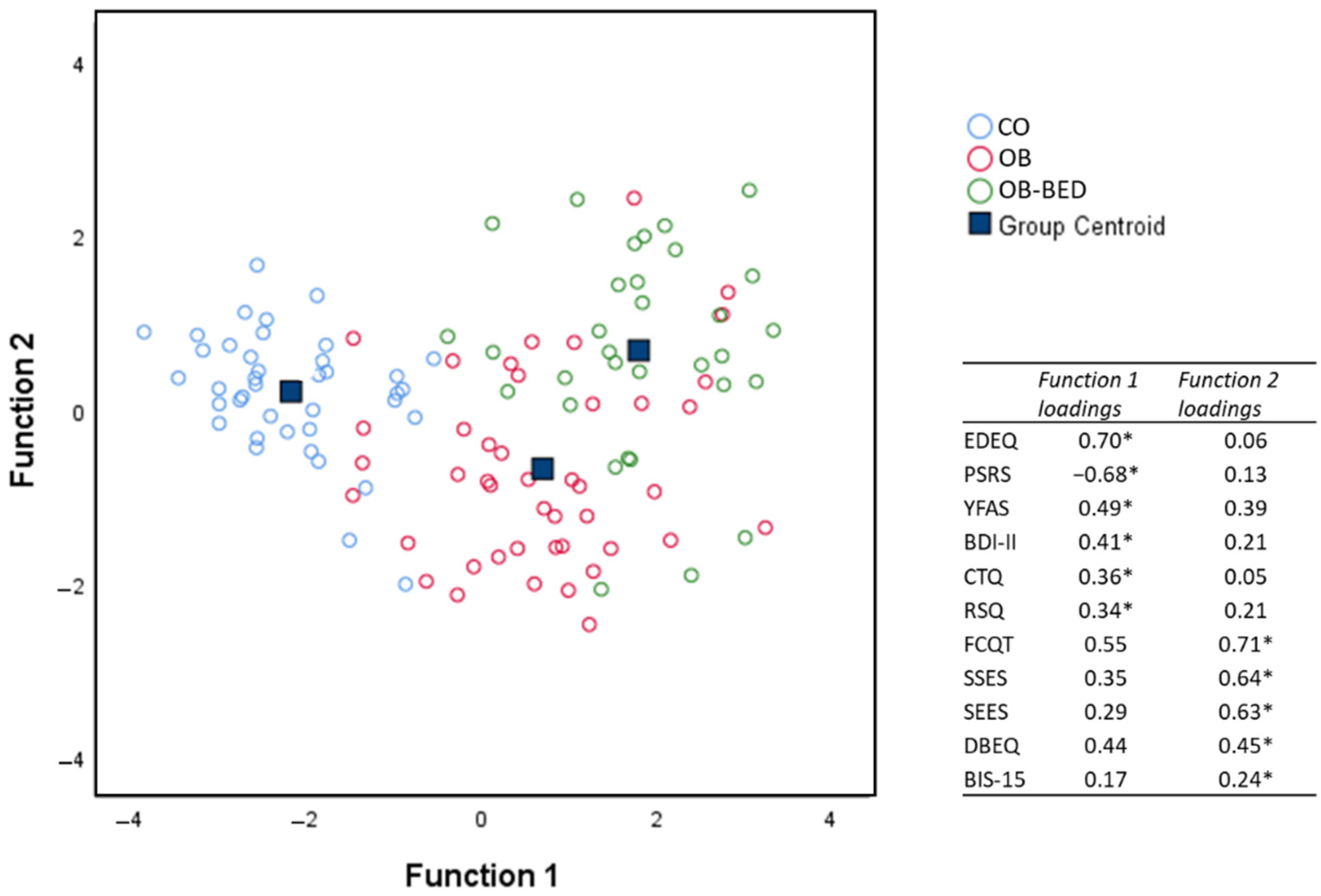
3.5. Discriminant Analysis
4. Discussion
4.1. Eating-Related Symptomatology
4.2. General Psychopathology
4.3. Early Life Experiences
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Variable | CO | OB | OB-BED |
|---|---|---|---|
| EDEQ | |||
| Total | 0.7 ± 0.86 | 2.5 ± 1.26 | 3.2 ± 0.90 |
| Restraint | 0.8 ± 1.13 | 1.8 ± 1.54 | 1.8 ± 1.49 |
| Eating Concern | 0.2 ± 0.71 | 1.5 ± 1.43 | 2.5 ± 1.35 |
| Weight Concern | 0.7 ± 1.01 | 3.1 ± 1.43 | 3.9 ± 1.00 |
| Shape Concern | 1.1 ± 1.08 | 3.6 ± 1.47 | 4.4 ± 0.84 |
| SEES | |||
| Happiness | 3.0 ± 0.28 | 2.7 ± 0.59 | 2.7 ± 0.71 |
| Sadness | 3.2 ± 0.60 | 3.5 ± 0.68 | 4.3 ± 0.42 |
| Anger | 2.9 ± 0.59 | 2.9 ± 0.88 | 3.6 ± 0.81 |
| Fear | 2.7 ± 0.70 | 2.7 ± 0.81 | 3.4 ± 0.88 |
| SSES | |||
| Total | 2.8 ± 0.53 | 3.1 ± 0.79 | 3.9 ± 0.74 |
| DEBQ | |||
| Restraint | 2.3 ± 0.91 | 2.7 ± 0.79 | 2.4 ± 0.65 |
| External Eating | 2.9 ± 0.61 | 3.0 ± 0.73 | 3.6 ± 0.73 |
| Emo. Eating total | 1.9 ± 0.69 | 2.6 ± 0.98 | 3.7 ± 0.74 |
| Emo. E. Clearly Labelled | 1.8 ± 0.73 | 2.5 ± 1.05 | 3.6 ± 0.90 |
| Emo. E. Diffused | 2.2 ± 0.78 | 2.9 ± 1.16 | 4.0 ± 0.78 |
| PSRS | |||
| Total | 14.8 ± 3.72 | 7.8 ± 2.99 | 6.1 ± 3.07 |
| FCQT | |||
| Total | 68.9 ± 18.81 | 97.2 ± 37.58 | 142.3 ± 30.03 |
| Cues | 10.2 ± 3.29 | 11.4 ± 3.64 | 15.8 ± 3.92 |
| Hunger | 8.8 ± 2.92 | 11.1 ± 4.29 | 14.4 ± 4.10 |
| Emotions | 6.5 ± 3.00 | 10.6 ± 5.24 | 16.1 ± 4.47 |
| Intentions/Lack of Control | 15.1 ± 5.41 | 22.8 ± 10.04 | 34.3 ± 8.57 |
| Reinforcement | 15.0 ± 5.43 | 19.2 ± 8.88 | 28.6 ± 7.71 |
| Thoughts/Guilt | 13.3 ± 4.91 | 22.1 ± 11.17 | 33.1 ± 9.71 |
| YFAS | |||
| No. of Symptoms | 0.1 ± 0.78 | 3.1 ± 3.15 | 5.8 ± 3.35 |
| Severity, n | |||
| None | 44 | 32 | 10 |
| Mild | 0 | 3 | 3 |
| Moderate | 0 | 2 | 5 |
| Severe | 0 | 12 | 19 |
| BIS | |||
| Total | 29.3 ± 6.40 | 31.9 ± 6.34 | 34.4 ± 6.42 |
| Nonplanning | 10.8 ± 3.40 | 10.6 ± 3.20 | 11.8 ± 2.84 |
| Motoric | 10.1 ± 2.44 | 11.3 ± 2.64 | 11.1 ± 3.14 |
| Attentional | 8.5 ± 2.45 | 10.0 ± 2.96 | 11.5 ± 3.13 |
| BDI | |||
| Total | 6.2 ± 7.61 | 14.7 ± 9.67 | 19.7 ± 9.30 |
| CTQ | |||
| Total | 31.9 ± 6.16 | 45.2 ± 16.76 | 50.2 ± 15.75 |
| Emotional Abuse | 7.2 ± 2.62 | 11.1 ± 5.58 | 12.9 ± 5.60 |
| Physical Abuse | 5.3 ± 0.78 | 7.1 ± 3.54 | 6.9 ± 3.32 |
| Sexual Abuse | 5.0 ± 0.15 | 7.0 ± 4.83 | 6.8 ± 3.47 |
| Emotional Neglect | 8.3 ± 3.02 | 12.2 ± 5.24 | 14.6 ± 5.32 |
| Physical Neglect | 6.1 ± 1.83 | 7.8 ± 3.03 | 8.9 ± 3.32 |
| Denial | 0.6 ± 0.99 | 0.5 ± 0.91 | 0.2 ± 0.48 |
| RSQ | |||
| Fear Separation | 2.5 ± 0.69 | 2.6 ± 0.79 | 3.0 ± 0.65 |
| Fear Intimacy | 2.2 ± 0.65 | 2.5 ± 0.76 | 2.8 ± 0.94 |
| Lack Trust | 2.0 ± 0.74 | 2.7 ± 0.85 | 3.2 ± 0.77 |
| Wish Independence | 3.8 ± 0.75 | 4.1 ± 0.67 | 4.0 ± 0.70 |
References
- Qian, J.; Wu, Y.; Liu, F.; Zhu, Y.; Jin, H.; Zhang, H.; Wan, Y.; Li, C.; Yu, D. An update on the prevalence of eating disorders in the general population: A systematic review and meta-analysis. Eat. Weight Disord. 2021. [Google Scholar] [CrossRef]
- American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 0-89042-555-8.
- McCuen-Wurst, C.; Ruggieri, M.; Allison, K.C. Disordered eating and obesity: Associations between binge-eating disorder, night-eating syndrome, and weight-related comorbidities. Ann. N. Y. Acad. Sci. 2018, 1411, 96–105. [Google Scholar] [CrossRef]
- World Health Organization. Country Profiles on Nutrition, Physical Activity and Obesity in the 53 WHO European Region Member States. Methodology and Summary; WHO Regional Office for Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- Kessler, R.C.; Berglund, P.A.; Chiu, W.T.; Deitz, A.C.; Hudson, J.I.; Shahly, V.; Aguilar-Gaxiola, S.; Alonso, J.; Angermeyer, M.C.; Benjet, C.; et al. The prevalence and correlates of binge eating disorder in the World Health Organization World Mental Health Surveys. Biol. Psychiatr. 2013, 73, 904–914. [Google Scholar] [CrossRef] [Green Version]
- Flegal, K.M.; Kit, B.K.; Orpana, H.; Graubard, B.I. Association of all-cause mortality with overweight and obesity using standard body mass index categories: A systematic review and meta-analysis. JAMA 2013, 309, 71–82. [Google Scholar] [CrossRef] [Green Version]
- Chu, D.-T.; Minh Nguyet, N.T.; Nga, V.T.; Thai Lien, N.V.; Vo, D.D.; Lien, N.; Nhu Ngoc, V.T.; Son, L.H.; Le, D.-H.; Nga, V.B.; et al. An update on obesity: Mental consequences and psychological interventions. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 155–160. [Google Scholar] [CrossRef]
- Villarejo, C.; Fernández-Aranda, F.; Jiménez-Murcia, S.; Peñas-Lledó, E.; Granero, R.; Penelo, E.; Tinahones, F.J.; Sancho, C.; Vilarrasa, N.; Montserrat-Gil De Bernabé, M.; et al. Lifetime obesity in patients with eating disorders: Increasing prevalence, clinical and personality correlates. Eur. Eat. Disord. Rev. 2012, 20, 250–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmisano, G.L.; Innamorati, M.; Vanderlinden, J. Life adverse experiences in relation with obesity and binge eating disorder: A systematic review. J. Behav. Addict. 2016, 5, 11–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caslini, M.; Bartoli, F.; Crocamo, C.; Dakanalis, A.; Clerici, M.; Carrà, G. Disentangling the association between child abuse and eating disorders: A systematic review and meta-analysis. Psychosom. Med. 2016, 78, 79–90. [Google Scholar] [CrossRef]
- Amianto, F.; Spalatro, A.V.; Rainis, M.; Andriulli, C.; Lavagnino, L.; Abbate-Daga, G.; Fassino, S. Childhood emotional abuse and neglect in obese patients with and without binge eating disorder: Personality and psychopathology correlates in adulthood. Psychiatr. Res. 2018, 269, 692–699. [Google Scholar] [CrossRef]
- Ehlert, U. Enduring psychobiological effects of childhood adversity. Psychoneuroendocrinology 2013, 38, 1850–1857. [Google Scholar] [CrossRef] [PubMed]
- Faber, A.; Dubé, L.; Knäuper, B. Attachment and eating: A meta-analytic review of the relevance of attachment for unhealthy and healthy eating behaviors in the general population. Appetite 2018, 123, 410–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tasca, G.A.; Balfour, L. Attachment and eating disorders: A review of current research. Int. J. Eat. Disord. 2014, 47, 710–717. [Google Scholar] [CrossRef]
- Maras, D.; Obeid, N.; Flament, M.; Buchholz, A.; Henderson, K.A.; Gick, M.; Goldfield, G.S. Attachment Style and Obesity: Disordered Eating Behaviors as a Mediator in a Community Sample of Canadian Youth. J. Dev. Behav. Pediatr. 2016, 37, 762–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yohn, S.E.; Galbraith, J.; Calipari, E.S.; Conn, P.J. Shared Behavioral and Neurocircuitry Disruptions in Drug Addiction, Obesity, and Binge Eating Disorder: Focus on Group I mGluRs in the Mesolimbic Dopamine Pathway. ACS Chem. Neurosci. 2019, 10, 2125–2143. [Google Scholar] [CrossRef]
- Giel, K.E.; Teufel, M.; Junne, F.; Zipfel, S.; Schag, K. Food-related impulsivity in obesity and binge eating disorder—A systematic update of the evidence. Nutrients 2017, 9, 1170. [Google Scholar] [CrossRef] [Green Version]
- Paslakis, G.; Kühn, S.; Grunert, S.; Erim, Y. Explicit and Implicit Approach vs. Avoidance Tendencies towards High vs. Low Calorie Food Cues in Patients with Obesity and Active Binge Eating Disorder. Nutrients 2017, 9, 1068. [Google Scholar] [CrossRef]
- Hege, M.A.; Stingl, K.T.; Kullmann, S.; Schag, K.; Giel, K.E.; Zipfel, S.; Preissl, H. Attentional impulsivity in binge eating disorder modulates response inhibition performance and frontal brain networks. Int. J. Obes. 2015, 39, 353–360. [Google Scholar] [CrossRef]
- Hernandez, D.; Mehta, N.; Geliebter, A. Meal-Related Acyl and Des-Acyl Ghrelin and Other Appetite-Related Hormones in People with Obesity and Binge Eating. Obesity 2019, 27, 629–635. [Google Scholar] [CrossRef]
- Schulz, S.; Laessle, R.G. Associations of negative affect and eating behaviour in obese women with and without binge eating disorder. Eat. Weight Disord. 2010, 15, e287–e293. [Google Scholar] [CrossRef] [PubMed]
- Krehbiel, J.; Halbeisen, G.; Kühn, S.; Erim, Y.; Paslakis, G. Too hot to handle: Mood states moderate implicit approach vs. avoidance tendencies toward food cues in patients with obesity and active binge eating disorder. J. Psychiatr. Res. 2021, 143, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.B.; Jones, P.J.; Dreier, M.; Elliott, H.; Grilo, C.M. Core psychopathology of treatment-seeking patients with binge-eating disorder: A network analysis investigation. Psychol. Med. 2019, 49, 1923–1928. [Google Scholar] [CrossRef]
- Lewer, M.; Bauer, A.; Hartmann, A.; Vocks, S. Different Facets of Body Image Disturbance in Binge Eating Disorder: A Review. Nutrients 2017, 9, 1294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rø, Ø.; Reas, D.L.; Rosenvinge, J. The impact of age and BMI on Eating Disorder Examination Questionnaire (EDE-Q) scores in a community sample. Eat. Behav. 2012, 13, 158–161. [Google Scholar] [CrossRef] [PubMed]
- Wiedemann, A.A.; Ivezaj, V.; Barnes, R.D. Characterizing emotional overeating among patients with and without binge-eating disorder in primary care. Gen. Hosp. Psychiatr. 2018, 55, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Zeeck, A.; Stelzer, N.; Linster, H.W.; Joos, A.; Hartmann, A. Emotion and eating in binge eating disorder and obesity. Eur. Eat. Disord. Rev. 2010, 19, 426–437. [Google Scholar] [CrossRef]
- Ricca, V.; Castellini, G.; Lo Sauro, C.; Ravaldi, C.; Lapi, F.; Mannucci, E.; Rotella, C.M.; Faravelli, C. Correlations between binge eating and emotional eating in a sample of overweight subjects. Appetite 2009, 53, 418–421. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.; Levitan, R.D.; Carter, J.; Kaplan, A.S.; Reid, C.; Curtis, C.; Patte, K.; Kennedy, J.L. Personality and eating behaviors: A case–control study of binge eating disorder. Int. J. Eat. Disord. 2008, 41, 243–250. [Google Scholar] [CrossRef]
- Pinaquy, S.; Chabrol, H.; Simon, C.; Louvet, J.P.; Barbe, P. Emotional eating, alexithymia, and binge-eating disorder in obese women. Obes. Res. 2003, 11, 195–201. [Google Scholar] [CrossRef]
- Meule, A.; Reichenberger, J.; Blechert, J. Development and preliminary validation of the Salzburg Stress Eating Scale. Appetite 2018, 120, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Agüera, Z.; Lozano-Madrid, M.; Mallorquí-Bagué, N.; Jiménez-Murcia, S.; Menchón, J.M.; Fernández-Aranda, F. A review of binge eating disorder and obesity. Neuropsychiatrie 2021, 35, 57–67. [Google Scholar] [CrossRef]
- Johnson, F.; Pratt, M.; Wardle, J. Dietary restraint and self-regulation in eating behavior. Int. J. Obes. 2012, 36, 665–674. [Google Scholar] [CrossRef] [Green Version]
- Spoor, S.T.P.; Stice, E.; Bekker, M.H.J.; Van Strien, T.; Croon, M.A.; Van Heck, G.L. Relations between dietary restraint, depressive symptoms, and binge eating: A longitudinal study. Int. J. Eat. Disord. 2006, 39, 700–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meule, A.; Lutz, A.; Vögele, C.; Kübler, A. Food cravings discriminate differentially between successful and unsuccessful dieters and non-dieters. Validation of the Food Cravings Questionnaires in German. Appetite 2012, 58, 88–97. [Google Scholar] [CrossRef]
- Meule, A. Twenty Years of the Food Cravings Questionnaires: A Comprehensive Review. Curr. Addict. Rep. 2020, 7, 30–43. [Google Scholar] [CrossRef] [Green Version]
- Van den Eynde, F.; Koskina, A.; Syrad, H.; Guillaume, S.; Broadbent, H.; Campbell, I.C.; Schmidt, U. State and trait food craving in people with bulimic eating disorders. Eat. Behav. 2012, 13, 414–417. [Google Scholar] [CrossRef]
- Carter, J.C.; Van Wijk, M.; Rowsell, M. Symptoms of ‘food addiction’ in binge eating disorder using the Yale Food Addiction Scale version 2.0. Appetite 2019, 133, 362–369. [Google Scholar] [CrossRef]
- Davis, C.; Curtis, C.; Levitan, R.D.; Carter, J.C.; Kaplan, A.S.; Kennedy, J.L. Evidence that “food addiction” is a valid phenotype of obesity. Appetite 2011, 57, 711–717. [Google Scholar] [CrossRef]
- Davis, C. Compulsive Overeating as an Addictive Behavior: Overlap between Food Addiction and Binge Eating Disorder. Curr. Obes. Rep. 2013, 2, 171–178. [Google Scholar] [CrossRef] [Green Version]
- Penzenstadler, L.; Soares, C.; Karila, L.; Khazaal, Y. Systematic Review of Food Addiction as Measured with the Yale Food Addiction Scale: Implications for the Food Addiction Construct. Curr. Neuropharmacol. 2018, 17, 526–538. [Google Scholar] [CrossRef]
- Hession, M.; Rolland, C.; Kulkarni, U.; Wise, A.; Broom, J. Systematic review of randomized controlled trials of low-carbohydrate vs. low-fat/low-calorie diets in the management of obesity and its comorbidities. Obes. Rev. 2009, 10, 36–50. [Google Scholar] [CrossRef]
- Brownley, K.A.; Berkman, N.D.; Peat, C.M.; Lohr, K.N.; Cullen, K.E.; Bann, C.M.; Bulik, C.M. Binge-Eating Disorder in Adults: A Systematic Review and Meta-analysis. Ann. Intern. Med. 2016, 165, 409–420. [Google Scholar] [CrossRef] [Green Version]
- White, M.A.; Kalarchian, M.A.; Masheb, R.M.; Marcus, M.D.; Grilo, C.M. Loss of control over eating predicts outcomes in bariatric surgery patients: A prospective, 24-month follow-up study. J. Clin. Psychiatr. 2010, 71, 175–184. [Google Scholar] [CrossRef] [Green Version]
- Hilbert, A.; Petroff, D.; Herpertz, S.; Pietrowsky, R.; Tuschen-Caffier, B.; Vocks, S.; Schmidt, R. Meta-Analysis of the Efficacy of Psychological and Medical Treatments for Binge-Eating Disorder. J. Consult. Clin. Psychol. 2019, 87, 91–105. [Google Scholar] [CrossRef] [PubMed]
- Grilo, C.M. Psychological and Behavioral Treatments for Binge-Eating Disorder. J. Clin. Psychiatr. 2017, 78 (Suppl. S1), 20–24. [Google Scholar] [CrossRef]
- Escandón-Nagel, N.; Peró, M.; Grau, A.; Soriano, J.; Feixas, G. Alimentación emocional y conflictos cognitivos como predictores del trastorno por atracón en pacientes con obesidad. Int. J. Clin. Health Psychol. 2018, 18, 52–59. [Google Scholar] [CrossRef]
- Gearhardt, A.; White, M.; Potenza, M. Binge eating disorder and food addiction. Curr. Drug Abuse Rev. 2011, 4, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meule, A. German Version of the Eating Disorder Diagnostic Scale—DSM-5 Version 2015. Available online: https://adrianmeule.files.wordpress.com/2013/05/eddsgerman.pdf (accessed on 10 October 2021).
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Fairburn, C.G.; Beglin, S.J. Assessment of eating disorders: Interview or self-report questionnaire? Int. J. Eat. Disord. 1994, 16, 363–370. [Google Scholar] [PubMed]
- Fairburn, C.G.; Cooper, Z. The eating disorder examination. In Binge Eating: Nature, Assessment and Treatment; Fairburn, C.G., Wilson, G.T., Eds.; Guilford Press: New York, NY, USA, 1993; pp. 317–360. [Google Scholar]
- Hilbert, A.; Tuschen-Caffier, B. Eating Disorder Examination–Questionnaire: Deutschsprachige Übersetzung; Münster Verlag Psychotherapie: Münster, Germany, 2006. [Google Scholar]
- Meule, A.; Reichenberger, J.; Blechert, J. Development and Preliminary Validation of the Salzburg Emotional Eating Scale. Front. Psychol. 2018, 9, 88. [Google Scholar] [CrossRef]
- Reichenberger, J.; Pannicke, B.; Arend, A.K.; Petrowski, K.; Blechert, J. Does stress eat away at you or make you eat? EMA measures of stress predict day to day food craving and perceived food intake as a function of trait stress-eating. Psychol. Health 2021, 36, 129–147. [Google Scholar] [CrossRef]
- van Strien, T.; Frijters, J.E.R.; Bergers, G.P.A.; Defares, P.B. The Dutch Eating Behavior Questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. Int. J. Eat. Disord. 1986, 5, 295–315. [Google Scholar] [CrossRef]
- Nagl, M.; Hilbert, A.; de Zwaan, M.; Braehler, E.; Kersting, A. The German Version of the Dutch Eating Behavior Questionnaire: Psychometric Properties, Measurement Invariance, and Population-Based Norms. PLoS ONE 2016, 11, e0162510. [Google Scholar] [CrossRef] [PubMed]
- Fishbach, A.; Friedman, R.S.; Kruglanski, A.W. Leading us not unto temptation: Momentary allurements elicit overriding goal activation. J. Pers. Soc. Psychol. 2003, 84, 296–309. [Google Scholar] [CrossRef]
- Meule, A.; Papies, E.K.; Kübler, A. Differentiating between successful and unsuccessful dieters. Validity and reliability of the Perceived Self-Regulatory Success in Dieting Scale. Appetite 2012, 58, 822–826. [Google Scholar] [CrossRef] [PubMed]
- Cepeda-Benito, A.; Gleaves, D.; Williams, T.; Erath, S. The development and validation of the State and Trait Food-Cravings Questionnaire. Behav. Ther. 2000, 31, 151–173. [Google Scholar] [CrossRef]
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Development of the Yale Food Addiction Scale Version 2.0. Psychol. Addict. Behav. J. Soc. Psychol. Addict. Behav. 2016, 30, 113–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meule, A.; Müller, A.; Gearhardt, A.N.; Blechert, J. German version of the Yale Food Addiction Scale 2.0: Prevalence and correlates of “food addiction” in students and obese individuals. Appetite 2017, 115, 54–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meule, A.; Vögele, C.; Kübler, A. Psychometric evaluation of the German Barratt Impulsiveness Scale-Short Version (BIS-15). Diagnostica 2011, 57, 126–133. [Google Scholar] [CrossRef]
- Hautzinger, M.; Keller, F.; Kühner, C. BDI-II. Beck-Depressions-Inventar, 2nd ed.; Pearson: London, UK, 2009. [Google Scholar]
- Bader, K.; Hänny, C.; Schäfer, V.; Neuckel, A.; Kuhl, C. Childhood Trauma Questionnaire-Psychometrische Eigenschaften einer deutschsprachigen Version. [Childhood Trauma Questionnaire-Psychometric properties of a German version]. Z. Klin. Psychol. Psychother. 2009, 38, 223–230. [Google Scholar] [CrossRef]
- Steffanowski, A.; Oppl, M.; Meyerberg, J.; Juergen, S.; Wittmann, W.; Nübling, R. Psychometrische Überprüfung einer Deutschsprachigen Version des Relationship Scales Questionaire (RSQ); Psychosozial: Giessen, Germany, 2001; pp. 320–342. ISBN 3-89806-081-0. [Google Scholar]
- Hilbert, A.; de Zwaan, M.; Braehler, E. How Frequent Are Eating Disturbances in the Population? Norms of the Eating Disorder Examination-Questionnaire. PLoS ONE 2012, 7, e29125. [Google Scholar] [CrossRef] [Green Version]
- Özdin, S.; Karabekiroğlu, A.; Özbalcı, G.S.; Aker, A.A. The effect of cognitive symptoms in binge eating disorder on depression and self-esteem: A cross-sectional study. Eat. Weight Disord. 2021, 26, 1483–1489. [Google Scholar] [CrossRef] [PubMed]
- Çalışır, S.; Çalışır, A.; Arslan, M.; İnanlı, İ.; Çalışkan, A.M.; Eren, İ. Assessment of depressive symptoms, self-esteem, and eating psychopathology after laparoscopic sleeve gastrectomy: 1-year follow-up and comparison with healthy controls. Eat. Weight Disord. 2020, 25, 1515–1523. [Google Scholar] [CrossRef]
- Grilo, C.M.; White, M.A.; Gueorguieva, R.; Wilson, G.T.; Masheb, R.M. Predictive significance of the overvaluation of shape/weight in obese patients with binge eating disorder: Findings from a randomized controlled trial with 12-month follow-up. Psychol. Med. 2013, 43, 1335–1344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gagnon-Girouard, M.P.; Bégin, C.; Provencher, V.; Tremblay, A.; Boivin, S.; Lemieux, S. Can we apply the dual-pathway model of overeating to a population of weight-preoccupied overweight women? Int. J. Eat. Disord. 2009, 42, 244–252. [Google Scholar] [CrossRef]
- Zambrowicz, R.; Schebendach, J.; Sysko, R.; Mayer, L.E.S.; Walsh, B.T.; Steinglass, J.E. Relationship between three factor eating questionnaire-restraint subscale and food intake. Int. J. Eat. Disord. 2019, 52, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Meule, A.; Richard, A.; Schnepper, R.; Reichenberger, J.; Georgii, C.; Naab, S.; Voderholzer, U.; Blechert, J. Emotion regulation and emotional eating in anorexia nervosa and bulimia nervosa. Eat. Disord. 2021, 29, 175–191. [Google Scholar] [CrossRef] [Green Version]
- Schulz, S.; Laessle, R.G. Stress-induced laboratory eating behavior in obese women with binge eating disorder. Appetite 2012, 58, 457–461. [Google Scholar] [CrossRef]
- Benzerouk, F.; Djerada, Z.; Bertin, E.; Barrière, S.; Gierski, F.; Kaladjian, A. Contributions of emotional overload, emotion dysregulation, and impulsivity to eating patterns in obese patients with binge eating disorder and seeking bariatric surgery. Nutrients 2020, 12, 3099. [Google Scholar] [CrossRef]
- Mason, T.B.; Lewis, R.J. Profiles of Binge Eating: The Interaction of Depressive Symptoms, Eating Styles, and Body Mass Index. Eat. Disord. 2014, 22, 450–460. [Google Scholar] [CrossRef]
- Ferrer-Garcia, M.; Pla-Sanjuanelo, J.; Dakanalis, A.; Vilalta-Abella, F.; Riva, G.; Fernandez-Aranda, F.; Sánchez, I.; Ribas-Sabaté, J.; Andreu-Gracia, A.; Escandón-Nagel, N.; et al. Eating behavior style predicts craving and anxiety experienced in food-related virtual environments by patients with eating disorders and healthy controls. Appetite 2017, 117, 284–293. [Google Scholar] [CrossRef] [Green Version]
- Innamorati, M.; Imperatori, C.; Balsamo, M.; Tamburello, S.; Belvederi Murri, M.; Contardi, A.; Tamburello, A.; Fabbricatore, M. Food cravings questionnaire-trait (FCQ-T) discriminates between obese and overweight patients with and without binge eating tendencies: The italian version of the FCQ-T. J. Pers. Assess. 2014, 96, 632–639. [Google Scholar] [CrossRef] [PubMed]
- Grilo, C.M.; White, M.A.; Barnes, R.D.; Masheb, R.M. Psychiatric disorder co-morbidity and correlates in an ethnically diverse sample of obese patients with binge eating disorder in primary care settings. Compr. Psychiatr. 2013, 54, 209–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fauconnier, M.; Rousselet, M.; Brunault, P.; Thiabaud, E.; Lambert, S.; Rocher, B.; Challet-Bouju, G.; Grall-Bronnec, M. Food addiction among female patients seeking treatment for an eating disorder: Prevalence and associated factors. Nutrients 2020, 12, 1897. [Google Scholar] [CrossRef]
- Kessler, R.M.; Hutson, P.H.; Herman, B.K.; Potenza, M.N. The neurobiological basis of binge-eating disorder. Neurosci. Biobehav. Rev. 2016, 63, 223–238. [Google Scholar] [CrossRef] [Green Version]
- Bénard, M.; Camilleri, G.; Etilé, F.; Méjean, C.; Bellisle, F.; Reach, G.; Hercberg, S.; Péneau, S. Association between Impulsivity and Weight Status in a General Population. Nutrients 2017, 9, 217. [Google Scholar] [CrossRef]
- Loeber, S.; Rustemeier, M.; Paslakis, G.; Pietrowsky, R.; Müller, A.; Herpertz, S. Mood and restrained eating moderate food-associated response inhibition in obese individuals with binge eating disorder. Psychiatr. Res. 2018, 264, 346–353. [Google Scholar] [CrossRef]
- Smith, C.E.; Hawkins, M.A.W.; Williams-Kerver, G.A.; Duncan, J. Depression subtypes, binge eating, and weight loss in bariatric surgery candidates. Surg. Obes. Relat. Dis. 2020, 16, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Udo, T.; McKee, S.A.; Grilo, C.M. Factor structure and clinical utility of the Beck Depression Inventory in patients with binge eating disorder and obesity. Gen. Hosp. Psychiatr. 2015, 37, 120–125. [Google Scholar] [CrossRef] [Green Version]
- Meule, A.; Blechert, J. Interactive and indirect effects of trait impulsivity facets on body mass index. Appetite 2017, 118, 60–65. [Google Scholar] [CrossRef]
- Belli, H.; Ural, C.; Akbudak, M.; Sagaltıcı, E. Levels of childhood traumatic experiences and dissociative symptoms in extremely obese patients with and without binge eating disorder. Nord. J. Psychiatr. 2019, 73, 527–531. [Google Scholar] [CrossRef]
- Palmisano, G.L.; Innamorati, M.; Sarracino, D.; Bosco, A.; Pergola, F.; Scaltrito, D.; Giorgio, B.; Vanderlinden, J. Trauma and dissociation in obese patients with and without binge eating disorder: A case–control study. Cogent Psychol. 2018, 5, 1–20. [Google Scholar] [CrossRef]
- Han, S.; Carole Pistole, M. College student binge eating: Insecure attachment and emotion regulation. J. Coll. Stud. Dev. 2014, 55, 16–29. [Google Scholar] [CrossRef]
- Shakory, S.; Van Exan, J.; Mills, J.S.; Sockalingam, S.; Keating, L.; Taube-Schiff, M. Binge eating in bariatric surgery candidates: The role of insecure attachment and emotion regulation. Appetite 2015, 91, 69–75. [Google Scholar] [CrossRef]
- Blomquist, K.K.; Ansell, E.B.; White, M.A.; Masheb, R.M.; Grilo, C.M. Interpersonal problems and developmental trajectories of binge eating disorder. Compr. Psychiatr. 2012, 53, 1088–1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Variable | CO | OB | OB-BED |
|---|---|---|---|
| n (m, f) | 14, 30 | 17, 33 | 10, 27 |
| age | 41.7 ± 16.8 | 46.1 ± 10.7 | 39.3 ± 11.2 |
| BMI (kg/m2) | 22.5 ± 1.6 | 42.9 ± 9.1 | 46.3 ± 9.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sommer, L.M.; Halbeisen, G.; Erim, Y.; Paslakis, G. Two of a Kind? Mapping the Psychopathological Space between Obesity with and without Binge Eating Disorder. Nutrients 2021, 13, 3813. https://doi.org/10.3390/nu13113813
Sommer LM, Halbeisen G, Erim Y, Paslakis G. Two of a Kind? Mapping the Psychopathological Space between Obesity with and without Binge Eating Disorder. Nutrients. 2021; 13(11):3813. https://doi.org/10.3390/nu13113813
Chicago/Turabian StyleSommer, Laura Marie, Georg Halbeisen, Yesim Erim, and Georgios Paslakis. 2021. "Two of a Kind? Mapping the Psychopathological Space between Obesity with and without Binge Eating Disorder" Nutrients 13, no. 11: 3813. https://doi.org/10.3390/nu13113813
APA StyleSommer, L. M., Halbeisen, G., Erim, Y., & Paslakis, G. (2021). Two of a Kind? Mapping the Psychopathological Space between Obesity with and without Binge Eating Disorder. Nutrients, 13(11), 3813. https://doi.org/10.3390/nu13113813