
An Evaluation of Omega-3 Status and Intake in Canadian Elite Rugby 7s Players

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Design
2.3. Food Frequency Questionnaire
2.4. Blood Collection and Preparation
2.5. Blood Analysis
2.6. Statistical Analysis
3. Results
3.1. Participant Data
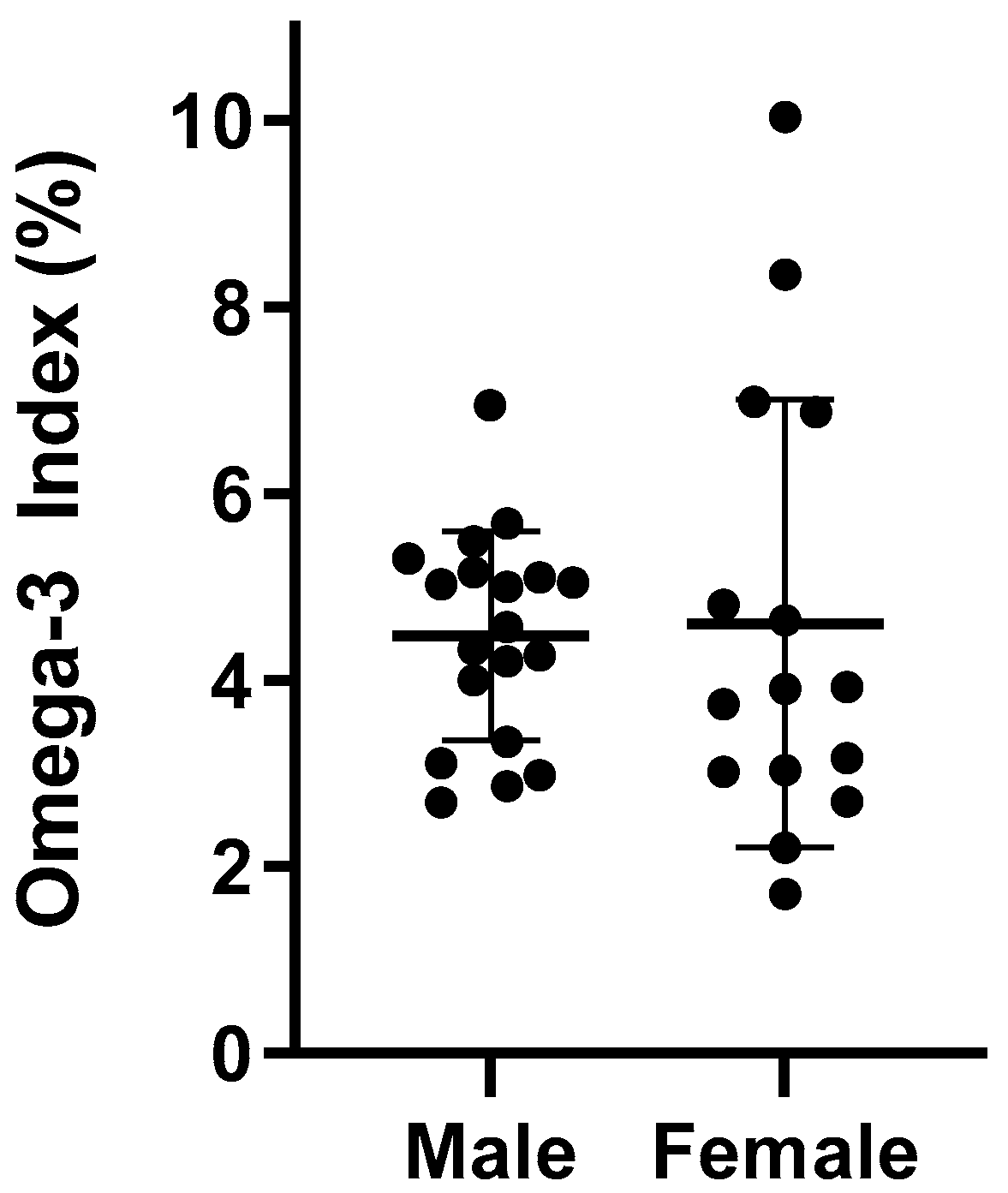
3.2. Erythrocyte Fatty Acids and Omega 3 Index (O3I)
3.3. Dietary Intake
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fuller, C.W.; Taylor, A.; Raftery, M. 2016 Rio Olympics: An epidemiological study of the men’s and women’s Rugby-7s tournaments. Br. J. Sports Med. 2017, 51, 1272–1278. [Google Scholar] [CrossRef]
- Fuller, C.W.; Taylor, A.; Raftery, M. Epidemiology of concussion in men’s elite Rugby-7s (Sevens World Series) and Rugby-15s (Rugby World Cup, Junior World Championship and Rugby Trophy, Pacific Nations Cup and English Premiership). Br. J. Sports Med. 2015, 49, 478–483. [Google Scholar] [CrossRef]
- Lopez, V.; Ma, R.; Weinstein, M.G.; Cantu, R.C.; Myers, L.S.D.; Nadkar, N.S.; Victoria, C.; Allen, A.A. Concussive Injuries in Rugby 7s: An American Experience and Current Review. Med. Sci. Sports Exerc. 2016, 48, 1320–1330. [Google Scholar] [CrossRef]
- Gardner, A.J.; Iverson, G.L.; Williams, W.H.; Baker, S.; Stanwell, P. A systematic review and meta-analysis of concussion in Rugby Union. Sports Med. 2014, 44, 1717–1731. [Google Scholar] [CrossRef]
- Arterburn, L.M.; Hall, E.B.; Oken, H. Distribution, interconversion, and dose response of n-3 fatty acids in humans. Am. J. Clin. Nutr. 2006, 83, 1467S–1476S. [Google Scholar] [CrossRef] [PubMed]
- Bailes, J.E.; Mills, J.D. Docosahexaenoic acid reduces traumatic axonal injury in a rodent head injury model. J. Neurotrauma 2010, 27, 1617–1624. [Google Scholar] [CrossRef] [Green Version]
- Mills, J.D.; Hadley, K.; Bailes, J.E. Dietary supplementation with the Omega-3 fatty acid docosahexaenoic acid in traumatic brain injury. Neurosurgery 2011, 68, 474–481. [Google Scholar] [CrossRef] [Green Version]
- Oliver, J.M.; Anzalone, A.J.; Turner, S.M. Protection before Impact: The Potential Neuroprotective Role of Nutritional Supplementation in Sports-Related Head Trauma. Sports Med. 2018, 48, 39–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schober, M.E.; Requena, D.F.; Abdullah, O.M.; Casper, T.C.; Beachy, J.; Malleske, D.; Pauly, J.R. Dietary Docosahexaenoic Acid Improves Cognitive Function, Tissue Sparing, and Magnetic Resonance Imaging Indices of Edema and White Matter Injury in the Immature Rat after Traumatic Brain Injury. J. Neurotrauma 2016, 33, 390–402. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 36, 2315–2381. [Google Scholar] [CrossRef]
- Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; National Academy Press: Washington, DC, USA, 2005. [Google Scholar] [CrossRef]
- Stark, K.D.; Van Elswyk, M.E.; Higgins, M.R.; Weatherford, C.A.; Salem, N. Global survey of the omega-3 fatty acids, docosahexaenoic acid and eicosapentaenoic acid in the blood stream of healthy adults. Prog. Lipid Res. 2016, 63, 132–152. [Google Scholar] [CrossRef]
- Papanikolaou, Y.; Brooks, J.; Reider, C.; Fulgoni, V.L. U.S. adults are not meeting recommended levels for fish and omega-3 fatty acid intake: Results of an analysis using observational data from NHANES 2003–2008. Nutr. J. 2014, 13, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Wilson, P.B.; Madrigal, L.A. Associations between Whole Blood and Dietary Omega-3 Polyunsaturated Fatty Acid Levels in Collegiate Athletes. Int. J. Sport Nutr. Exerc. Metab. 2016, 26, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Ritz, P.P.; Rogers, M.B.; Zabinsky, J.S.; Hedrick, V.E.; Rockwell, J.A.; Rimer, E.G.; Kostelnik, S.B.; Hulver, M.W.; Rockwell, M.S. Dietary and biological assessment of the omega-3 status of collegiate athletes: A cross-sectional analysis. PLoS ONE 2020, 15, e0228834. [Google Scholar] [CrossRef] [PubMed]
- Vannice, G.; Rasmussen, H. Position of the Academy of Nutrition and Dietetics: Dietary Fatty Acids for Healthy Adults. J. Acad. Nutr. Diet. 2014, 114, 136–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maughan, R.J.; Burke, L.M.; Dvorak, J.; Larson-Meyer, D.E.; Peeling, P.; Phillips, S.M.; Rawson, E.S.; Walsh, N.P.; Garthe, I.; Geyer, H.; et al. IOC consensus statement: Dietary supplements and the high-performance athlete. Br. J. Sports Med. 2018, 52, 439–455. [Google Scholar] [CrossRef]
- Harris, W.S. The omega-3 index: Clinical utility for therapeutic intervention. Curr. Cardiol. Rep. 2010, 12, 503–508. [Google Scholar] [CrossRef]
- Von Schacky, C. Omega-3 index and cardiovascular health. Nutrients 2014, 6, 799–814. [Google Scholar] [CrossRef] [PubMed]
- Langlois, K.; Ratnayake, W.M.N. Omega-3 Index of Canadian adults. Health Rep. 2015, 26, 3–11. [Google Scholar] [PubMed]
- Von Schacky, C.; Kemper, M.; Haslbauer, R.; Halle, M. Low omega-3 index in 106 German elite winter endurance athletes: A pilot study. International. J. Sport Nutr. Exerc. Metab. 2014, 24, 559–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anzalone, A.; Carbuhn, A.; Jones, L.; Gallop, A.; Smith, A.; Johnson, P.; Swearingen, L.; Moore, C.; Rimer, E.; McBeth, J.; et al. The omega-3 index in National collegiate athletic Association division I collegiate football athletes. J. Athl. Train. 2019, 54, 7–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sublette, M.E.; Segal-Isaacson, C.J.; Cooper, T.B.; Fekri, S.; Vanegas, N.; Galfalvy, H.C.; Oquendo, M.A.; Maan, J.J. Validation of a food frequency questionnaire to assess intake of n-3 polyunsaturated fatty acids in subjects with and without major depressive disorder. J. Am. Diet Assoc. 2011, 111, 117–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Cancer Institute Applied Research Program. DHQ Nutrient Database. Available online: http://riskfactor.cancer.gov/DHQ/database/ (accessed on 5 May 2021).
- US Department of Agriculture, Agricultural Research Service. USDA National Nutrient Database for Standard Reference, Release 22. In Nutrient Data Laboratory Home Page [Internet]. 2009. [Google Scholar]
- Pennington, J.A.T. Bowes & Church’s Food Values of Portions Commonly Used; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005. [Google Scholar]
- Folch, J.; Lees, M.; Sloane Stanley, G.H. A Simple Method for the Isolation and Purification of Total Lipides from Animal Tissues. J Biol. Chem. 1957, 226, 497–509. [Google Scholar] [CrossRef]
- Buchanan, C.D.C.; Lust, C.A.C.; Burns, J.L.; Hillyer, L.M.; Martin, S.A.; Wittert, G.A.; Ma, D.W.L. Analysis of major fatty acids from matched plasma and serum samples reveals highly comparable absolute and relative levels. Protaglandins Leukot Essent Fat. Acids 2021, 168, 102268. [Google Scholar] [CrossRef] [PubMed]
- Rett, B.S.; Whelan, J. Increasing dietary linoleic acid does not increase tissue arachidonic acid content in adults consuming Western-type diets: A systematic review. Nutr. Metab. 2011, 8, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prien, A.; Grafe, A.; Rössler, R.; Junge, A.; Verhagen, E. Epidemiology of Head Injuries Focusing on Concussions in Team Contact Sports: A Systematic Review. Sports Med. 2018, 48, 953–969. [Google Scholar] [CrossRef]
- Demonty, I.; Langlois, K.; Greene-Finestone, L.S.; Zoka, R.; Nguyen, L. Proportions of long-chain omega-3 fatty acids in erythrocyte membranes of Canadian adults: Results from the Canadian Health Measures survey 2012–2015. Am. J. Clin. Nutr. 2021, 113, 993–1008. [Google Scholar] [CrossRef]
- Nelson, J.R.; Raskin, S. The eicosapentaenoic acid:arachidonic acid ratio and its clinical utility in cardiovascular disease. Postgrad Med. 2019, 131, 268–277. [Google Scholar] [CrossRef] [Green Version]
- Calder, P.C. Marine omega-3 fatty acids and inflammatory processes: Effects, mechanisms and clinical relevance. Biochim. Biophys. Acta 2015, 1851, 469–484. [Google Scholar] [CrossRef]
- Wu, A.; Ying, Z.; Gomez-Pinilla, F. Exercise facilitates the action of dietary DHA on functional recovery after brain trauma. Neuroscience 2013, 248, 655–663. [Google Scholar] [CrossRef] [Green Version]
- Desai, A.; Kevala, K.; Kim, H.Y. Depletion of brain docosahexaenoic acid impairs recovery from traumatic brain injury. PLoS ONE 2014, 9, e86472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.; Van, K.C.; Gavitt, B.J.; Grayson, J.K.; Lu, Y.; Lyeth, B.G.; Pichakron, K.O. Effect of fish oil supplementation in a rat model of multiple mild traumatic brain injuries. Restor. Neurol. Neurosci. 2013, 31, 647–659. [Google Scholar] [CrossRef]
- Pan, H.C.; Kao, T.K.; Ou, Y.C.; Yang, D.Y.; Yen, Y.J.; Wang, C.C.; Chuang, Y.H.; Liao, S.L.; Raung, S.L.; Wu, C.W.; et al. Protective effect of docosahexaenoic acid against brain injury in ischemic rats. J. Nutr. Biochem. 2009, 20, 715–725. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.; Ying, Z.H.E.; Gomez-Pinilla, F. Omega-3 Fatty Acids Supplementation Restores Mechanisms that Maintain Brain Homeostasis in Traumatic Brain Injury. J. Neurotrauma 2007, 24, 1587–1595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, A.; Ying, Z.; Gomez-Pinilla, F. The salutary effects of DHA dietary supplementation on cognition, neuroplasticity, and membrane homeostasis after brain trauma. J. Neurotrauma 2011, 28, 2113–2122. [Google Scholar] [CrossRef] [Green Version]
- Lewis, M.; Ghassemi, P.; Hibbeln, J. Therapeutic use of omega-3 fatty acids in severe head trauma. Am. J. Emerg. Med. 2013, 31, 273.e5–273.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, L.; Bailes, J.; Dedhia, H.; Zikos, A.; Singh, A.; McDowell, D.; Failinger, C.; Biundo, R.; Petrick, J.; Carpenter, J. Surviving a mine explosion. J. Am. Coll. Surg. 2008, 207, 276–283. [Google Scholar] [CrossRef]
- Oliver, J.M.; Jones, M.T.; Kirk, K.M.; Gable, D.A.; Repshas, J.T.; Johnson, T.A.; Andréasson, U.; Norgren, N.; Blennow, K.; Zetterberg, H. Effect of docosahexaenoic acid on a biomarker of head trauma in American Football. Med. Sci. Sports Exerc. 2016, 48, 974–982. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Male (n = 19) | Female (n = 15) | p-Value | |
|---|---|---|---|
| Age (y) | 24.84 ± 2.32 | 23.45 ± 3.10 | 0.147 |
| Height (cm) | 185.80 ± 3.59 | 170.14 ± 6.47 | <0.001 |
| Weight (kg) | 95.23 ± 6.93 | 71.21 ± 5.79 | <0.001 |
| BMI (kg/m2) | 27.57 ± 1.67 | 24.61 ± 1.66 | <0.001 |
| Male (n = 19) | Female (n = 15) | p-Value | |
|---|---|---|---|
| EPA | 0.71 ± 0.28 | 0.87 ± 0.76 | 0.681 |
| DHA | 3.77 ± 0.94 | 3.74 ± 1.69 | 0.537 |
| ALA | 0.26 ± 0.11 | 0.27 ± 0.15 | 1.00 |
| AA | 12.41 ± 1.40 | 11.40 ± 2.79 | 0.319 |
| O3I | 4.48 ± 1.12 | 4.61 ± 2.40 | 0.471 |
| Male (n = 19) | Female (n = 15) | Total | |
|---|---|---|---|
| With Supplementation | |||
| Low risk | 0 (0%) | 2 (18.2%) | 2 (8.7%) |
| Intermediate risk | 9 (75%) | 3 (27.3%) | 12 (52.2%) |
| High risk | 3 (25%) | 6 (54.5%) | 9 (39.1%) |
| Without Supplementation | |||
| Low risk | 0 (0%) | 0 (0%) | 0 (0%) |
| Intermediate risk | 5 (71.4%) | 1 (25%) | 6 (54.5%) |
| High risk | 2 (28.6%) | 3 (75%) | 5 (45.5%) |
| Without Supplementation | With Supplementation | |||
|---|---|---|---|---|
| Male (n = 7) | Female (n = 4) | Male (n = 12) | Female (n = 11) | |
| EPA (mg·day−1) | 0.05 ± 0.03 | 0.07 ± 0.07 | 1272 ± 536 | 1189 ± 451 |
| DHA (mg·day−1) | 0.11 ± 0.07 | 0.16 ± 0.14 | 636 ± 268 | 595 ± 226 |
| ALA (mg·day−1) | 0.78 ± 0.78 | 0.11 ± 0.07 | 0.78 ± 0.78 | 0.11 ± 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Armstrong, A.; Anzalone, A.J.; Pethick, W.; Murray, H.; Dahlquist, D.T.; Askow, A.T.; Heileson, J.L.; Hillyer, L.M.; Ma, D.W.L.; Oliver, J.M. An Evaluation of Omega-3 Status and Intake in Canadian Elite Rugby 7s Players. Nutrients 2021, 13, 3777. https://doi.org/10.3390/nu13113777
Armstrong A, Anzalone AJ, Pethick W, Murray H, Dahlquist DT, Askow AT, Heileson JL, Hillyer LM, Ma DWL, Oliver JM. An Evaluation of Omega-3 Status and Intake in Canadian Elite Rugby 7s Players. Nutrients. 2021; 13(11):3777. https://doi.org/10.3390/nu13113777
Chicago/Turabian StyleArmstrong, Ashley, Anthony J. Anzalone, Wendy Pethick, Holly Murray, Dylan T. Dahlquist, Andrew T. Askow, Jeffery L. Heileson, Lyn M. Hillyer, David W. L. Ma, and Jonathan M. Oliver. 2021. "An Evaluation of Omega-3 Status and Intake in Canadian Elite Rugby 7s Players" Nutrients 13, no. 11: 3777. https://doi.org/10.3390/nu13113777
APA StyleArmstrong, A., Anzalone, A. J., Pethick, W., Murray, H., Dahlquist, D. T., Askow, A. T., Heileson, J. L., Hillyer, L. M., Ma, D. W. L., & Oliver, J. M. (2021). An Evaluation of Omega-3 Status and Intake in Canadian Elite Rugby 7s Players. Nutrients, 13(11), 3777. https://doi.org/10.3390/nu13113777