
Oral Nutritional Supplementation Improves Growth in Children at Malnutrition Risk and with Picky Eating Behaviors

 , , ,
, , ,
Abstract
:1. Introduction
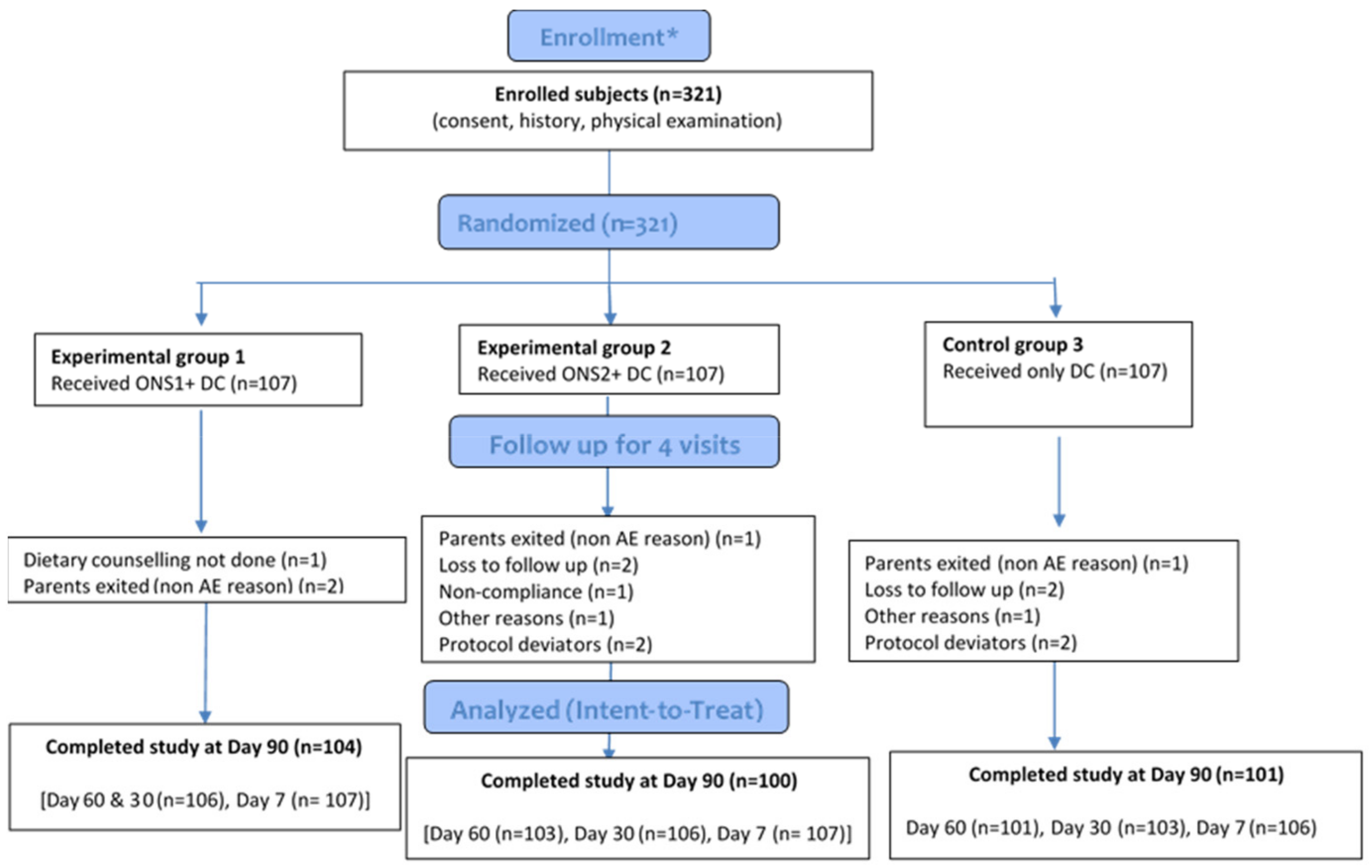
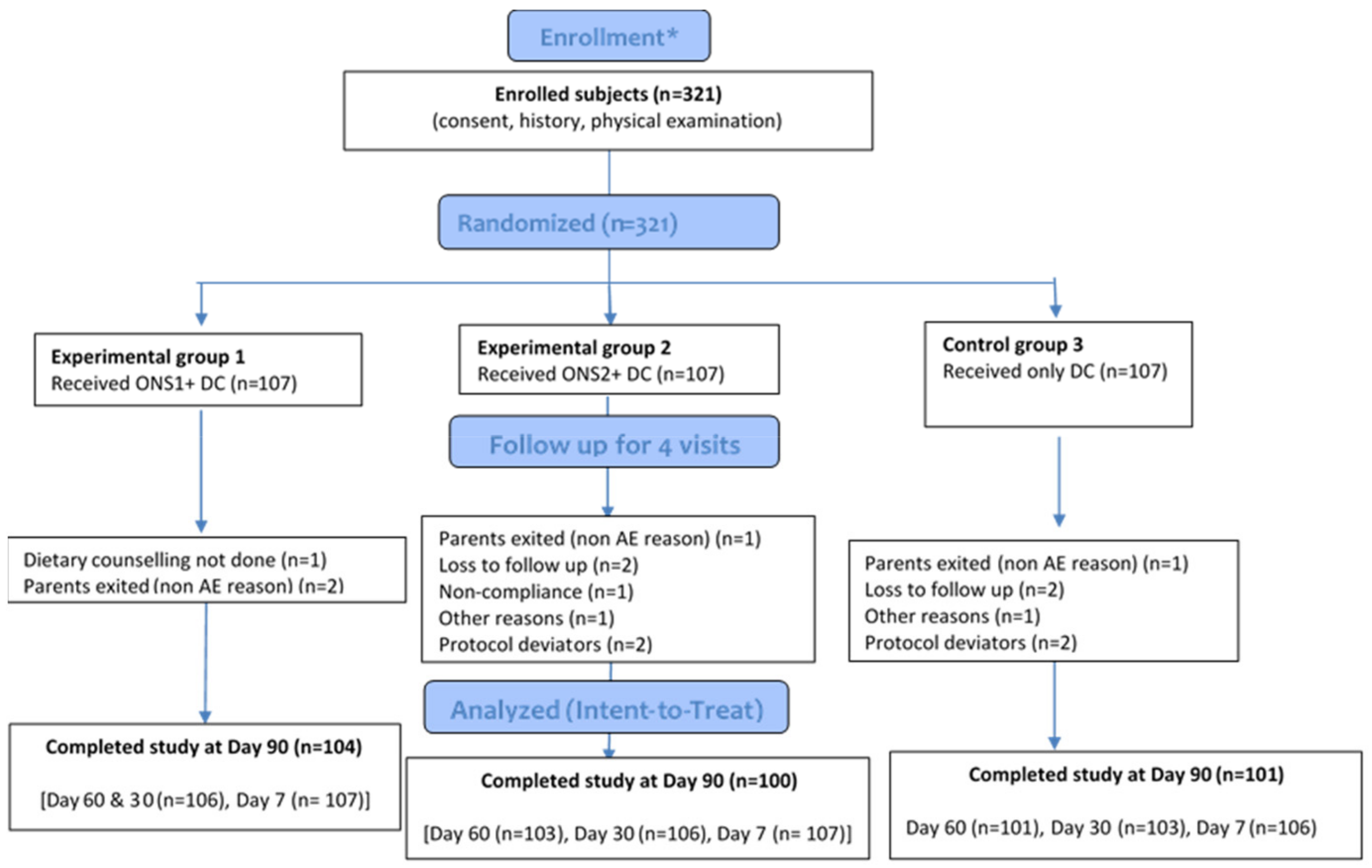
2. Materials and Methods
3. Results
3.1. Baseline Socio-Demographic and Anthropometric Characteristics
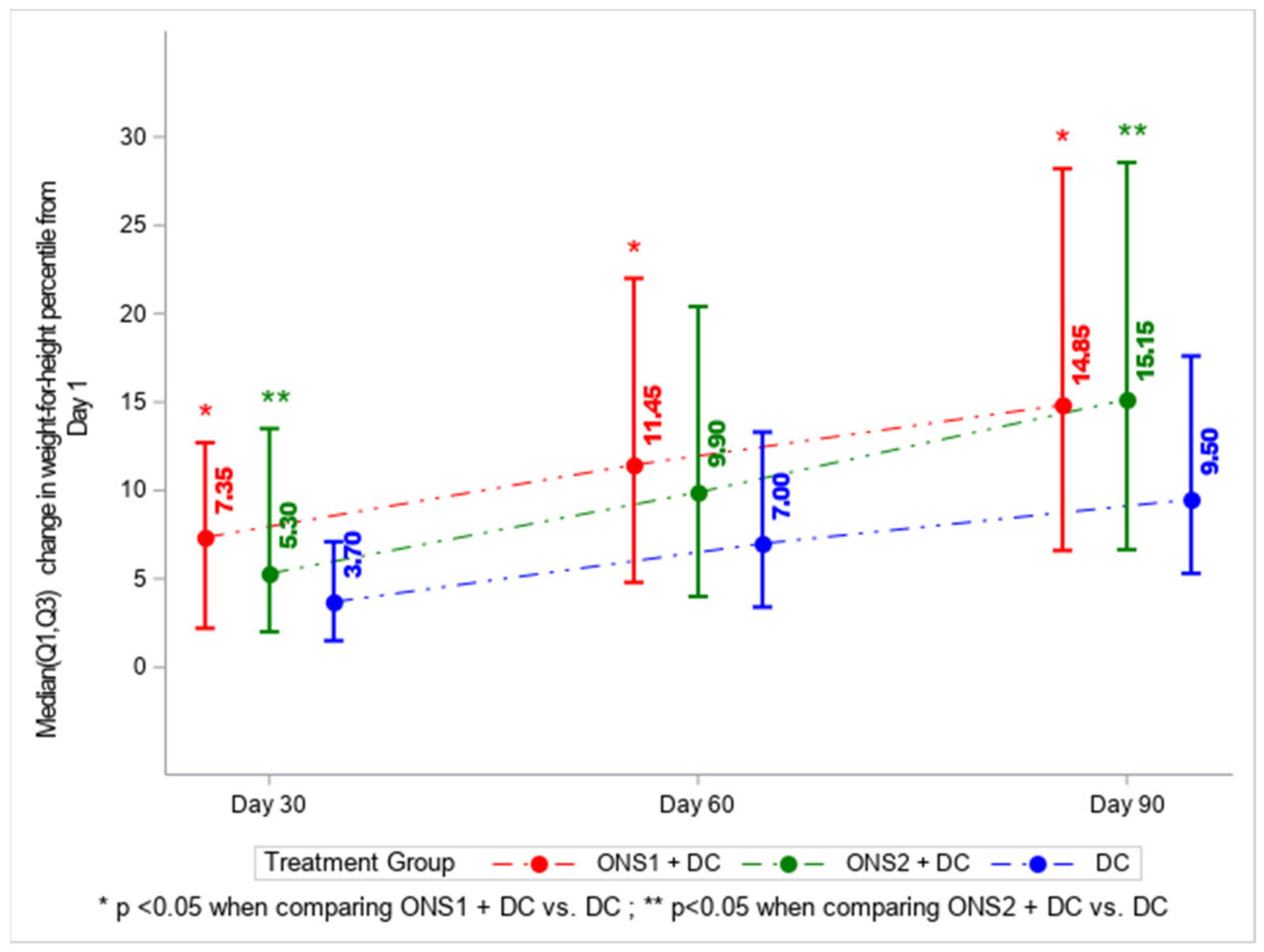
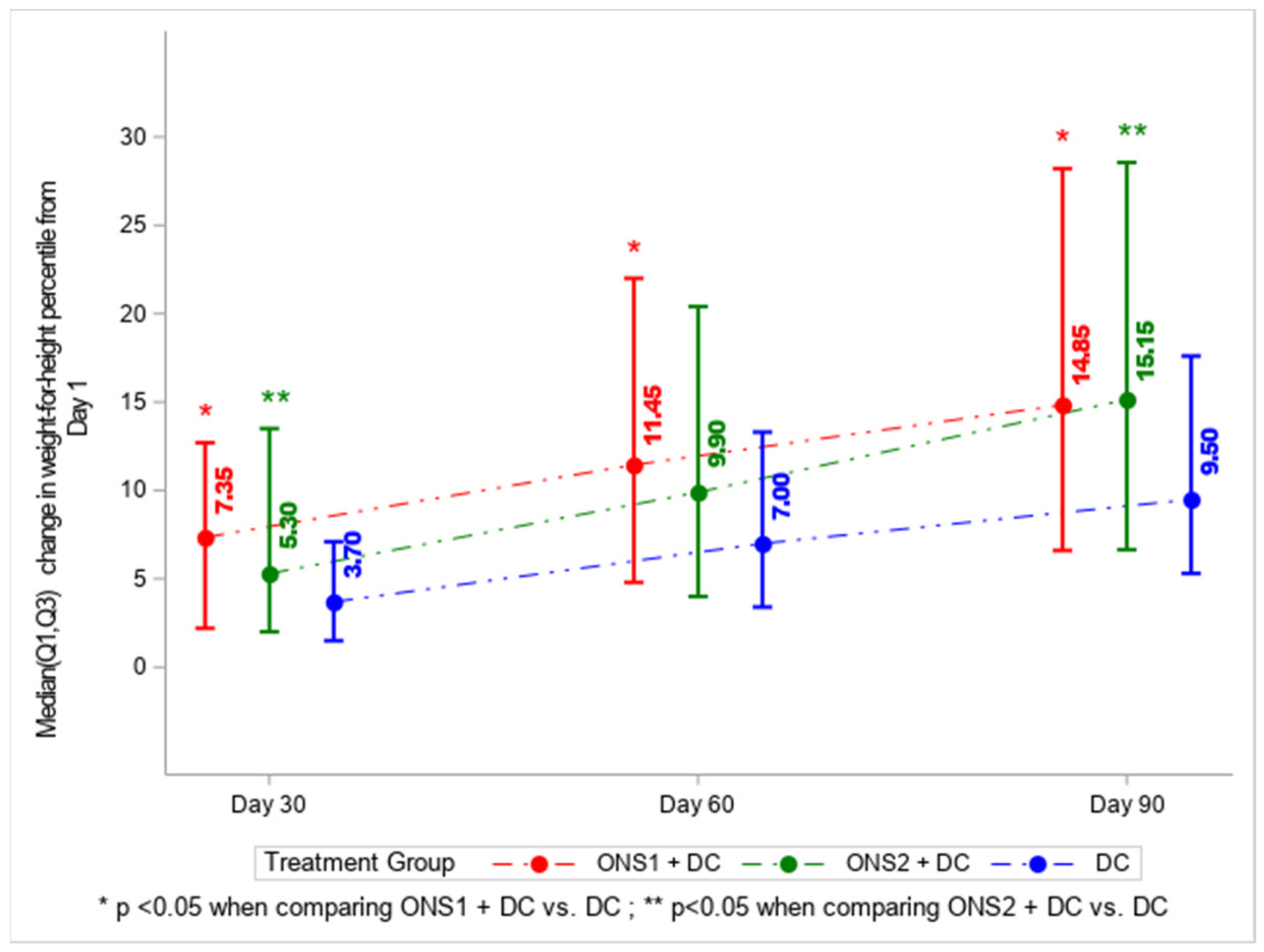
3.2. Primary Outcome: Change in Weight-for-Height Percentile
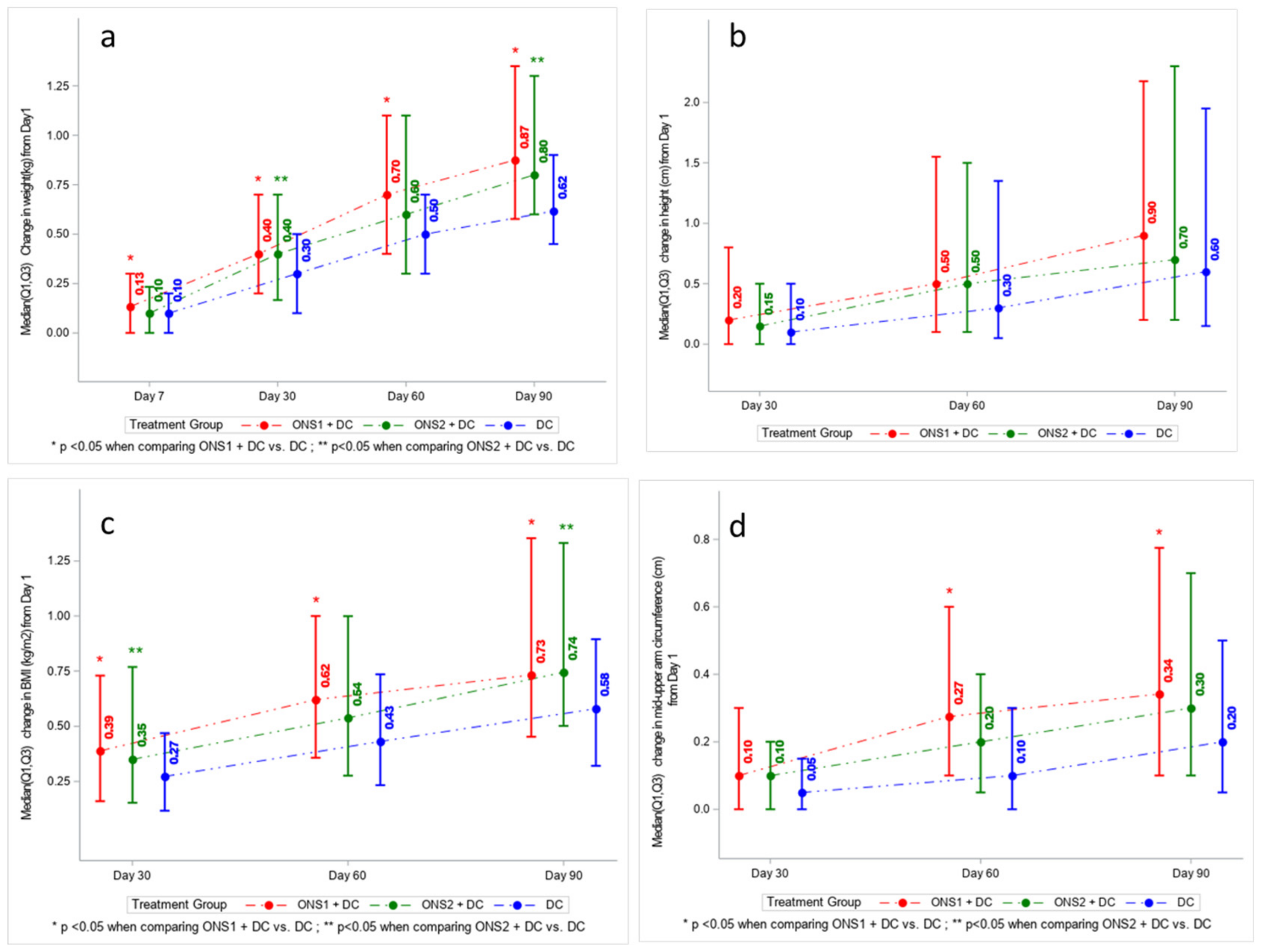
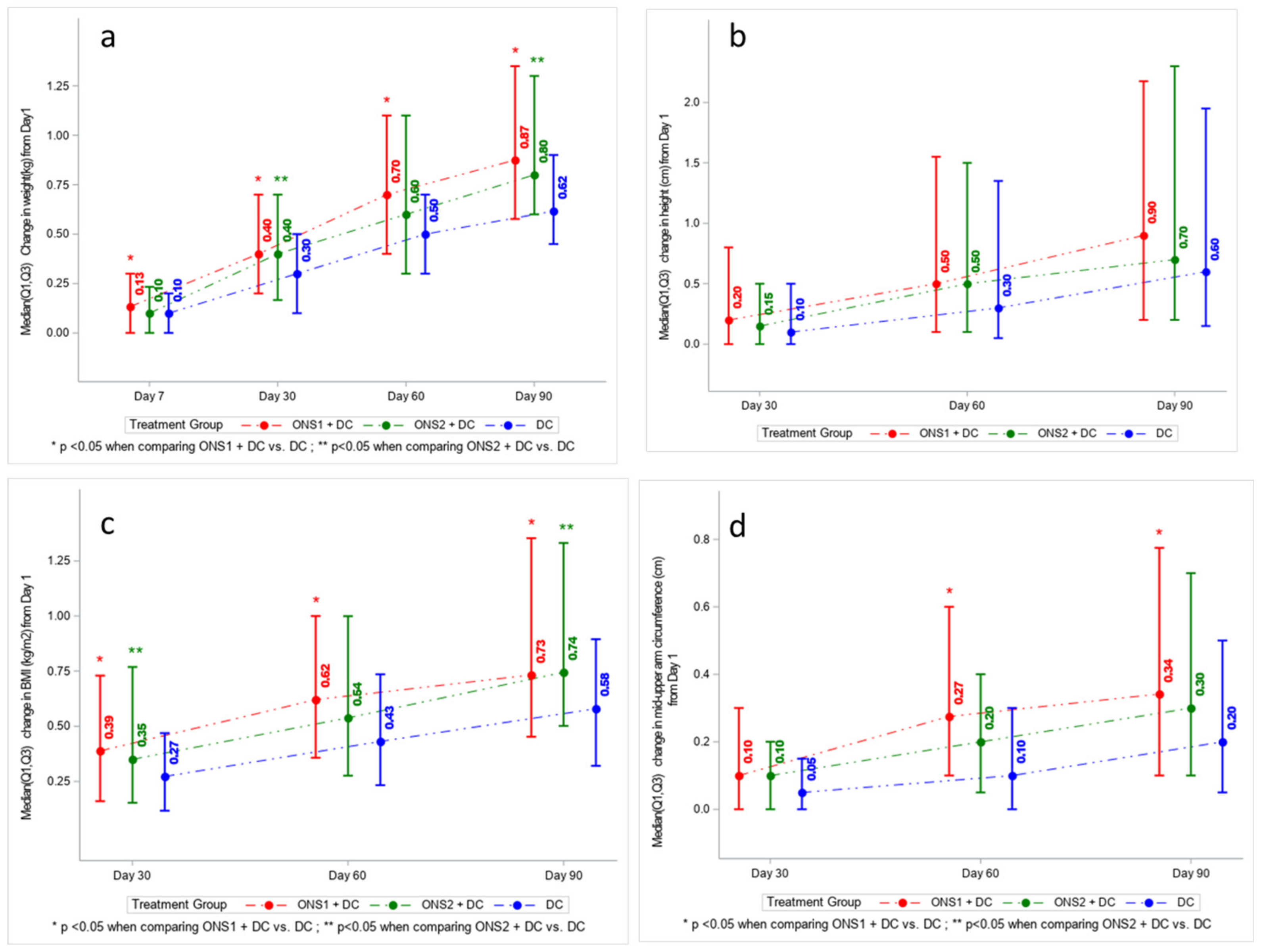
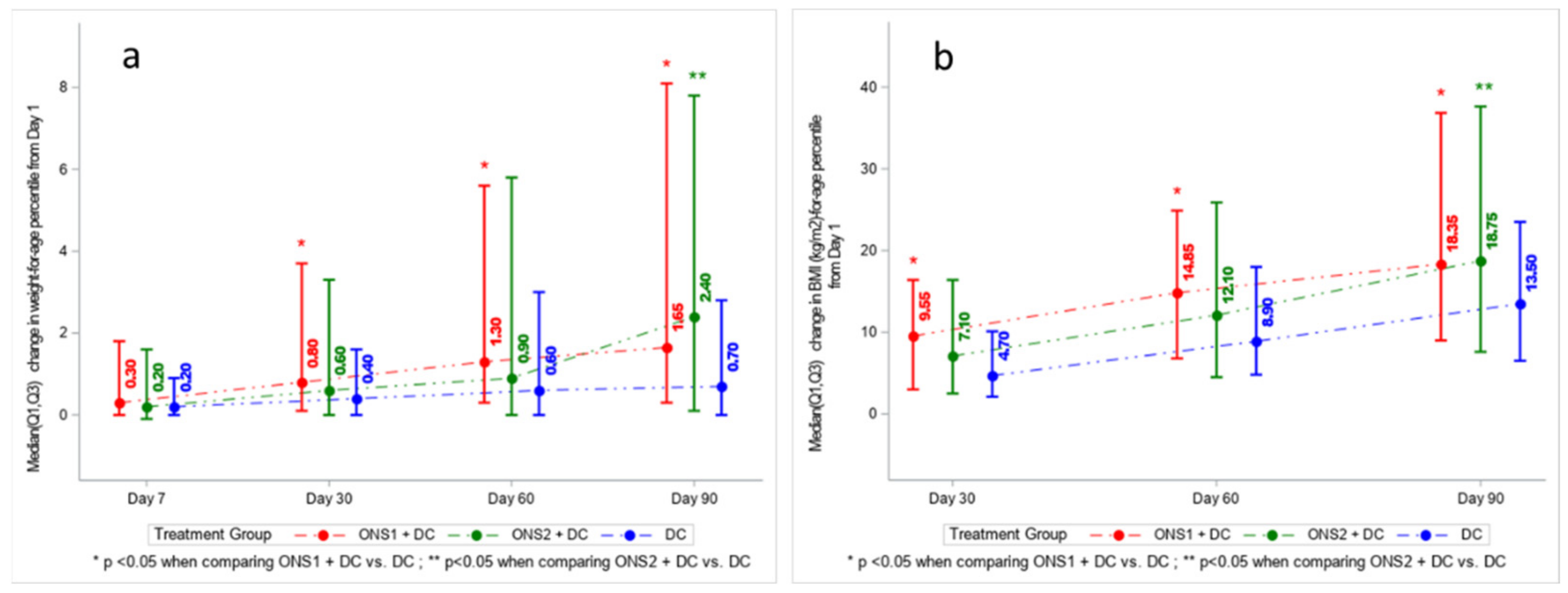
3.3. Absolute Change in Weight, Height, BMI, and MUAC across Time Points
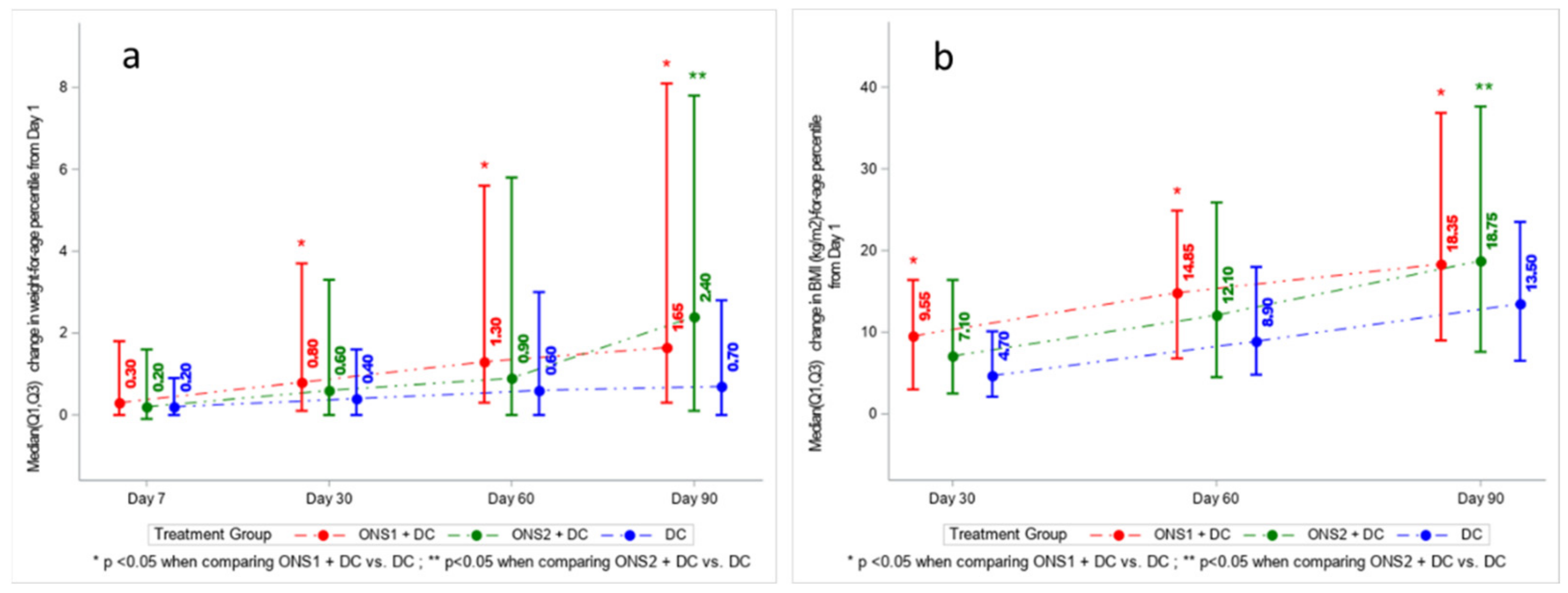
3.4. Changes in Growth Indicators (as Percentiles and Z-Scores) across Time Points
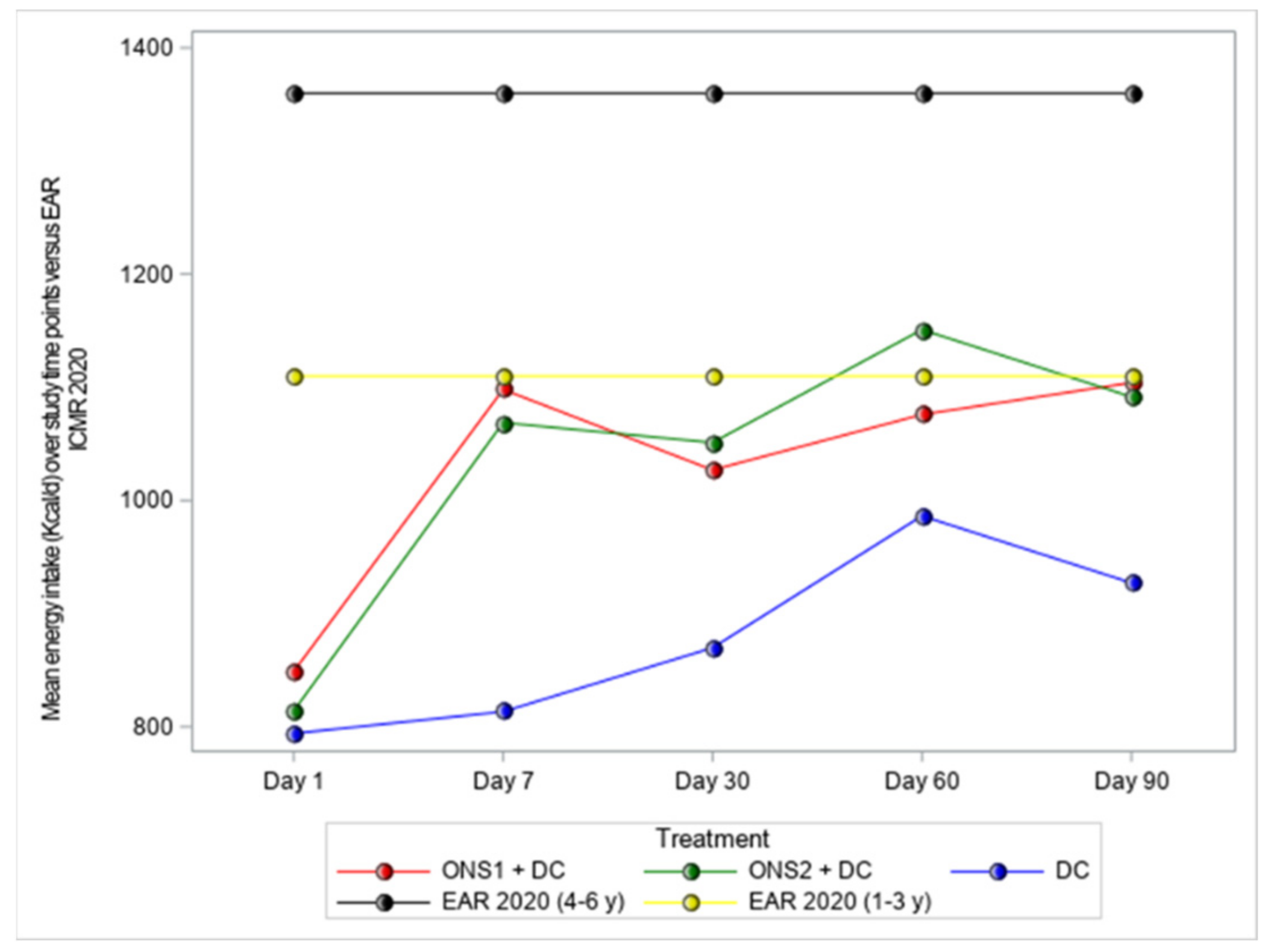
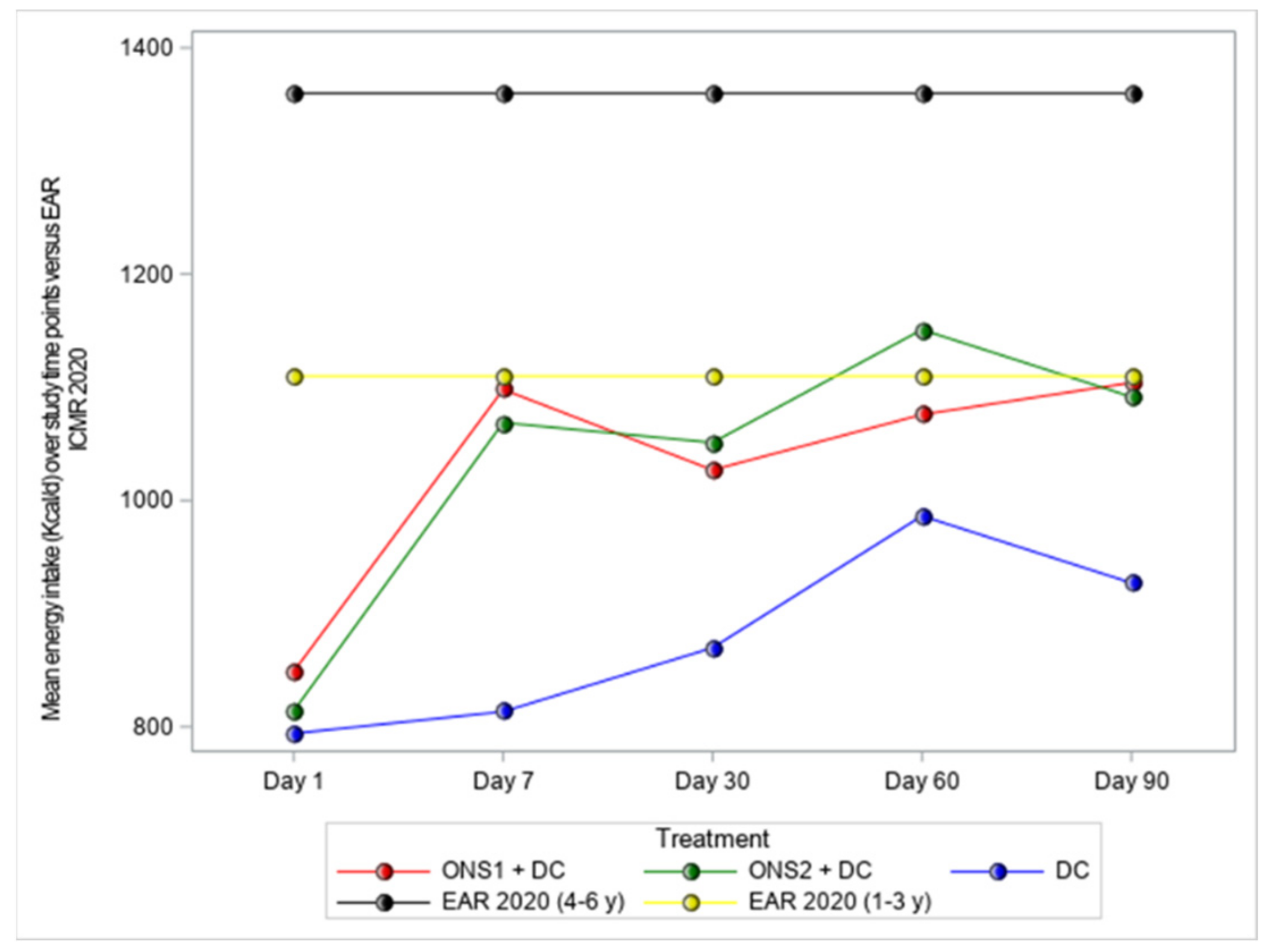
3.5. Dietary Parameters
3.6. Adverse Events
4. Discussion
- Children at risk of malnutrition (Z-score between −2 and −1) are at increased risk of impaired growth and other morbidities; when these children also have picky eating behaviors, they are at even greater risk for poor growth and health outcomes. For such children, it is important for healthcare providers to offer timely and effective interventions aimed at stopping further growth faltering and promoting catch-up growth.
- Daily ONS consumption, along with dietary counseling (DC) on healthier eating behaviors, can be used to help ensure adequate growth and to lessen risk for morbidities. In this study of catch-up growth, we examined the impact of two ONS formulas—one milk-based (ONS-1) and the other lactose-free (ONS-2)—used over a 90-day interval along with DC.
- Findings showed significant increases in weight-for-height percentile for ONS1 + DC and for ONS2 + DC interventions, as compared to DC only. Anthropometric measurements (weight and body mass index) also increased significantly over time for the two ONS groups.
- Growth parameters were comparable for both groups receiving ONS, suggesting the effects of these ONS formulas are similarly beneficial in promoting growth.
- ONS groups trended toward greater height gain but not full catch-up to WHO growth standards. Previous studies have shown that height improvement was only observed with intervention of longer duration (>6 months
- Findings in this study are consistent with previous studies in which ONS, along with dietary counseling, were more effective than dietary counseling alone in promoting catch-up growth in at-risk children.
4.1. Other Studies on Picky Eating Behaviors and Growth/Health Impairment in Young Children
4.2. Strengths and Limitations of This Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. The WHO Child Growth Standards. Available online: https://www.who.int/childgrowth/standards/en/ (accessed on 21 December 2020).
- De Onis, M.; Branca, F. Childhood stunting: A global perspective. Matern. Child Nutr. 2016, 12 (Suppl. S1), 12–26. [Google Scholar] [CrossRef]
- Mwangome, M.; Prentice, A.M. Tackling the triple threats of childhood malnutrition. BMC Med. 2019, 17, 210. [Google Scholar] [CrossRef] [PubMed]
- UNICEF-WHO-World Bank. Levels and Trends in Child Malnutrition: Key Findings of the 2019 Edition of the Joint Child Malnutrition Estimates; United Nations Children’s Fund (UNICEF): New York, NY, USA; World Health Organization: Geneva, Switzerland; International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2019. [Google Scholar]
- International Institute for Population Sciences (IIPS) and ICF. National Family Health Survey (NFHS-4), 2015–2016; International Institute for Population Sciences (IIPS): Mumbai, India, 2017; Available online: http://rchiips.org/NFHS/NFHS-4Reports/India.pdf (accessed on 12 October 2021).
- Murarkar, S.; Gothankar, J.; Doke, P.; Pore, P.; Lalwani, S.; Dhumale, G.; Quraishi, S.; Patil, R.; Waghachavare, V.; Dhobale, R.; et al. Prevalence and determinants of undernutrition among under-five children residing in urban slums and rural area, Maharashtra, India: A community-based cross-sectional study. BMC Public Health 2020, 20, 1559. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, O.; Kim, R.; Sarwal, R.; James, K.; Subramanian, S. Trends in underweight, stunting, and wasting prevalence and inequality among children under three in Indian states, 1993–2016. Sci. Rep. 2021, 11, 1413. [Google Scholar] [CrossRef] [PubMed]
- Independent Evaluation Group (IEG). What Can We Learn from Nutrition Impact Evaluations? Lessons from a Review of Interventions to Reduce Childhood Malnutrition in Developing Countries; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2010. [Google Scholar]
- United Nations Children’s Fund (UNICEF). Progress for Children: A Report Card on Nutrition. Available online: https://www.unicef.org/progressforchildren/2006n4/index_undernutrition.html (accessed on 14 November 2020).
- World Health Organization (WHO). The Z-Score or Standard Deviation Classification System. Available online: https://www.who.int/nutgrowthdb/about/introduction/en/index4.html (accessed on 23 April 2021).
- Mehta, N.M.; Corkins, M.R.; Lyman, B.; Malone, A.; Goday, P.S.; Carney, L.N.; Monczka, J.L.; Plogsted, S.W.; Schwenk, W.F. American Society for Parenteral Enteral Nutrition Board of Directors. Defining pediatric malnutrition: A paradigm shift toward etiology-related definitions. J. Parenter. Enter. Nutr. 2013, 37, 460–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations Children’s Fund (UNICEF). The State of the World’s Children 2019. Children, Food and Nutrition: Growing Well in a Changing World. Available online: https://www.unicef.org/reports/state-of-worlds-children-2019 (accessed on 21 March 2021).
- Taylor, C.M.; Emmett, P.M. Picky eating in children: Causes and consequences. Proc. Nutr. Soc. 2019, 78, 161–169. [Google Scholar] [CrossRef] [Green Version]
- Volger, S.; Sheng, X.; Tong, L.M.; Zhao, D.; Fan, T.; Zhang, F.; Ge, J.; Ho, W.M.; Hays, N.P.; Yao, M.P. Nutrient intake and dietary patterns in children 2.5–5 years of age with picky eating behaviours and low weight-for-height. Asia Pac. J. Clin. Nutr. 2017, 26, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Dubois, L.; Farmer, A.; Girard, M.; Peterson, K.; Tatone-Tokuda, F. Problem eating behaviors related to social factors and body weight in preschool children: A longitudinal study. Int. J. Behav. Nutr. Phys. Act. 2007, 4, 9. [Google Scholar] [CrossRef] [Green Version]
- Xue, Y.; Lee, E.; Ning, K.; Zheng, Y.; Ma, D.; Gao, H.; Yang, B.; Bai, Y.; Wang, P.; Zhang, Y. Prevalence of picky eating behaviour in Chinese school-age children and associations with anthropometric parameters and intelligence quotient. A cross-sectional study. Appetite 2015, 91, 248–255. [Google Scholar] [CrossRef] [Green Version]
- Antoniou, E.E.; Roefs, A.; Kremers, S.P.; Jansen, A.; Gubbels, J.S.; Sleddens, E.F.; Thijs, C. Picky eating and child weight status development: A longitudinal study. J. Hum. Nutr. Diet. 2016, 29, 298–307. [Google Scholar] [CrossRef]
- Ibrahim, M.K.; Zambruni, M.; Melby, C.L.; Melby, P.C. Impact of childhood malnutrition on host defense and infection. Clin. Microbiol. Rev. 2017, 30, 919–971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouma, S. Diagnosing pediatric malnutrition. Nutr. Clin. Pract. 2017, 32, 52–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olofin, I.; McDonald, C.M.; Ezzati, M.; Flaxman, S.; Black, R.E.; Fawzi, W.W.; Caulfield, L.E.; Danaei, G. Nutrition Impact Model Study. Associations of suboptimal growth with all-cause and cause-specific mortality in children under five years: A pooled analysis of ten prospective studies. PLoS ONE 2013, 8, e64636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, R.; Kerr, K.; Brunton, C.; Williams, J.; DeWitt, T.; Wulf, K. A first step towards eliminating malnutrition: A proposal for universal nutrition screening in pediatric practice. Nutr. Diet. Suppl. 2021, 13, 17–24. [Google Scholar] [CrossRef]
- Shim, J.O.; Kim, S.; Choe, B.H.; Seo, J.H.; Yang, H.R. Effect of nutritional supplement formula on catch-up growth in young children with nonorganic faltering growth: A prospective multicenter study. Nutr. Res. Pract. 2020, 14, 230–241. [Google Scholar] [CrossRef]
- Indian Council of Medical Research. ICMR-NIN Expert Group on Nutrient Requirement for Indians, Recommended Dietary Allowances (RDA) and Estimated Average Requirements (EAR)—2020; ICMR-National Institute of Nutrition: Telangana, India, 2020. [Google Scholar]
- Mayneris-Perxachs, J.; Swann, J.R. Metabolic phenotyping of malnutrition during the first 1000 days of life. Eur. J. Nutr. 2019, 58, 909–930. [Google Scholar] [CrossRef] [Green Version]
- Roberts, J.L.; Stein, A.D. The impact of nutritional interventions beyond the first 2 years of life on linear growth: A systematic review and meta-analysis. Adv. Nutr. 2017, 8, 323–336. [Google Scholar] [CrossRef] [Green Version]
- Carruth, B.R.; Skinner, J.; Houck, K.; Moran, J., 3rd; Coletta, F.; Ott, D. The phenomenon of ‘‘picky eater’’: A behavioral marker in eating patterns of toddlers. J. Am. Coll. Nutr. 1998, 17, 180–186. [Google Scholar] [CrossRef]
- Jacobi, C.; Schmitz, G.; Agras, W.S. Is picky eating an eating disorder? Int. J. Eat. Disord. 2008, 41, 626–634. [Google Scholar] [CrossRef]
- Brown, C.L.; Vander Schaaf, E.B.; Cohen, G.M.; Irby, M.B.; Skelton, J.A. Association of picky eating and food neophobia with weight: A systematic review. Child. Obes. 2016, 12, 247–262. [Google Scholar] [CrossRef] [Green Version]
- Mascola, A.J.; Bryson, S.W.; Agras, W.S. Picky eating during childhood: A longitudinal study to age 11 years. Eat. Behav. 2010, 11, 253–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, A.K.; Marchand, V.; Sauve, R.S.; Canadian Paediatric Society Nutrition; Gastroenterology Committee. The ‘picky eater’: The toddler or preschooler who does not eat. Paediatr. Child Health 2012, 17, 455–460. [Google Scholar] [CrossRef]
- Taylor, C.M.; Steer, C.D.; Hays, N.P.; Emmett, P.M. Growth and body composition in children who are picky eaters: A longitudinal view. Eur. J. Clin. Nutr. 2019, 73, 869–878. [Google Scholar] [CrossRef] [PubMed]
- Scharf, R.J.; Rogawski, E.T.; Murray-Kolb, L.E.; Maphula, A.; Svensen, E.; Tofail, F.; Rasheed, M.; Abreu, C.; Vasquez, A.O.; Shrestha, R.; et al. Early childhood growth and cognitive outcomes: Findings from the MAL-ED study. Matern. Child Nutr. 2018, 14, e12584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poh, B.K.; Rojroonwasinkul, N.; Le Nyugen, B.K.; Budiman, B.; Ng, L.O.; Soonthorndhada, K.; Xuyen, H.T.; Deurenberg, P.; Parikh, P. Relationship between anthropometric indicators and cognitive performance in Southeast Asian school-aged children. Br. J. Nutr. 2013, 110 (Suppl. S3), S57–S64. [Google Scholar] [CrossRef]
- Nassar, M.F.; Shaaban, S.Y.; Nassar, J.F.; Younis, N.T.; Abdel-Mobdy, A.E. Language skills and intelligence quotient of protein energy malnutrition survivors. J. Trop. Pediatr. 2012, 58, 226–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perignon, M.; Fiorentino, M.; Kuong, K.; Burja, K.; Parker, M.; Sisokhom, S.; Chamnan, C.; Berger, J.; Wieringa, F.T. Stunting, poor iron status and parasite infection are significant risk factors for lower cognitive performance in Cambodian school-aged children. PLoS ONE 2014, 9, e112605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sudfeld, C.R.; McCoy, D.C.; Fink, G.; Muhihi, A.; Bellinger, D.C.; Masanja, H.; Smith, E.R.; Danaei, G.; Ezzati, M.; Fawzi, W.W. Malnutrition and its determinants are associated with suboptimal cognitive, communication, and motor development in Tanzanian children. J. Nutr. 2015, 145, 2705–2714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Victora, C.G.; Adair, L.; Fall, C.; Hallal, P.C.; Martorell, R.; Richter, L.; Sachdev, H.S.; Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: Consequences for adult health and human capital. Lancet 2008, 371, 340–357. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, L.; Cervantes, E.; Ortiz, R. Malnutrition and gastrointestinal and respiratory infections in children: A public health problem. Int. J. Environ. Res. Public Health 2011, 8, 1174–1205. [Google Scholar] [CrossRef] [Green Version]
- Gwela, A.; Mupere, E.; Berkley, J.A.; Lancioni, C. Undernutrition, host immunity and vulnerability to infection among young children. Pediatr. Infect. Dis. J. 2019, 38, e175–e177. [Google Scholar] [CrossRef]
- Gambra-Arzoz, M.; Alonso-Cadenas, J.A.; Jimenez-Legido, M.; Lopez-Gimenez, M.R.; Martin-Rivada, A.; de Los Angeles Martinez-Ibeas, M.; Canedo-Villarroya, E.; Pedron-Giner, C. Nutrition risk in hospitalized pediatric patients: Higher complication rate and higher costs related to malnutrition. Nutr. Clin. Pract. 2020, 35, 157–163. [Google Scholar] [CrossRef] [Green Version]
- Pesch, M.H.; Bauer, K.W.; Christoph, M.J.; Larson, N.; Neumark-Sztainer, D. Young adult nutrition and weight correlates of picky eating during childhood. Public Health Nutr. 2020, 23, 987–995. [Google Scholar] [CrossRef] [PubMed]
- Gat-Yablonski, G.; Phillip, M. Nutritionally-induced catch-up growth. Nutrients 2015, 7, 517–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alarcon, P.A.; Lin, L.H.; Noche, M., Jr.; Hernandez, V.C.; Cimafranca, L.; Lam, W.; Comer, G.M. Effect of oral supplementation on catch-up growth in picky eaters. Clin. Pediatr. 2003, 42, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, A.K.; Kishore, B.; Shaikh, I.; Satyavrat, V.; Kumar, A.; Shah, T.; Pote, P.; Shinde, S.; Berde, Y.; Low, Y.L.; et al. Effect of oral nutritional supplementation on growth and recurrent upper respiratory tract infections in picky eating children at nutritional risk: A randomized, controlled trial. J. Int. Med. Res. 2018, 48, 2186–2201. [Google Scholar] [CrossRef] [PubMed]
- Dempster, R.; Burdo-Hartman, W.; Halpin, E.; Williams, C. Estimated cost-effectiveness of intensive interdisciplinary behavioral treatment for increasing oral intake in children with feeding difficulties. J. Pediatr. Psychol. 2016, 41, 857–866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakdawalla, D.N.; Mascarenhas, M.; Jena, A.B.; Vanderpuye-Orgle, J.; LaVallee, C.; Linthicum, M.T.; Snider, J.T. Impact of oral nutrition supplements on hospital outcomes in pediatric patients. JPEN J. Parenter. Enter. Nutr. 2014, 38, 42S–49S. [Google Scholar] [CrossRef]
- Mehndiratta, C.; Bhasin, J.; Khadilkar, V.; Kochar, I.; Pai, U.; Mittal, G.; Sanskar, P.; Agrawal, T. Effectiveness of nutritional supplement in growth and development of children aged 2–12 years. Matern. Pediatr. Nutr. 2021, 4, nr126. [Google Scholar]
- Phillips, C.A.; Bailer, J.; Foster, E.; Li, Y.; Dogan, P.; Smith, E.; Reilly, A.; Freedman, J. Evaluation of an automated pediatric malnutrition screen using anthropometric measurements in the electronic health record: A quality improvement initiative. Supportive Care Cancer 2020, 28, 1659–1666. [Google Scholar] [CrossRef]
- Vijayananthan, A.; Nawawi, O. The importance of Good Clinical Practice guidelines and its role in clinical trials. Biomed. Imaging Interv. J. 2008, 4, e5. [Google Scholar] [CrossRef] [PubMed]
- Abbott Nutrition. Oral Nutritional Supplementation in Picky Eating Children: NCT02523027 14/8/2015. Available online: https://clinicaltrials.gov/ct2/show/NCT02523027?term=oral+nutritional+supplementation&cntry=IN&draw=2&rank=2 (accessed on 6 March 2021).
- Abbott Nutrition International India. A Study of an Oral Nutritional Supplementation in Picky Eating Children: CTRI/2015/10/006330, 29/10/2015. Available online: http://ctri.nic.in/Clinicaltrials/pdf_generate.php?trialid=12708&EncHid=&modid=&compid=%27,%2712708det%27 (accessed on 6 March 2021).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total N = 321 | ONS1 + DC N = 107 | ONS2 + DC N = 107 | DC Only N = 107 | p-Value | ||
|---|---|---|---|---|---|---|---|
| ONS1 + DC vs. DC Only | ONS2 + DC vs. DC Only | ONS1 + DC vs. ONS2 + DC | |||||
| Age (years) # | 2.93 (2.47, 3.35) | 2.94 (2.46, 3.38) | 3.01 (2.47, 3.35) | 2.92 (2.47, 3.37) | 1.00 | 1.00 | 1.00 |
| Male, n (%) | 193 (60.1) | 70 (65.4) | 63 (58.9) | 60 (56.1) | 0.50 | 0.68 | 0.65 |
| Female, n (%) | 128 (39.9) | 37 (34.6) | 44 (41.1) | 47 (43.9) | |||
| Weight (kg) * | 11.11 (1.55) | 11.18 (1.51)) | 11.12 (1.58) | 11.04 (1.57) | 1.00 | 1.00 | 1.00 |
| Height (cm) * | 88.78 (7.09) | 88.89 (6.97) | 89.08 (7.19) | 88.38 (7.15) | 1.00 | 0.93 | 1.00 |
| BMI (kg/m2) * | 14.06 (0.58) | 14.11(0.48) | 13.98 (0.57) | 14.10 (0.67) | 0.98 | 0.05 | 0.09 |
| MUAC (cm) * | 14.08 (1.41) | 14.11 (1.47) | 14.00 (1.39) | 14.11 (1.37) | 0.84 | 0.78 | 0.84 |
| Z-scores | |||||||
| Weight-for-age * | −1.94 (0.98) | −1.92 (0.94) | −1.94 (1.01) | −1.97 (1.01) | 1.00 | 1.00 | 1.00 |
| Weight-for-height * | −1.46 (0.34) | −1.43 (0.28) | −1.52 (0.31) | −1.44 (0.42) | 0.94 | 0.08 | 0.04 |
| BMI-for-age * | −1.27 (0.45) | −1.24 (0.38) | −1.34 (0.45) | −1.24 (0.51) | 0.99 | 0.05 | 0.06 |
| Height-for-age * | −1.66 (1.65) | −1.67 (1.57) | −1.58 (1.71) | −1.74 (1.67) | 1.00 | 0.88 | 1.00 |
| MUAC-for-age * | −1.37 (1.26) | −1.36 (1.34) | −1.43 (1.25) | −1.33 (1.20) | 1.00 | 0.90 | 1.00 |
| Percentiles | |||||||
| Weight-for-age # | 2.60 (0.60, 9.30) | 2.80 (0.50, 9.00) | 2.40 (0.60, 8.60) | 2.30 (0.50, 10.60) | 1.00 | 1.00 | 1.00 |
| Weight-for-height # | 7.00 (4.40, 10.80) | 7.20 (4.80, 11.80) | 6.70 (3.90, 9.80) | 7.40 (4.50, 11.30) | 0.51 | 0.40 | 0.22 |
| BMI-for-age # | 9.60 (5.60, 15.00) | 10.20 (5.90, 15.70) | 8.20 (4.90, 14.30) | 9.90 (5.90, 16.80) | 0.86 | 0.30 | 0.27 |
| Height-for-age # | 4.90 (0.40, 29.10) | 5.20 (0.30, 23.40) | 5.60 (0.50, 29.20) | 4.10 (0.30, 32.20) | 1.00 | 1.00 | 1.00 |
| MUAC-for-age # | 9.00 (3.50, 26.60) | 9.90 (4.50, 25.70) | 8.40 (2.90, 28.70) | 8.30 (2.70, 26.80) | 1.00 | 1.00 | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khanna, D.; Yalawar, M.; Saibaba, P.V.; Bhatnagar, S.; Ghosh, A.; Jog, P.; Khadilkar, A.V.; Kishore, B.; Paruchuri, A.K.; Pote, P.D.; et al. Oral Nutritional Supplementation Improves Growth in Children at Malnutrition Risk and with Picky Eating Behaviors. Nutrients 2021, 13, 3590. https://doi.org/10.3390/nu13103590
Khanna D, Yalawar M, Saibaba PV, Bhatnagar S, Ghosh A, Jog P, Khadilkar AV, Kishore B, Paruchuri AK, Pote PD, et al. Oral Nutritional Supplementation Improves Growth in Children at Malnutrition Risk and with Picky Eating Behaviors. Nutrients. 2021; 13(10):3590. https://doi.org/10.3390/nu13103590
Chicago/Turabian StyleKhanna, Deepti, Menaka Yalawar, Pinupa Venkata Saibaba, Shirish Bhatnagar, Apurba Ghosh, Pramod Jog, Anuradha Vaman Khadilkar, Bala Kishore, Anil Kumar Paruchuri, Prahalad D. Pote, and et al. 2021. "Oral Nutritional Supplementation Improves Growth in Children at Malnutrition Risk and with Picky Eating Behaviors" Nutrients 13, no. 10: 3590. https://doi.org/10.3390/nu13103590
APA StyleKhanna, D., Yalawar, M., Saibaba, P. V., Bhatnagar, S., Ghosh, A., Jog, P., Khadilkar, A. V., Kishore, B., Paruchuri, A. K., Pote, P. D., Mandyam, R. D., Shinde, S., Shah, A., & Huynh, D. T. T. (2021). Oral Nutritional Supplementation Improves Growth in Children at Malnutrition Risk and with Picky Eating Behaviors. Nutrients, 13(10), 3590. https://doi.org/10.3390/nu13103590