
Are Food Additives a Really Problematic Hidden Source of Potassium for Chronic Kidney Disease Patients?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Analysis of Current European Food Additives Legislation
- (1)
- What food additives contain potassium in their chemical formulation.
- (2)
- In which food categories are each of them allowed.
- (3)
- The maximum level of each additive allowed according to food categories.
2.2. Potassium Content in Potassium-Additives
2.3. Label Analysis
2.4. Statistical Analysis
3. Results
3.1. Authorized Additives with Potassium
3.2. Food Categories and Maximum Level Authorized
3.3. Potassium Additives in Food
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Food Category | Specifications | Maximum Level (mg/L or mg/Kg) |
|---|---|---|
| Dairy products | Unflavoured sterilized and UHT milk | 1000 |
| Flavoured fermented milk products including heat-treated products | 3000 | |
| Partly dehydrated milk with less than 28% solids | 1000 | |
| Partly dehydrated milk with more than 28% solids | 1500 | |
| Dried milk and dried skimmed milk | 2500 | |
| sterilized, pasteurized, UHT cream and whipped cream | 5000 | |
| Unripened cheese except mozzarella | 2000 | |
| Processed cheese | 20,000 | |
| Unripened cheese products | 2000 | |
| Whipped cream analogues | 5000 | |
| Processed cheese analogues | 20,000 | |
| Beverage whiteners | 30,000 | |
| Fat and oil emulsions | Soured cream butter | 2000 |
| Spreadable fats | 5000 | |
| Ice-cream | 1000 | |
| Fruit and vegetables | Fruit preparations excluding compote | 800 |
| Glazings for vegetable products | 4000 | |
| Nut butters and nut spreads (spreadable fats excluding butter) | 5000 | |
| Processed potato products including pre-fried frozen en deep-frozen potatoes | 5000 | |
| Desserts | Desserts | 3000 |
| Dry powdered dessert mixes | 7000 | |
| Confectionery | Sugar confectionery, except candied fruit | 5000 |
| Candied fruit | 800 | |
| Chewing gum | Quantum satis | |
| Decorations, coatings and fillings, except fruit-based fillings | 5000 | |
| Toppings (syrups for pancakes, flavoured syrups for milkshakes and ice cream; similar products) | 3000 | |
| Cereals and cereal products | Flours | 2500 |
| Self-raising flour | 20,000 | |
| Breakfast cereals | 5000 | |
| Noodles | 2000 | |
| Batters | 12,000 | |
| Soda bread and fine bakery wares | 20,000 | |
| Ready-to-eat savouries and snacks | Potato-, cereal-, flour- or starch-based snacks | 5000 |
| Meat and meat preparations | Non-heat-treated processed meat | 5000 |
| Heat-treated processed meat (except foie gras) | 5000 | |
| Glazings for meat | 4000 | |
| Fish and fisheries products | Frozen and deep-frozen fish fillets, molluscs and crustaceans | 5000 |
| Canned crustaceans products; surimi and similar products | 1000 | |
| Fish and crustacean paste and in processed frozen and deep-frozen molluscs and crustaceans | 5000 | |
| Eggs and egg products | Liquid egg (white, yolk or whole egg) | 10,000 |
| Salts, spices, soups, sauces, salads and protein products | Salt and salt substitutes | 10,000 |
| Soups and broths | 3000 | |
| Sauces | 5000 | |
| Vegetable protein drinks | 20,000 | |
| Alcoholic and non-alcoholic beverages | Water, including natural mineral water | 500 |
| Flavored drinks | 700 | |
| Whey protein containing sport drinks | 4000 | |
| Vegetable protein drinks | 20,000 | |
| Chocolate and malt dairy-based drinks | 2000 | |
| Coffee-based drinks for vending machines; Instant tea and instant herbal infusions | 2000 | |
| Cider and perry | 1000 | |
| Fruit wine and made wine | 1000 | |
| Mead | 1000 | |
| Spirit drinks (except: whisky, whiskey) | 1000 | |
| Aromatized wines | 1000 | |
| Aromatized wine-based drinks | 1000 | |
| Other alcoholic drinks including mixtures of alcoholic drinks with non-alcoholic drinks and spirits with less than 15% of alcohol | 1000 | |
| Foods intended for particular nutritional uses | Infant formulae as defined by Directive 2006/141/EC | 1000 |
| Follow-on formulae as defined by Directive 2006/141/EC | 1000 | |
| Processed cereal-based foods and baby foods for infants and young children as defined by Directive 2006/125/EC | 1000 (sonly cereals-E340) 5000 (biscuits and rusks-E450) | |
| Other foods for young children | 1000 | |
| Dietary foods for infants for special medical purposes and special formulae for infants | 1000 | |
| Foods suitable for people intolerant to gluten | 5000 | |
| Dietary foods for weight control diets intended to replace total daily food intake or an individual meal (the whole or part of the total daily diet) | 5000 | |
| Food supplements | Quantum satis |
| Food Category | Specifications | Maximum Level (mg/L or mg/Kg) |
|---|---|---|
| Dairy products | Curdled milk | 1000 * |
| Non-heat-treated dairy-based desserts | 300 ** | |
| Unripened cheese | 1000 * | |
| Cheese, prepacked, sliced and cut; layered cheese and cheese with added foods | 1000 * | |
| Ripened products surface treatment | Quantum satis | |
| Whey cheese, prepacked, sliced; layered cheese and cheese and cheese with added foods | 1000 * | |
| Processed cheese | 2000 * | |
| Unripened products; ripened products, prepacked, sliced; layered ripened products and ripened products with added foods | 1000 * | |
| Analogues of cheese based on protein | 2000 | |
| Ripened products surface treatment | Quantum satis | |
| Fat and oil emulsions | Fat emulsions (excluding butter) with a fat content of 60% or more | 1000 * |
| Fat emulsions with a fat content less than 60% | 2000 * | |
| Fruit and vegetables | Surface treatment of unpeeled fresh citrus fruit | 20 * |
| Dried fruit | 1000 * | |
| Olives and olive-based preparations | 1000 * | |
| Vegetables in vinegar, oil, or brine (excluding olives) | 2000 ** | |
| Fruit and vegetable preparations including seaweed based preparations, fruit-based sauces, aspic, excluding purée, mousse, compote, salads and similar products, canned or bottled | 1000 * | |
| 1000 ** (olive-based preparations) | ||
| Low-sugar and similar low calorie or sugar-free products, mermeladas | 1000 ** | |
| Low-sugar and similar low calorie or sugar-free products, spreads, mermeladas | 1000 ** | |
| Fruit-based spreads, mermeladas | 1000 ** | |
| Marmelade | 1500 ** | |
| Potato dough and pre-fried potato slices | 2000 | |
| Nuts | Coated nuts | 1000 *** |
| Desserts | Non-heat-treated dairy-based desserts | 300 ** |
| Confectionery | Candied, crystallized or glacé fruit and vegetables | 1000 ** |
| Other confectionery including breath freshening microsweets | 1500 *** | |
| Chewing gum | 1500 ** | |
| Toppings (syrups for pancakes, flavored syrups for milkshakes and ice cream; similar products) | 1000 | |
| Other decorations, coatings and fillings, except fruit-based fillings | 1500 *** | |
| Cereals and cereal products | Potato Gnocchi | 1000 |
| Fillings of stuffed pasta (ravioli and similar) | 1000 | |
| Batters | 2000 * | |
| Polenta | 200 * | |
| Prepacked sliced bread and rye-bread, partially baked, prepacked bakery wares intended for retail sale and energy-reduced bread intended for retail sale | 2000 | |
| Fine bakery wares (only with Aw >0.65) | 2000 | |
| Ready-to-eat savouries and snacks | Potato-, cereal-, flour- or starch-based snacks | 1000 ** |
| Meat and meat preparations | Surface treatment of dried meat products | Quantum satis *** |
| Pâté | 1000 *** | |
| Collagen-based casings with Aw >0.6 | Quantum satis | |
| Jelly coatings of meat products (cooked, cured or dried) | 1000 *** | |
| Fish and fisheries products | Salted, dried fish | 200 |
| Semi-preserved fish and fisheries products including crustaceans, molluscs, surimi and fish/crustacean paste; cooked crustaceans and molluscs | 2000 ** | |
| Semi-preserved fish products including fish roe products | 2000 ** |
| Food Category | Specifications | Maximum Level (mg/L or mg/Kg) |
|---|---|---|
| Meat and meat preparations | Non-heat-treated processed meat | 150 * |
| Traditional immersion and dry cured products (Meat products cured by immersion in a curing solution containing nitrites and/or nitrates, salt and other components) or Traditional dry cured products. (Dry curing process involves dry application of curing mixture containing nitrites and/or nitrates, salt and other components to the surface of the meat followed by a period of stabilization/maturation). | 250 ** | |
| Dairy products | Ripened cheese (hard, semi-hard and semi-soft cheese) | 150 |
| Whey cheese (cheese milk of hard, semi-hard and semi-soft cheese) | 150 | |
| Cheese products (hard, semi-hard and semi-soft ripened products) | 150 | |
| Dairy analogues, including beverage whiteners (only dairy-based cheese analogue) | 150 | |
| Fish and fisheries products | Processed fish and fishery products including molluscs and crustaceans (only pickled herring and sprat) | 500 |
References
- GBD Chronic Kidney Disease Collaboration. Global, Regional, and National Burden of Chronic Kidney Disease, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.-J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef] [PubMed]
- Cupisti, A.; Brunori, G.; Di lorio, B.; D’Alessandro, C.; Pasticci, F.; Cosola, C.; Bellizzi, V.; Bolasco, P.; Capitanini, A.; Fantuzzi, A.L.; et al. Nutritional Treatment of Advanced CKD: Twenty Consensus Statements. J. Nephrol. 2018, 31, 457–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vega, L.B.; Galabia, E.R.; da Silva, J.B.; González, M.B.; Fresnedo, G.F.; Haces, C.P.; Fontanet, R.P.; Millán, J.C.R.S.; de Francisco, Á.L.M. Epidemiology of hyperkalemia in chronic kidney disease. Nefrología 2019, 39, 277–286. [Google Scholar] [CrossRef]
- Kovesdy, C.; Matsushita, K.; Sang, Y.; Brunskill, N.; Carrero, J.; Chodick, G.; Hasegawa, T.; Heerspink, H.; Hirayama, A.; Landman, G. Serumpotassium and Adverse Outcomes Across the Range of Kidney Function: A CKD Prognosis Consortium Meta-Analysis. Eur. Heart J. 2018, 39, 1535–1542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picard, K.; Silva, M.I.B.; Mager, D.; Richard, C. Dietary Potassium Intake and Risk of Chronic Kidney Disease Progression in Predialysis Patients with Chronic Kidney Disease: A Systematic Review. Adv. Nutr. 2020, 11, 1002–1015. [Google Scholar] [CrossRef] [PubMed]
- Academy of Nutrition and Dietetics. 2010 Chronic Kidney Disease (CKD) Evidence-Based Nutrition Practice Guideline. Evidence Analysis Library. 2010. Available online: https://www.andeal.org/topic.cfm?cat=3927 (accessed on 30 July 2021).
- Picard, K. Potassium Additves and Bioavailability: Are we Missing Something in Hyperkalemia Management? J. Ren. Nutr. 2019, 29, 350–353. [Google Scholar] [CrossRef] [PubMed]
- European Comission. Additives. What are Food Additives? Available online: https://ec.europa.eu/food/safety/food-improvement-agents/additives_en (accessed on 17 May 2021).
- Winger, R.J.; Uribarri, J.; Lloyd, L. Phosphorus-containing food additives: An insidious danger for people with chronic kidney disease. Trends Food Sci. Technol. 2012, 24, 92–102. [Google Scholar] [CrossRef]
- Sullivan, C.E.A. Effect of Food Additives on Hyerphosphatemia among Patients with End-Stage Renal Disease: A Randomized Controlled Trial. JAMA 2009, 301, 629–635. [Google Scholar] [CrossRef]
- Caldeira, D.; Amaral, T.; David, C.; Sampaio, C. Educational Strategies to Reduce Serum Phosphorus in Hyperphosphatemic Patients with Chronic Kidney Disease: Systematic Review with Meta-analysis. J. Ren. Nutr. 2011, 21, 285–294. [Google Scholar] [CrossRef]
- D’Alessandro, C.; Piccoli, G.B.; Cupisti, A. The “phosphorus pyramid”: A visual tool for dietary phosphate management in dialysis and CKD patients. BMC Nephrol. 2015, 16, 9. [Google Scholar] [CrossRef] [PubMed]
- Braschi, A.; Gill, l.; Naismith, D. Partial Subsitution of Sodium with Potassium in White Bread. Feasibility and Bioa-vailability. Int. J. Food Sci. Nutr. 2009, 60, 507–521. [Google Scholar] [CrossRef] [PubMed]
- Macdonald-Clarke, C.; Martin, B.R.; McCabe, L.D.; McCabe, G.P.; Lachcik, P.J.; Wastney, M.; Weaver, C.M. Bioavailability of potassium from potatoes and potassium gluconate: A randomized dose response trial. Am. J. Clin. Nutr. 2016, 104, 346–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Comission. Commission Regulation (EU) no 1129/2011 of 11 November 2011 Amending Annex II to Regulation (EC) no 1333/2008 of the European Parliament and of the Council by Establishing a Union List of Food Additives. OJEU 2011, 295, 1–178. [Google Scholar]
- The European Parliament and the Council of the European Union. Regulation (EC) no 1333/2008 of the European Parliament and of the Council of 16 December 2008 on Food Additives. OJEU 2008, 354, 16–33. [Google Scholar]
- European Parliament. Commission Regulation (EU) No 231/2012 of 9 March 2012 Laying Down Specifications for Food Additives Listed in Annexes II and III to Regulation (EC) No 1333/2008 of the European Parliament and of the Council Text with EEA Relevance. OJEU 2012, 83, 1–295. [Google Scholar]
- Cupisti, A.; Kovesdy, C.; Claudia D’Alessandro, C.; Kalantar-Zadeh, K. Dietary Approach to Recurrent or Chronic Hyper-kalaemia in Patients with Decreased Kidney Function. Nutrients 2018, 10, 261. [Google Scholar] [CrossRef] [Green Version]
- Lou, L.; Aranaudas, L.; Caverni, A.; Vercet, A.; Caramelo, R.; Munguía, P.; Campos, B.; García, M.; Moragrera, B.; Moreno, R.; et al. Fuentes Ocultas De Fósforo: Presencia De Aditivos Con Contenido En Fósforo En Los Alimentos Procesados. Rev. Nefrol. 2014, 34, 498–506. [Google Scholar]
- Parpia, A.; L’Abbé, M.; Goldstein, M.; Joanne Arcand, J.; Magnuson, B.; Darling, P. The Impact of Additives on the Phosphorus, Potassium, and Sodium Content of Commonly Consumed Meat, Poultry, and Fish Products among Patients with Chronic Kidney Disease. J. Ren. Nutr. 2018, 28, 83–90. [Google Scholar] [CrossRef]
- Sherman, R.; Metha, O. Phosphorus and Potassium Content of Enhanced Meat and Poultry Products: Implications for Patients Who Receive Dialysis. Clin. J. Am. Soc. Nephrol. 2009, 4, 1370–1373. [Google Scholar] [CrossRef]
- Caverni-Muñoz, A.; Martínez-Pineda, M.; Sanz-Paris, A.; Lou-Arnal, L.; Vercet-Tormo, A.; Yagüe-Ruiz, C. Actualización De Las Pautas Dietéticas En La Enfermedad Renal Crónica, 1st ed.; Alcer-Ebro: Zaragoza, Spain, 2017; p. 34. [Google Scholar]
- EFSA Panel on Food Additives and Flavourings (FAF); Younes, M.; Aquilina, G.; Castle, L.; Engel, K.; Fowler, P.; Frutos Fernandez, M.; Fürst, P.; Gürtler, R.; Gundert-Remy, U.; et al. Opinion on the Follow-Up of the Re-Evaluation of Sorbic Acid (E200) and Potassium Sorbate (E202) as Food Additives. EFSA J. 2019, 17, 5625. [Google Scholar]
- World Health Organization. Regional Office for Europe. Mapping Salt Reduction Initiatives in the WHO European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 2013; p. 64. [Google Scholar]
- The European Parliament and the Council of the European Union. Regulation (EU) No 1169/2011 of the European Parliament and of the Council of 25 October 2011 on the Provision of Food Information to Consumers, Amending Regulations (EC) No 1924/2006 and (EC) No 1925/2006 of the European Parliament and of the Council, and Repealing Commission Directive 87/250/EEC, Council Directive 90/496/EEC, Commission Directive 1999/10/EC, Directive 2000/13/EC of the European Parliament and of the Council, Commission Directives 2002/67/EC and 2008/5/EC and Commission Regulation (EC) No 608/2004 Text with EEA Relevance. OJEU 2011, 304, 1–65. [Google Scholar]
- Parpia, A.; Goldstein, M.; Arcand, J.; Cho, F.; L’Abbé, M.; Darling, P. Sodium-Reduced Meat and Poultry Products Contain a Significant Amount of Potassium from Food Additives. JAND 2018, 118, 878–885. [Google Scholar] [CrossRef] [PubMed]
- Nerbass, F.B.; Calice-Silva, V.; Pecoits-Filho, R. Sodium Intake and Blood Pressure in Patients with Chronic Kidney Disease: A Salty Relationship. Blood Purif. 2018, 45, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Cobb, M.; Pacitti, D. The Importance of Sodium Restrictions in Chronic Kidney Disease. J. Ren. Nutr. 2018, 28, e37–e40. [Google Scholar] [CrossRef] [Green Version]
- McMahon, E.; Campbell, K.; Bauer, J.; Mudge, D.; Kelly, J. Altered Dietary Salt Intake for People with Chronic Kidney Disease. Cochrane Database Syst. Rev. 2021, 6, CD010070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kidney Disease: Improving Global Outcomes (KDIGO) Blood Pressure Work Group. KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney Int. 2021, 99, S1–S87. [Google Scholar] [CrossRef]
- Sarathy, S.; Sullivan, C.; Leon, J.B.; Sehgal, A.R. Fast Food, Phosphorus-Containing Additives, and the Renal Diet. J. Ren. Nutr. 2008, 18, 466–470. [Google Scholar] [CrossRef]
 France;
France;  Germany;
Germany;  Spain;
Spain;  Global sample.
France; Germany; Spain; Global sample.
Global sample.
France; Germany; Spain; Global sample.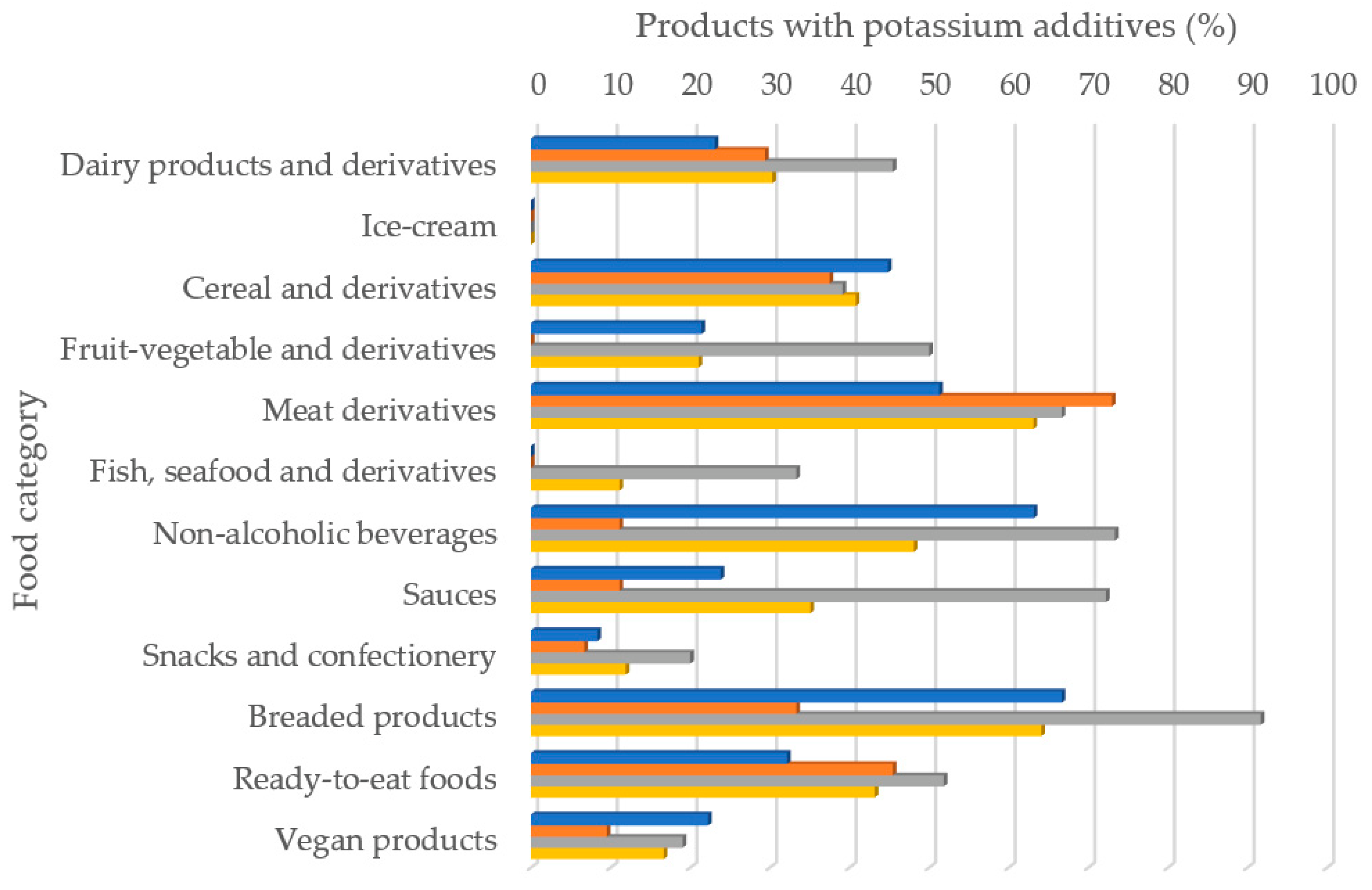 HKC: additives with high potassium content; MKC: additives with moderate potassium content;
HKC: additives with high potassium content; MKC: additives with moderate potassium content;  LKC: additives with low potassium content.
HKC: additives with high potassium content; MKC: additives with moderate potassium content; LKC: additives with low potassium content.
LKC: additives with low potassium content.
HKC: additives with high potassium content; MKC: additives with moderate potassium content; LKC: additives with low potassium content.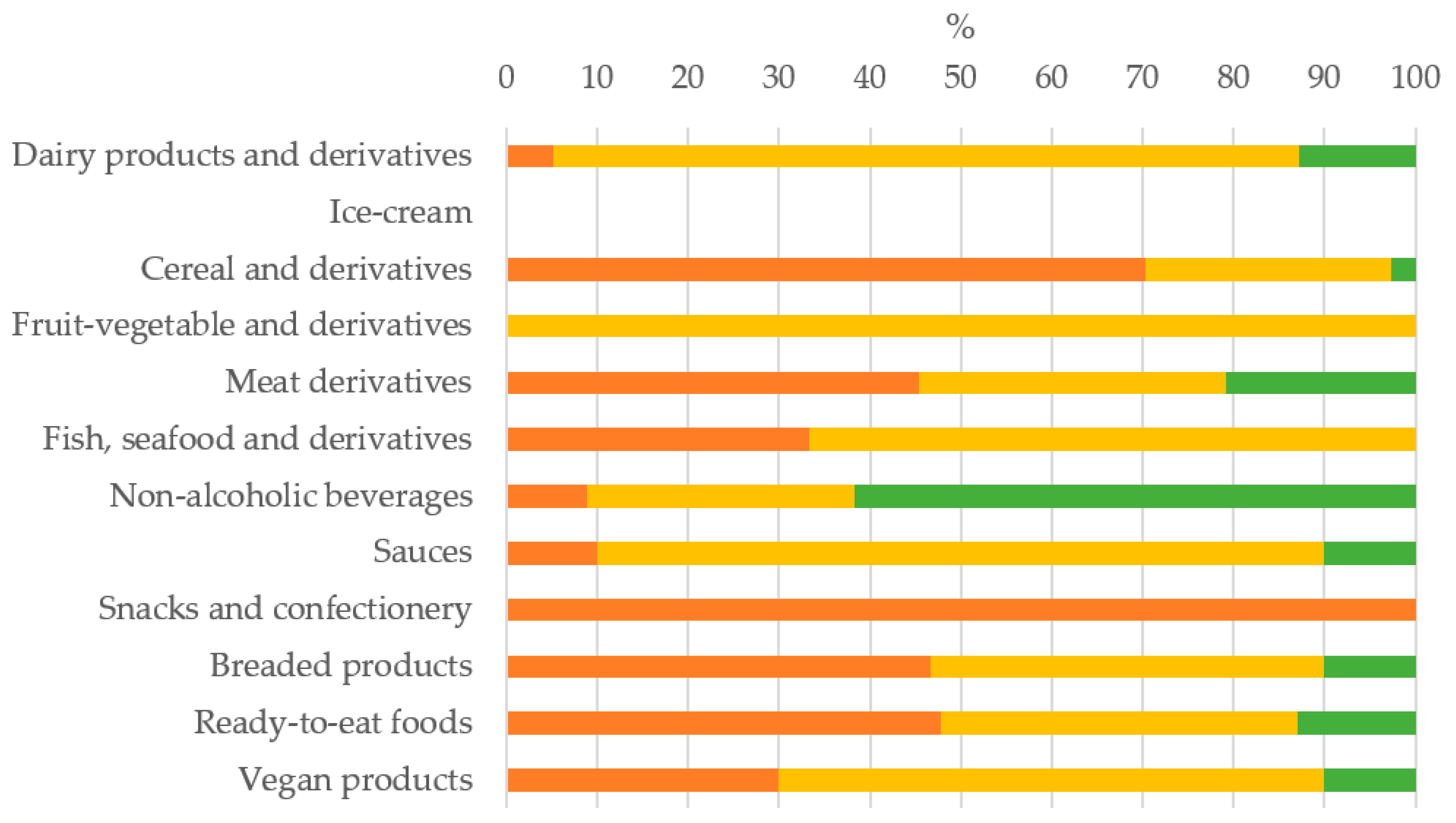 France; Germany; Spain; Global sample.
France; Germany; Spain; Global sample.
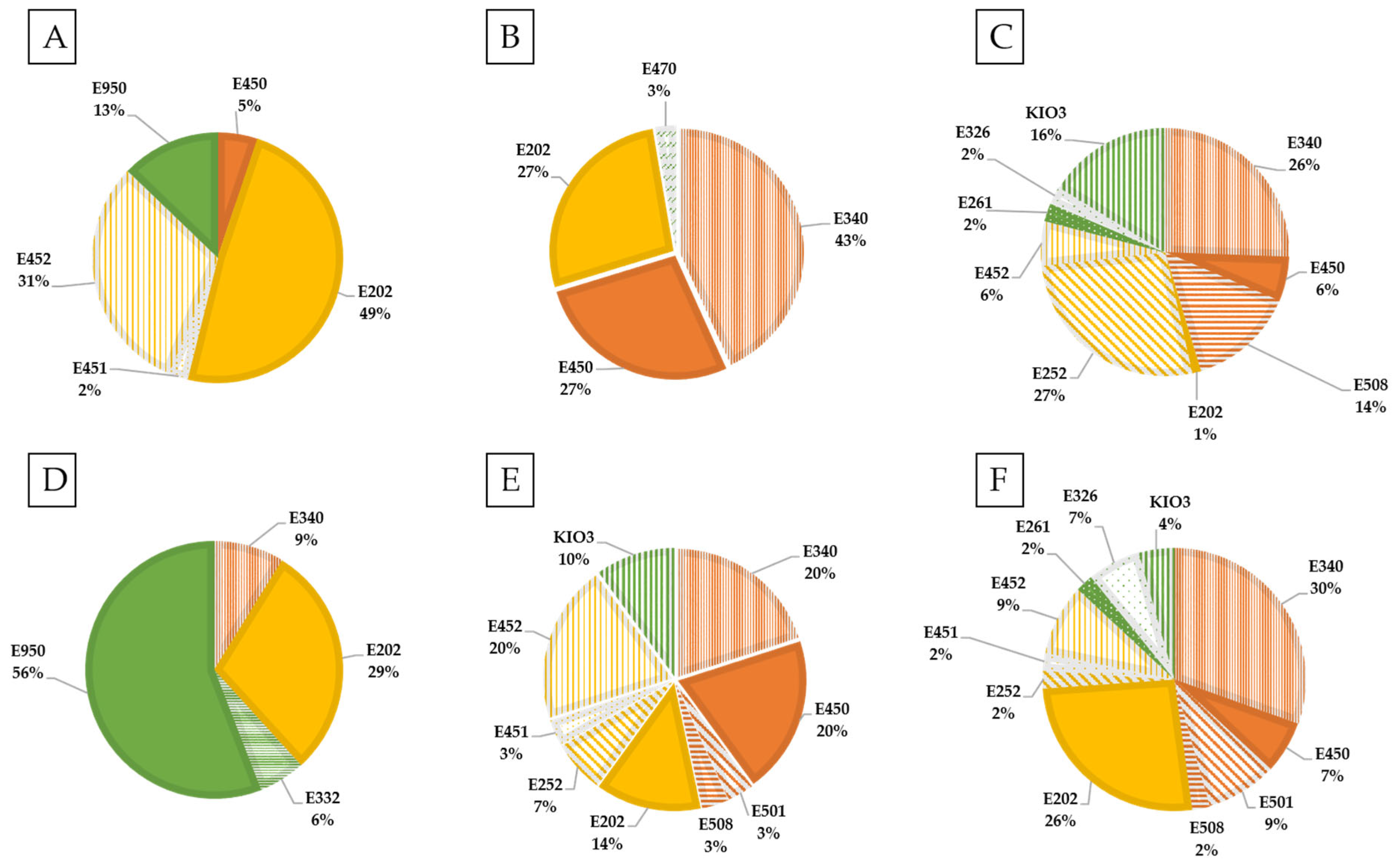
France; Germany; Spain; Global sample.
France; Germany; Spain; Global sample.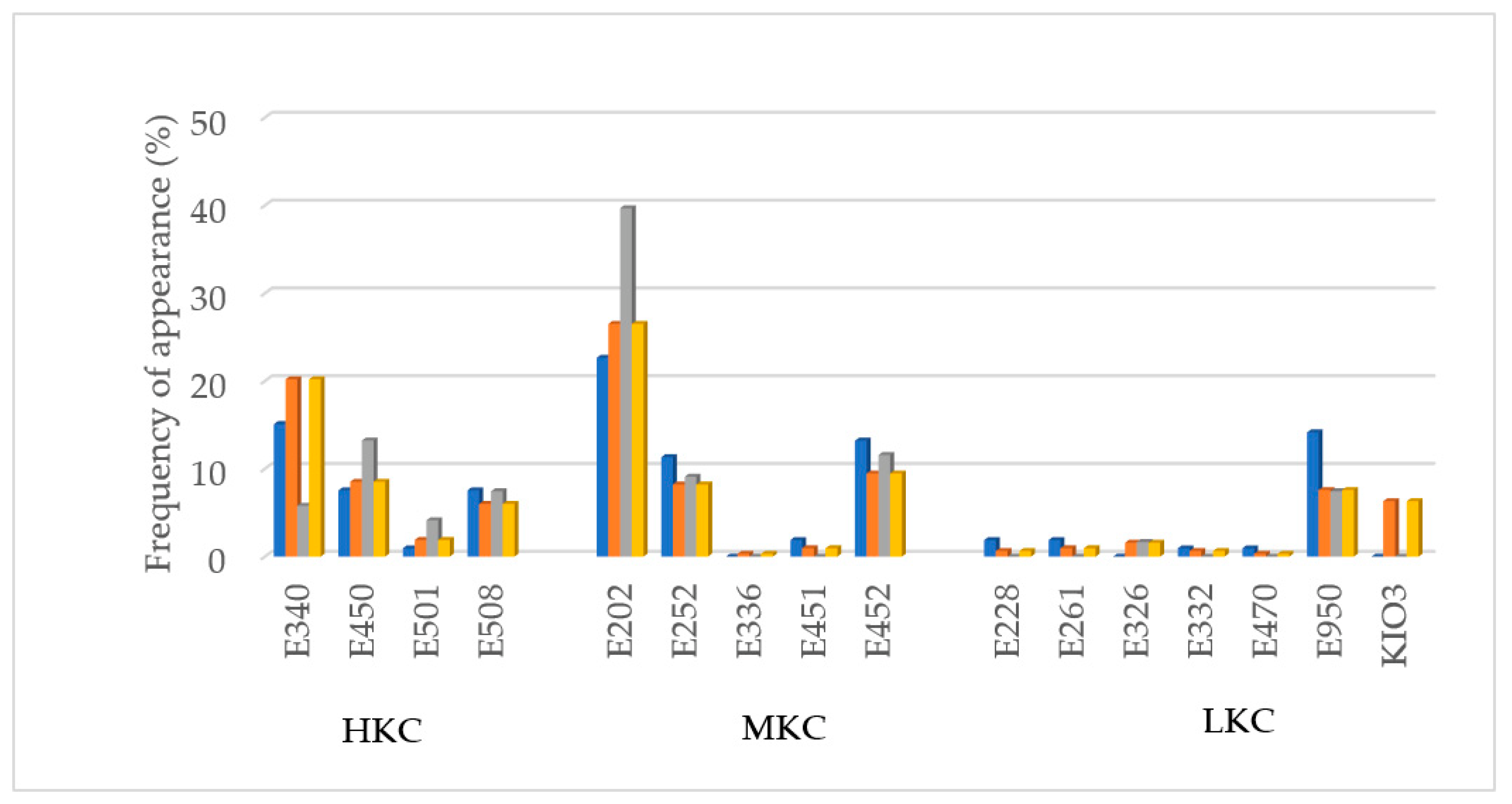
| Food Category | France (n = 270) | Germany (n = 233) | Spain (n = 212) | Total (n = 715) |
|---|---|---|---|---|
| Dairy products and derivatives | 65 | 34 | 33 | 132 |
| Ice-cream | 4 | 3 | 3 | 10 |
| Cereal and derivatives | 29 | 24 | 23 | 76 |
| Fruit/vegetable and derivatives | 14 | 12 | 12 | 38 |
| Meat derivatives | 39 | 37 | 27 | 103 |
| Fish, seafood and derivatives | 6 | 6 | 6 | 18 |
| Non-alcoholic beverages | 19 | 18 | 15 | 52 |
| Sauces | 21 | 18 | 18 | 57 |
| Snacks and confectionery | 12 | 15 | 15 | 42 |
| Breaded products | 15 | 12 | 12 | 39 |
| Ready-to-eat foods | 28 | 33 | 27 | 88 |
| Vegan products | 18 | 21 | 21 | 60 |
| LKC * (<25% by Weight of K) | MKC * (25–39% by Weight of K) | HKC * (≥40% by Weight of K) | ||||||
|---|---|---|---|---|---|---|---|---|
| E-Number | Name | Potassium Weight (%) | E-Number | Name | Potassium Weight (%) | E-Number | Name | Potassium Weight (%) |
| E 212 | Potassium benzoate | 18.1 | E 202 | Potassium sorbate | 25.8 | E 249 | Potassium nitrite | 43.6 |
| E 228 | Potassium hydrogen sulphite | 9.1 | E 224 | Potassium metabisulphite | 31.7 | E 340 | Potassium diphosphates | 44.0 |
| E 261 | Potassium acetate | 39.4 | E 252 | Potassium nitrate | 38.3 | E 340 | Potassium triphosphates | 53.6 |
| E 261 | Potassium diacetate | 15.8 | E 283 | Potassium propionate | 34.5 | E 450 | Tetrapotassium diphosphate | 45.0 |
| E 326 | Potassium lactate | 20.1 | E 332 | Potassium citrates | 35.8 | E 501ii | Potassium hydrogen carbonate | 56.0 |
| E 332 | Potassium citrates | 16.8 | E 336 | Potassium ditartrates | 32.9 | E 508 | Potassium chloride | 51.9 |
| E 336 | Potassium tartrates | 16.8 | E 340 | Potassium monophosphates | 28.4 | E 515 | Potassium sulphates | 44.4 |
| E 337 | Sodium potassium tartrate | 13.7 | E 351 | Potassium malate | 26.0 | E 525 | Potassium hydroxide | 62.7 |
| E 402 | Potassium alginate | 17.4 | E 357 | Potassium adipate | 34.8 | |||
| E 470a | Sodium, potassium and calcium salts of fatty acids | 17.9 | E 451ii | Pentapotassium triphosphate | 39.2 | |||
| E 522 | Aluminium potassium sulphate | 8.2 | E452ii | Potassium polyphosphate | 32.8 | |||
| E 555 | Potassium aluminium silicate | 9.7 | E 456 | Potassium polyaspartate | 25.0 | |||
| E 577 | Potassium gluconate | 16.5 | E 501 | Potassium carbonates | 38.7 | |||
| E 622 | Monopotassium glutamate | 19.0 | E 515i | Potassium acid sulfate | 28.4 | |||
| E 628 | Dipotassium guanylate | 17.3 | E 536 | Potassium ferrocyanide | 36.7 | |||
| E 632 | Dipotassium inosinate | 17.9 | ||||||
| E 950 | Acesulfame K | 19.2 | ||||||
| E 954 | Saccharin and its Na, K and Ca salts | 16.1 | ||||||
| Food Category | Specifications |
|---|---|
| Dairy products | Unflavored fermented dairy products heat-treated after fermentation |
| Flavored fermented dairy products, even heat-treated | |
| Other creams | |
| Unripened cheese, except mozzarella and unripened cheese fermented by the action of living organisms, without flavoring | |
| Processed cheese | |
| Cheese products (excluding dessert products) | |
| Dairy analogues, including beverage whiteners | |
| Ice-cream | Ice-cream |
| Fats, oils and their emulsions | Other fat and oil emulsions including spreads as defined by Regulation (EC) No 1234/2007 and liquid emulsions |
| Vegetable oil pan spray | |
| Fruits and vegetables | Dried fruit and vegetables |
| Fruit and vegetables in vinegar, oil, or brine | |
| Fruit and vegetable preparations excluding compote | |
| Nut butters and nut spreads | |
| Processed potato products | |
| Nuts | Processed nuts |
| Desserts | Desserts excluding dairy products, ice-creams, and fruit vegetables. |
| Confectionery products | Cocoa and chocolate products, energy-reduced only or no added sugar |
| Other confectionery products, including breath fresheners | |
| Chewing gum | |
| Decorations, coatings and fillings | |
| Cereals and derivatives | Starches |
| Breakfast cereals | |
| Dry pasta, gluten-free or intended for low-protein diets | |
| Potato gnocchi | |
| Fillings of stuffed pasta (ravioli and similar) | |
| Noodles | |
| Batters | |
| Pre-cooked or processed cereals | |
| Bread and rolls excluding those prepared solely with the following ingredients: wheat flour, water, yeast or leaven, salt. | |
| Fine bakery wares | |
| Ready-to-eat savouries and snacks | Potato-, cereal-, flour- or starch-based snacks |
| Meat and meat derivatives | Non-heat-treated processed meat |
| Heat-treated processed meat excluding foie gras, foie gras entier, blocs de foie gras. | |
| Casings and coatings and decorations for meat | |
| Seafood and derivatives | Processed fish and fishery products including mollusks and crustaceans |
| Fish roe | |
| Eggs and egg products | Processed eggs and egg products |
| Salt, spices, soups, sauces, salads, and protein products | Other sugars and syrups |
| Salt Substitutes, Seasonings, and Dressings | |
| Sauces | |
| Vinegars | |
| Mustard | |
| Soups and broths | |
| Salads and savoury based sandwich spreads | |
| Beverages | Fruit juices and vegetable or legume juices |
| Fruit nectars | |
| Flavoured drinks | |
| Others | |
| Cider and perry | |
| Fruit wine and made wine | |
| Mead | |
| Spirit drinks | |
| Aromatised wines | |
| Aromatised wine-based drinks | |
| Aromatised wine-product cocktails | |
| Other alcoholic drinks including mixtures of alcoholic drinks with non-alcoholic drinks and spirits with less than 15% of alcohol | |
| Foods intended for particular nutritional uses as defined by Directive 2009/39/EC. | Dietary foods for special medical purposes |
| Dietary foods for weight control diets intended to replace total daily food intake or an individual meal (the whole or part of the total daily diet) | |
| Foods suitable for people intolerant to gluten | |
| Food supplements |
| Food Category | France | Germany | Spain | Global Sample |
|---|---|---|---|---|
| Dairy products and derivatives | 3 | 3 | 4 | 5 |
| Ice-cream | 0 | 0 | 0 | 0 |
| Cereal and derivatives | 4 | 3 | 3 | 4 |
| Fruit/vegetable and derivatives | 1 | 0 | 1 | 1 |
| Meat derivatives | 6 | 6 | 7 | 9 |
| Fish, seafood and derivatives | 0 | 0 | 2 | 2 |
| Non-alcoholic beverages | 3 | 2 | 3 | 4 |
| Sauces | 2 | 2 | 2 | 4 |
| Snacks and confectionery | 1 | 1 | 2 | 2 |
| Breaded products | 5 | 2 | 6 | 9 |
| Ready-to-eat foods | 6 | 6 | 5 | 11 |
| Vegan products | 2 | 2 | 2 | 4 |
| Functional Property | Frequency of Use (%) | Main Potassium Additives Used |
|---|---|---|
| Preservative | 36.96 | E202/E252/E261 |
| Stabilizer | 20.19 | E340/E450 |
| Flavoring agent | 12.73 | E508/KIO3 |
| Sweetener | 10.56 | E950 |
| Emulsifying salt | 7.45 | E340/E450/E451/E452 |
| Raising agent | 6.52 | E340/E450/ |
| Acidity regulators | 3.73 | E332/E501/E326/E340/E452 |
| Other | 1.86 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Pineda, M.; Vercet, A.; Yagüe-Ruiz, C. Are Food Additives a Really Problematic Hidden Source of Potassium for Chronic Kidney Disease Patients? Nutrients 2021, 13, 3569. https://doi.org/10.3390/nu13103569
Martínez-Pineda M, Vercet A, Yagüe-Ruiz C. Are Food Additives a Really Problematic Hidden Source of Potassium for Chronic Kidney Disease Patients? Nutrients. 2021; 13(10):3569. https://doi.org/10.3390/nu13103569
Chicago/Turabian StyleMartínez-Pineda, Montserrat, Antonio Vercet, and Cristina Yagüe-Ruiz. 2021. "Are Food Additives a Really Problematic Hidden Source of Potassium for Chronic Kidney Disease Patients?" Nutrients 13, no. 10: 3569. https://doi.org/10.3390/nu13103569
APA StyleMartínez-Pineda, M., Vercet, A., & Yagüe-Ruiz, C. (2021). Are Food Additives a Really Problematic Hidden Source of Potassium for Chronic Kidney Disease Patients? Nutrients, 13(10), 3569. https://doi.org/10.3390/nu13103569