Changes in Consumers’ Food Practices during the COVID-19 Lockdown, Implications for Diet Quality and the Food System: A Cross-Continental Comparison

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Sampling
2.2. Procedure
2.3. Survey Measures
2.3.1. Cooking Related Variables
2.3.2. COVID-19 Related Issues
2.3.3. Food Practices
2.3.4. Diet Quality
2.4. Statistical Analysis
3. Results
3.1. Participant Sociodemographic Characteristics
3.2. EFA and CFA Validation of Emergency Situation Food Practices Measure
3.2.1. EFA
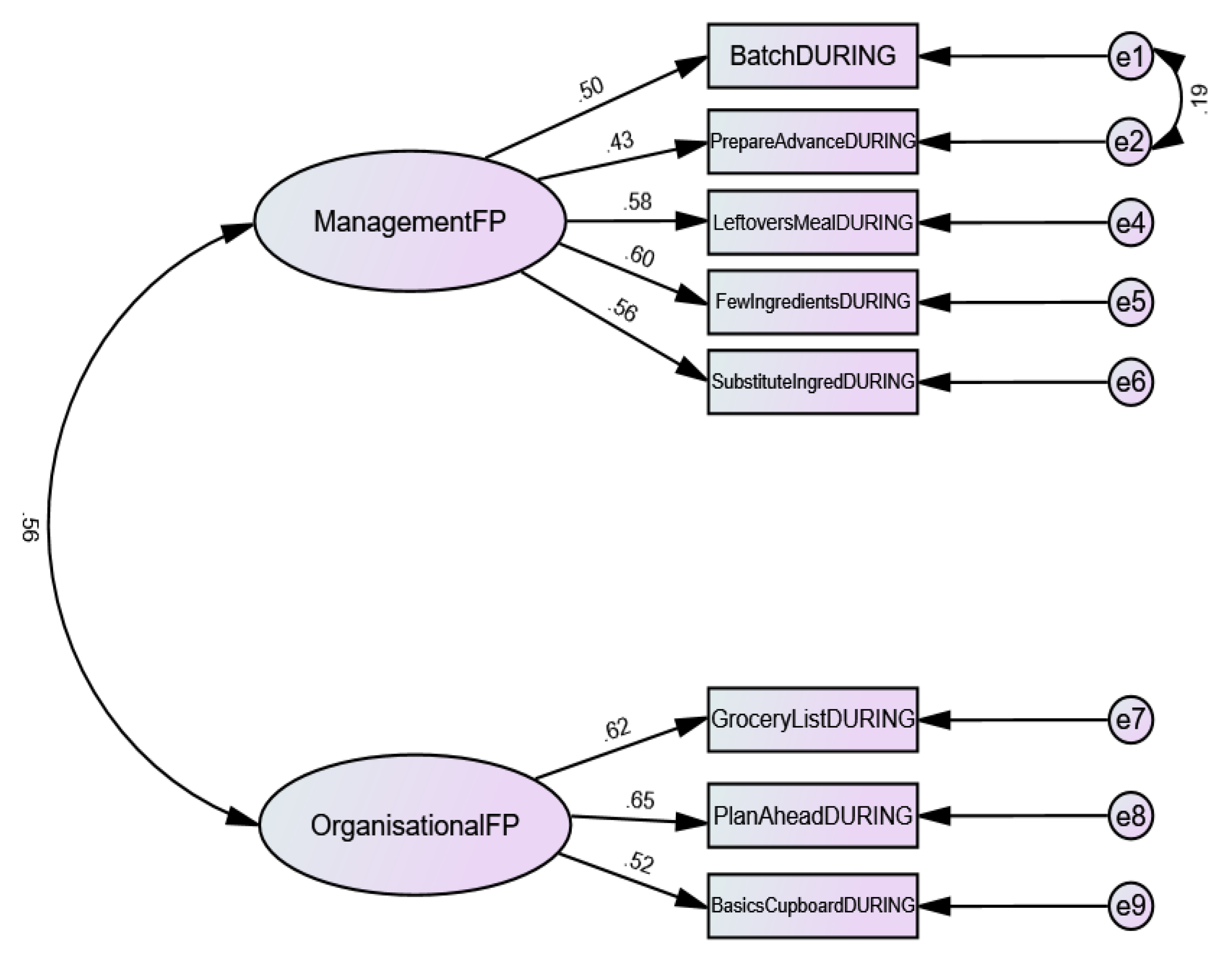
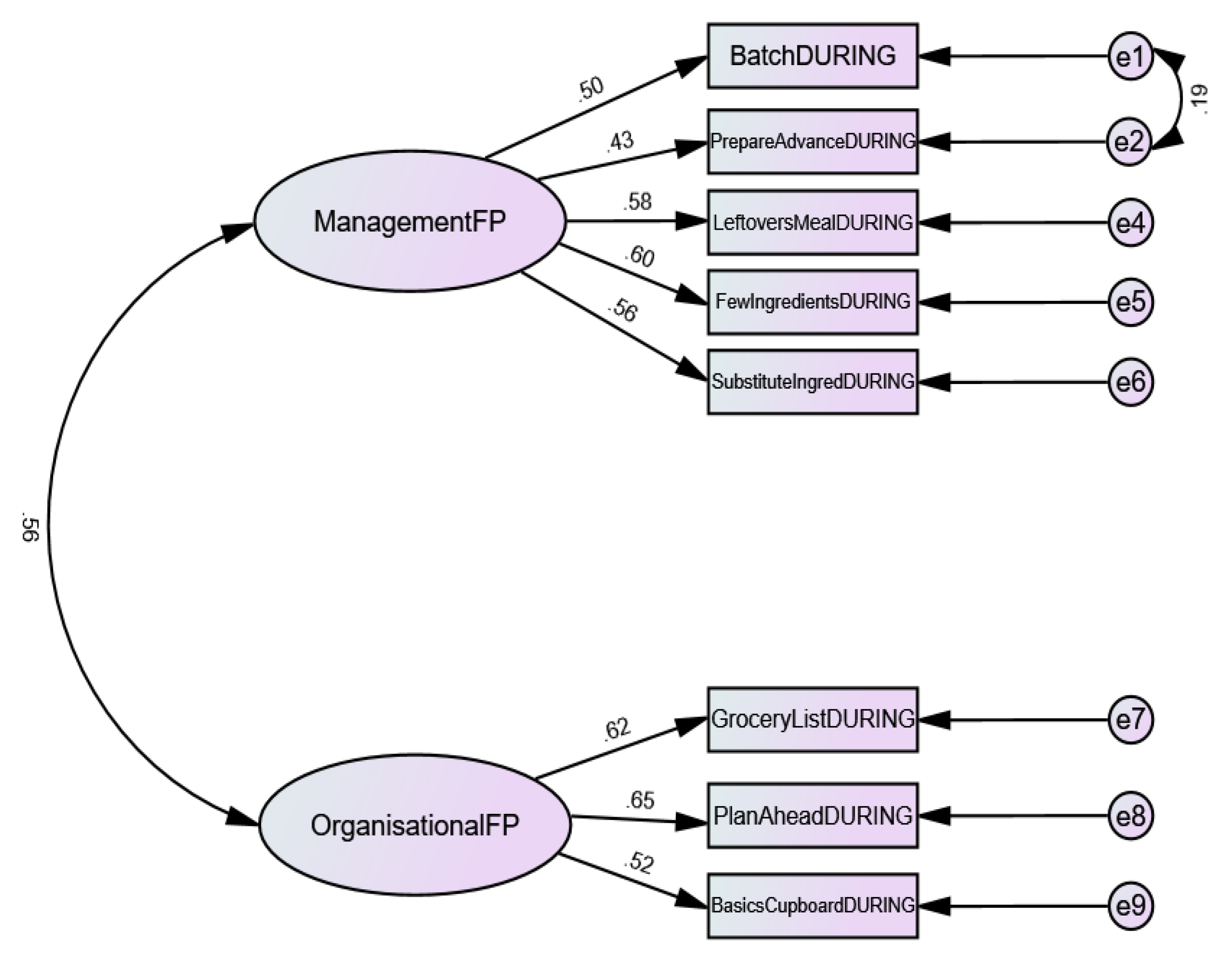
3.2.2. CFA
3.3. Food Practice Changes Relating to COVID-19 within Countries
3.3.1. Cooking Related Variables
3.3.2. COVID-19 Related Issues
3.3.3. Food Practices
3.3.4. Diet Quality
3.4. Inter Region Differences
3.4.1. Cooking Related Variables
3.4.2. COVID-19 Related Issues
3.4.3. Food Practices
3.4.4. Diet Quality
4. Discussion
4.1. Implications for Health and Food Systems for Continued (Local or Regional) Lockdowns and into the Future
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Laborde, D.; Vos, R.; Martin, W.J. Poverty and food insecurity could grow dramatically as COVID-19 spreads. In Food SecurIty, Poverty, and InequalIty; International Food Policy Research Institute (IFPRI): Washington, DC, USA, 2020; pp. 16–19. [Google Scholar]
- Kramer, A.; Kramer, K.Z. The potential impact of the Covid-19 pandemic on occupational status, work from home, and occupational mobility. J. Vocat. Behav. 2020, 119, 103442. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.C.; Prayag, G.; Fieger, P.; Dyason, D. Beyond panic buying: Consumption displacement and COVID-19. J. Serv. Manag. 2020. ahead of print. [Google Scholar] [CrossRef]
- Hobbs, J.E. Food supply chains during the COVID-19 pandemic. Can. J. Agric. Econ. 2020, 68, 171–176. [Google Scholar] [CrossRef] [Green Version]
- Lavelle, F.; McGowan, L.; Spence, M.; Caraher, M.; Raats, M.M.; Hollywood, L.; McDowell, D.; McCloat, A.; Mooney, E.; Dean, M. Barriers and facilitators to cooking from ‘scratch’ using basic or raw ingredients: A qualitative interview study. Appetite 2016, 107, 383–391. [Google Scholar] [CrossRef] [Green Version]
- McGowan, L.; Pot, G.K.; Stephen, A.M.; Lavelle, F.; Spence, M.; Raats, M.; Hollywood, L.; McDowell, D.; McCloat, A.; Mooney, E.; et al. The influence of socio-demographic, psychological and knowledge-related variables alongside perceived cooking and food skills abilities in the prediction of diet quality in adults: A nationally representative cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Lavelle, F.; Bucher, T.; Dean, M.; Brown, H.M.; Rollo, M.E.; Collins, C.E. Diet quality is more strongly related to food skills rather than cooking skills confidence: Results from a national cross-sectional survey. Nutr. Diet. 2019, 77, 112–120. [Google Scholar] [CrossRef]
- Wolfson, J.A.; Lahne, J.; Raj, M.; Insolera, N.; Lavelle, F.; Dean, M. Food agency in the united states: Associations with cooking behavior and dietary intake. Nutrients 2020, 12, 877. [Google Scholar] [CrossRef] [Green Version]
- Wolfson, J.A.; Bleich, S.N. Is cooking at home associated with better diet quality or weight-loss intention? Public Health Nutr. 2015, 18, 1397–1406. [Google Scholar] [CrossRef] [Green Version]
- Mills, S.; Brown, H.; Wrieden, W.; White, M.; Adams, J. Frequency of eating home cooked meals and potential benefits for diet and health: Cross-sectional analysis of a population-based cohort study. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–11. [Google Scholar] [CrossRef]
- Blanchflower, D.G.; Oswald, A.J.; Stewart-Brown, S. Is Psychological Well-Being Linked to the Consumption of Fruit and Vegetables? Soc. Indic. Res. 2013, 114, 785–801. [Google Scholar] [CrossRef] [Green Version]
- Crawford, D.; Ball, K.; Mishra, G.; Salmon, J.; Timperio, A. Which food-related behaviours are associated with healthier intakes of fruits and vegetables among women? Public Health Nutr. 2007, 10, 256–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Ansari, W.; Adetunji, H.; Oskrochi, R. Food and mental health: Relationship between food and perceived stress and depressive symptoms among university students in the United Kingdom. Cent. Eur. J. Public Health 2014, 22, 90–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCloat, A.; Mooney, E.; Hollywood, L.E. Have Irish parents put cooking on the back burner? An Island of Ireland study of the food skills, cooking confidence and practices of parents. Br. Food J. 2017, 119, 992–1002. [Google Scholar] [CrossRef]
- Lang, T.; Caraher, M. Is there a culinary skills transition? Data and debate from the UK about changes in cooking culture. J. Home Econ. Inst. Aust. 2001, 8, 2–14. [Google Scholar]
- Utter, J.; Denny, S.; Lucassen, M.; Dyson, B. Adolescent Cooking Abilities and Behaviors: Associations With Nutrition and Emotional Well-Being. J. Nutr. Educ. Behav. 2016, 48, 35–41. [Google Scholar] [CrossRef]
- Smith, L.P.; Ng, S.W.; Popkin, B.M. Trends in US home food preparation and consumption: Analysis of national nutrition surveys and time use studies from 1965–1966 to 2007–2008. Nutr. J. 2013, 12, 45. [Google Scholar] [CrossRef] [Green Version]
- Buckley, M.; Cowan, C.; McCarthy, M. The convenience food market in Great Britain: Convenience food lifestyle (CFL) segments. Appetite 2007, 49, 600–617. [Google Scholar] [CrossRef]
- De Boer, M.; McCarthy, M.; Cowan, C.; Ryan, I. The influence of lifestyle characteristics and beliefs about convenience food on the demand for convenience foods in the Irish market. Food Qual. Prefer. 2004, 15, 155–165. [Google Scholar] [CrossRef]
- Sheely, M. Global Adoption of Convenience Foods. Am. J. Agric. Econ. 2008, 90, 1356–1365. [Google Scholar] [CrossRef] [Green Version]
- Bava, C.M.; Jaeger, S.R.; Park, J. Constraints upon food provisioning practices in “busy” women’s lives: Trade-offs which demand convenience. Appetite 2008, 50, 486–498. [Google Scholar] [CrossRef] [PubMed]
- Reicks, M.; Trofholz, A.C.; Stang, J.S.; Laska, M.N. Impact of Cooking and Home Food Preparation Interventions Among Adults: Outcomes and Implications forFuture Programs. J. Nutr. Educ. Behav. 2014, 46, 259–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reicks, M.; Kocher, M.; Reeder, J. Impact of Cooking and Home Food Preparation Interventions Among Adults: A Systematic Review (2011–2016). J. Nutr. Educ. Behav. 2018, 50, 148–172. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.; Kupferschmidt, K. Countries test tactics in “war” against COVID-19. Science 2020, 367, 1287–1288. [Google Scholar] [CrossRef] [Green Version]
- Baker, M.G.; Wilson, N.; Anglemyer, A. Successful Elimination of Covid-19 Transmission in New Zealand. N. Engl. J. Med. 2020, 383, e56. [Google Scholar] [CrossRef]
- Bashir, M.F.; Ma, B.; Bilal; Komal, B.; Bashir, M.A.; Tan, D.; Bashir, M. Correlation between climate indicators and COVID-19 pandemic in New York, USA. Sci. Total Environ. 2020, 728, 138835. [Google Scholar] [CrossRef]
- Badr, H.S.; Du, H.; Marshall, M.; Dong, E.; Squire, M.M.; Gardner, L.M. Association between mobility patterns and COVID-19 transmission in the USA: A mathematical modelling study. Lancet Infect. Dis. 2020, 20, 1247–1254. [Google Scholar] [CrossRef]
- Mance, D.; Vretenar, N.; Gojković, J. Comparison of European Union Public Health Systems. Sel. Pap. 2019, 65–77. [Google Scholar] [CrossRef]
- Jarvis, C.I.; Van Zandvoort, K.; Gimma, A.; Prem, K.; Auzenbergs, M.; O’Reilly, K.; Medley, G.; Emery, J.C.; Houben, R.M.G.J.; Davies, N.; et al. Quantifying the impact of physical distance measures on the transmission of COVID-19 in the UK. BMC Med. 2020, 18, 1–10. [Google Scholar] [CrossRef]
- Davis, N.; Carroll, R. Experts Divided over Comparison of UK and Ireland’s Coronavirus Records. The Guardian. Available online: https://www.theguardian.com/world/2020/apr/13/experts-divided-comparison-uk-ireland-coronavirus-record (accessed on 26 October 2020).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Ann. Intern. Med. 2007, 147, 573. [Google Scholar] [CrossRef] [Green Version]
- Lavelle, F.; McGowan, L.; Hollywood, L.; Surgenor, D.; McCloat, A.; Mooney, E.; Caraher, M.; Raats, M.; Dean, M. The development and validation of measures to assess cooking skills and food skills. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Roe, L.; Strong, C.; Whiteside, C.; Neil, A.; Mant, D. Dietary intervention in primary care: Validity of the dine method for diet assessment. Fam. Pract. 1994, 11, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Yong, A.G.; Pearce, S. A Beginner’s Guide to Factor Analysis: Focusing on Exploratory Factor Analysis. Tutor. Quant. Methods Psychol. 2013, 9, 79–94. [Google Scholar] [CrossRef]
- Kaiser, H.F. An index of factorial simplicity. Psychometrika 1974, 39, 31–36. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 3rd ed.; Sage Publication: London, UK, 2013. [Google Scholar]
- Kaiser, H.F. The Application of Electronic Computers to Factor Analysis. Educ. Psychol. Meas. 1960, 20, 141–151. [Google Scholar] [CrossRef]
- Carpenter, S. Ten Steps in Scale Development and Reporting: A Guide for Researchers. Commun. Methods Meas. 2018, 12, 25–44. [Google Scholar] [CrossRef]
- Hinkin, T.R.; Tracey, J.B.; Enz, C.A. Scale construction: Developing reliable and valid measurement instruments. J. Hosp. Tour. Res. 1997, 21, 100–120. [Google Scholar] [CrossRef]
- Mills, S.; Adams, J.; Wrieden, W.; White, M.; Brown, H. Sociodemographic characteristics and frequency of consuming home-cooked meals and meals from out-of-home sources: Cross-sectional analysis of a population-based cohort study. Proc. Int. Astron. Union 2018, 21, 2255–2266. [Google Scholar] [CrossRef] [Green Version]
- Cairney, P. The UK government ’ s COVID - 19 policy: Assessing evidence—Informed policy analysis in real time. Br. Polit. 2020. [Google Scholar] [CrossRef]
- Loxton, M.; Truskett, R.; Scarf, B.; Sindone, L.; Baldry, G.; Zhao, Y. Consumer Behaviour during Crises: Preliminary Research on How Coronavirus Has Manifested Consumer Panic Buying, Herd Mentality, Changing Discretionary Spending and the Role of the Media in Influencing Behaviour. J. Risk Financ. Manag. 2020, 13, 166. [Google Scholar] [CrossRef]
- Sim, K.; Chua, H.C.; Vieta, E.; Fernandez, G. The anatomy of panic buying related to the current COVID-19 pandemic. Psychiatry Res. 2020, 288, 113015. [Google Scholar] [CrossRef] [PubMed]
- Naeem, M. Do social media platforms develop consumer panic buying during the fear of Covid-19 pandemic. J. Retail. Consum. Serv. 2021, 58, 102226. [Google Scholar] [CrossRef]
- Arafat, S.M.Y.; Kar, S.K.; Menon, V.; Kaliamoorthy, C.; Mukherjee, S.; Alradie-Mohamed, A.; Sharma, P.; Marthoenis, M.; Kabir, R. Panic buying: An insight from the content analysis of media reports during COVID-19 pandemic. Neurol. Psychiatry Brain Res. 2020, 37, 100–103. [Google Scholar] [CrossRef]
- Paci-Green, R.; Berardi, G. Do global food systems have an Achilles heel? The potential for regional food systems to support resilience in regional disasters. J. Environ. Stud. Sci. 2015, 5, 685–698. [Google Scholar] [CrossRef]
- Brunner, T.A.; van der Horst, K.; Siegrist, M. Convenience food products. Drivers for consumption. Appetite 2010, 55, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, M.; Ponzo, V.; Rosato, R.; Scumaci, E.; Goitre, I.; Benso, A.; Belcastro, S.; Crespi, C.; De Michieli, F.; Ghigo, E.; et al. Changes in weight and nutritional habits in adults with obesity during the “lockdown” period caused by the COVID-19 virus emergency. Nutrients 2020, 12, 2016. [Google Scholar] [CrossRef] [PubMed]
- Bhutani, S.; Cooper, J.A. COVID-19–Related Home Confinement in Adults: Weight Gain Risks and Opportunities. Obesity 2020, 28, 1576–1577. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; North, C.S. Mental Health and the Covid-19 Pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef]
- Ornell, F.; Schuch, J.B.; Sordi, A.O.; Kessler, F.H.P. “Pandemic fear” and COVID-19: Mental health burden and strategies. Brazilian, J. Psychiatry 2020, 42, 232–235. [Google Scholar] [CrossRef] [Green Version]
- Trattner, C.; Elsweiler, D.; Howard, S. Estimating the healthiness of internet recipes: A cross-sectional study. Front. Public Health 2017, 5, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Easterbrook-Smith, G. By Bread Alone: Baking as Leisure, Performance, Sustenance, During the COVID-19 Crisis. Leis. Sci. 2020, 1–7. [Google Scholar] [CrossRef]
- Tison, G.H.; Avram, R.; Kuhar, P.; Abreau, S.; Marcus, G.M.; Pletcher, M.J.; Olgin, J.E. Worldwide Effect of COVID-19 on Physical Activity: A Descriptive Study. Ann. Intern. Med. 2020, 173, 767–770. [Google Scholar] [CrossRef] [PubMed]
- Heinonen, K.; Strandvik, T. Reframing service innovation: COVID-19 as a catalyst for imposed service innovation. J. Serv. Manag. 2020. ahead of print. [Google Scholar] [CrossRef]
- Pantano, E.; Pizzi, G.; Scarpi, D.; Dennis, C. Competing during a pandemic? Retailers’ ups and downs during the COVID-19 outbreak. J. Bus. Res. 2020, 116, 209–213. [Google Scholar] [CrossRef]
- Galper, D.I.; Trivedi, M.H.; Barlow, C.E.; Dunn, A.L.; Kampert, J.B. Inverse association between physical inactivity and mental health in men and women. Med. Sci. Sports Exerc. 2006, 38, 173–178. [Google Scholar] [CrossRef] [Green Version]
- Dietz, W.; Santos-Burgoa, C. Obesity and its Implications for COVID-19 Mortality. Obesity 2020, 28, 1005. [Google Scholar] [CrossRef] [Green Version]
- Wolfson, J.A.; Leung, C.W. Food Insecurity During COVID-19: An Acute Crisis With Long-Term Health Implications. Am. J. Public Health 2020, 110, e1–e3. [Google Scholar] [CrossRef]
- Wiersma, W. The Validity of Surveys: Online and Offline. Oxf. Internet Inst. 2013, 18, 321–340. [Google Scholar]
- Kooij, D.T.A.M. The Impact of the Covid-19 Pandemic on Older Workers: The Role of Self-Regulation and Organizations. Work Aging Retire. 2020, 6, 233–237. [Google Scholar] [CrossRef]

{kind=link}
| Country/Region | Island of Ireland | Great Britain | USA | New Zealand | ||||
|---|---|---|---|---|---|---|---|---|
| Characteristic | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| Total (n) | 538 | 961 | 381 | 480 | ||||
| Age | 35.91 | 12.52 | 50.66 | 15.34 | 53.69 | 18.41 | 45.71 | 17.20 |
| Body Mass Index | 26.03 | 5.72 | 26.43 | 5.38 | 29.01 | 8.36 | 26.61 | 6.17 |
| n | % | n | % | n | % | n | % | |
| Gender | ||||||||
| Male | 67 | 12.5 | 468 | 48.7 | 176 | 46.1 | 229 | 47.7 |
| Female | 471 | 87.5 | 490 | 51.0 | 204 | 53.4 | 249 | 51.9 |
| Other | 3 | 0.3 | 2 | 0.5 | 2 | 0.4 | ||
| Education | ||||||||
| None | 3 | 0.3 | 3 | 0.6 | ||||
| Primary School | 3 | 0.6 | 11 | 1.1 | 3 | 0.8 | 10 | 2.1 |
| Secondary School | 74 | 13.8 | 238 | 24.8 | 66 | 17.3 | 104 | 21.7 |
| Additional Training | 85 | 15.8 | 217 | 22.6 | 76 | 19.9 | 106 | 22.1 |
| Undergraduate degree | 176 | 32.7 | 310 | 32.3 | 132 | 34.6 | 161 | 33.5 |
| Postgraduate degree | 200 | 37.2 | 182 | 18.9 | 105 | 27.4 | 96 | 20.0 |
| Employment Status | ||||||||
| Full Time | 300 | 55.8 | 396 | 41.2 | 130 | 34.0 | 237 | 49.4 |
| Furloughed or temporarily unemployed | 72 | 13.4 | 114 | 11.9 | 26 | 6.8 | 13 | 2.7 |
| Part time (less than 8 h per week) | 17 | 3.2 | 22 | 2.3 | 20 | 5.2 | 21 | 4.4 |
| Part time (greater than 8 h per week) | 74 | 13.8 | 88 | 9.2 | 17 | 4.5 | 51 | 10.6 |
| Retired | 11 | 2.0 | 233 | 24.2 | 149 | 39.0 | 80 | 16.7 |
| Long term sickness/disability | 9 | 1.7 | 31 | 3.2 | 9 | 2.4 | 22 | 4.6 |
| Unemployed (either seeking or not seeking employment) | 55 | 10.2 | 77 | 8.0 | 31 | 8.1 | 56 | 11.7 |
| Working from Home | ||||||||
| All working hours | 232 | 43.1 | 301 | 31.3 | 102 | 26.7 | 84 | 17.5 |
| Some working hours | 49 | 9.1 | 69 | 7.2 | 21 | 5.5 | 68 | 14.2 |
| Not working from home | 110 | 20.4 | 136 | 14.2 | 43 | 11.3 | 156 | 32.5 |
| Essential Worker Status | ||||||||
| Yes | 139 | 25.8 | 206 | 21.4 | 97 | 25.4 | 132 | 27.5 |
| No | 233 | 43.3 | 290 | 30.2 | 60 | 15.7 | 167 | 34.8 |
| Unsure | 20 | 3.7 | 10 | 1.0 | 10 | 2.6 | 10 | 2.1 |
| Parental Status (Under-16) | ||||||||
| Yes | 124 | 23.0 | 140 | 14.6 | 51 | 13.4 | 93 | 19.4 |
| No | 268 | 49.8 | 664 | 69.1 | 266 | 69.6 | 294 | 61.3 |
| Island of Ireland (n = 538) | Great Britain (n = 961) | USA (n = 382) | New Zealand (n = 480) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Before | During | Significance | Before | During | Significance | Before | During | Significance | Before | During | Significance |
| Cooking Related variables | Mean (SD) | Mean (SD) | p | Mean (SD) | Mean (SD) | p | Mean (SD) | Mean (SD) | p | Mean (SD) | Mean (SD) | p |
| Dinner—readymade | 1.88 (1.06) | 1.52 (0.81) | <0.0001 | 2.35 (1.13) | 2.14 (1.13) | <0.0001 | 2.62 (1.27) | 2.53 (1.35) | 0.1011 | 1.98 (1.09) | 1.84 (1.16) | 0.0002 |
| Dinner—mixed ingredients | 3.61 (1.39) | 3.58 (1.58) | 0.3403 | 3.29 (1.25) | 3.29 (1.37) | 0.9960 | 3.20 (1.39) | 3.20 (1.47) | 0.7604 | 3.25 (1.35) | 3.29 (1.49) | 0.3373 |
| Dinner—fresh ingredients | 4.42 (1.17) | 4.77 (1.11) | <0.0001 | 4.12 (1.26) | 4.25 (1.37) | <0.0001 | 3.53 (1.45) | 3.55 (1.49) | 0.6751 | 4.29 (1.25) | 4.32 (1.35) | 0.2351 |
| Eat Take Away | 2.58 (0.91) | 1.87 (.86) | <0.0001 | 2.34 (0.98) | 1.83 (1.02) | <0.0001 | 3.01 (1.26) | 2.62 (1.37) | <0.0001 | 2.63 (0.97) | 1.55 (1.02) | <0.0001 |
| Throw Away food—prepare too much | 2.63 (1.40) | 2.14 (1.14) | <0.0001 | 1.98 (1.20) | 1.80 (1.07) | <0.0001 | 2.11 (1.39) | 1.98 (1.33) | 0.0042 | 1.89 (1.14) | 1.71 (1.07) | <0.0001 |
| Throw awaypast the use-by date | 2.74 (1.04) | 2.22 (0.92) | <0.0001 | 2.06 (1.00) | 1.90 (0.99) | <0.0001 | 2.35 (1.27) | 2.20 (1.27) | 0.0010 | 2.01 (0.97) | 1.85 (1.01) | <0.0001 |
| Bake | 1.92 (0.90) | 2.82 (1.17) | <0.0001 | 2.15 (1.09) | 2.45 (1.23) | <0.0001 | 2.45 (1.34) | 2.53 (1.34) | 0.0929 | 2.35 (1.06) | 2.74 (1.23) | <0.0001 |
| COVID-19 related issues | ||||||||||||
| Difficulty finding ingredients | 2.12 (0.70) | 3.08 (0.79) | <0.0001 | 2.13 (0.78) | 2.85 (0.83) | <0.0001 | 2.25 (0.97) | 2.69 (1.03) | <0.0001 | 2.29 (0.83) | 2.70 (0.95) | <0.0001 |
| Bulk buying | 2.31 (0.99) | 2.92 (1.05) | <0.0001 | 2.33 (0.98) | 2.73 (1.04) | <0.0001 | 2.63 (1.06) | 3.14 (1.14) | <0.0001 | 2.49 (0.92) | 2.82 (1.03) | <0.0001 |
| Food Practices (FP) | ||||||||||||
| Organisational | 11.07 (2.49) | 12.82 (1.97) | <0.0001 | 10.95 (2.54) | 11.82 (2.48) | <0.0001 | 10.59 (2.69) | 11.18 (2.70) | <0.0001 | 10.90 (2.45) | 11.68 (2.48) | <0.0001 |
| Management | 14.78 (2.98) | 14.82 (3.04) | 0.4379 | 13.53 (2.99) | 13.95 (3.23) | <0.0001 | 13.27 (3.55) | 13.96 (3.90) | <0.0001 | 14.17 (2.88) | 14.27 (3.01) | 0.1117 |
| Overall Emergency Situation FP | 25.85 (4.63) | 27.64 (4.18) | <0.0001 | 24.48 (4.41) | 25.77 (4.62) | <0.0001 | 23.86 (5.08) | 25.14 (5.46) | <0.0001 | 25.07 (4.34) | 25.94 (4.46) | <0.0001 |
| Diet Quality Indicators | ||||||||||||
| Portions of Fruit per day | 2.21 (1.32) | 2.29 (1.46) | 0.0343 | 2.29 (1.52) | 2.39 (1.53) | <0.0001 | 1.93 (1.60) | 2.06 (1.80) | 0.0163 | 2.17 (1.59) | 2.30 (1.62) | 0.0029 |
| Portions of Veg per day | 2.56 (1.37) | 2.81 (1.47) | <0.0001 | 2.66 (1.47) | 2.89 (1.63) | <0.0001 | 2.08 (1.55) | 2.29 (1.76) | 0.0106 | 2.62 (1.56) | 2.82 (1.71) | <0.0001 |
| Saturated Fat | 11.96 (4.57) | 13.34 (4.86) | <0.0001 | 9.82 (4.28) | 10.46 (4.58) | <0.0001 | 10.57 (5.26) | 10.89 (5.33) | 0.0222 | 9.98 (4.30) | 10.79 (4.82) | <0.0001 |
| IOI | GB | USA | NZ | Significance | |
|---|---|---|---|---|---|
| Change | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | p |
| Cooking related variables | |||||
| Dinner—readymade | −0.36 (0.89) a | −0.22 (0.85) b | −0.09 (0.97) b | −0.14 (0.89) b | 0.000 |
| Dinner—mixed ingred. | −0.03 (0.99) | 0.00 (0.77) | 0.01 (0.93) | 0.05 (0.91) | 0.647 |
| Dinner—fresh | 0.35 (0.85) a | 0.12 (0.75) b | 0.02 (0.95) b | 0.03 (0.81) b | 0.000 |
| Eat Take Away | −0.71 (1.00) a | −0.51 (0.91) b | −0.40 (1.32) b | −1.08 (1.08) c | 0.000 |
| Throw Away—too much | −0.49 (0.98) a | −0.18 (0.74) b | −0.12 (0.94) b | −0.18 (0.88) b | 0.000 |
| Throw away—date | −0.53 (0.95) a | −0.16 (0.71) b | −0.15 (0.86) b | −0.17 (0.82) b | 0.000 |
| Bake | 0.90 (0.98) a | 0.30 (0.87) b | 0.07 (1.01) c | 0.39 (0.95) b | 0.000 |
| COVID-19 related issues | |||||
| Difficulty finding ingredients | 0.96 (0.98) a | 0.72 (0.99) b | 0.44 (1.05) c | 0.41 (0.92) c | 0.000 |
| Bulk buying | 0.61 (1.05) a | 0.40 (1.01) bc | 0.51 (1.12) ab | 0.33 (0.89) c | 0.000 |
| Food Practices (FP) | |||||
| Organisational | 1.75 (2.39) a | 0.87 (1.83) b | 0.59 (1.84) c | 0.78 (1.73) bc | 0.000 |
| Management | 0.05 (2.85) a | 0.42 (2.15) b | 0.69 (2.32) b | 0.10 (2.12) a | 0.000 |
| Overall Emergency Situation FP | 1.79 (4.51) a | 1.29 (3.27) ab | 1.28 (3.51) ab | 0.88 (3.01) b | 0.002 |
| Diet Quality indicators | |||||
| Fruit | 0.10 (1.17) | 0.13 (1.01) | 0.13 (1.24) | 0.13 (0.98) | 0.950 |
| Veg | 0.25 (0.97) | 0.24 (0.92) | 0.19 (1.16) | 0.16 (0.88) | 0.391 |
| Saturated Fat | 1.40 (3.51) a | 0.66 (3.05) b | 0.39 (3.57) b | 0.83 (3.29) b | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murphy, B.; Benson, T.; McCloat, A.; Mooney, E.; Elliott, C.; Dean, M.; Lavelle, F. Changes in Consumers’ Food Practices during the COVID-19 Lockdown, Implications for Diet Quality and the Food System: A Cross-Continental Comparison. Nutrients 2021, 13, 20. https://doi.org/10.3390/nu13010020
Murphy B, Benson T, McCloat A, Mooney E, Elliott C, Dean M, Lavelle F. Changes in Consumers’ Food Practices during the COVID-19 Lockdown, Implications for Diet Quality and the Food System: A Cross-Continental Comparison. Nutrients. 2021; 13(1):20. https://doi.org/10.3390/nu13010020
Chicago/Turabian StyleMurphy, Blain, Tony Benson, Amanda McCloat, Elaine Mooney, Chris Elliott, Moira Dean, and Fiona Lavelle. 2021. "Changes in Consumers’ Food Practices during the COVID-19 Lockdown, Implications for Diet Quality and the Food System: A Cross-Continental Comparison" Nutrients 13, no. 1: 20. https://doi.org/10.3390/nu13010020