Coffee Consumption among Adults in the United States by Demographic Variables and Purchase Location: Analyses of NHANES 2011–2016 Data

Abstract
1. Introduction
2. Materials and Methods
2.1. Dietary Intake Databases
2.2. Participant Characteristics
2.3. Defining Coffee Consumers
2.4. Defining Source Locations for Coffees
2.5. Diet Quality Indicators
2.6. Data Availability and Ethical Approval
2.7. Statistical Analyses
3. Results
3.1. Characteristics of Coffee Consumption among Adults Aged > 20 years
3.2. Coffee Consumers versus Non Consumers
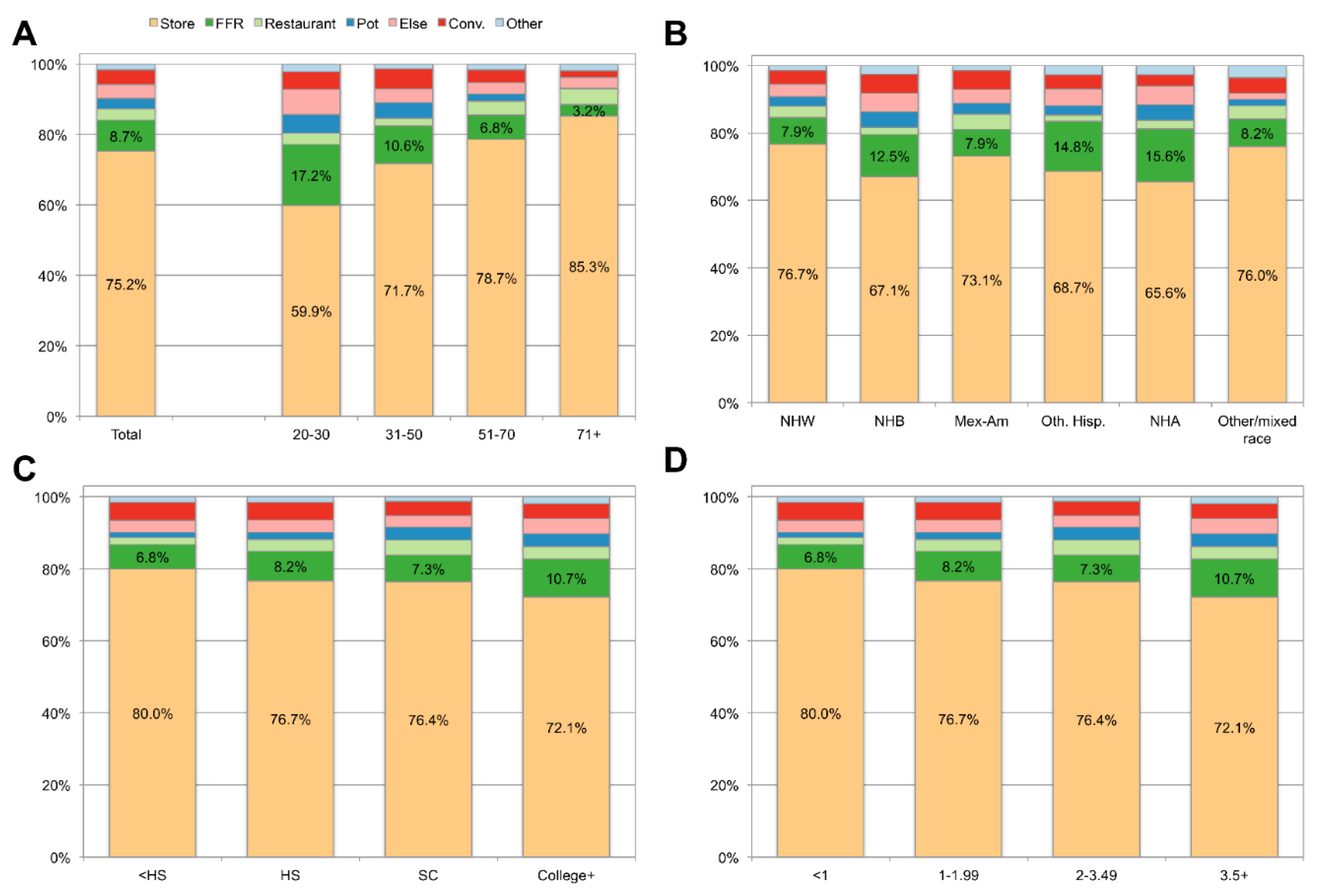
3.3. Coffee Source Locations by Age and Socio-Demographics
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Landais, E.; Moskal, A.; Mullee, A.; Nicolas, G.; Gunter, M.J.; Huybrechts, I.; Overvad, K.; Roswall, N.; Affret, A.; Fagherazzi, G.; et al. Coffee and Tea Consumption and the Contribution of Their Added Ingredients to Total Energy and Nutrient Intakes in 10 European Countries: Benchmark Data from the Late 1990s. Nutrients 2018, 10, 725. [Google Scholar] [CrossRef] [PubMed]
- Loftfield, E.; Freedman, N.D.; Dodd, K.W.; Vogtmann, E.; Xiao, Q.; Sinha, R.; I Graubard, B. Coffee Drinking Is Widespread in the United States, but Usual Intake Varies by Key Demographic and Lifestyle Factors. J. Nutr. 2016, 146, 1762–1768. [Google Scholar] [CrossRef] [PubMed]
- Vieux, F.; Maillot, M.; Rehm, C.D.; Barrios, P.; Drewnowski, A. Trends in tap and bottled water consumption among children and adults in the United States: Analyses of NHANES 2011-16 data. Nutr. J. 2020, 19, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Vieux, F.; Maillot, M.; Rehm, C.; Drewnowski, A. Tea Consumption Patterns in Relation to Diet Quality among Children and Adults in the United States: Analyses of NHANES 2011–2016 Data. Nutrients 2019, 11, 2635. [Google Scholar] [CrossRef]
- Vieux, F.; Maillot, M.; Rehm, C.D.; Drewnowski, A. Flavonoid Intakes in the US Diet Are Linked to Higher Socioeconomic Status and to Tea Consumption: Analyses of NHANES 2011–16 Data. J. Nutr. 2020, 150, 2147–2155. [Google Scholar] [CrossRef]
- Maillot, M.; Rehm, C.D.; Vieux, F.; Rose, C.M.; Drewnowski, A. Beverage consumption patterns among 4-19 y old children in 2009-14 NHANES show that the milk and 100% juice pattern is associated with better diets. Nutr. J. 2018, 17, 54. [Google Scholar] [CrossRef]
- Miranda, A.M.; Steluti, J.; Fisberg, R.M.; Marchioni, D.M.L. Association between Coffee Consumption and Its Polyphenols with Cardiovascular Risk Factors: A Population-Based Study. Nutrients 2017, 9, 276. [Google Scholar] [CrossRef]
- Benson, S.; Unice, K.M.; Glynn, M.E. Hourly and daily intake patterns among U.S. caffeinated beverage consumers based on the National Health and Nutrition Examination Survey (NHANES, 2013–2016). Food Chem. Toxicol. 2019, 125, 271–278. [Google Scholar] [CrossRef]
- Lieberman, H.R.; Agarwal, S.; Fulgoni, V.L. Daily patterns of caffeine intake and the association of intake with multiple sociodemographic and lifestyle factors in US adults Based on the NHANES 2007–2012 Surveys. J. Acad. Nutr. Diet. 2019, 119, 106–114. [Google Scholar] [CrossRef]
- Ahluwalia, N.; Herrick, K. Caffeine intake from food and beverage sources and trends among children and adolescents in the United States: Review of national quantitative studies from 1999 to 2011. Adv. Nutr. 2015, 6, 102–111. [Google Scholar] [CrossRef]
- Drewnowski, A.; Rehm, C. Sources of Caffeine in Diets of US Children and Adults: Trends by Beverage Type and Purchase Location. Nutrients 2016, 8, 154. [Google Scholar] [CrossRef] [PubMed]
- Key Coffee Statistics. Available online: https://myfriendscoffee.com/usa-coffee-statistics/ (accessed on 28 June 2020).
- National Coffee Association the 2020 National Coffee Data Trends Report. Available online: https://www.ncausa.org/Industry-Resources/Market-Research/NCDT (accessed on 16 August 2020).
- National Center for Health Statistics NHANES—About the National Health and Nutrition Examination Survey. Available online: https://www.cdc.gov/nchs/nhanes/about_nhanes.htm (accessed on 22 July 2019).
- US Department of Health and Human Services. Dietary Guidelines for Americans 2015–2020; Skyhorse Publishing Inc.: New York, NY, USA, 2017; ISBN 9780160934650. [Google Scholar]
- Drewnowski, A.; Rehm, C.D. Consumption of added sugars among US children and adults by food purchase location and food source. Am. J. Clin. Nutr. 2014, 100, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Nishi, S.K.; Jessri, M.; L’Abbe, M. Assessing the Dietary Habits of Canadians by Eating Location and Occasion: Findings from the Canadian Community Health Survey, Cycle 2.2. Nutrients 2018, 10, 682. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Rehm, C.D. Sodium Intakes of US Children and Adults from Foods and Beverages by Location of Origin and by Specific Food Source. Nutrients 2013, 5, 1840–1855. [Google Scholar] [CrossRef] [PubMed]
- Shan, Z.; Rehm, C.D.; Rogers, G.; Ruan, M.; Wang, D.D.; Hu, F.B.; Mozaffarian, D.; Zhang, F.F.; Bhupathiraju, S.N. Trends in Dietary Carbohydrate, Protein, and Fat Intake and Diet Quality Among US Adults. 1999-2016. JAMA 2019, 322, 1178–1187. [Google Scholar] [CrossRef]
- Center for Health Statistics. N. NHANES Phone Follow-up Dietary Interviewer Procedures Manual. Available online: https://www.cdc.gov/nchs/data/nhanes/nhanes_09_10/phone_follow_up_dietary_procedures_manual_mar_2010.pdf (accessed on 23 July 2019).
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; A Ingwersen, L.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture. A.R.S. USDA Food and Nutrient Database for Dietary Studies 2013–2014. Food Surveys Research Group Home Page. Available online: https://data.nal.usda.gov/dataset/food-and-nutrient-database-dietary-studies-fndds (accessed on 23 July 2019).
- Bowman, S.A.; Clemens, J.C.; Thoerig, R.C.; Friday, J.E.; Shimizu, M.; Moshfegh, A.J. Food Patterns Equivalents Database 2009–2010: Methodology and User Guide; Food Surveys Research Group, Beltsville Human Nutrition Research Center, Agricultural Research Service, United States Department of Agriculture: Washington, DC, USA, 2013.
- Krebs-Smith, S.M.; Pannucci, T.; Subar, A.F.; I Kirkpatrick, S.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef]
- Vieux, F.; Maillot, M.; Rehm, C.D.; Drewnowski, A. Designing Optimal Breakfast for the United States Using Linear Programming and the NHANES 2011-2014 Database: A Study from the International Breakfast Research Initiative (IBRI). Nutrients 2019, 11, 1374. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. NHANES—NCHS Research Ethics Review Board Approval. Available online: https://www.cdc.gov/nchs/nhanes/irba98.htm (accessed on 23 July 2019).
- Centers for Disease Control and Prevention. NHANES—National Health and Nutrition Examination Survey Homepage. Available online: https://www.cdc.gov/nchs/nhanes/index.htm (accessed on 23 July 2019).
- Williamson, G. The role of polyphenols in modern nutrition. Nutr. Bull. 2017, 42, 226–235. [Google Scholar] [CrossRef]
- Fukushima, Y.; Tashiro, T.; Kumagai, A.; Ohyanagi, H.; Horiuchi, T.; Takizawa, K.; Sugihara, N.; Kishimoto, Y.; Taguchi, C.; Tani, M.; et al. Coffee and beverages are the major contributors to polyphenol consumption from food and beverages in Japanese middle-aged women. J. Nutr. Sci. 2014, 3. [Google Scholar] [CrossRef]
- Popkin, B.; E Armstrong, L.; Bray, G.M.; Caballero, B.; Frei, B.; Willett, W.C. A new proposed guidance system for beverage consumption in the United States. Am. J. Clin. Nutr. 2006, 83, 529–542. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| n | % Consumers | Mean g/day | |
|---|---|---|---|
| Total | 14,865 | 59.5 | 324 |
| Age group | |||
| 20–30 | 2850 | 38.9 | 164 |
| 31–50 | 5071 | 57.8 | 308 |
| 51–70 | 4873 | 69.2 | 430 |
| ≥71 | 2071 | 74.3 | 361 |
| p-value | <0.001 | <0.001 | |
| Gender | |||
| Male | 7223 | 58.7 | 357 |
| Female | 7642 | 60.3 | 293 |
| p-value | 0.18 | <0.001 | |
| Race/ethnicity | |||
| Non-Hispanic white | 5786 | 63.7 | 386 |
| Non-Hispanic black | 3343 | 37.7 | 140 |
| Mexican-American | 2010 | 58.3 | 238 |
| Other Hispanic | 1590 | 64.5 | 248 |
| Non-Hispanic Asian | 1656 | 50.8 | 187 |
| Other/mixed race | 480 | 59.9 | 325 |
| p-value | <0.001 | <0.001 | |
| Education a | |||
| <High school | 3280 | 60.0 | 307 |
| High school | 3257 | 57.7 | 319 |
| Some college | 4533 | 56.8 | 323 |
| ≥College | 3787 | 63.4 | 338 |
| p-value | 0.002 | 0.39 | |
| Family income-to-poverty b | |||
| <1.00 | 3119 | 50.3 | 252 |
| 1.00–1.99 | 3601 | 56.0 | 287 |
| 2.00–3.49 | 2836 | 60.3 | 340 |
| ≥3.5 | 4101 | 64.4 | 364 |
| Missing | 1208 | 59.7 | 316 |
| p-value | <0.001 | <0.001 |
| Mean (95% CI) | ||||
|---|---|---|---|---|
| Model 1 Energy-Adjusted a | Model 2 Multivariable-Adjusted b | |||
| Coffee Consumer (n = 8551) | Non-Consumer (n = 6314) | Coffee Consumer (n = 8551) | Non-Consumer (n = 6314) | |
| Calories, kcal/day | 2065 (2039, 2091) *** | 2118 (2091, 2145) | 2089 (2068, 2111) | 2082 (2061, 2105) |
| Macronutrients | ||||
| Protein, g/day | 81.2 (80.2, 82.2) | 79.9 (78.9, 81) | 81.1 (80.2, 82) | 80 (78.9, 81.1) |
| Carbohydrate, g/day | 235.4 (233.4, 237.4) *** | 244.4 (242.3, 246.6) | 235.7 (234.1, 237.3) *** | 244.1 (241.7, 246.4) |
| Added sugar, teaspoon/day | 14.6 (14.2, 15) *** | 16.5 (16, 17) | 14.8 (14.5, 15.2) *** | 16.1 (15.6, 16.6) |
| Total fat, g/day | 77.2 (76.6, 77.9) *** | 75.5 (74.7, 76.2) | 77 (76.5, 77.6) ** | 75.8 (75, 76.6) |
| PUFA, g/day | 24.9 (24.7, 25.2) *** | 24.3 (24, 24.7) | 24.8 (24.6, 25) * | 24.5 (24.2, 24.8) |
| MUFA, g/day | 27.2 (27, 27.5) *** | 26.4 (26.1, 26.7) | 27.2 (26.9, 27.4) ** | 26.5 (26.2, 26.9) |
| SFA, g/day | 18.2 (18, 18.4) *** | 17.7 (17.5, 18) | 18.2 (18, 18.3) * | 17.8 (17.6, 18.1) |
| Solid fat, g/day | 32.8 (32.3, 33.3) *** | 31.7 (31.1, 32.2) | 32.7 (32.3, 33.2) ** | 31.8 (31.3, 32.3) |
| Other dietary constituents | ||||
| Caffeine, mg/day | 238.8 (230.6, 247.0) *** | 63.9 (57.9, 69.8) *** | 233.0 (226.5, 239.6) *** | 72.3 (66.4, 78.2) |
| Calcium, mg/day | 948.3 (935.4, 961.2) | 941.8 (920, 963.6) | 940.5 (928.1, 953) | 953.2 (933.1, 973.2) |
| Potassium, mg/day | 2787.6 (2753.4, 2821.7) *** | 2466.6 (2429.1, 2504.1) | 2742.2 (2713.9, 2770.5) *** | 2533.2 (2497.4, 2569.1) |
| Magnesium, mg/day | 313.2 (308.3, 318.1) *** | 285.7 (281.2, 290.3) | 309.4 (305, 313.8) *** | 291.3 (286.5, 296) |
| Vitamin C, mg/day | 81.3 (78.5, 84.1) ** | 86.4 (82.4, 90.5) | 80 (77.5, 82.4) *** | 88.4 (84.3, 92.6) |
| Vitamin D, mcg/day | 4.8 (4.6, 4.9) | 4.6 (4.4, 4.8) | 4.7 (4.5, 4.8) | 4.7 (4.5, 4.9) |
| Sodium, mg/day | 3397.3 (3365.5, 3429) | 3436.6 (3397.5, 3475.7) | 3400.7 (3372.1, 3429.3) | 3431.6 (3393.4, 3469.7) |
| Cholesterol, mcg/day | 290.8 (284.5, 297) *** | 273.9 (268.8, 279.1) | 291.1 (285.1, 297) *** | 273.5 (267.9, 279.1) |
| Alcohol, g/day | 9.5 (8.7, 10.3) *** | 7.1 (6.4, 7.8) | 9.6 (8.9, 10.2) *** | 7 (6.2, 7.8) |
| Nutrient density/diet quality | ||||
| NRF9.3 | 436.2 (430.2, 442.1) *** | 414.3 (407.8, 420.7) | 430 (424.7, 435.2) | 423.4 (416.9, 429.9) |
| HEI-2015 | 52.9 (52.3, 53.5) *** | 50.4 (49.8, 50.9) | 52.3 (51.9, 52.8) ** | 51.2 (50.6, 51.8) |
| Mean (95% CI)a | p-Trend | ||||
|---|---|---|---|---|---|
| Non-Consumers (n = 6314) | T1 [1.3–319.2 g/day] (n = 3532) | T2 [319.3–585 g/day] (n = 2834) | T3 [≥585.2 g/day] (n = 2185) | ||
| Calories, kcal/day | 2080 (2057, 2103) | 1997.6 (1967, 2029) | 2103.9 (2063, 2145) | 2172.7 (2134, 2211) | <0.001 |
| Macronutrients | |||||
| Protein, g/day | 80.1 (79, 81.2) | 81.6 (80.2, 83) | 81.2 (79.8, 82.6) | 80.5 (79.3, 81.6) | 0.484 |
| Carbohydrate, g/day | 244.2 (241.8, 246.5) | 238.7 (236.4, 241.1) | 235.6 (232.5, 238.7) | 232.5 (229.9, 235) | <0.001 |
| Added sugar, teaspoon/day | 16.1 (15.6, 16.6) | 14.6 (14, 15.2) | 15 (14.5, 15.5) | 15 (14.5, 15.4) | 0.002 |
| Total fat, g/day | 75.8 (75, 76.6) | 75.9 (75.1, 76.8) | 77 (75.9, 78.1) | 78.1 (77.2, 79.1) | <0.001 |
| PUFA, g/day | 24.5 (24.2, 24.8) | 24.2 (23.8, 24.6) | 24.9 (24.5, 25.2) | 25.4 (25, 25.8) | <0.001 |
| MUFA, g/day | 26.5 (26.2, 26.9) | 26.8 (26.4, 27.1) | 27.1 (26.6, 27.6) | 27.6 (27.2, 28.1) | <0.001 |
| SFA, g/day | 17.8 (17.5, 18.1) | 18.1 (17.8, 18.4) | 18.2 (17.8, 18.6) | 18.2 (17.9, 18.5) | 0.092 |
| Solid fat, g/day | 31.8 (31.3, 32.3) | 31.3 (30.6, 32) | 32.9 (32.3, 33.5) | 34 (33.2, 34.9) | <0.001 |
| Other dietary constituents | |||||
| Caffeine, mg/day | 68.5 (62.7, 74.3) | 125 (118.7, 131.4) | 202.4 (196.4, 208.5) | 380 (365.4, 394.7) | <0.001 |
| Calcium, mg/day | 953.2 (933.2, 973.3) | 942.4 (920, 964.7) | 939.7 (918.5, 961) | 939.4 (915.3, 963.4) | 0.333 |
| Potassium, mg/day | 2529.7 (2493.7, 2565.7) | 2647.7 (2605.8, 2689.6) | 2697.6 (2646.3, 2749) | 2889 (2850.6, 2927.5) | <0.001 |
| Magnesium, mg/day | 291.1 (286.3, 295.8) | 304.5 (297.9, 311.2) | 307.1 (300.3, 313.8) | 317 (311.6, 322.4) | <0.001 |
| Vitamin C, mg/day | 88.6 (84.4, 92.8) | 84.8 (80.9, 88.7) | 81.2 (76.5, 85.9) | 73.6 (69.8, 77.4) | <0.001 |
| Vitamin D, mcg/day | 4.7 (4.5, 4.9) | 4.8 (4.6, 5) | 4.7 (4.4, 5) | 4.5 (4.2, 4.7) | 0.247 |
| Sodium, mg/day | 3432.8 (3394.6, 3470.9) | 3445.2 (3396.1, 3494.2) | 3371.5 (3325.1, 3417.9) | 3383.1 (3325.9, 3440.3) | 0.049 |
| Cholesterol, mcg/day | 273.5 (267.8, 279.1) | 288.6 (279.2, 298) | 292.9 (282.7, 303.2) | 291.8 (281.8, 301.8) | 0.002 |
| Alcohol, g/day | 7 (6.2, 7.8) | 9 (8.2, 9.9) | 9.6 (8.6, 10.6) | 10.1 (8.9, 11.2) | <0.001 |
| Nutrient density/diet quality | |||||
| NRF9.3 | 423.5 (417.1, 430) | 435.6 (428.4, 442.8) | 428.4 (420.4, 436.4) | 425.5 (418.4, 432.6) | 0.596 |
| HEI-2015 | 51.2 (50.6, 51.8) | 52.8 (52, 53.5) | 52.4 (51.7, 53.1) | 51.8 (51.1, 52.6) | 0.076 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rehm, C.D.; Ratliff, J.C.; Riedt, C.S.; Drewnowski, A. Coffee Consumption among Adults in the United States by Demographic Variables and Purchase Location: Analyses of NHANES 2011–2016 Data. Nutrients 2020, 12, 2463. https://doi.org/10.3390/nu12082463
Rehm CD, Ratliff JC, Riedt CS, Drewnowski A. Coffee Consumption among Adults in the United States by Demographic Variables and Purchase Location: Analyses of NHANES 2011–2016 Data. Nutrients. 2020; 12(8):2463. https://doi.org/10.3390/nu12082463
Chicago/Turabian StyleRehm, Colin D., Joseph C. Ratliff, Claudia S. Riedt, and Adam Drewnowski. 2020. "Coffee Consumption among Adults in the United States by Demographic Variables and Purchase Location: Analyses of NHANES 2011–2016 Data" Nutrients 12, no. 8: 2463. https://doi.org/10.3390/nu12082463
APA StyleRehm, C. D., Ratliff, J. C., Riedt, C. S., & Drewnowski, A. (2020). Coffee Consumption among Adults in the United States by Demographic Variables and Purchase Location: Analyses of NHANES 2011–2016 Data. Nutrients, 12(8), 2463. https://doi.org/10.3390/nu12082463