Estimated Intakes of Nutrients and Polyphenols in Participants Completing the MaPLE Randomised Controlled Trial and Its Relevance for the Future Development of Dietary Guidelines for the Older Subjects

 ,
,  ,
,  , ,
, , 
 ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Nutritional and Polyphenol Composition of the Menus
2.3. Evaluation of Actual Energy, Nutrient and Polyphenol Intake
2.4. Statistical Analysis
3. Results
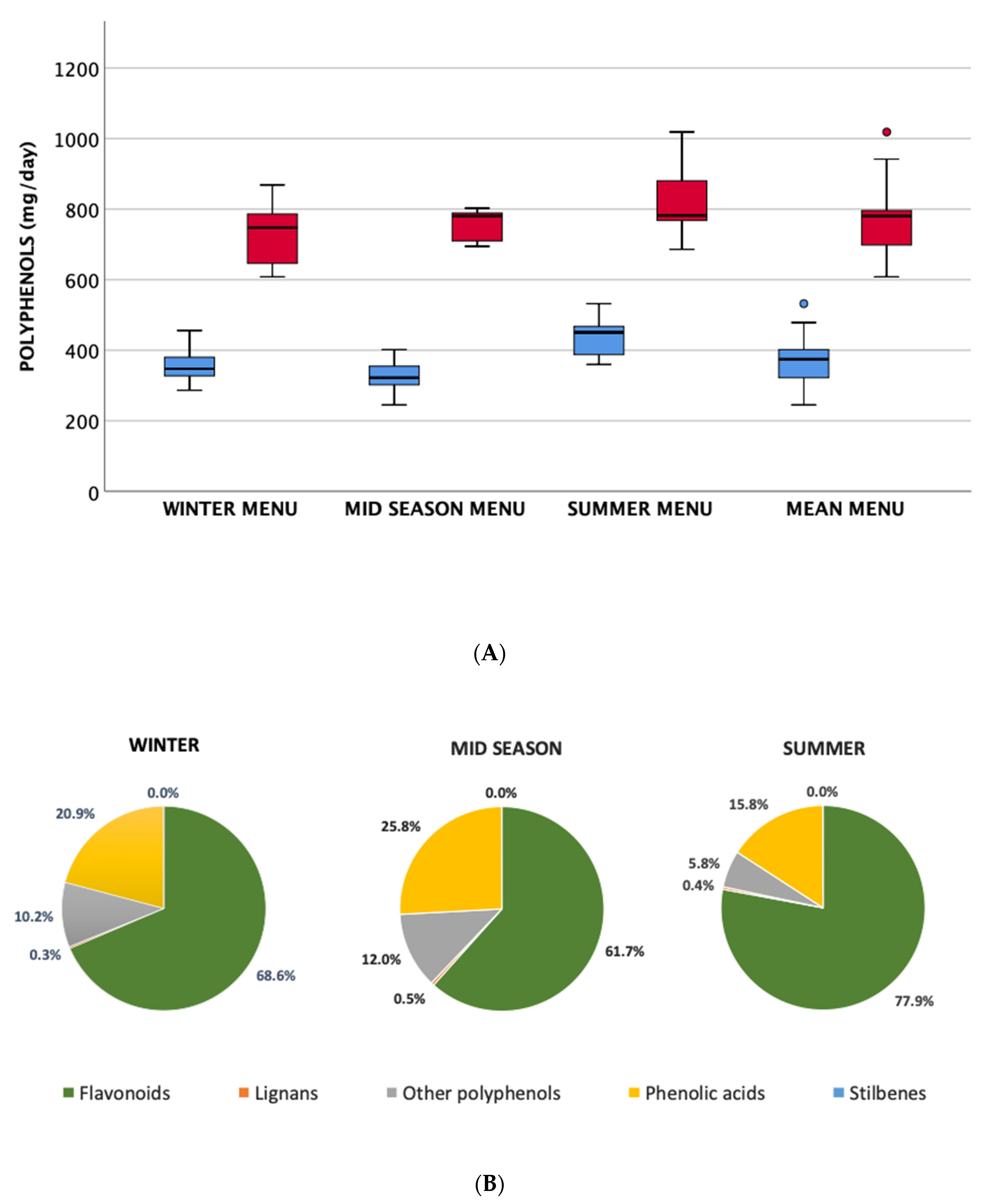
3.1. Nutritional Composition of Menus
3.2. Actual Energy, Nutrient and Polyphenol Intake at Baseline and during the Intervention
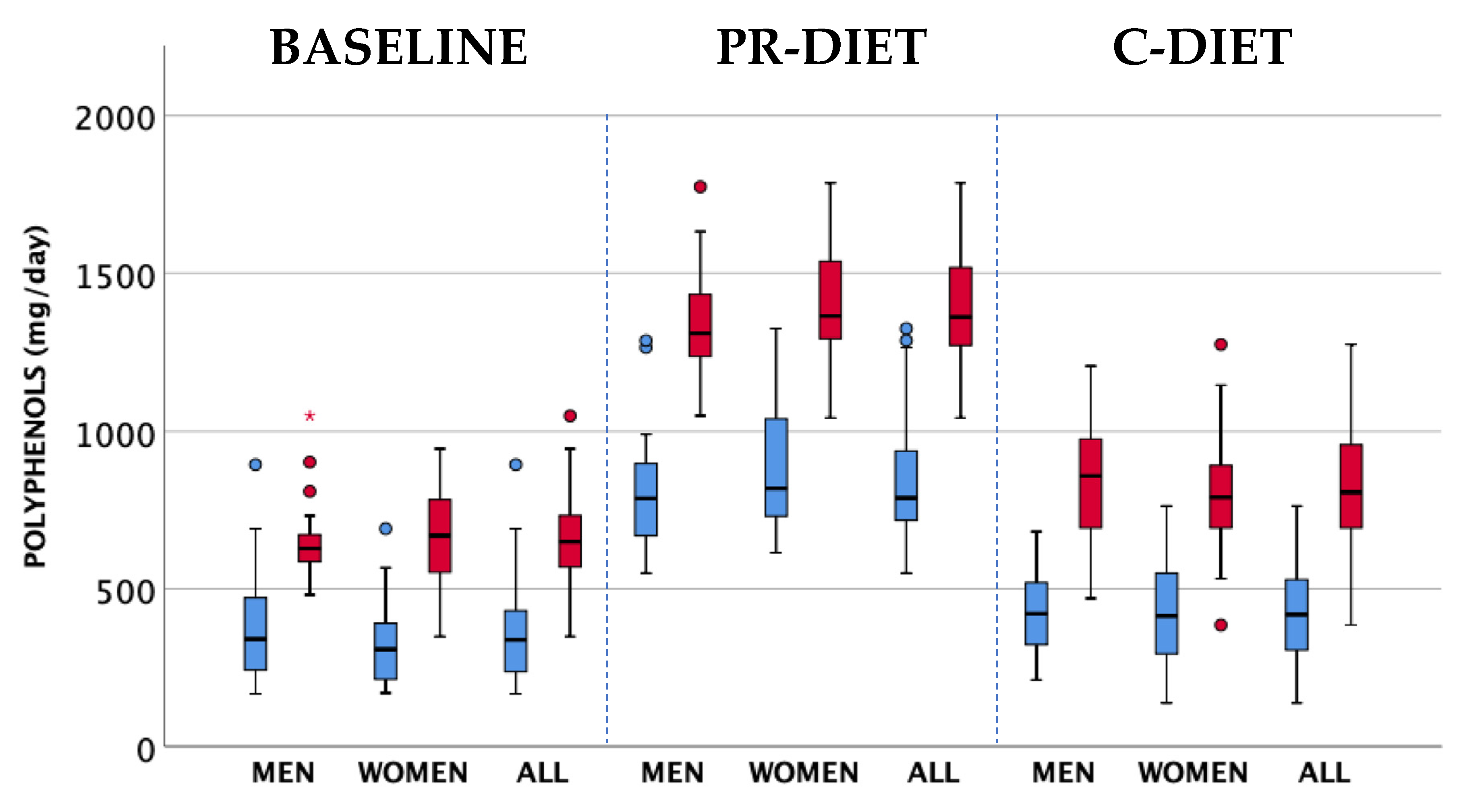
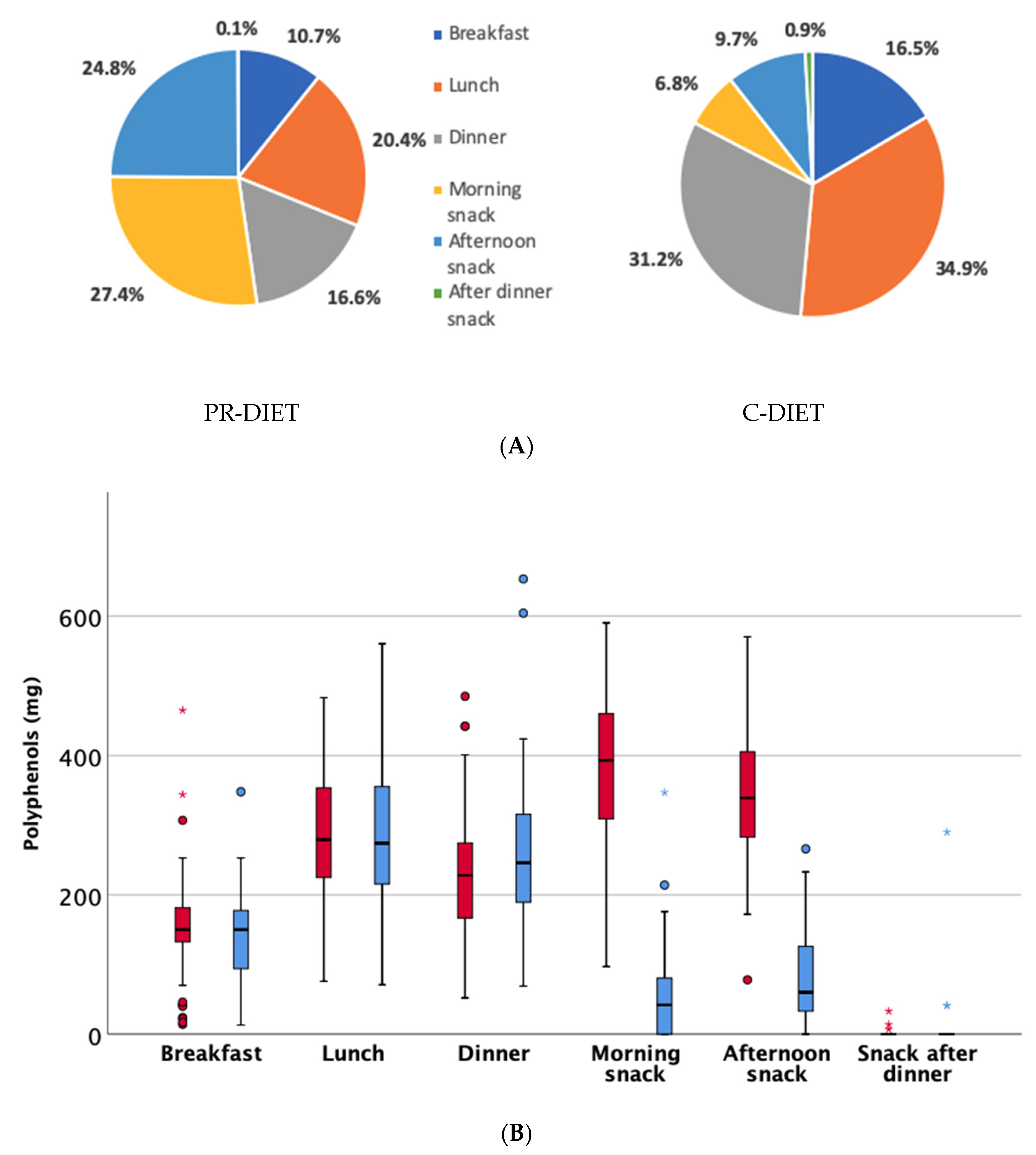
3.3. Polyphenol Intake at Baseline and during Intervention
4. Discussion
5. Conclusions and Perspectives
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z.; et al. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef]
- SINU. LARN—Livelli di Assunzione di Riferimento di Nutrienti ed Energia—IV Revisione; SICS: Milan, Italy, 2014; ISBN 9788890685224. [Google Scholar]
- Amarya, S.; Singh, K.; Sabharwal, M. Changes during aging and their association with malnutrition. J. Clin. Gerontol. Geriatr. 2015, 6, 78–84. [Google Scholar] [CrossRef]
- Volkert, D.; Beck, A.M.; Cederholm, T.; Cruz-Jentoft, A.; Goisser, S.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C.C.; et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin. Nutr. 2019, 38, 10–47. [Google Scholar] [CrossRef] [PubMed]
- Del Bo’, C.; Bernardi, S.; Marino, M.; Porrini, M.; Tucci, M.; Guglielmetti, S.; Cherubini, A.; Carrieri, B.; Kirkup, B.; Kroon, P.; et al. Systematic Review on Polyphenol Intake and Health Outcomes: Is there Sufficient Evidence to Define a Health-Promoting Polyphenol-Rich Dietary Pattern? Nutrients 2019, 11, 1355. [Google Scholar]
- Cherniack, E.P. Polyphenols and Aging; Malavolta, M., Mocchegiani, E., Eds.; Elsevier Inc.: London, UK, 2016; ISBN 9780128018163. [Google Scholar]
- Zamora-Ros, R.; Knaze, V.; Rothwell, J.A.; Hémon, B.; Moskal, A.; Overvad, K.; Tjønneland, A.; Kyrø, C.; Fagherazzi, G.; Boutron-Ruault, M.-C.; et al. Dietary polyphenol intake in Europe: The European Prospective Investigation into Cancer and Nutrition (EPIC) study. Eur. J. Nutr. 2016, 55, 1359–1375. [Google Scholar] [CrossRef] [PubMed]
- Karam, J.; Bibiloni, M.M.; Tur, J.A. Polyphenol estimated intake and dietary sources among older adults from Mallorca Island. PLoS ONE 2018, 13, e0191573. [Google Scholar] [CrossRef] [PubMed]
- Miranda, A.M.; Steluti, J.; Fisberg, R.M.; Marchioni, D.M. Dietary intake and food contributors of polyphenols in adults and elderly adults of Sao Paulo: A population-based study. Br. J. Nutr. 2016, 115, 1061–1070. [Google Scholar] [CrossRef]
- Ziauddeen, N.; Rosi, A.; Del Rio, D.; Amoutzopoulos, B.; Nicholson, S.; Page, P.; Scazzina, F.; Brighenti, F.; Ray, S.; Mena, P. Dietary intake of (poly)phenols in children and adults: Cross-sectional analysis of UK National Diet and Nutrition Survey Rolling Programme (2008–2014). Eur. J. Nutr. 2019, 58, 3183–3198. [Google Scholar] [CrossRef]
- Bell, C.L.; Lee, A.S.W.; Tamura, B.K. Malnutrition in the nursing home. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 17–23. [Google Scholar] [CrossRef]
- Serrano-Urrea, R.; Garcia-Meseguer, M.J. Malnutrition in an Elderly Population without Cognitive Impairment Living in Nursing Homes in Spain: Study of Prevalence Using the Mini Nutritional Assessment Test. Gerontology 2013, 59, 490–498. [Google Scholar] [CrossRef]
- Vandewoude, M.F.J.; van Wijngaarden, J.P.; De Maesschalck, L.; Luiking, Y.C.; Van Gossum, A. The prevalence and health burden of malnutrition in Belgian older people in the community or residing in nursing homes: Results of the NutriAction II study. Aging Clin. Exp. Res. 2019, 31, 175–183. [Google Scholar] [CrossRef] [PubMed]
- FAO. Dietary Assessment. A Resource Guide to Method Selection and Application in Low Resource Settings; Elsevier: Rome, Italy, 2018; ISBN 9780120883936. [Google Scholar]
- Bernardi, S.; Del Bo’, C.; Marino, M.; Gargari, G.; Cherubini, A.; Andrés-Lacueva, C.; Hidalgo-Liberona, N.; Peron, G.; González-Dominguez, R.; Kroon, P.; et al. Polyphenols and Intestinal Permeability: Rationale and Future Perspectives. J. Agric. Food Chem. 2020, 68, 1816–1829. [Google Scholar] [CrossRef] [PubMed]
- Guglielmetti, S.; Bernardi, S.; Del Bo’, C.; Cherubini, A.; Porrini, M.; Gargari, G.; Hidalgo-Liberona, N.; Gonzalez-Dominguez, R.; Peron, G.; Zamora-Ros, R.; et al. Effect of a polyphenol-rich dietary pattern on intestinal permeability and gut and blood microbiomics in older subjects: Study protocol of the MaPLE randomised controlled trial. BMC Geriatr. 2020, 20, 77. [Google Scholar] [CrossRef] [PubMed]
- Singleton, V.L.; Rossi, J.A. Colorimetry of total phenolics with phosphomolybdic-phosphotungstic acid reagents. Am. J. Enol. Vitic. 1965, 16, 144–158. [Google Scholar]
- Zamora-Ros, R.; Rabassa, M.; Cherubini, A.; Urpi-Sarda, M.; Llorach, R.; Bandinelli, S.; Ferrucci, L.; Andres-Lacueva, C. Comparison of 24-h volume and creatinine-corrected total urinary polyphenol as a biomarker of total dietary polyphenols in the Invecchiare InCHIANTI study. Anal. Chim. Acta 2011, 704, 110–115. [Google Scholar] [CrossRef]
- Zamora-Ros, R.; Rabassa, M.; Cherubini, A.; Urpí-Sardà, M.; Bandinelli, S.; Ferrucci, L.; Andres-Lacueva, C. High Concentrations of a Urinary Biomarker of Polyphenol Intake Are Associated with Decreased Mortality in Older Adults. J. Nutr. 2013, 143, 1445–1450. [Google Scholar] [CrossRef]
- Rabassa, M.; Zamora-Ros, R.; Andres-Lacueva, C.; Urpi-Sarda, M.; Bandinelli, S.; Ferrucci, L.; Cherubini, A. Association between both total baseline urinary and dietary polyphenols and substantial physical performance decline risk in older adults: A 9-year follow-up of the InCHIANTI study. J. Nutr. Health Aging 2016, 20, 478–484. [Google Scholar] [CrossRef]
- Rabassa, M.; Cherubini, A.; Zamora-Ros, R.; Urpi-Sarda, M.; Bandinelli, S.; Ferrucci, L.; Andres-Lacueva, C. Low Levels of a Urinary Biomarker of Dietary Polyphenol Are Associated with Substantial Cognitive Decline over a 3-Year Period in Older Adults: The Invecchiare in Chianti Study. J. Am. Geriatr. Soc. 2015, 63, 938–946. [Google Scholar] [CrossRef]
- Nibir, Y.M.; Sumit, A.F.; Akhand, A.A.; Ahsan, N.; Hossain, M.S. Comparative assessment of total polyphenols, antioxidant and antimicrobial activity of different tea varieties of Bangladesh. Asian Pac. J. Trop. Biomed. 2017, 7, 352–357. [Google Scholar] [CrossRef]
- Vrhovsek, U.; Rigo, A.; Tonon, D.; Mattivi, F. Quantitation of Polyphenols in Different Apple Varieties. J. Agric. Food Chem. 2004, 52, 6532–6538. [Google Scholar] [CrossRef]
- Cleverdon, R.; Elhalaby, Y.; McAlpine, M.; Gittings, W.; Ward, W. Total Polyphenol Content and Antioxidant Capacity of Tea Bags: Comparison of Black, Green, Red Rooibos, Chamomile and Peppermint over Different Steep Times. Beverages 2018, 4, 15. [Google Scholar] [CrossRef]
- Ministero della Salute. Linee di Indirizzo Nazionale per la Ristorazione Ospedaliera e Assistenziale; Ministero della salute: Rome, Italy, 2011.
- Trang, S.; Fraser, J.; Wilkinson, L.; Steckham, K.; Oliphant, H.; Fletcher, H.; Tzianetas, R.; Arcand, J. A Multi-Center Assessment of Nutrient Levels and Foods Provided by Hospital Patient Menus. Nutrients 2015, 7, 9256–9264. [Google Scholar] [CrossRef]
- Thibault, R.; Chikhi, M.; Clerc, A.; Darmon, P.; Chopard, P.; Genton, L.; Kossovsky, M.P.; Pichard, C. Assessment of food intake in hospitalised patients: A 10-year comparative study of a prospective hospital survey. Clin. Nutr. 2011, 30, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Coulston, A.M.; Mandelbaum, D.; Reaven, G.M. Dietary management of nursing home residents with non-insulin-dependent diabetes mellitus. Am. J. Clin. Nutr. 1990, 51, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez Rejón, A.I.; Ruiz López, M.D.; Malafarina, V.; Puerta, A.; Zuñiga, A.; Artacho, R. Menus offered in long-term care homes: Quality of meal service and nutritional analysis. Nutr. Hosp. 2017, 34, 584. [Google Scholar] [CrossRef] [PubMed]
- Vucea, V.; Keller, H.H.; Morrison, J.M.; Duncan, A.M.; Duizer, L.M.; Carrier, N.; Lengyel, C.O.; Slaughter, S.E. Nutritional quality of regular and pureed menus in Canadian long term care homes: An analysis of the Making the Most of Mealtimes (M3) project. BMC Nutr. 2017, 3, 80. [Google Scholar] [CrossRef]
- World Health Organization. Food Based Dietary Guidelines in the WHO European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 2003. [Google Scholar]
- Bartali, B.; Salvini, S.; Turrini, A.; Lauretani, F.; Russo, C.R.; Corsi, A.M.; Bandinelli, S.; D’Amicis, A.; Palli, D.; Guralnik, J.M.; et al. Age and Disability Affect Dietary Intake. J. Nutr. 2003, 133, 2868–2873. [Google Scholar] [CrossRef]
- Bartali, B.; Frongillo, E.A.; Bandinelli, S.; Lauretani, F.; Semba, R.D.; Fried, L.P.; Ferrucci, L. Low Nutrient Intake Is an Essential Component of Frailty in Older Persons. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 589–593. [Google Scholar] [CrossRef]
- Taguchi, C.; Kishimoto, Y.; Takeuchi, I.; Tanaka, M.; Iwashima, T.; Fukushima, Y.; Kondo, K. Estimated Dietary Polyphenol Intake and Its Seasonal Variations among Japanese University Students. J. Nutr. Sci. Vitaminol. (Tokyo) 2019, 65, 192–195. [Google Scholar] [CrossRef]
- Kent, K.; Charlton, K.E.; Lee, S.; Mond, J.; Russell, J.; Mitchell, P.; Flood, V.M. Dietary flavonoid intake in older adults: How many days of dietary assessment are required and what is the impact of seasonality? Nutr. J. 2018, 17, 7. [Google Scholar] [CrossRef]
- Taguchi, C.; Fukushima, Y.; Kishimoto, Y.; Saita, E.; Suzuki-Sugihara, N.; Yoshida, D.; Kondo, K. Polyphenol Intake from Beverages in Japan over an 18-Year Period (1996–2013): Trends by Year, Age, Gender and Season. J. Nutr. Sci. Vitaminol. (Tokyo) 2015, 61, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Tatsumi, Y.; Ishihara, J.; Morimoto, A.; Ohno, Y.; Watanabe, S. Seasonal differences in total antioxidant capacity intake from foods consumed by a Japanese population. Eur. J. Clin. Nutr. 2014, 68, 799–803. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Tresserra-Rimbau, A.; Medina-Remón, A.; Pérez-Jiménez, J.; Martínez-González, M.A.; Covas, M.I.; Corella, D.; Salas-Salvadó, J.; Gómez-Gracia, E.; Lapetra, J.; Arós, F.; et al. Dietary intake and major food sources of polyphenols in a Spanish population at high cardiovascular risk: The PREDIMED study. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Stepaniak, U.; Topor-Mądry, R.; Szafraniec, K.; Pająk, A. Estimated dietary intake and major food sources of polyphenols in the Polish arm of the HAPIEE study. Nutrition 2014, 30, 1398–1403. [Google Scholar] [CrossRef]
- Tresserra-Rimbau, A.; Guasch-Ferré, M.; Salas-Salvadó, J.; Toledo, E.; Corella, D.; Castañer, O.; Guo, X.; Gómez-Gracia, E.; Lapetra, J.; Arós, F.; et al. Intake of Total Polyphenols and Some Classes of Polyphenols Is Inversely Associated with Diabetes in Elderly People at High Cardiovascular Disease Risk. J. Nutr. 2015, 146, 767–777. [Google Scholar]
- Peron, G.; Hidalgo-Liberona, N.; González-Domínguez, R.; Garcia-Aloy, M.; Guglielmetti, S.; Bernardi, S.; Kirkup, B.; Kroon, P.A.; Cherubini, A.; Riso, P.; et al. Exploring the Molecular Pathways Behind the Effects of Nutrients and Dietary Polyphenols on Gut Microbiota and Intestinal Permeability: A Perspective on the Potential of Metabolomics and Future Clinical Applications. J. Agric. Food Chem. 2020, 68, 1780–1789. [Google Scholar] [CrossRef]
- Amiot, M.J.; Riva, C.; Vinet, A. Effects of dietary polyphenols on metabolic syndrome features in humans: A systematic review. Obes. Rev. 2016, 17, 573–586. [Google Scholar] [CrossRef]
- Cao, H.; Ou, J.; Chen, L.; Zhang, Y.; Szkudelski, T.; Delmas, D.; Daglia, M.; Xiao, J. Dietary polyphenols and type 2 diabetes: Human Study and Clinical Trial. Crit. Rev. Food Sci. Nutr. 2019, 59, 3371–3379. [Google Scholar] [CrossRef]
- Kim, Y.; Keogh, J.; Clifton, P. Polyphenols and Glycemic Control. Nutrients 2016, 8, 17. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| TPC | TP | Flavonoids | Phenolic Acids | Stilbenes | Lignans | Other | |
|---|---|---|---|---|---|---|---|
| Blood orange juice | 178 | 63.4 | 42.0 | 21.4 | - | - | - |
| Blood orange fruit | 178 | 34.8 | 23.1 | 11.8 | - | - | - |
| Renetta apple | 296 | 225.9 | 201.2 | 24.7 | - | 0.01 | - |
| Renetta apple purée + | 167 | 150.6 | 134.1 | 16.5 | - | 0.00 | - |
| Whole blueberry § | 291 | 259.5 | 165.1 | 94.5 | - | - | - |
| Blueberry purée ✥ | 259 | 199.0 | 163.6 | 35.4 | - | 0.0 | 0.02 |
| Pomegranate juice | 189 | 135.5 | 55.1 | 80.3 | - | - | - |
| Green tea * | 146 | 129.2 | 116.2 | 13.0 | - | 0.08 | - |
| Cocoa powder ° | 234 | 92.2 | 90.5 | 1.7 | - | 0.00 | 0.01 |
| Chocolate callets | 337 | 167.8 | 165.4 | 2.4 | 0.01 | - | - |
| Nutritional Factor | Winter Menu | Mid-Season Menu | Summer Menu | Mean Menu |
|---|---|---|---|---|
| Energy (kcal) | 1889 ± 102 a | 2012 ± 176 a,b | 2028 ± 66 b | 1976 ± 133 |
| Total CHO (% of energy) | 47.4 ± 3.2 | 46.4 ± 4.7 | 46.5 ± 3.0 | 46.8 ± 3.5 |
| Simple CHO (% of energy) | 20.6 ± 2.2 | 19.8 ± 0.6 | 20.3 ± 1.4 | 20.2 ± 1.5 |
| Total protein (% of energy) | 18.7 ± 2.5 | 20.0 ± 2.3 | 19.6 ± 2.7 | 19.4 ± 2.5 |
| Animal protein (% of energy) | 11.1 ± 2.8 | 13.4 ± 2.8 | 12.8 ± 2.5 | 12.4 ± 0.3 |
| Plant protein (% of energy) | 6.2 ± 0.9 | 6.2 ± 1.1 | 6.4 ± 0.8 | 6.3 ± 0.1 |
| Total Lipids (% of energy) | 34.1 ± 4.2 | 33.7 ± 4.1 | 34.0 ± 4.6 | 33.9 ± 4.1 |
| SFA (% of energy) | 8.7 ± 1.3 | 8.9 ± 2.0 | 8.6 ± 1.8 | 8.7 ± 1.6 |
| MUFA (% of energy) | 17.9 ± 3.3 | 16.9 ± 2.4 | 17.7 ± 2.2 | 17.5 ± 2.6 |
| PUFA (% of energy) | 3.7 ± 0.8 | 3.8 ± 0.7 | 3.9 ± 1.4 | 3.8 ± 1.0 |
| ω-3 (% of energy) | 0.7 ± 0.4 | 0.7 ± 0.4 | 0.7 ± 0.4 | 0.7 ± 0.4 |
| ω-6 (% of energy) | 3.0 ± 0.9 | 3.0 ± 0.8 | 3.2 ± 1.3 | 3.0 ± 1.0 |
| Total Fibre (g/1000 Kcal) | 12.2 ± 2.1 | 11.6 ± 2.4 | 12.3 ± 1.7 | 12.0 ± 2.0 |
| Cholesterol (mg) | 264 ± 91 | 358 ± 134 | 288 ± 123 | 303 ± 118 |
| Total proteins (g) | 88.1 ± 14.3 | 100.9 ± 19.6 | 98.8 ± 11.3 | 95.9 ± 15.7 |
| Animal protein (g) | 56.0 ± 13.8 | 68.3 ± 20.5 | 64.8 ± 10.9 | 63.0 ± 15.7 |
| Plant protein (g) | 30.6 ± 4.1 | 30.9 ± 4.2 | 32.6 ± 4.0 | 31.4 ± 4.0 |
| Total lipids (g) | 71.2 ± 7.8 | 75.3 ± 12.5 | 76.5 ± 12.3 | 74.3 ± 10.7 |
| SFA (g) | 18.3 ± 3.3 | 19.8 ± 4.6 | 19.4 ± 4.4 | 19.1 ± 4.0 |
| MUFA (g) | 37.3 ± 5.8 | 38.0 ± 7.1 | 40.1 ± 5.8 | 38.5 ± 6.0 |
| PUFA (g) | 7.7 ± 1.6 | 8.5 ± 2.1 | 8.7 ± 3.4 | 8.3 ± 2.4 |
| Total ω-3 (g) | 1.4 ± 0.8 | 1.5 ± 0.9 | 1.6 ± 0.9 | 1.5 ± 0.9 |
| Total ω-6 (g) | 6.2 ± 1.8 | 6.7 ± 2.1 | 7.1 ± 3.0 | 6.7 ± 3.0 |
| Fibre (g/day) | 22.9 ± 4.2 | 23.2 ± 4.4 | 24.8 ± 2.9 | 23.6 ± 3.8 |
| Calcium (mg) | 643 ± 254 | 666 ± 175 | 638 ± 112 | 649 ± 180 |
| Iron (mg) | 11.9 ± 2.0 | 14.2 ± 2.9 | 12.1 ± 1.0 | 12.7 ± 2.3 |
| Vitamin B12 (mcg) | 4.8 ± 2.2 | 5.3 ± 2.3 | 6.3 ± 5.1 | 5.5 ± 3.4 |
| Vitamin C (mg) | 225 ± 33 | 233 ± 28 | 242 ± 45 | 233 ± 35 |
| Vitamin E (mg) | 13.7 ± 1.9 | 15 ± 3.2 | 15.5 ± 2.4 | 14.8 ± 2.6 |
| Vitamin B1 (mg) | 1.4 ± 0.4 | 1.6 ± 0.4 | 1.5 ± 0.4 | 1.5 ± 0.4 |
| Folates (mcg) | 342 ± 78 | 377 ± 138 | 340 ± 70 | 353 ± 97 |
| Vitamin B6 (mg) | 2.3 ± 0.6 | 2.7 ± 0.7 | 2.5 ± 0.4 | 2.5 ± 0.6 |
| Variables | All (n = 51) | Women (n = 29) | Men (n = 22) | p-Value † |
|---|---|---|---|---|
| Energy (kcal) | 1582 ± 108 | 1569 ± 110 | 1599 ± 105 | 0.318 |
| Total CHO (% of energy) | 50.0 ± 2.7 | 50.0 ± 2.7 | 49.8 ± 2.7 | 0.641 |
| Simple CHO (% of energy) | 20.4 ± 3.1 | 20.3 ± 3.3 | 20.5 ± 3.0 | 0.939 |
| Proteins (% of energy) | 17.8 ± 0.8 | 18.0 ± 0.8 | 17.7 ± 0.9 | 0.216 |
| Animal proteins (% of energy) | 12.1± 1.1 | 12.2 ± 1.0 | 11.8 ± 1.1 | 0.262 |
| Plant proteins (% of energy) | 5.7 ± 0.6 | 5.7 ± 0.6 | 5.7 ± 0.6 | 0.864 |
| Total lipids (% of energy) | 32.1 ± 2.3 | 31.9 ± 2.2 | 32.4 ± 2.5 | 0.441 |
| SFA (% of energy) | 8.6 ± 1.5 | 8.6 ± 1.4 | 8.7 ± 1.7 | 0.655 |
| MUFA (% of energy) | 16.3 ± 1.3 | 16.3 ± 1.1 | 16.4 ± 1.6 | 0.834 |
| PUFA (% of energy) | 3.2 ± 0.5 | 3.3 ± 0.6 | 3.2 ± 0.4 | 0.435 |
| ω-3 (% of energy) | 0.6 ± 0.2 | 0.6 ± 0.1 | 0.6 ± 0.2 | 0.753 |
| ω-6 (% of energy) | 2.5 ± 0.4 | 2.6 ± 0.5 | 2.5 ± 0.2 | 0.341 |
| Total Fibre (g/1000 kcal) | 11.2 ± 1.2 | 11.3 ± 1.1 | 11.1 ± 1.3 | 0.458 |
| Cholesterol (mg) | 207.7 ± 30.3 | 204.3 ± 29.9 | 212.2 ± 30.9 | 0.682 |
| Total CHO (g) | 210.7 ± 21.5 | 209.6 ± 22.8 | 212.2 ± 20.1 | 0.864 |
| Simple CHO (g) | 81.0 ± 15.2 | 80.8 ± 15.4 | 81.3 ± 15.2 | 0.954 |
| Proteins (g) | 70.3 ± 4.0 | 70.2 ± 4.0 | 70.4 ± 4.0 | 0.849 |
| Animal proteins (g) | 47.6 ± 3.9 | 47.9 ± 3.7 | 47.2 ± 4.2 | 0.536 |
| Plant proteins (g) | 22.4 ± 2.7 | 22.2 ± 2.7 | 22.7 ± 2.8 | 0.601 |
| Total lipids (g) | 56.2 ± 4.9 | 55.2 ± 3.8 | 57.5 ± 5.8 | 0.192 |
| SFA (g) | 15.2 ± 3.0 | 14.9 ± 2.7 | 15.5 ± 3.3 | 0.447 |
| MUFA (g) | 28.7 ± 2.4 | 28.3 ± 1.2 | 29.1 ± 3.4 | 0.575 |
| PUFA (g) | 5.7 ± 0.7 | 5.7 ± 0.7 | 5.7 ± 0.8 | 0.371 |
| Total ω-3 (g) | 1.1 ± 0.3 | 1.1 ± 0.1 | 1.1 ± 0.4 | 0.600 |
| Total ω-6 (g) | 4.5 ± 0.6 | 4.5 ± 0.6 | 4.4 ± 0.5 | 0.274 |
| Fibre (g/day) | 17.8 ± 2.4 | 17.8 ± 2.2 | 17.8 ± 2.6 | 0.932 |
| Calcium (mg) | 804 ± 136 | 808 ± 128 | 799 ± 147 | 0.761 |
| Iron (mg) | 9.4 ± 0.9 | 9.4 ± 0.7 | 9.4 ± 1.0 | 0.879 |
| Vitamin B12 (µg) | 4.2 ± 1.0 | 4.2 ± 0.4 | 4.3 ± 1.5 | 0.394 |
| Vitamin C (mg) | 111.8 ± 56.1 | 115.1 ± 45.2 | 107.4 ± 68.8 | 0.464 |
| Vitamin E (mg) | 11.4 ± 2.9 | 11.5 ± 1.3 | 11.2 ± 4.1 | 0.327 |
| Vitamin B1 (mg) | 0.8 ± 0.2 | 0.8 ± 0.1 | 0.7 ± 0.2 | 0.156 |
| Folates (µg) | 302 ± 73 | 311 ± 54 | 289 ± 93 | 0.536 |
| Vitamin B6 (mg) | 1.5 ± 0.3 | 1.5 ± 0.2 | 1.4 ± 0.3 | 0.588 |
| Flavonoids (mg) | 181.1 ± 137.5 | 174.4 ± 123.7 | 190.8 ± 157.8 | 0.984 |
| Phenolic acids (mg) | 130.9 ± 36.0 | 126.6 ± 28.6 | 137.1 ± 44.5 | 0.598 |
| Stilbenes (mg) | 0.04 ± 0.06 | 0.04 ± 0.06 | 0.04 ± 0.07 | 0.542 |
| Lignans (mg) | 0.8 ± 0.2 | 0.8 ± 0.2 | 0.8 ± 0.2 | 0.737 |
| Other polyphenols (mg) | 27.8 ± 4.3 | 28.0 ± 3.7 | 27.6 ± 5.0 | 0.723 |
| Title 1 | Flavonoids | Phenolic Acids | Stilbenes | Lignans | Other Polyphenols |
|---|---|---|---|---|---|
| PR-diet | |||||
| All | 634.3 ± 171.8 | 198.1 ± 52.2 | 0.2 ± 0.4 | 0.8 ± 0.3 | 16.4 ± 5.3 |
| Men | 594.6 ± 152.2 | 201.1 ± 74.3 | 0.4 ± 0.6 | 0.7 ± 0.3 | 16.7 ± 6.3 |
| Women | 662.1 ± 163.5 | 195.9 ± 42.0 | 0.1 ± 0.2 | 0.8 ± 0.3 | 16.2 ± 5.3 |
| p value # | 0.098 | 0.810 | 0.108 | 0.206 | 0.827 |
| C-diet | |||||
| All | 273.8 ± 119.8 | 128.2 ± 60.9 | 0.3 ± 0.5 | 0.9 ± 0.4 | 17.0 ± 5.4 |
| Men | 260.9 ± 109.6 | 128.8 ± 57.8 | 0.4 ± 0.4 | 0.9 ± 0.4 | 15.9 ± 5.7 |
| Women | 282.9 ± 125.6 | 127.8 ± 63.0 | 0.2 ± 0.5 | 0.9 ± 0.4 | 17.8 ± 4.9 |
| p value # | 0.453 | 0.271 | 0.033 | 0.745 | 0.271 |
| p value † | <0.0001 | <0.0001 | 0.386 | 0.303 | 0.164 |
| p value ¥ | <0.0001 | 0.001 | 0.575 | 0.068 | 0.807 |
| p value § | <0.0001 | <0.0001 | 0.348 | 0.060 | 0.331 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martini, D.; Bernardi, S.; Del Bo’, C.; Hidalgo Liberona, N.; Zamora-Ros, R.; Tucci, M.; Cherubini, A.; Porrini, M.; Gargari, G.; González-Domínguez, R.; et al. Estimated Intakes of Nutrients and Polyphenols in Participants Completing the MaPLE Randomised Controlled Trial and Its Relevance for the Future Development of Dietary Guidelines for the Older Subjects. Nutrients 2020, 12, 2458. https://doi.org/10.3390/nu12082458
Martini D, Bernardi S, Del Bo’ C, Hidalgo Liberona N, Zamora-Ros R, Tucci M, Cherubini A, Porrini M, Gargari G, González-Domínguez R, et al. Estimated Intakes of Nutrients and Polyphenols in Participants Completing the MaPLE Randomised Controlled Trial and Its Relevance for the Future Development of Dietary Guidelines for the Older Subjects. Nutrients. 2020; 12(8):2458. https://doi.org/10.3390/nu12082458
Chicago/Turabian StyleMartini, Daniela, Stefano Bernardi, Cristian Del Bo’, Nicole Hidalgo Liberona, Raul Zamora-Ros, Massimiliano Tucci, Antonio Cherubini, Marisa Porrini, Giorgio Gargari, Raúl González-Domínguez, and et al. 2020. "Estimated Intakes of Nutrients and Polyphenols in Participants Completing the MaPLE Randomised Controlled Trial and Its Relevance for the Future Development of Dietary Guidelines for the Older Subjects" Nutrients 12, no. 8: 2458. https://doi.org/10.3390/nu12082458
APA StyleMartini, D., Bernardi, S., Del Bo’, C., Hidalgo Liberona, N., Zamora-Ros, R., Tucci, M., Cherubini, A., Porrini, M., Gargari, G., González-Domínguez, R., Peron, G., Kirkup, B., Kroon, P. A., Andres-Lacueva, C., Guglielmetti, S., & Riso, P. (2020). Estimated Intakes of Nutrients and Polyphenols in Participants Completing the MaPLE Randomised Controlled Trial and Its Relevance for the Future Development of Dietary Guidelines for the Older Subjects. Nutrients, 12(8), 2458. https://doi.org/10.3390/nu12082458