Effects of Lifestyle Modification Interventions to Prevent and Manage Child and Adolescent Obesity: A Systematic Review and Meta-Analysis

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Objectives
2.2. Types of Studies and Participants
2.3. Types of Interventions
- Dietary interventions including nutrition education and provision of balanced meals;
- Physical activity including promotion of physical exercise and reduction in sedentary behaviors;
- Behavioral therapy;
- Combination of any of these interventions.
2.4. Types of Outcome Measures
2.5. Search Methods
2.6. Data Collection and Analysis
2.7. Quality Assessment
3. Results
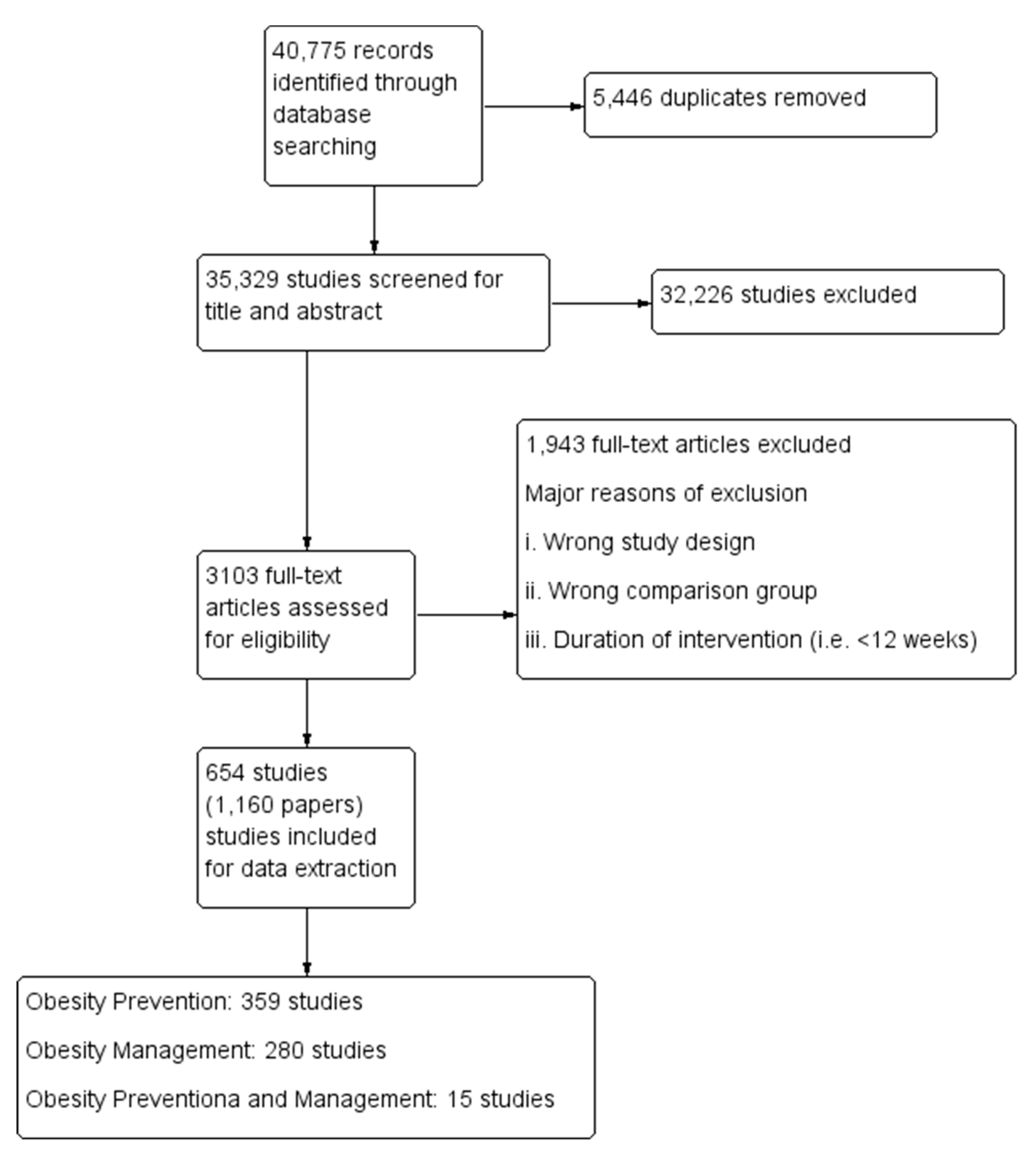
3.1. Results of the Search
3.2. Description of Included Studies
- Diet only interventions—34 studies;
- Exercise only interventions—57 studies;
- Behavioral therapy only intervention—89 studies;
- Diet and Exercise interventions—99 studies;
- Diet and Behavioral therapy interventions—7 studies;
- Exercise and behavioral therapy interventions—47 studies;
- Diet, exercise and behavioral therapy interventions—26 studies.
- Diet only interventions—17 studies;
- Exercise only interventions—59 studies;
- Behavioral therapy only intervention—63 studies;
- Diet and Exercise interventions—57 studies;
- Diet and Behavioral therapy interventions—5 studies;
- Exercise and behavioral therapy interventions—30 studies;
- Diet, exercise and behavioral therapy interventions—49 studies.
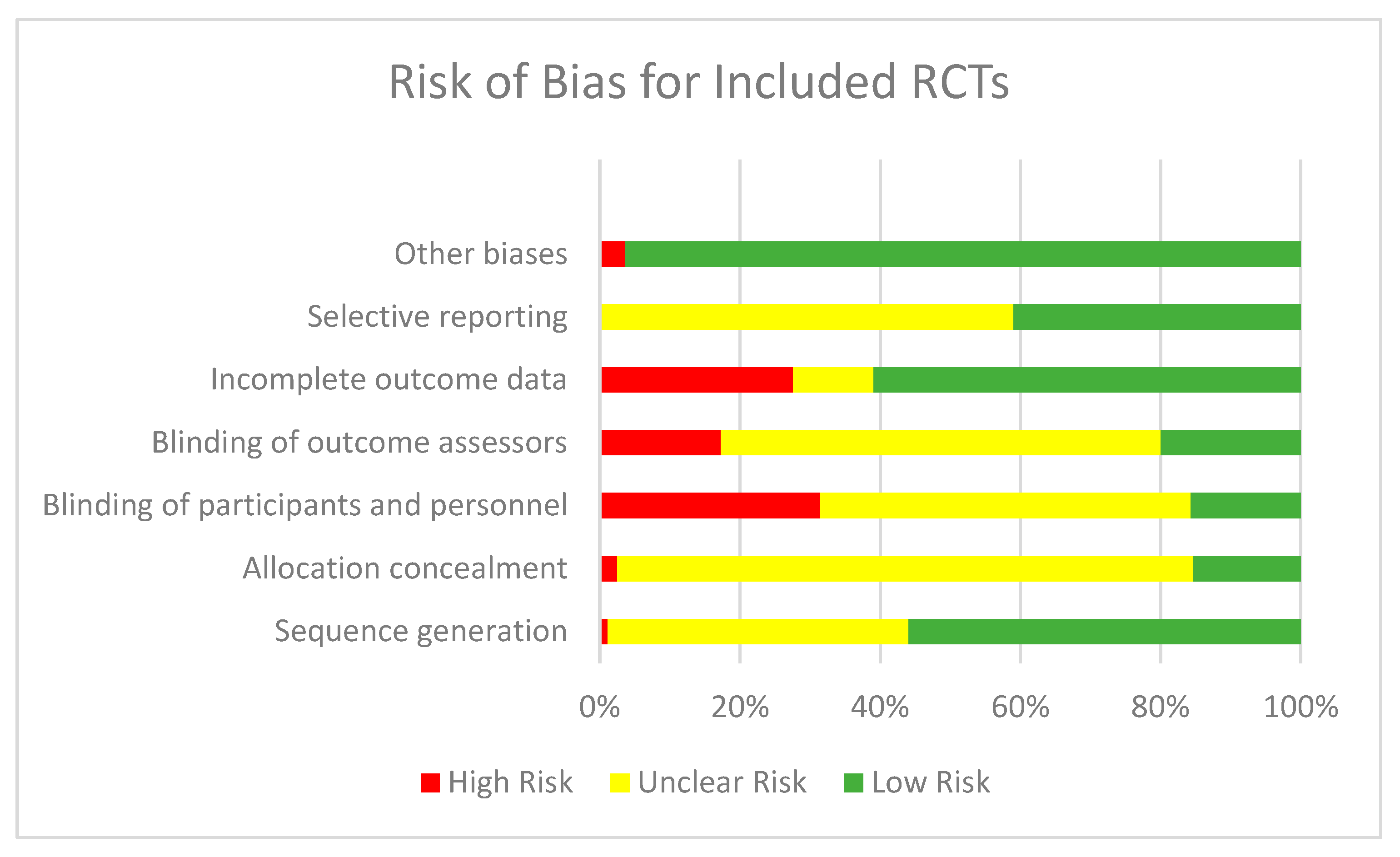
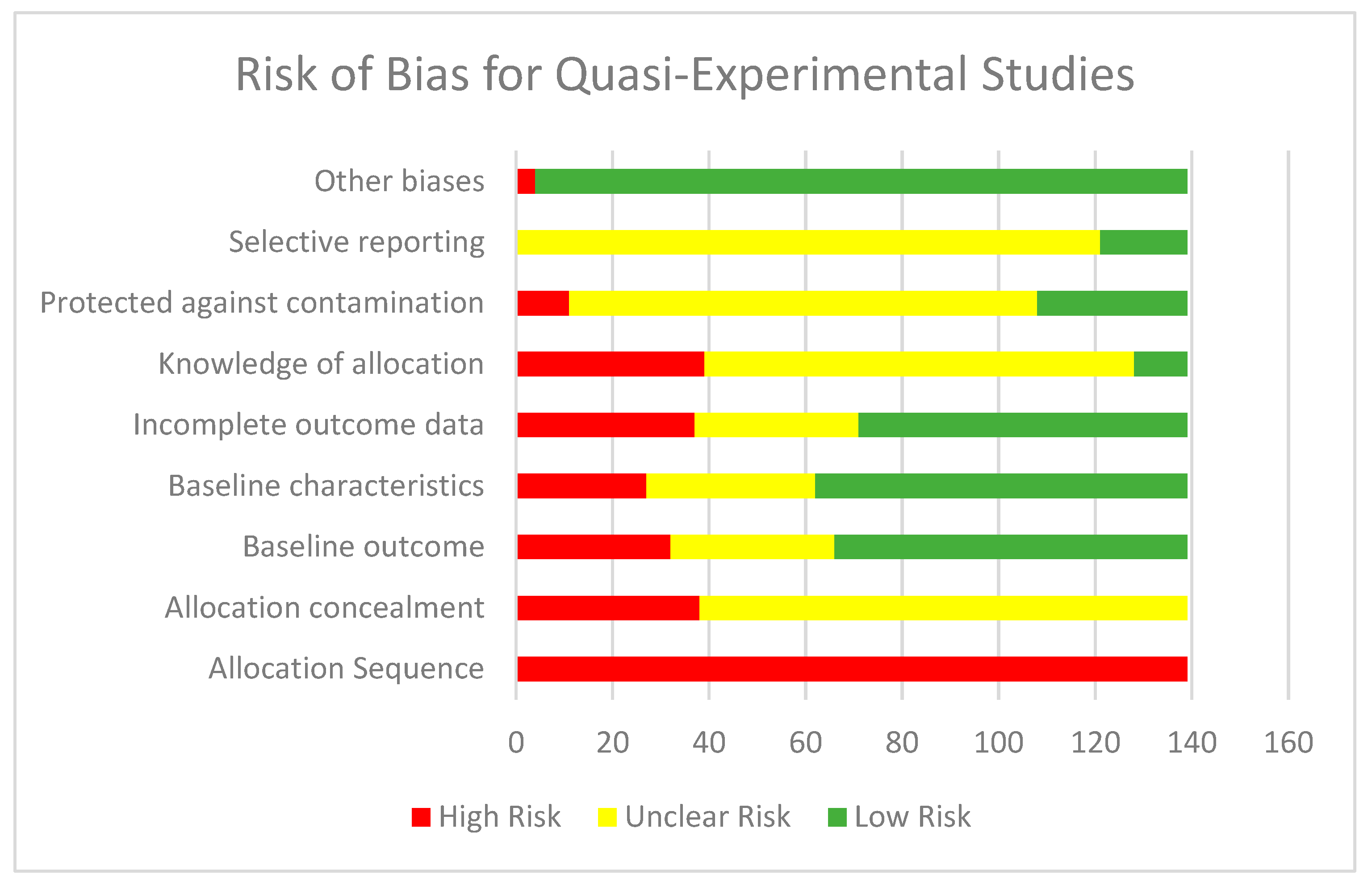
3.3. Risk of Bias
3.3.1. For Randomized Control Trials
3.3.2. For Quasi-Experimental Studies
3.4. PROGRESS Findings
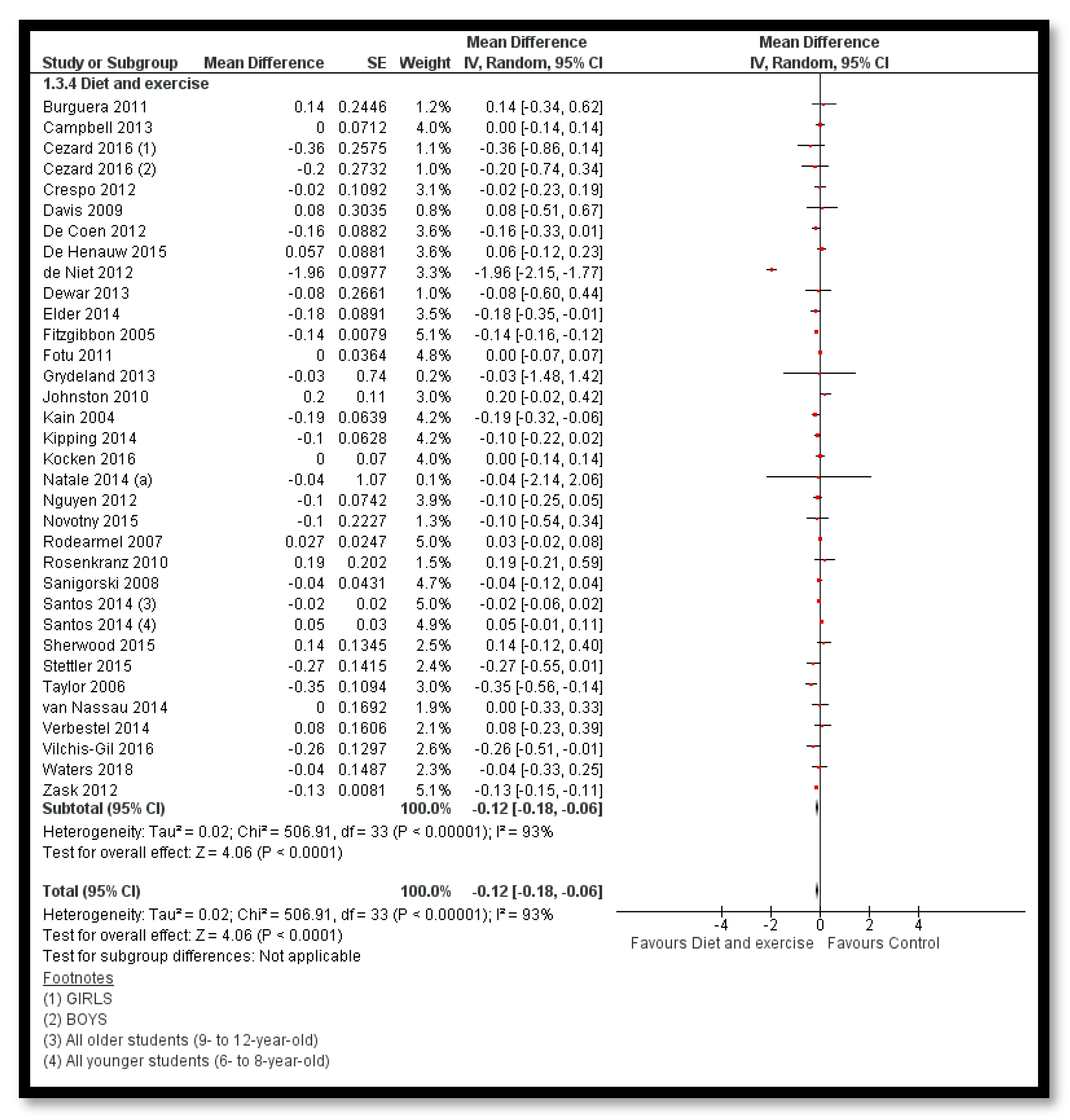
3.5. Effects of Interventions
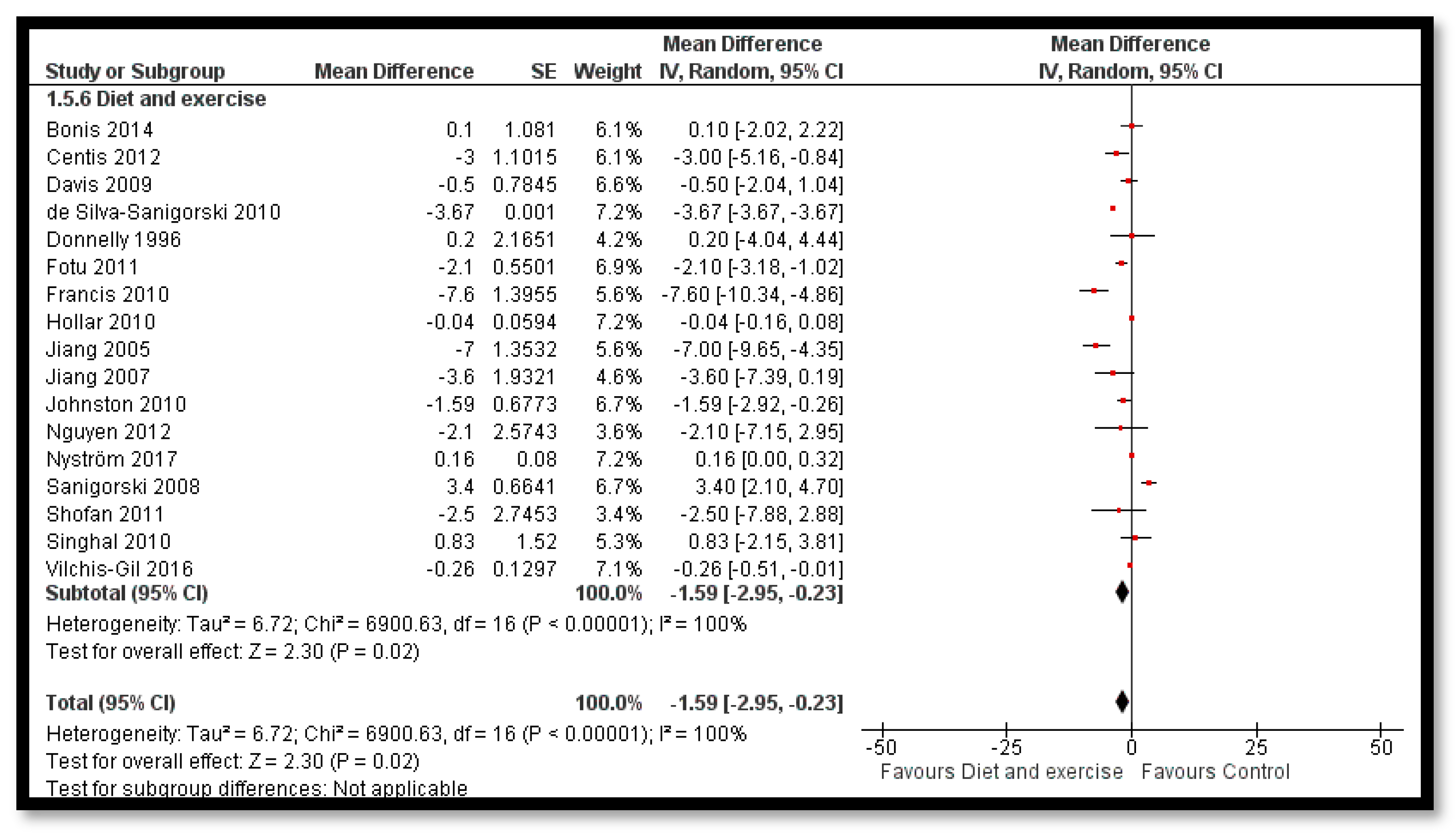
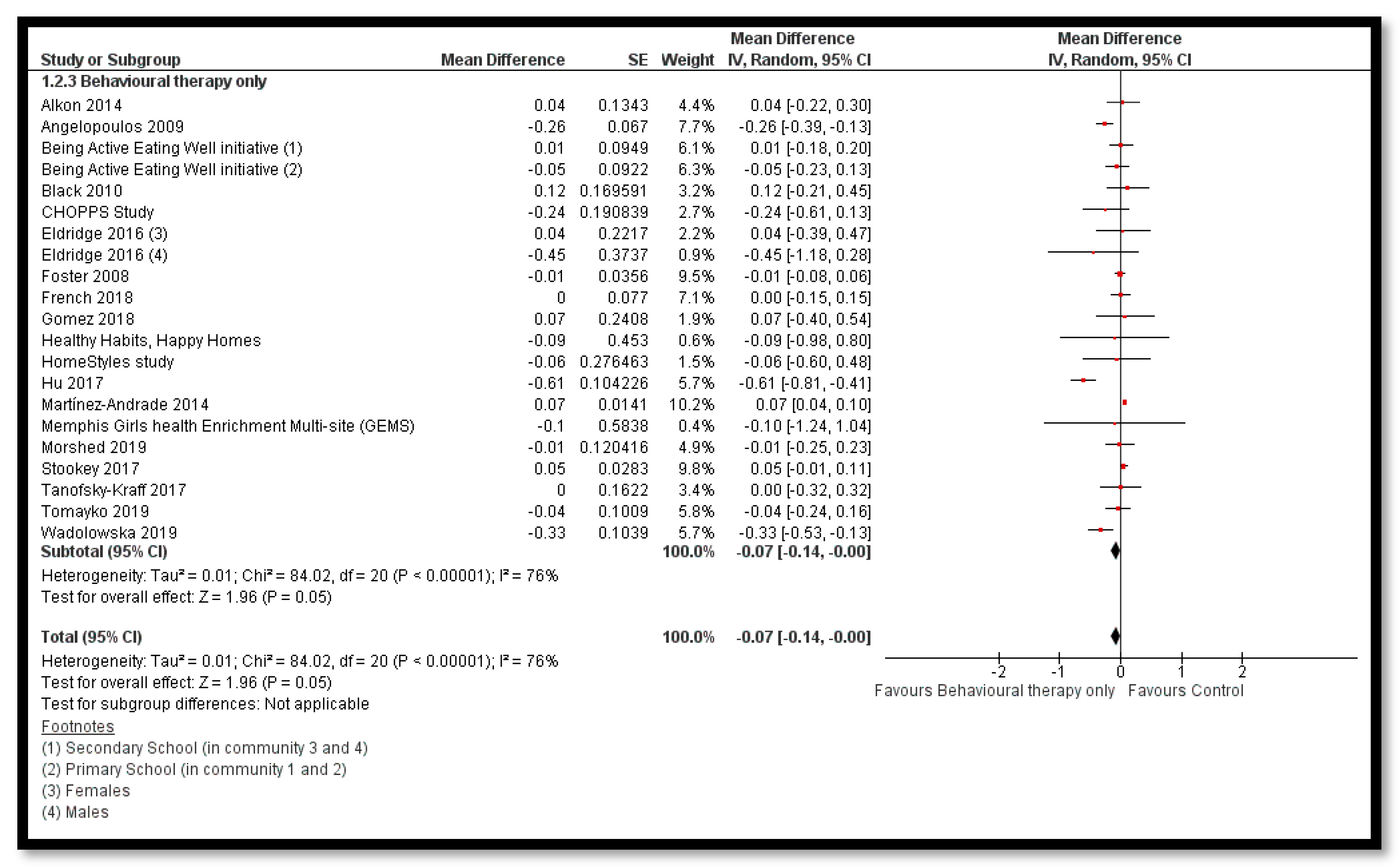
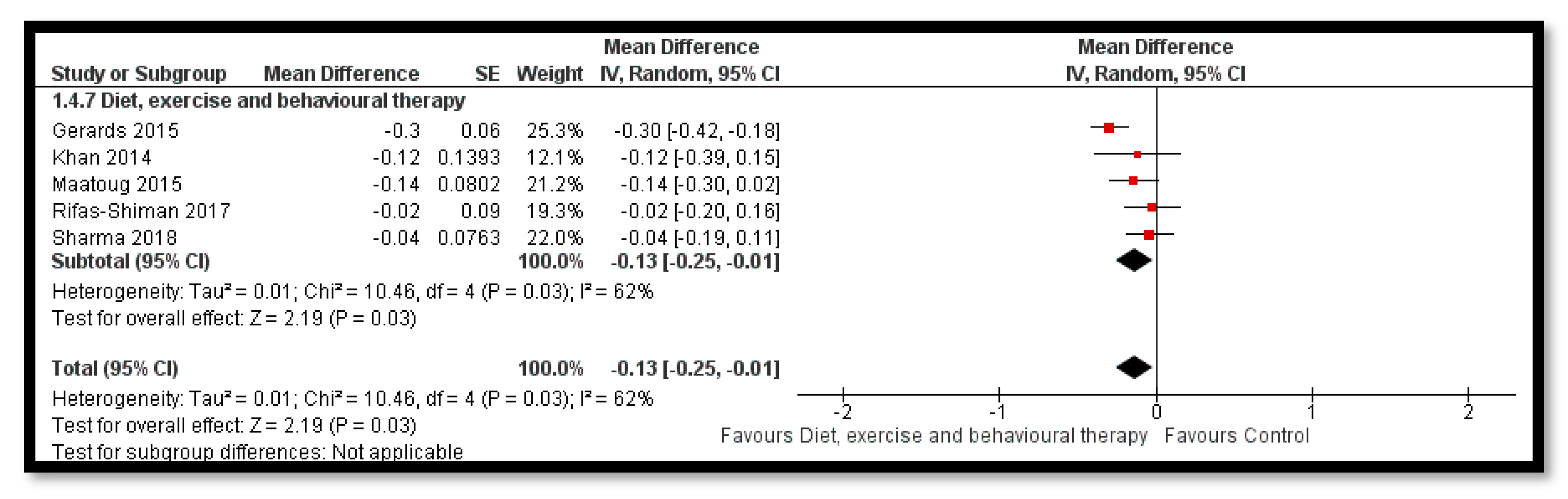
3.5.1. Comparison 1: Obesity Prevention
Primary Outcomes
Sensitivity Analysis for the Primary Outcomes
Secondary Outcomes
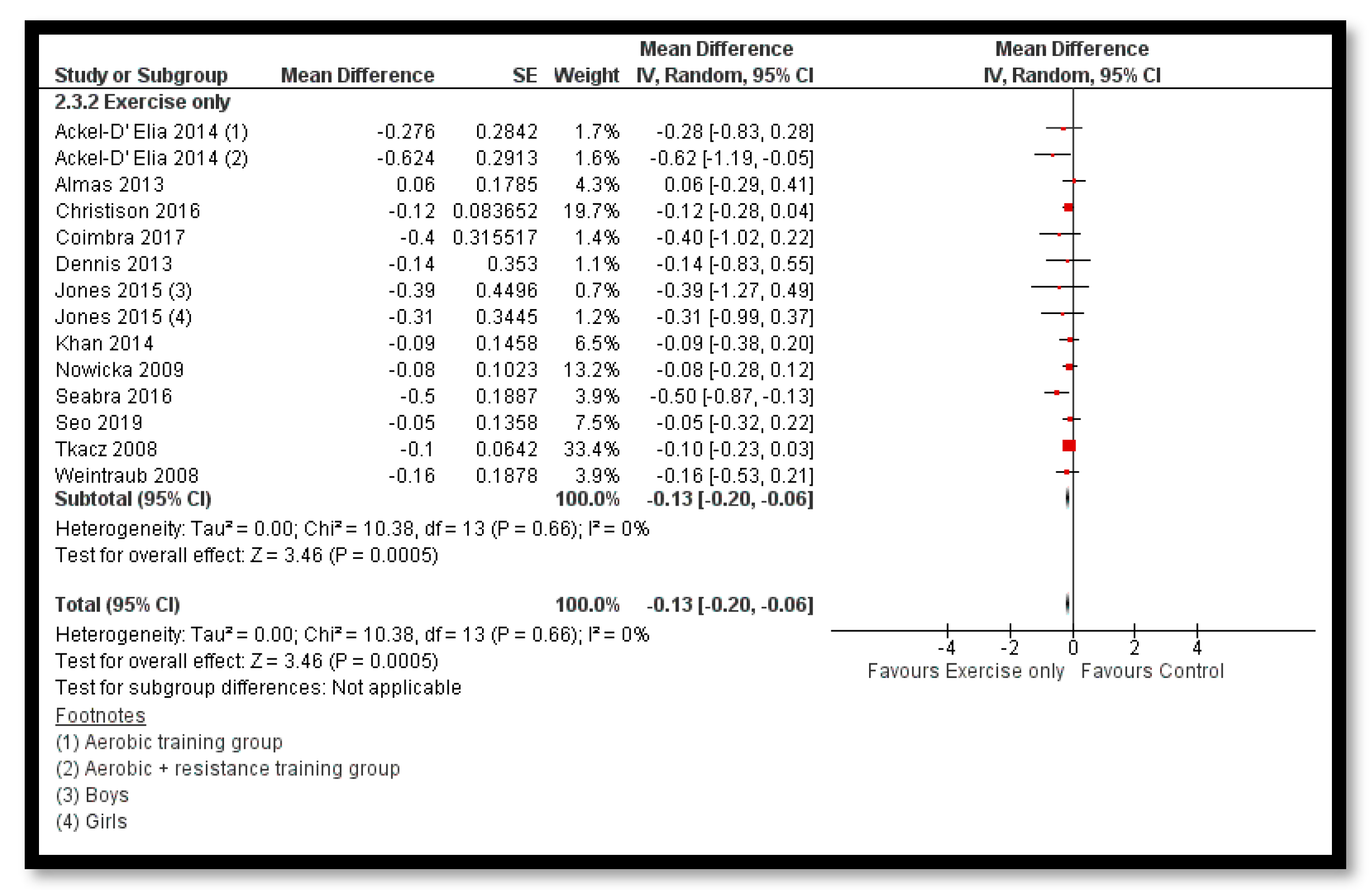
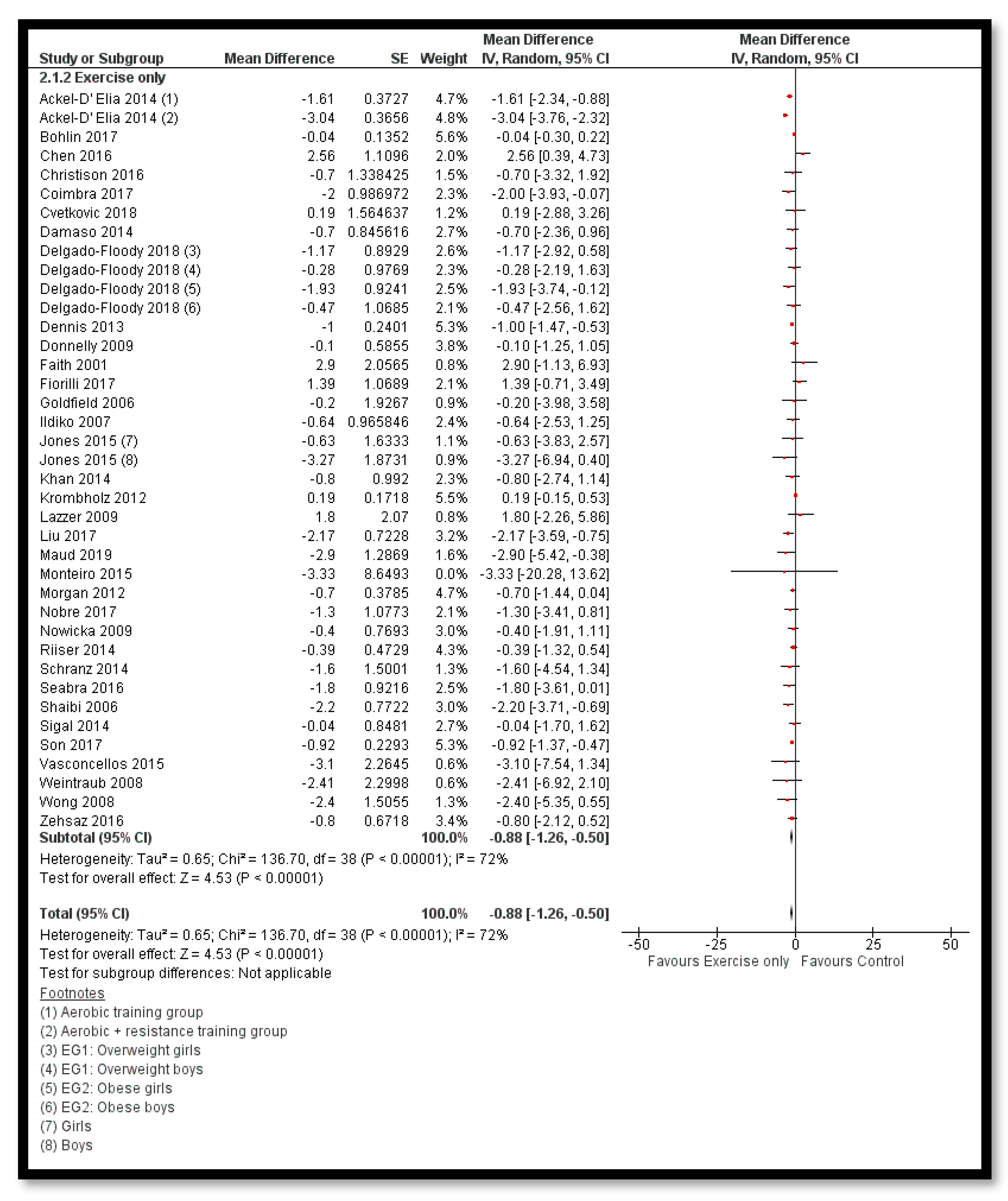
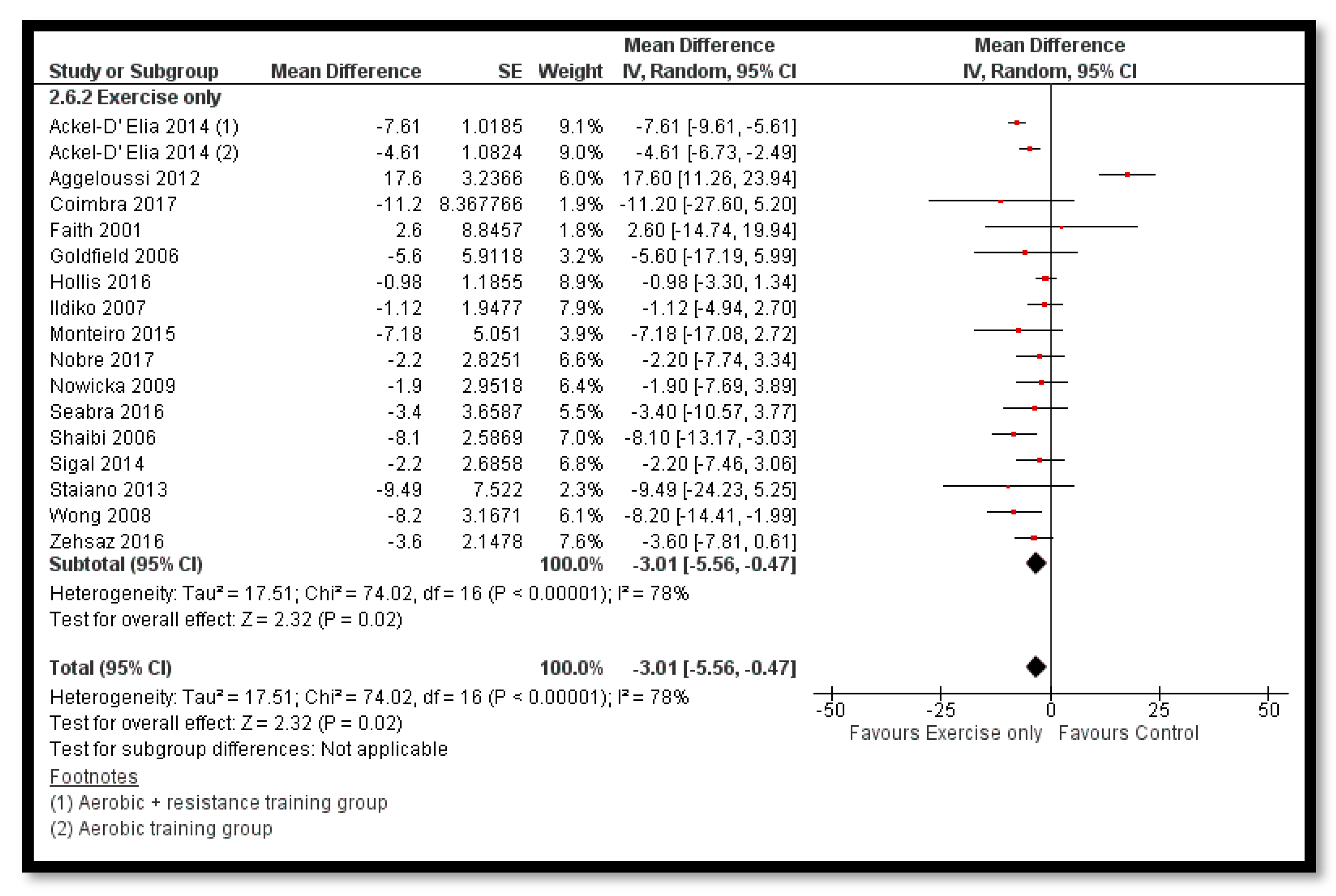
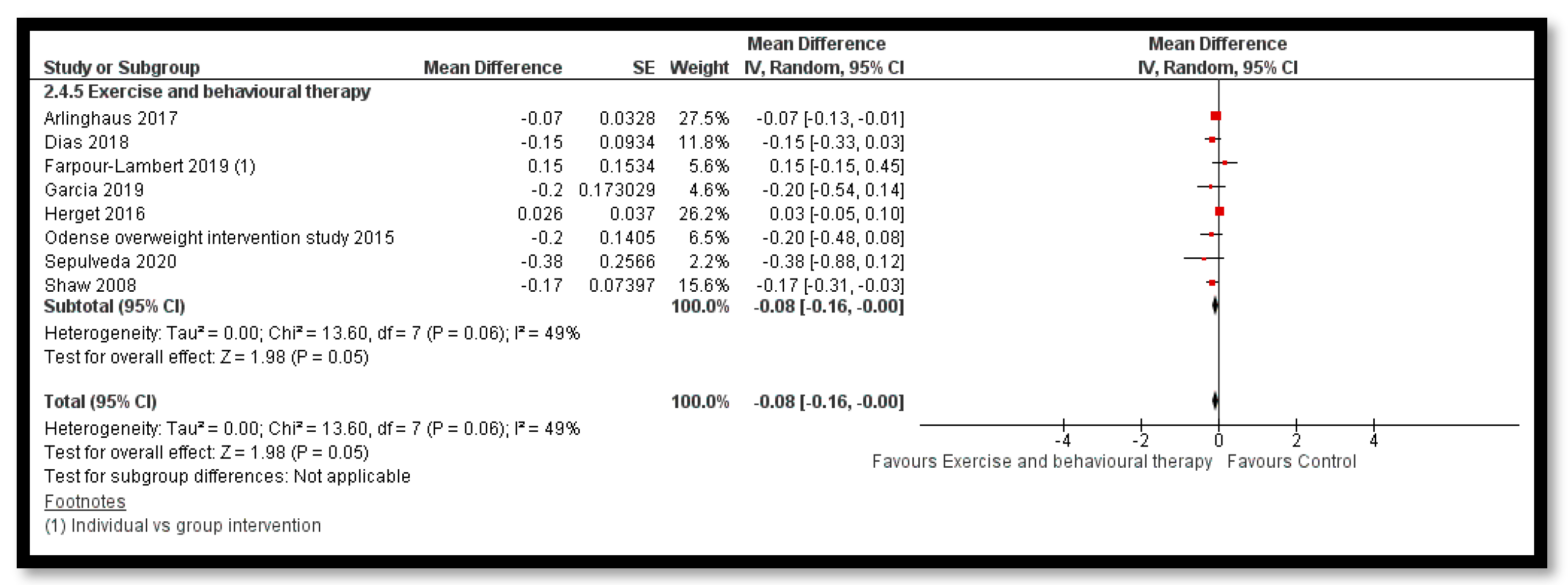
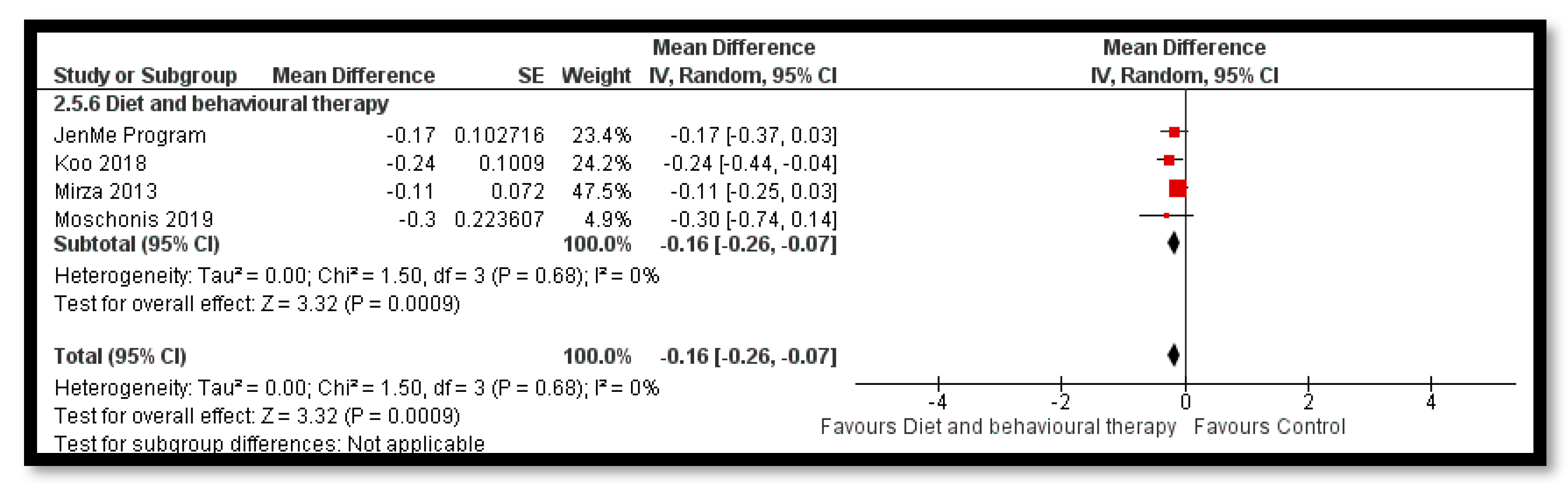
3.5.2. Comparison 2: Obesity Management
Primary Outcomes
Sensitivity Analysis for the Primary Outcomes
Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Karnik, S.; Kanekar, A. Childhood obesity: A global public health crisis. Int. J. Prev. Med. 2012, 3, 1. [Google Scholar]
- The Global Nutrition Report. 2019 [cited 2020 05/06/2020]. Available online: https://globalnutritionreport.org/ (accessed on 10 May 2019).
- Friedrich, M. Global obesity epidemic worsening. JAMA 2017, 318, 603. [Google Scholar] [CrossRef] [PubMed]
- Abarca-Gómez, L.; A Abdeen, Z.; Hamid, Z.A.; Abu-Rmeileh, N.M.; Acosta-Cazares, B.; Acuin, C.; Adams, R.J.; Aekplakorn, W.; Afsana, K.; A Aguilar-Salinas, C.; et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Skinner, A.C.; Ravanbakht, S.N.; Skelton, J.A.; Perrin, E.M.; Armstrong, S.C. Prevalence of Obesity and Severe Obesity in US Children, 1999–2016. Pediatrics 2018, 141, e20173459. [Google Scholar] [CrossRef] [PubMed]
- van Jaarsveld, C.H.; Gulliford, M.C. Childhood obesity trends from primary care electronic health records in England between 1994 and 2013: Population-based cohort study. Arch. Dis. Child. 2015, archdischild-2014-307151. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity and Overweight Factsheet. [cited 2020 03/06/2020]. 2017. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 11 May 2019).
- Popkin, B.M.; Slining, M. New dynamics in global obesity facing low-and middle-income countries. Obes. Rev. 2013, 14, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Bovet, P.; Ma, C.; Zhao, M.; Liang, Y.; Xi, B. Prevalence of underweight and overweight among young adolescents aged 12–15 years in 58 low-income and middle-income countries. Pediatric Obes. 2019, 14. [Google Scholar] [CrossRef]
- Roth, C.L.; Jain, V. Rising Obesity in Children: A Serious Public Health Concern; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- World Health Organization. Consideration of the Evidence on Childhood Obesity for the Commission on Ending Childhood Obesity: Report of the Ad Hoc Working Group on Science and Evidence for Ending Childhood Obesity; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Luttikhuis, H.O.; Baur, L.; Jansen, H.; A Shrewsbury, V.; O’Malley, C.; Stolk, R.P.; Summerbell, C.D. WITHDRAWN: Interventions for treating obesity in children. Cochrane Database Syst. Rev. 2019, 3, CD001872. [Google Scholar] [CrossRef]
- Pandita, A.; Sharma, D.; Pandita, D.; Pawar, S.; Tariq, M.; Kaul, A. Childhood obesity: Prevention is better than cure. Diabetes, Metab. Syndr. Obesity: Targets Ther. 2016, 9, 83–89. [Google Scholar] [CrossRef]
- Pineda, E.; Swinburn, B.; Sassi, F. Effective school food environment interventions for the prevention of childhood obesity: Systematic review and meta-analysis. Lancet 2019, 394, S77. [Google Scholar] [CrossRef]
- Mei, H.; Xiong, Y.; Xie, S.; Guo, S.; Li, Y.; Guo, B.; Zhang, J. The impact of long-term school-based physical activity interventions on body mass index of primary school children—A meta-analysis of randomized controlled trials. BMC Public Heal. 2016, 16, 205. [Google Scholar] [CrossRef] [PubMed]
- Viitasalo, A.; Eloranta, A.-M.; Lintu, N.; Väistö, J.; Venäläinen, T.; Kiiskinen, S.; Karjalainen, P.; Peltola, J.; Lampinen, E.-K.; Haapala, E.A.; et al. The effects of a 2-year individualized and family-based lifestyle intervention on physical activity, sedentary behavior and diet in children. Prev. Med. 2016, 87, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, S.G.; Asnaani, A.; Vonk, I.J.J.; Sawyer, A.T.; Fang, A. The Efficacy of Cognitive Behavioral Therapy: A Review of Meta-analyses. Cogn. Ther. Res. 2012, 36, 427–440. [Google Scholar] [CrossRef] [PubMed]
- Graf, C.; Rost, S.V.; Koch, B.; Heinen, S.; Falkowski, G.; Dordel, S.; Bjarnason-Wehrens, B.; Sreeram, N.; Brockmeier, K.; Christ, H.; et al. Data from the StEP TWO programme showing the effect on blood pressure and different parameters for obesity in overweight and obese primary school children. Cardiol. Young 2005, 15, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Hofsteenge, G.H.; Weijs, P.J.; Waal, H.A.D.-V.D.; De Wit, M.; Chinapaw, M.J. Effect of the Go4it multidisciplinary group treatment for obese adolescents on health related quality of life: A randomised controlled trial. BMC Public Heal. 2013, 13, 939. [Google Scholar] [CrossRef]
- Schranz, N.; Tomkinson, G.; Parletta, N.; Petkov, J.; Olds, T. Can resistance training change the strength, body composition and self-concept of overweight and obese adolescent males? A randomised controlled trial. Br. J. Sports Med. 2014, 48, 1482–1488. [Google Scholar] [CrossRef]
- Toulabi, T.; Nikoo, M.K.N.; Amini, F.; Nazari, H.; Mardani, M. The influence of a behavior modification interventional program on body mass index in obese adolescents. J. Formos. Med Assoc. 2012, 111, 153–159. [Google Scholar] [CrossRef]
- Vos, R.C.; Wit, J.M.; Pijl, H.; Kruyff, C.C.; Houdijk, M.C. The effect of family-based multidisciplinary cognitive behavioral treatment in children with obesity: Study protocol for a randomized controlled trial. Trials 2011, 12, 110. [Google Scholar] [CrossRef]
- De Bourdeaudhuij, I.; Van Cauwenberghe, E.; Spittaels, H.; Oppert, J.-M.; Rostami, C.; Brug, J.; Van Lenthe, F.; Lobstein, T.; Maes, L. School-based interventions promoting both physical activity and healthy eating in Europe: A systematic review within the HOPE project. Obes. Rev. 2011, 12, 205–216. [Google Scholar] [CrossRef]
- Kobes, A.; Kretschmer, T.; Timmerman, G.; Schreuder, P. Interventions aimed at preventing and reducing overweight/obesity among children and adolescents: A meta-synthesis. Obes. Rev. 2018, 19, 1065–1079. [Google Scholar] [CrossRef]
- Luttikhuis, H.O.; Baur, L.; Jansen, H.; A Shrewsbury, V.; O’Malley, C.; Stolk, R.P.; Summerbell, C. Cochrane review: Interventions for treating obesity in children. Evid.-Based Child Heal. A Cochrane Rev. J. 2009, 4, 1571–1729. [Google Scholar] [CrossRef]
- Mead, E.; Brown, T.; Rees, K.; Azevedo, L.B.; Whittaker, V.; Jones, D.; Olajide, J.; Mainardi, G.M.; Corpeleijn, E.; O’Malley, C.; et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese children from the age of 6 to 11 years. Cochrane Database Syst. Rev. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Waters, E.; De Silva-Sanigorski, A.; Burford, B.J.; Brown, T.; Campbell, K.J.; Gao, Y.; Armstrong, R.; Prosser, L.; Summerbell, C.D. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2011, CD001871. [Google Scholar] [CrossRef]
- Colquitt, J.L.; Loveman, E.; O’Malley, C.; Azevedo, L.B.; Mead, E.; Al-Khudairy, L.; Ells, L.J.; Metzendorf, M.-I.; Rees, K. Diet, physical activity, and behavioural interventions for the treatment of overweight or obesity in preschool children up to the age of 6 years. Cochrane Database Syst. Rev. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Faraoni, D.; Schaefer, S.T. Randomized controlled trials vs. observational studies: Why not just live together? BMC Anesthesiol. 2016, 16, 102. [Google Scholar] [CrossRef] [PubMed]
- Black, N. Why we need observational studies to evaluate the effectiveness of health care. BMJ 1996, 312, 1215–1218. [Google Scholar] [CrossRef] [PubMed]
- Hannan, E.L. Randomized clinical trials and observational studies: Guidelines for assessing respective strengths and limitations. JACC Cardiovasc. Interv. 2008, 1, 211–217. [Google Scholar] [CrossRef]
- Oakley, A.; Strange, V.; Bonell, C.; Allen, E.; Stephenson, J. Process evaluation in randomised controlled trials of complex interventions. BMJ 2006, 332, 413–416. [Google Scholar] [CrossRef]
- Mulder, R.; Singh, A.B.; Hamilton, A.; Das, P.; Outhred, T.; Morris, G.; Bassett, D.; Baune, B.T.; Berk, M.; Boyce, P.; et al. The limitations of using randomised controlled trials as a basis for developing treatment guidelines. Évid. Based Ment. Heal. 2017, 21, 4–6. [Google Scholar] [CrossRef]
- Cochrane, T. Review Manager (RevMan) 5.3.; The Nordic Cochrane Centre: Copenhagen, Denmark, 2008. [Google Scholar]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2011; Volume 4. [Google Scholar]
- Practice, E.; Care, O.O. EPOC Resources for Review Authors; Norwegian Knowledge Centre for the Health Services: Oslo, Norway, 2015. [Google Scholar]
- Guyatt, G.; Oxman, A.D.; E Vist, G.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.J.; Norris, S. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Kesztyüs, D.; Lauer, R.; Kesztyüs, T.; Kilian, R.; Steinacker, J.M.; on behalf of the “Join the Healthy Boat” Study Group. Costs and effects of a state-wide health promotion program in primary schools in Germany – the Baden-Württemberg Study: A cluster-randomized, controlled trial. PLOS ONE 2017, 12, e0172332. [Google Scholar] [CrossRef]
- Sutherland, R.; Reeves, P.; Campbell, E.; Lubans, D.R.; Morgan, P.J.; Nathan, N.; Wolfenden, L.; Okely, A.D.; Gillham, K.; Davies, L.; et al. Cost effectiveness of a multi-component school-based physical activity intervention targeting adolescents: The ’Physical Activity 4 Everyone’ cluster randomized trial. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 94. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Pallan, M.; Liu, W.J.; Hemming, K.; Frew, E.; Lin, R.; Martin, J.; Zanganeh, M.; Hurley, K.; Cheng, K.K.; et al. The CHIRPY DRAGON intervention in preventing obesity in Chinese primary-school--aged children: A cluster-randomised controlled trial. PLoS Med. 2019, 16, e1002971. [Google Scholar] [CrossRef] [PubMed]
- McCollister, K.E.; Tolbert, D.V.; Mishra, S.; Natale, R.; Uhlhorn, S.; Messiah, S.E. Cost Analysis of a Childcare Center-Based Intervention to Prevent Obesity in the Preschool Years. J. Compr. Pediatr. 2015, 6, 6. [Google Scholar] [CrossRef]
- Canaway, A.; Frew, E.; Lancashire, E.; Pallan, M.; Hemming, K.; Adab, P.; On behalf of the WAVES trial investigators. Economic evaluation of a childhood obesity prevention programme for children: Results from the WAVES cluster randomised controlled trial conducted in schools. PLoS ONE 2019, 14, e0219500. [Google Scholar] [CrossRef] [PubMed]
- Moodie, M.; Herbert, J.K.; De Silva-Sanigorski, A.M.; Mavoa, H.M.; Keating, C.L.; Carter, R.C.; Waters, E.; Gibbs, L.; Swinburn, B.A. The cost-effectiveness of a successful community-based obesity prevention program: The be active eat well program. Obesity 2013, 21, 2072–2080. [Google Scholar] [CrossRef] [PubMed]
- Epstein, L.H.; Paluch, R.A.; Wrotniak, B.H.; Daniel, T.O.; Kilanowski, C.; Wilfley, D.; Finkelstein, E. Cost-Effectiveness of Family-Based Group Treatment for Child and Parental Obesity. Child. Obes. 2014, 10, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Goldfield, G.; Epstein, L.; Kilanowski, C.; Paluch, R.; Kogut-Bossler, B. Cost-effectiveness of group and mixed family-based treatment for childhood obesity. Int. J. Obes. 2001, 25, 1843–1849. [Google Scholar] [CrossRef]
- Quattrin, T.; Cao, Y.; Paluch, R.A.; Roemmich, J.N.; Ecker, M.A.; Epstein, L.H. Cost-effectiveness of Family-Based Obesity Treatment. Pediatrics 2017, 140, e20162755. [Google Scholar] [CrossRef]
- Robertson, W.; Fleming, J.; Kamal, A.; Hamborg, T.; A Khan, K.; Griffiths, F.; Stewart-Brown, S.; Stallard, N.; Petrou, S.; Simkiss, D.; et al. Randomised controlled trial evaluating the effectiveness and cost-effectiveness of ‘Families for Health’, a family-based childhood obesity treatment intervention delivered in a community setting for ages 6 to 11 years. Heal. Technol. Assess. 2017, 21, 1–180. [Google Scholar] [CrossRef] [PubMed]
- Sharifi, M.; Franz, C.; Horan, C.M.; Giles, C.M.; Long, M.W.; Ward, Z.; Resch, S.C.; Marshall, R.; Gortmaker, S.L.; Taveras, E.M. Cost-Effectiveness of a Clinical Childhood Obesity Intervention. Pediatrics 2017, 140, e20162998. [Google Scholar] [CrossRef] [PubMed]
- Anderson, Y.C.; Leung, W.; Grant, C.C.; Cave, T.L.; Derraik, J.G.; Cutfield, W.S.; Pereira, N.M.; Hofman, P.L.; Sullivan, T.A. Economic evaluation of a multi-disciplinary community-based intervention programme for New Zealand children and adolescents with obesity. Obes. Res. Clin. Pr. 2018, 12, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Kalavainen, M.; Karjalainen, S.; Martikainen, J.; Korppi, M.; Linnosmaa, I.; Nuutinen, O. Cost-effectiveness of routine and group programs for treatment of obese children. Pediatr. Int. 2009, 51, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Panca, M.; Christie, D.; Cole, T.J.; Costa, S.; Gregson, J.; Holt, R.; Hudson, L.D.; Kessel, A.S.; Kinra, S.; Mathiot, A.; et al. Cost-effectiveness of a community-delivered multicomponent intervention compared with enhanced standard care of obese adolescents: Cost-utility analysis alongside a randomised controlled trial (the HELP trial). BMJ Open 2018, 8, e018640. [Google Scholar] [CrossRef]
- Larsen, K.T.; Huang, T.; Møller, N.C.; Andersen, L.B.; Sørensen, J. Cost-effectiveness of a day-camp weight-loss intervention programme for children: Results based on a randomised controlled trial with one-year follow-up. Scand. J. Public Heal. 2017, 45, 666–674. [Google Scholar] [CrossRef]
- Wake, M.; Gold, L.; McCallum, Z.; Gerner, B.; Waters, E. Economic Evaluation of a Primary Care Trial to Reduce Weight Gain in Overweight/Obese Children: The LEAP Trial. Ambul. Pediatr. 2008, 8, 336–341. [Google Scholar] [CrossRef]
- Zylke, J.W.; Bauchner, H. Preventing Obesity in Children: A Glimmer of Hope. JAMA 2018, 320, 443–444. [Google Scholar] [CrossRef]
- Vissers, D.; Hens, W.; Hansen, D.; Taeymans, J. The Effect of Diet or Exercise on Visceral Adipose Tissue in Overweight Youth. Med. Sci. Sports Exerc. 2016, 48, 1415–1424. [Google Scholar] [CrossRef]
- Lien, A.S.-Y.; Tsai, J.-L.; Lee, J.-T.; Wu, M.-Y.; Jiang, Y.-D.; Yen, H.-R. A Systematic Review and Meta-Analysis of the Effect of Lifestyle Modification on Metabolic Control in Overweight Children. Evid.-Based Complement. Altern. Med. 2017, 2017, 1–12. [Google Scholar] [CrossRef]
- Coppock, J.H.; Ridolfi, D.R.; Hayes, J.F.; Stpaul, M.; Wilfley, D.E. Current Approaches to the Management of Pediatric Overweight and Obesity. Curr. Treat. Options Cardiovasc. Med. 2014, 16, 343. [Google Scholar] [CrossRef] [PubMed]
- Miri, S.F.; Javadi, M.; Lin, C.-Y.; Griffiths, M.D.; Björk, M.; Pakpour, A.H. Effectiveness of cognitive-behavioral therapy on nutrition improvement and weight of overweight and obese adolescents: A randomized controlled trial. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2190–2197. [Google Scholar] [CrossRef] [PubMed]
- Wilfley, D.E.; Hayes, J.F.; Balantekin, K.N.; Van Buren, R.J.; Epstein, L.H. Behavioral interventions for obesity in children and adults: Evidence base, novel approaches, and translation into practice. Am. Psychol. 2018, 73, 981–993. [Google Scholar] [CrossRef] [PubMed]
- Sonntag, D. Why Early Prevention of Childhood Obesity Is More Than a Medical Concern: A Health Economic Approach. Ann. Nutr. Metab. 2017, 70, 175–178. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PROGRESS-Plus Factors | Summary of Reported Factors |
|---|---|
| Place of residence/setting | No. studies conducted in high-income countries (HICs): 533 No. studies conducted in upper-middle-income countries (UMICs): 70 No. studies conducted in lower-middle-income countries (LMICs): 13 40 studies had no country stated. |
| Race/ethnicity/culture/language | Almost half of the included studies specified details under this domain while reporting the baseline characteristics of the study population. |
| Occupation | This is one of the most under-reported categories in the studies probably since the study population were children and adolescents. Very few studies reported the occupation of the parents of the enrolled chidlren and adolescents. |
| Gender/sex | This category was reported in almost every study, although few did not provide the specific distribution of the sample by sex when participants from both sexes were included. Most studies were conducted with children and adolescents, but some also included only adolescents or only children. |
| Religion | This is also one of the under-reported categories in the studies. Very few studies reported on this domain. |
| Education | Since many studies were carried out in school settings, majority of such studies reported the level of education as preschool/elementary, primary or secondary. |
| Socioeconomic status | This factor was also poorly reported in the published data of the included studies. Moreover, various studies used different definitions of the socio-economic status. Majorly, the studies reported income, class, or the areas of residence (rural/urban/mixed) under this domain. |
| Social capital | Few studies directly reported any measurement of social capital. Indirectly, some studies reported that participants were recruited through schools, clinics, hospitals and sports/recreation centres, thus indicating that participants had at least one social connection or network. |
| Plus (other characteristics) | All studies reported on age, as this factor is essential for their analysis. Many reported the participants’ Body Mass Index (BMI) and other body measures e.g., height, weight, skinfold thickness. Studies including parents also reported parent education, occupation, income and marital status although very infrequently. |
| Recruitment methods | Most studies recruited their participants through similar strategies: schools, mailings, printed ads and flyers distributed in school campuses, community centres, clinics or hospitals, through advertisement on local radio and television. Most of the studies took place in HICs and in children and/or adolescents, hence the use of schools and community centres. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salam, R.A.; Padhani, Z.A.; Das, J.K.; Shaikh, A.Y.; Hoodbhoy, Z.; Jeelani, S.M.; Lassi, Z.S.; Bhutta, Z.A. Effects of Lifestyle Modification Interventions to Prevent and Manage Child and Adolescent Obesity: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 2208. https://doi.org/10.3390/nu12082208
Salam RA, Padhani ZA, Das JK, Shaikh AY, Hoodbhoy Z, Jeelani SM, Lassi ZS, Bhutta ZA. Effects of Lifestyle Modification Interventions to Prevent and Manage Child and Adolescent Obesity: A Systematic Review and Meta-Analysis. Nutrients. 2020; 12(8):2208. https://doi.org/10.3390/nu12082208
Chicago/Turabian StyleSalam, Rehana A., Zahra A. Padhani, Jai K. Das, Amina Y. Shaikh, Zahra Hoodbhoy, Sarah Masroor Jeelani, Zohra S. Lassi, and Zulfiqar A. Bhutta. 2020. "Effects of Lifestyle Modification Interventions to Prevent and Manage Child and Adolescent Obesity: A Systematic Review and Meta-Analysis" Nutrients 12, no. 8: 2208. https://doi.org/10.3390/nu12082208
APA StyleSalam, R. A., Padhani, Z. A., Das, J. K., Shaikh, A. Y., Hoodbhoy, Z., Jeelani, S. M., Lassi, Z. S., & Bhutta, Z. A. (2020). Effects of Lifestyle Modification Interventions to Prevent and Manage Child and Adolescent Obesity: A Systematic Review and Meta-Analysis. Nutrients, 12(8), 2208. https://doi.org/10.3390/nu12082208