Electrolyte Intake and Major Food Sources of Sodium, Potassium, Calcium and Magnesium among a Population in Western Austria

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Electrolyte Intake
2.3. Statistical Analysis
3. Results
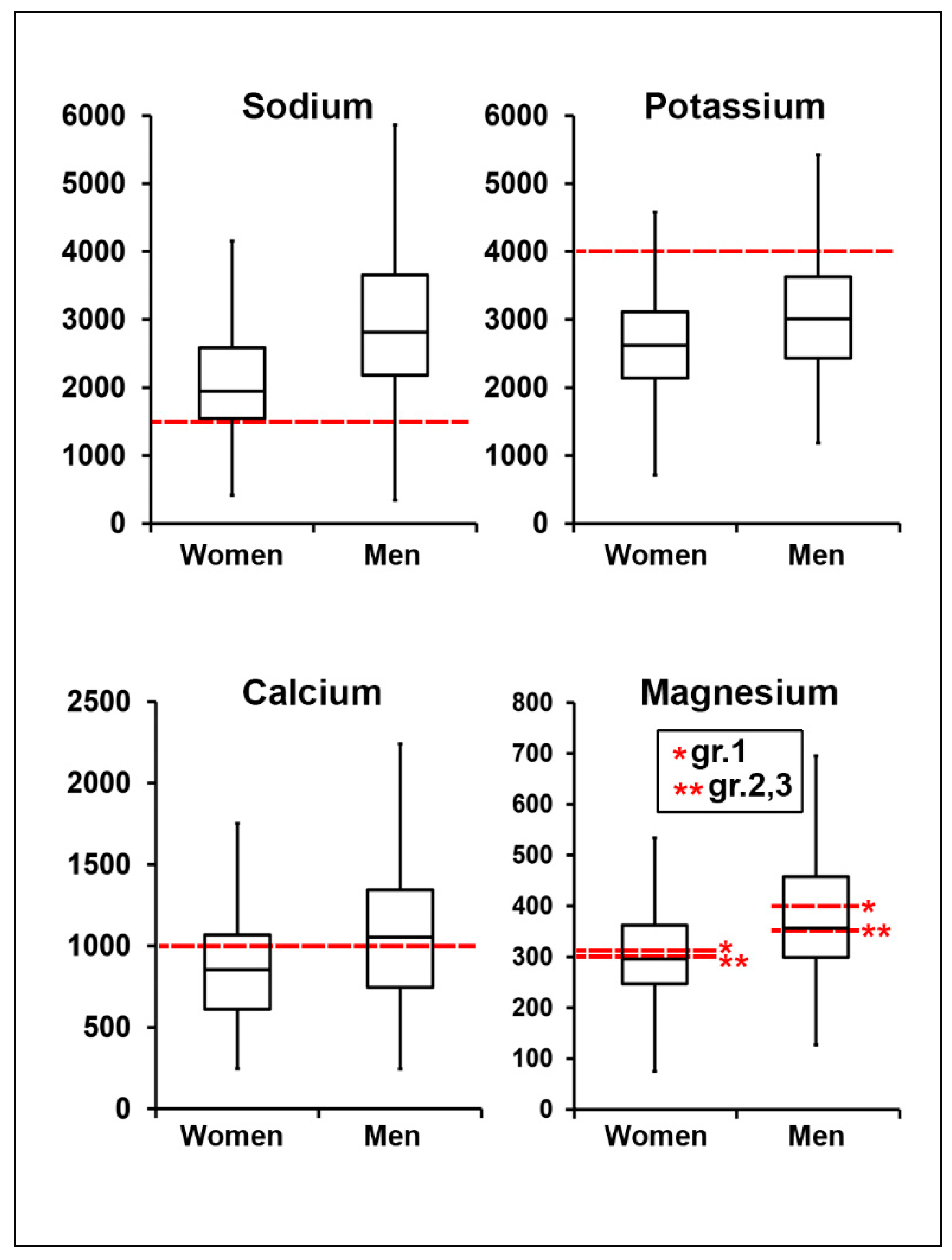
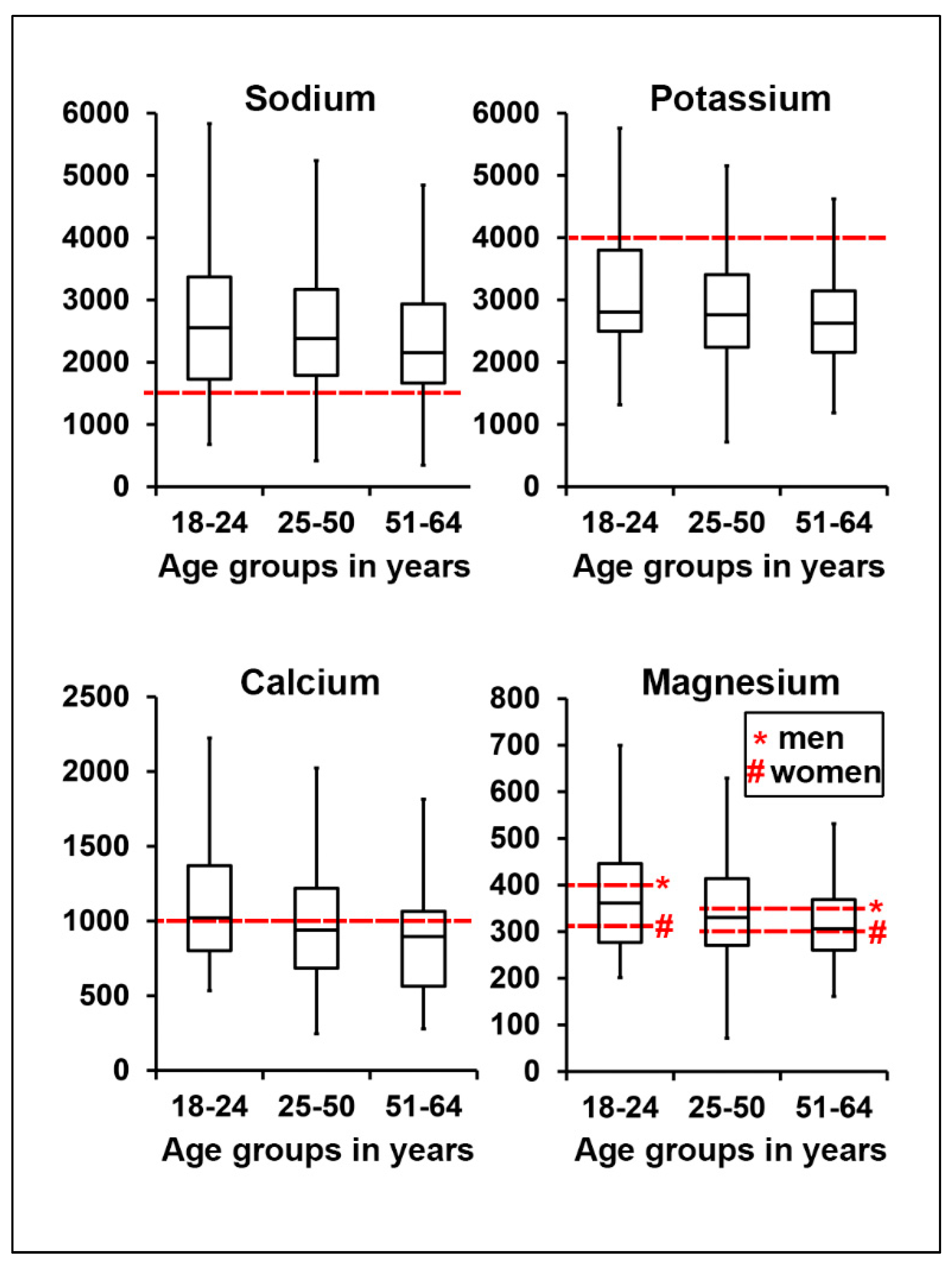
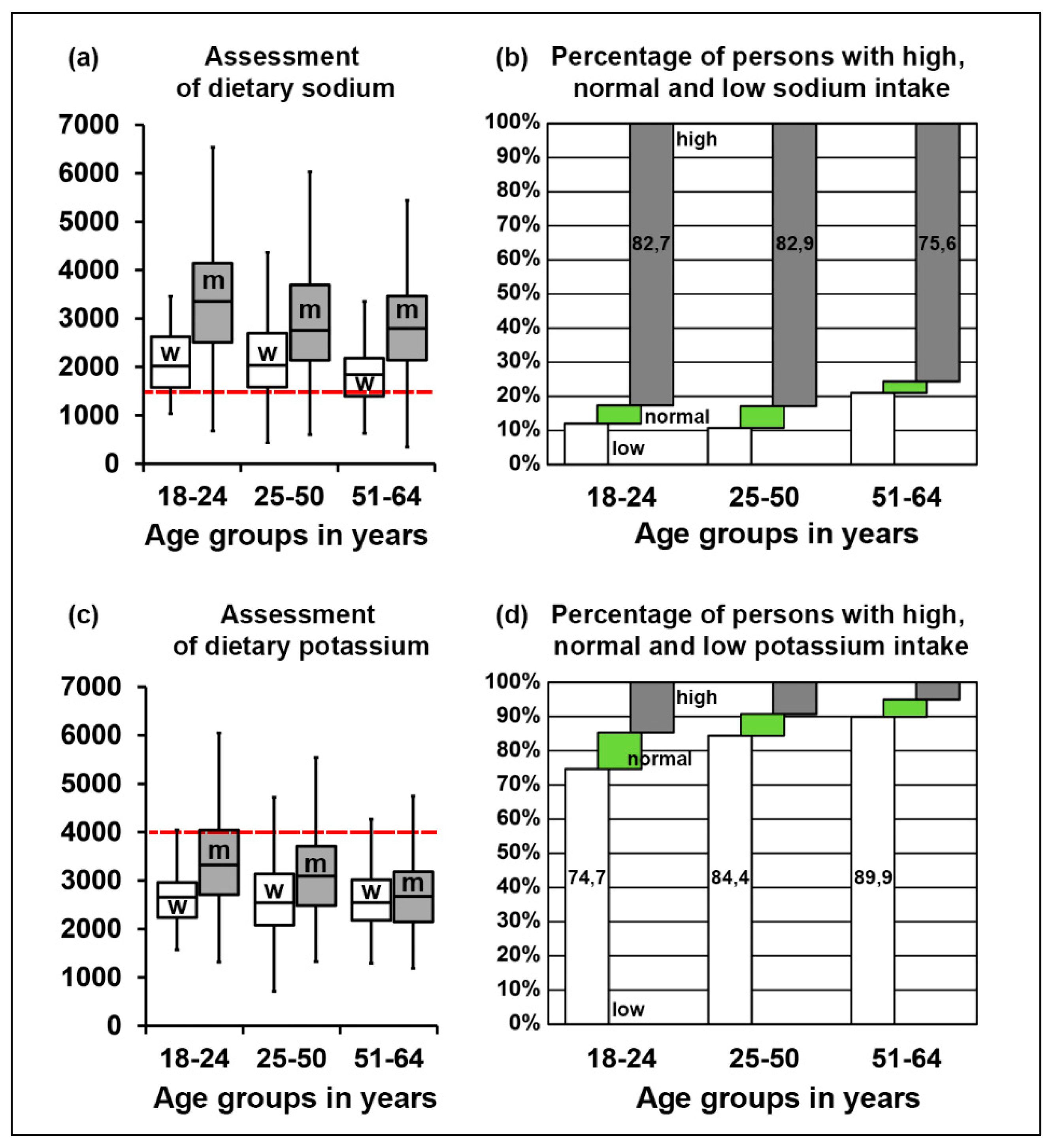
3.1. Assessment of Electrolyte Intake
3.2. Main Food Sources of Electrolyte Intake
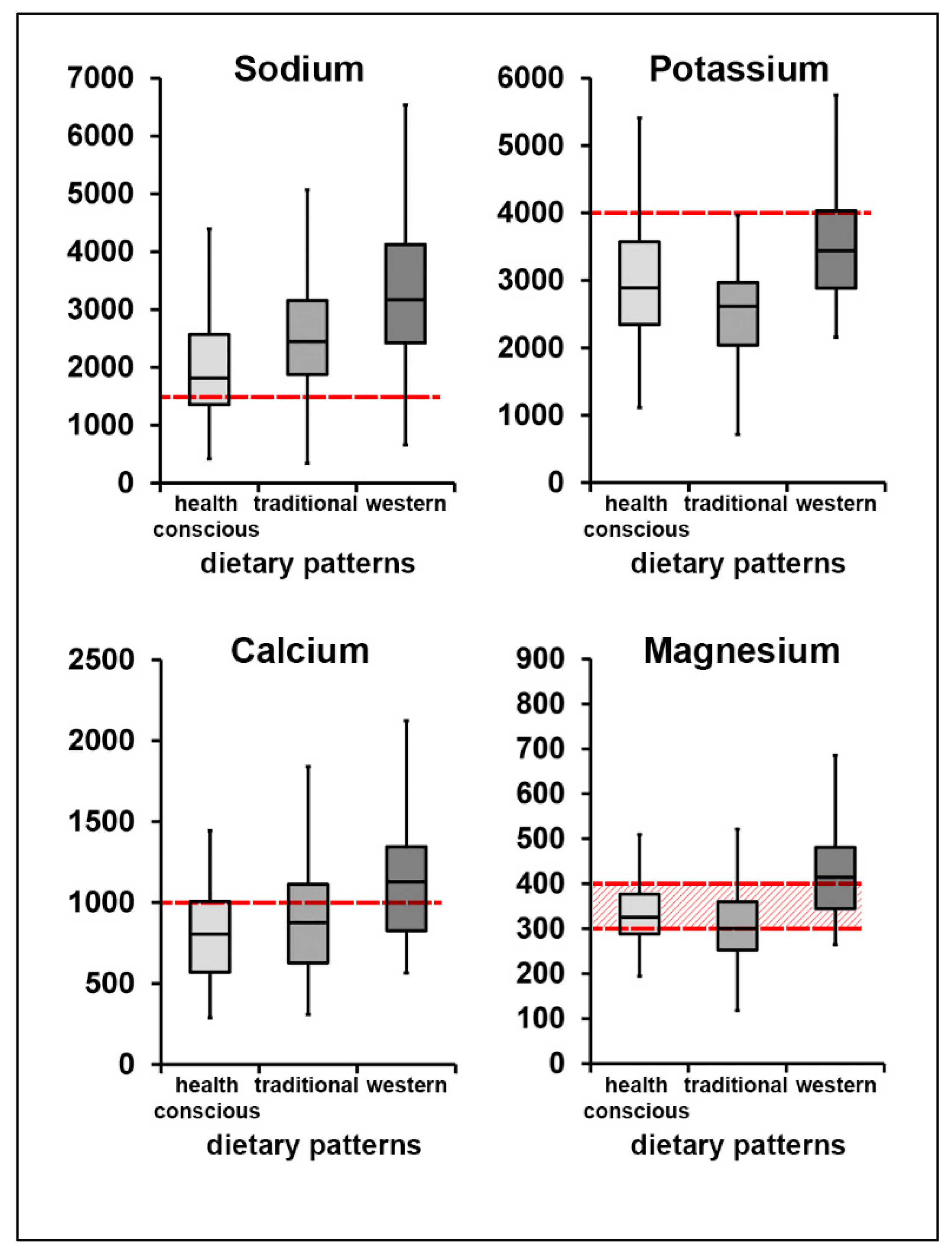
3.3. Electrolyte Intake among Dietary Patterns
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kear, T.M. Fluid and Electrolyte Management Across the Age Continuum. Nephrol. Nurs. J. 2017, 44, 491–496. [Google Scholar]
- DGE; Österreichische Gesellschaft für Ernährung; Schweizerische Gesellschaft für Ernährung. Referenzwerte für die Nährstoffzufuhr, 2nd ed.; Losebl.-Ausg; Deutsche Ges. f. Ernährung: Bonn, Germany, 2016.
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; De Simone, G.; Dominczak, A.F.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- WHO. Potassium Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- EFSA. EFSA Panel on Dietetic Products, Nutrition and Allergies. Scientific opinion on dietary reference values for potassium. EFSA J. 2016, 14, 4592. [Google Scholar] [CrossRef]
- Vaskonen, T. Dietary minerals and modification of cardiovascular risk factors. J. Nutr. Biochem. 2003, 14, 492–506. [Google Scholar] [CrossRef]
- Elin, R.J. Assessment of magnesium status for diagnosis and therapy. Magnes. Res. 2010, 23, S194–S198. [Google Scholar] [CrossRef]
- Liamis, G.; Rodenburg, E.M.; Hofman, A.; Zietse, R.; Stricker, B.H.; Hoorn, E.J. Electrolyte Disorders in Community Subjects: Prevalence and Risk Factors. Am. J. Med. 2013, 126, 256–263. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Li, J.; MacGregor, G.A. Effect of longer term modest salt reduction on blood pressure: Cochrane systematic review and meta-analysis of randomised trials. BMJ 2013, 346, f1325. [Google Scholar] [CrossRef]
- Graudal, N.A.; Hubeck-Graudal, T.; Jürgens, G. Effects of Low-Sodium Diet vs. High-Sodium Diet on Blood Pressure, Renin, Aldosterone, Catecholamines, Cholesterol, and Triglyceride (Cochrane Review). Am. J. Hypertens. 2012, 25, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Resnick, L.M. Cellular calcium and magnesium metabolism in the pathophysiology and treatment of hypertension and related metabolic disorders. Am. J. Med. 1992, 93, S11–S20. [Google Scholar] [CrossRef]
- Han, H.; Fang, X.; Wei, X.; Liu, Y.; Jin, Z.; Chen, Q.; Fan, Z.; Aaseth, J.; Hiyoshi, A.; He, J.; et al. Dose-response relationship between dietary magnesium intake, serum magnesium concentration and risk of hypertension: A systematic review and meta-analysis of prospective cohort studies. Nutr. J. 2017, 16, 26. [Google Scholar] [CrossRef] [PubMed]
- Binia, A.; Jaeger, J.; Hu, Y.; Singh, A.; Zimmermann, D. Daily potassium intake and sodium-to-potassium ratio in the reduction of blood pressure. J. Hypertens. 2015, 33, 1509–1520. [Google Scholar] [CrossRef]
- Polonia, J.; Monteiro, J.; Almeida, J.; Silva, J.A.; Bertoquini, S. High salt intake is associated with a higher risk of cardiovascular events. Blood Press. Monit. 2016, 21, 301–306. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Fahimi, S.; Singh, G.M.; Micha, R.; Khatibzadeh, S.; Engell, R.E.; Lim, S.; Danaei, G.; Ezzati, M.; Powles, J. Global Sodium Consumption and Death from Cardiovascular Causes. N. Engl. J. Med. 2014, 371, 624–634. [Google Scholar] [CrossRef]
- Resnick, L.M. Cellular ions in hypertension, insulin resistance, obesity, and diabetes: A unifying theme. J. Am. Soc. Nephrol. 1992, 3 (Suppl. S4), S78–S85. [Google Scholar]
- Chung, M.; Tang, A.M.; Fu, Z.; Wang, D.D.; Newberry, S.J. Calcium Intake and Cardiovascular Disease Risk: An Updated Systematic Review and Meta-analysis. Ann. Intern. Med. 2016, 165, 856–866. [Google Scholar] [CrossRef]
- Bolland, M.; Bauer, D.; Huang, J.; Ou, H.-Y.; Chiu, K.C. Calcium Supplements and Fracture Prevention. N. Engl. J. Med. 2014, 370, 386–388. [Google Scholar] [CrossRef]
- Resnick, L.M.; Barbagallo, M.; Gupta, R.K.; Laragh, J.H. Ionic basis of hypertension in diabetes mellitus. Role of hyperglycemia. Am. J. Hypertens. 1993, 6, 413–417. [Google Scholar] [CrossRef]
- Beugelsdijk, S.; Van Schaik, T. Differences in social capital between 54 Western European regions. Reg. Stud. 2005, 39, 1053–1064. [Google Scholar] [CrossRef]
- Romon, I.; Jougla, E.; Balkau, B.; Fagot-Campagna, A. The burden of diabetes-related mortality in France in 2002: An analysis using both underlying and multiple causes of death. Eur. J. Epidemiol. 2008, 23, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Dorner, T.; Rieder, A. Epidemiologie der koronaren Herzkrankheit und Bedeutung für die Prävention. J. Kardiol. Aust. J. Cardiol. 2005, 12, 13–15. [Google Scholar]
- Großschädl, F.; Stronegger, W.J. Regional trends in obesity and overweight among Austrian adults between 1973 and 2007. Wien. Klin. Wochenschr. 2012, 124, 363–369. [Google Scholar] [CrossRef]
- Müller-Nordhorn, J.; Rossnagel, K.; Mey, W.; Willich, S.N. Regional variation and time trends in mortality from ischaemic heart disease: East and West Germany 10 years after reunification. J. Epidemiol. Community Health 2004, 58, 481–485. [Google Scholar] [CrossRef]
- Stein, K.V.; Rieder, A.; Dorner, T. East-West gradient in cardio-vascular mortality in Austria: How much can we explain by following the pattern of risk factors? Int. J. Health Geogr. 2011, 10, 59. [Google Scholar] [CrossRef]
- Elmadfa, I.; Hasenegger, V.; Wagner, K.; Putz, P.; Weidl, N.-M.; Wottawa, D.; Kuen, T.; Seiringer, G.; Meyer, A.L.; Sturtzel, B.; et al. Österreichischer Ernährungsbericht, 1st ed.; Elmadfa: Vienna, Austria, 2012. [Google Scholar]
- Weichselbaum, E.; Benelam, B.; Costa, H.S. Synthesis Report No 6: Traditional Foods in Europe J. EuroFIR Project Management Office/British Nutrition Foundation. United Kingdom. Available online: http://www.eurofir.net (accessed on 6 May 2010).
- Trichopoulou, A.; Soukara, S.; Vasilopoulou, E. Traditional foods: A science and society perspective. Trends Food Sci. Technol. 2007, 18, 420–427. [Google Scholar] [CrossRef]
- European Commission. Database of Origin and Registration (DOOR). Available online: http://ec.europa.eu/agriculture/quality/door/list.html?&recordStart=0&filter.dossierNumber=&filter.comboName=&filterMin.milestone__mask=&filterMin.milestone=&filterMax.milestone__mask=&filterMax.milestone=&filter.country=AT&filter.category=&filter.type=&filter.status=&locale=en (accessed on 12 June 2012).
- Egg, S.; Erler, J.; Perktold, B.; Hasenegger, V.; Rust, P.; Ramoner, R.; König, J.; Purtscher, A.E. Traditional v. modern dietary patterns among a population in western Austria: Associations with body composition and nutrient profile. Public Health Nutr. 2018, 22, 455–465. [Google Scholar] [CrossRef]
- Statistics Austria. Causes of Death at a Glance: Current Annual Results. 2017. Available online: http://www.statistik.at/web_en/statistics/PeopleSociety/health/causes_of_death/causes_of_death_at_a_glance/index.html (accessed on 5 March 2019).
- European Commission. ECHI Indicator Development and Documentation: Joint Action for ECHIM Final Report Part II; National Institute for Public Health and the Environment (RIVM): Bilthoven, The Netherlands, 2012. [Google Scholar]
- EFSA. General principles for the collection of national food consumption data in the view of a pan-European dietary survey. EFSA J. 2009, 7, 1435. [Google Scholar] [CrossRef]
- Max Rubner-Institut; Bundesforschungsinstitut für Ernährung und Lebensmittel. Nationale Verzehrsstudie II. Ernahr. Wiss. Prax. 2008, 2, 77–81. [Google Scholar]
- Max Rubner-Institut; Bundesforschungsinstitut für Ernährung und Lebensmittel. Bundeslebensmittelschlüssel (BLS)-Version 3.02. 2019. Available online: http://www.blsdb.de (accessed on 28 January 2019).
- Olza, J.; Aranceta-Bartrina, J.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Gil, Á. Reported Dietary Intake, Disparity between the Reported Consumption and the Level Needed for Adequacy and Food Sources of Calcium, Phosphorus, Magnesium and Vitamin D in the Spanish Population: Findings from the ANIBES Study. Nutrients 2017, 9, 168. [Google Scholar] [CrossRef]
- Archer, E.; Hand, G.A.; Blair, S.N. Validity of U.S. Nutritional Surveillance: National Health and Nutrition Examination Survey Caloric Energy Intake Data, 1971–2010. PLoS ONE 2013, 8, e76632. [Google Scholar] [CrossRef]
- Powles, J.; Fahimi, S.; Micha, R.; Khatibzadeh, S.; Shi, P.; Ezzati, M.; Engell, R.E.; Lim, S.S.; Danaei, G.; Mozaffarian, D.; et al. Global, regional and national sodium intakes in 1990 and 2010: A systematic analysis of 24 h urinary sodium excretion and dietary surveys worldwide. BMJ Open 2013, 3, e003733. [Google Scholar] [CrossRef]
- Cogswell, M.E.; Zhang, Z.; Carriquiry, A.L.; Gunn, J.P.; Kuklina, E.V.; Saydah, S.H.; Yang, Q.; Moshfegh, A.J. Sodium and potassium intakes among US adults: NHANES 2003–2008. Am. J. Clin. Nutr. 2012, 96, 647–657. [Google Scholar] [CrossRef]
- Weaver, C.M. Potassium and Health. Adv. Nutr. 2013, 4, 368S–377S. [Google Scholar] [CrossRef] [PubMed]
- Brown, I.J.; Tzoulaki, I.; Candeias, V.; Elliott, P. Salt intakes around the world: Implications for public health. Int. J. Epidemiol. 2009, 38, 791–813. [Google Scholar] [CrossRef] [PubMed]
- Mensink, G.B.M.; Fletcher, R.; Gurinovic, M.; Huybrechts, I.; Lafay, L.; Serra-Majem, L.; Szponar, L.; Tetens, I.; Verkaik-Kloosterman, J.; Baka, A.; et al. Mapping low intake of micronutrients across Europe. Br. J. Nutr. 2013, 110, 755–773. [Google Scholar] [CrossRef]
- Rosanoff, A.; Weaver, C.M.; Rude, R.K. Suboptimal magnesium status in the United States: Are the health consequences underestimated? Nutr. Rev. 2012, 70, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Rust, P.; Ekmekcioglu, C. Impact of Salt Intake on the Pathogenesis and Treatment of Hypertension. Adv. Exp. Med. Biol. 2016, 956, 61–84. [Google Scholar] [CrossRef]
- Rust, P.; Hasenegger, V.; König, J. (Eds.) Österreichischer Ernährungsbericht 2017; Universität Wien: Vienna, Austria, 2017. [Google Scholar]
- Bundesministerium für Gesundheit und Frauen (Ed.) Die Österreichische Ernährungspyramide; Vienna, Austria, 2016. Available online: https://broschuerenservice.sozialministerium.at/Home/Download?publicationId=617 (accessed on 28 January 2019).
- Health Canada. Canada’s Dietary Guidelines for Health Professionals and Policy Makers; Health Canada = Santé Canada: Ottawa, ON, Canada, 2019. [Google Scholar]
- Marangoni, F.; Pellegrino, L.; Verduci, E.; Ghiselli, A.; Bernabei, R.; Calvani, R.; Cetin, I.; Giampietro, M.; Perticone, F.; Piretta, L.; et al. Cow’s Milk Consumption and Health: A Health Professional’s Guide. J. Am. Coll. Nutr. 2018, 38, 197–208. [Google Scholar] [CrossRef] [PubMed]
- Thorning, T.K.; Raben, A.; Tholstrup, T.; Soedamah-Muthu, S.S.; Givens, I.; Astrup, A. Milk and dairy products: Good or bad for human health? An assessment of the totality of scientific evidence. Food Nutr. Res. 2016, 60, 32527. [Google Scholar] [CrossRef] [PubMed]
- Balk, E.M.; Adam, G.P.; Langberg, V.N.; Earley, A.; Clark, P.; Ebeling, P.R.; Mithal, A.; Rizzoli, R.; Zerbini, C.A.F.; Pierroz, D.D.; et al. Global dietary calcium intake among adults: A systematic review. Osteoporos. Int. 2017, 28, 3315–3324. [Google Scholar] [CrossRef]
- Fang, A.; Li, K.; Guo, M.; He, J.; Li, H.; Shen, X.; Song, J. Long-Term Low Intake of Dietary Calcium and Fracture Risk in Older Adults With Plant-Based Diet: A Longitudinal Study From the China Health and Nutrition Survey. J. Bone Miner. Res. 2016, 31, 2016–2023. [Google Scholar] [CrossRef]
- Kong, S.H.; Kim, J.H.; Hong, A.R.; Cho, N.H.; Shin, C.S. Dietary calcium intake and risk of cardiovascular disease, stroke, and fracture in a population with low calcium intake. Am. J. Clin. Nutr. 2017, 106, 27–34. [Google Scholar] [CrossRef]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; Declerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT–Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Hodges, J.K.; Cao, S.; Cladis, D.P.; Weaver, C.M. Lactose Intolerance and Bone Health: The Challenge of Ensuring Adequate Calcium Intake. Nutrients 2019, 11, 718. [Google Scholar] [CrossRef]
- Weaver, C.M.; Stone, M.S.; Lobene, A.J.; Cladis, D.P.; Hodges, J.K. What Is the Evidence Base for a Potassium Requirement? Nutr. Today 2018, 53, 184–195. [Google Scholar] [CrossRef]
- Egg, S.; Erler, J.; Purtscher, A.-E. Tiroler Ernährungsbericht; Fhg-Zentrum für Gesundheitsberufe Tirol GmbH: Innsbruck, Austria, 2019. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Electrolytes | Women | Men |
|---|---|---|
| Sodium | 1500 | 1500 |
| Potassium | 4000 | 4000 |
| Calcium | 1000 | 1000 |
| Magnesium | ||
| age 18–24 years | 310 | 400 |
| age 25–64 years | 300 | 350 |
| Characteristics | Women | Men | Total |
|---|---|---|---|
| n | 235 | 228 | 463 |
| Age, years * | 41.0 (12.9) | 39.9 (12.9) | 40.4 (12.9) |
| Height, cm | 166.7 (5.9) | 178.9 (7.2) | 172.7 (8.9) |
| Weight, kg | 65.5 (13.4) | 81.4 (14.6) | 73.3 (16.1) |
| Waist circumference, cm | 85.9 (11.71) | 91.39 (11.8) | 88.6 (12.9) |
| Hip circumference, cm | 100.2 (10.1) | 100.9 (7.4) | 100.5 (8.9) |
| Waist-to-hip ratio | 0.86 (0.06) | 0.90 (0.07) | 0.88 (0.07) |
| BMI, kg/m2 | 23.6 (4.9) | 25.4 (4.0) | 24.5 (4.5) |
| Overweight/obese, % | 28.9 | 45.6 | 37.3 |
| Smoking, % | 21.7 | 26.8 | 24.3 |
| Migration background **, % | 23.8 | 23.2 | 23.5 |
| Education, % | |||
| Elementary school | 0.4 | 0.0 | 0.2 |
| Secondary school | 0.9 | 0.9 | 0.9 |
| Apprenticeship | 14.6 | 26.6 | 20.4 |
| Professional school | 17.2 | 9.0 | 13.2 |
| School with higher education (Matura) | 19.7 | 24.3 | 22.0 |
| University | 34.8 | 31.1 | 33.0 |
| Other | 12.4 | 8.1 | 10.3 |
| Occupation, % | |||
| Full-time | 63.9 | 86.8 | 75.8 |
| Part-time | 36.1 | 13.2 | 24.2 |
| Characteristics | Sodium | p-Value 1 | Potassium | p-Value | Calcium | p-Value | Magnesium | p-Value |
|---|---|---|---|---|---|---|---|---|
| gender * | ||||||||
| women | 2412.0 (58.9) | 3041.8 (63.5) | 983.6 (23.3) | 354.1 (7.6) | ||||
| men | 2639.8 (59.9) | 0.011 | 2824.7 (64.6) | 0.024 | 977.5 (23.7) | 0.862 | 352.5 (7.7) | 0.887 |
| age groups ** | 0.31 | 0.658 | 0.034 | 0.319 | ||||
| 18–24 years | 2487.9 (98.9) | 2922.9 (106.1) | 1048.1 (38.8) | 365.5 (12.7) | ||||
| 25–50 years | 2575.7 (51.6) | 2961.7 (55.3) | 987.7 (20.3) | 355.0 (6.6) | ||||
| 51–64 years | 2438.7 (77.9) | 2870.4 (83.6) | 921.0 (30.6) | 341.4 (10.0) | ||||
| women * | 0.083 | 0.335 | 0.18 | 0.184 | ||||
| 18–24 years | 2044.7 (107.9) | 2760.8 (131.3) | 946.1 (46.4) | 339.7 (15.7) | ||||
| 25–50 years | 2159.9 (57.9) | 2648.0 (70.5) | 860.6 (24.9) | 308.8 (8.4) | ||||
| 51–64 years | 1928.8 (86.5) | 2829.0 (105.2) | 840.5 (37.2) | 325.1 (12.6) | ||||
| men * | 0.899 | 0.06 | 0.105 | 0.072 | ||||
| 18–24 years | 2926.8 (169.4) | 3090.6 (169.3) | 1145.0 (63.2) | 393.1 (20.3) | ||||
| 25–50 years | 3005.6 (85.8) | 3286.5 (85.7) | 1120.3 (32.0) | 401.8 (10.2) | ||||
| 51–64 years | 2959.5 (131.3) | 2922.2 (131.2) | 1005.3 (49.0) | 358.8 (15.7) |
| Main Food Groups | Sodium | Potassium | Calcium | Magnesium |
|---|---|---|---|---|
| Water and mineral water, unsweetened tea | 1.4 | 0.9 | 12.5 | 6.4 |
| Fruit and vegetable juice | 0.1 | 3.8 | 1.0 | 2.0 |
| Sodas and energy drinks | 0.5 | 0.2 | 1.3 | 1.1 |
| Low sugar beverages, diet soda | 0.1 | 0.9 | 0.3 | 0.4 |
| Coffee and green/black tea | 0.6 | 8.0 | 3.7 | 8.5 |
| Fruits, vegetables and legumes | 5.8 | 26.3 | 7.5 | 14.5 |
| White bread | 13.0 | 2.8 | 3.2 | 5.7 |
| Whole grain bread | 11.4 | 5.0 | 1.8 | 8.1 |
| Refined grains | 5.7 | 3.0 | 2.2 | 5.8 |
| Whole grains | 0.3 | 1.4 | 0.4 | 3.8 |
| Potatoes | 0.6 | 6.2 | 0.7 | 3.0 |
| Milk and milk products | 3.1 | 8.2 | 19.9 | 5.7 |
| Cheese | 9.6 | 2.2 | 29.7 | 3.3 |
| Vegetable oils, nuts and seeds | 0.0 | 1.8 | 0.8 | 4.2 |
| Butter/margarine | 0.1 | 0.1 | 0.1 | 0.1 |
| Eggs | 0.1 | 0.0 | 0.0 | 0.0 |
| Meat and meat products | 11.5 | 7.8 | 1.2 | 5.3 |
| Fish and fish products | 8.9 | 2.6 | 0.6 | 2.2 |
| Sweets, desserts and cakes | 2.5 | 7.8 | 5.8 | 9.0 |
| Salty snacks and fast food | 1.5 | 2.1 | 0.5 | 1.4 |
| Alcoholic beverages | 0.3 | 2.8 | 1.0 | 4.4 |
| Condiments, sauces, spices, artificial sweeteners | 21.6 | 3.6 | 3.5 | 3.7 |
| Others (soy products, plant-based milk, soups, protein drinks, beer/wine alcohol-free) | 0.3 | 2.1 | 1.2 | 2.4 |
| Characteristics and Electrolyte Intake | Health-conscious Dietary Pattern | Traditional Dietary Pattern | Western Dietary Pattern | p-Value |
|---|---|---|---|---|
| n = 118 | n = 295 | n = 50 | ||
| Gender, % of women | 72.9 | 48.8 | 10.0 | <0.001 |
| Age, year * | 39.8 (1.1) | 42.5 (0.7) | 29.9 (1.8) | <0.001 |
| Energy intake, kcal/day ** | 1901.5 (61.7) | 2161.7 (35.0) | 2445.2 (141.2) | <0.001 |
| Electrolyte intake ** | ||||
| Sodium, mg/day | 2113.1 (106.3) | 2594.9 (60.3) | 2899.1 (243.2) | <0.001 |
| Potassium, mg/day | 3289.4 (108.2) | 2688.8 (61.4) | 3285.5 (247.6) | <0.001 |
| Calcium, mg/day | 939.7 (40.2) | 970.2 (22.8) | 1091.1 (91.9) | 0.317 |
| Magnesium, mg/day | 410.3 (12.5) | 321.8 (7.1) | 393.5 (28.6) | <0.001 |
| Main Food Groups | Participants | p-Value | |
|---|---|---|---|
| Group 1 (n = 66) | Group 2 (n = 65) | ||
| Water and mineral water, unsweetened tea | 1410.2 ± 138.6 | 1952.5 ± 131.1 | 0.002 |
| Sodas and energy drinks | 423.5 ± 54.5 | 100.8 ± 51.6 | 0.002 |
| Fruits and vegetables and legumes | 199.5 ± 37.4 | 508.3 ± 35.4 | <0.001 |
| White bread | 86.3 ±9.0 | 32.6 ± 8.4 | 0.001 |
| Milk and milk products | 70.4 ± 25.0 | 284.2 ± 23.6 | <0.001 |
| Cheese | 32.8 ± 11.7 | 97.6 ± 11.0 | 0.004 |
| Vegetable oils. nuts and seeds | 7.7 ± 3.3 | 24.3 ± 3.1 | 0.046 |
| Butter/margarine | 12.8 ± 1.6 | 8.0± 1.5 | 0.013 |
| Sweets. desserts and cakes | 149.00 ± 16.3 | 80.5 ± 15.4 | 0.034 |
| Others (soy products, plant-based milk, soups, protein drinks, beer/wine alcohol-free) | 72.1 ± 28.0 | 208.7 ± 26.5 | 0.022 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schiefermeier-Mach, N.; Egg, S.; Erler, J.; Hasenegger, V.; Rust, P.; König, J.; Purtscher, A.E. Electrolyte Intake and Major Food Sources of Sodium, Potassium, Calcium and Magnesium among a Population in Western Austria. Nutrients 2020, 12, 1956. https://doi.org/10.3390/nu12071956
Schiefermeier-Mach N, Egg S, Erler J, Hasenegger V, Rust P, König J, Purtscher AE. Electrolyte Intake and Major Food Sources of Sodium, Potassium, Calcium and Magnesium among a Population in Western Austria. Nutrients. 2020; 12(7):1956. https://doi.org/10.3390/nu12071956
Chicago/Turabian StyleSchiefermeier-Mach, Natalia, Sabrina Egg, Judith Erler, Verena Hasenegger, Petra Rust, Jürgen König, and Anna Elisabeth Purtscher. 2020. "Electrolyte Intake and Major Food Sources of Sodium, Potassium, Calcium and Magnesium among a Population in Western Austria" Nutrients 12, no. 7: 1956. https://doi.org/10.3390/nu12071956
APA StyleSchiefermeier-Mach, N., Egg, S., Erler, J., Hasenegger, V., Rust, P., König, J., & Purtscher, A. E. (2020). Electrolyte Intake and Major Food Sources of Sodium, Potassium, Calcium and Magnesium among a Population in Western Austria. Nutrients, 12(7), 1956. https://doi.org/10.3390/nu12071956