Obesity, Insulin Resistance, and Hyperandrogenism Mediate the Link between Poor Diet Quality and Ovarian Dysmorphology in Reproductive-Aged Women

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Ethical Approval
2.3. Study Participants
2.4. Study Procedures
2.4.1. Clinical Assessments
2.4.2. Biochemical Analyses
2.4.3. Ultrasonographic Assessments of Ovarian morphology
2.4.4. Dietary Assessments
2.4.5. Statistical Analyses
3. Results
3.1. Descriptive Statistics of Participants
3.2. Correlations between Dietary Patterns
3.3. Direct Associations
3.3.1. Direct Associations between Dietary Patterns and Ovarian Characteristics
3.3.2. Associations between Dietary Patterns and Metabolic and Reproductive Measures (Path a)
3.3.3. Associations between Metabolic and Reproductive Profiles and Ovarian Characteristics (Path b)
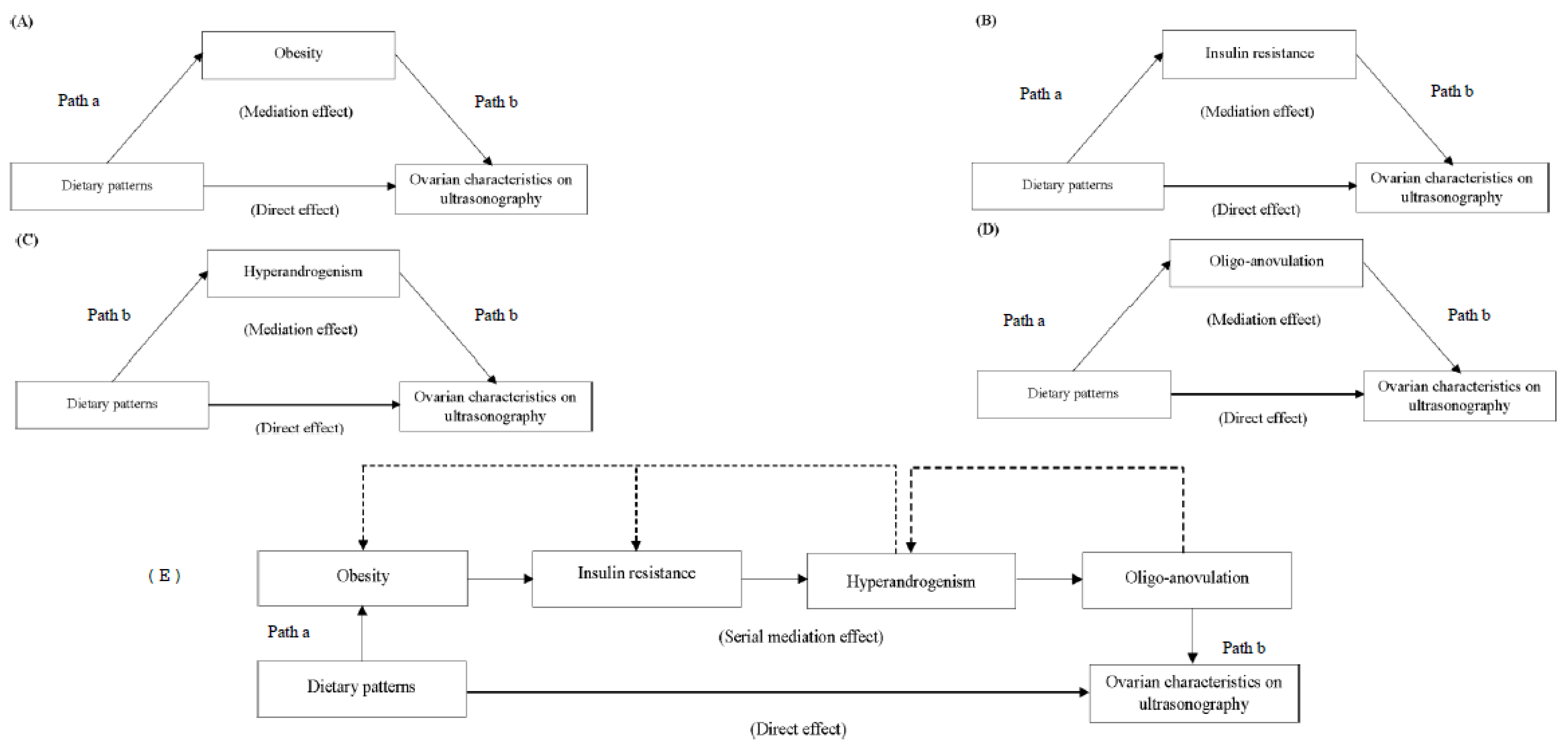
3.4. Indirect Associations
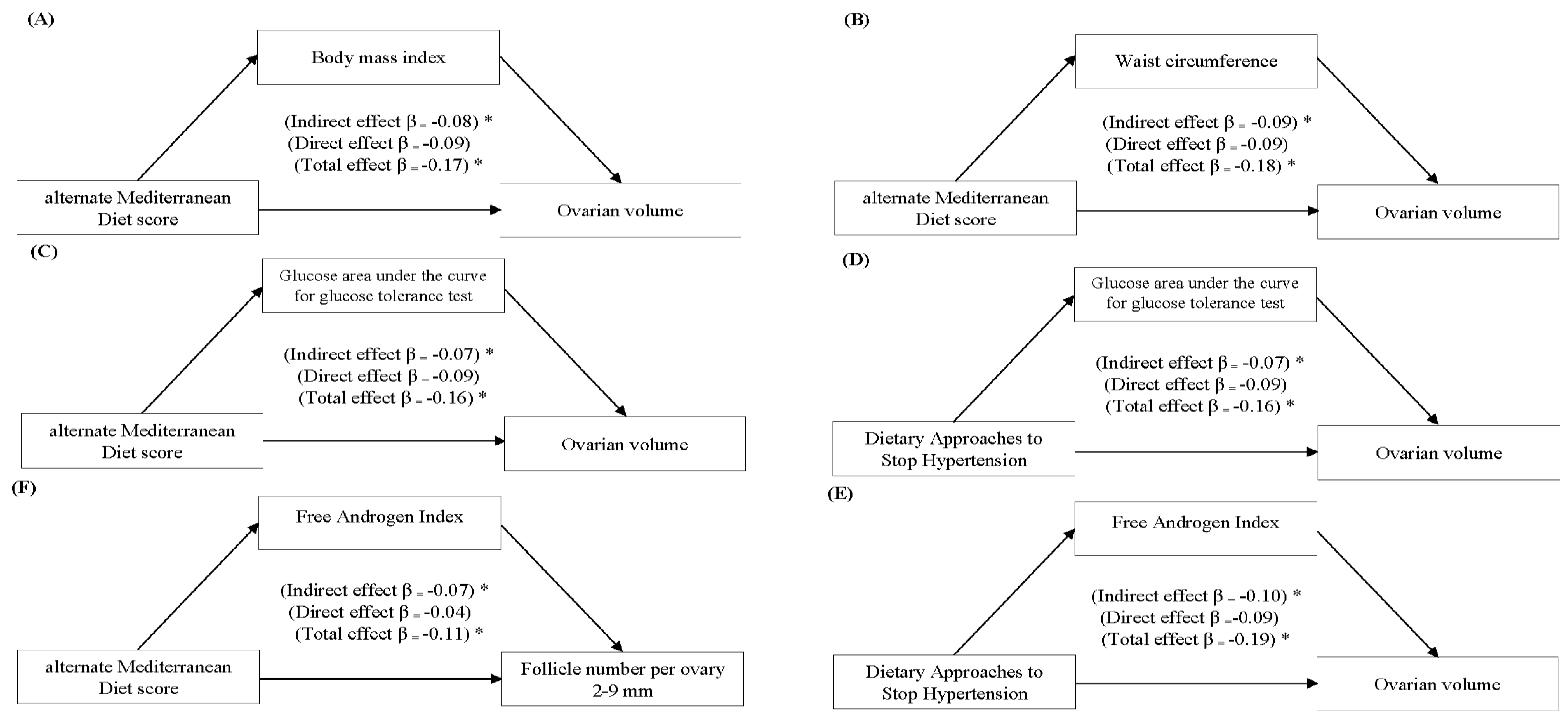
3.4.1. Simple Mediation Analyses Evaluating Associations between Dietary Patterns and Ovarian Characteristics
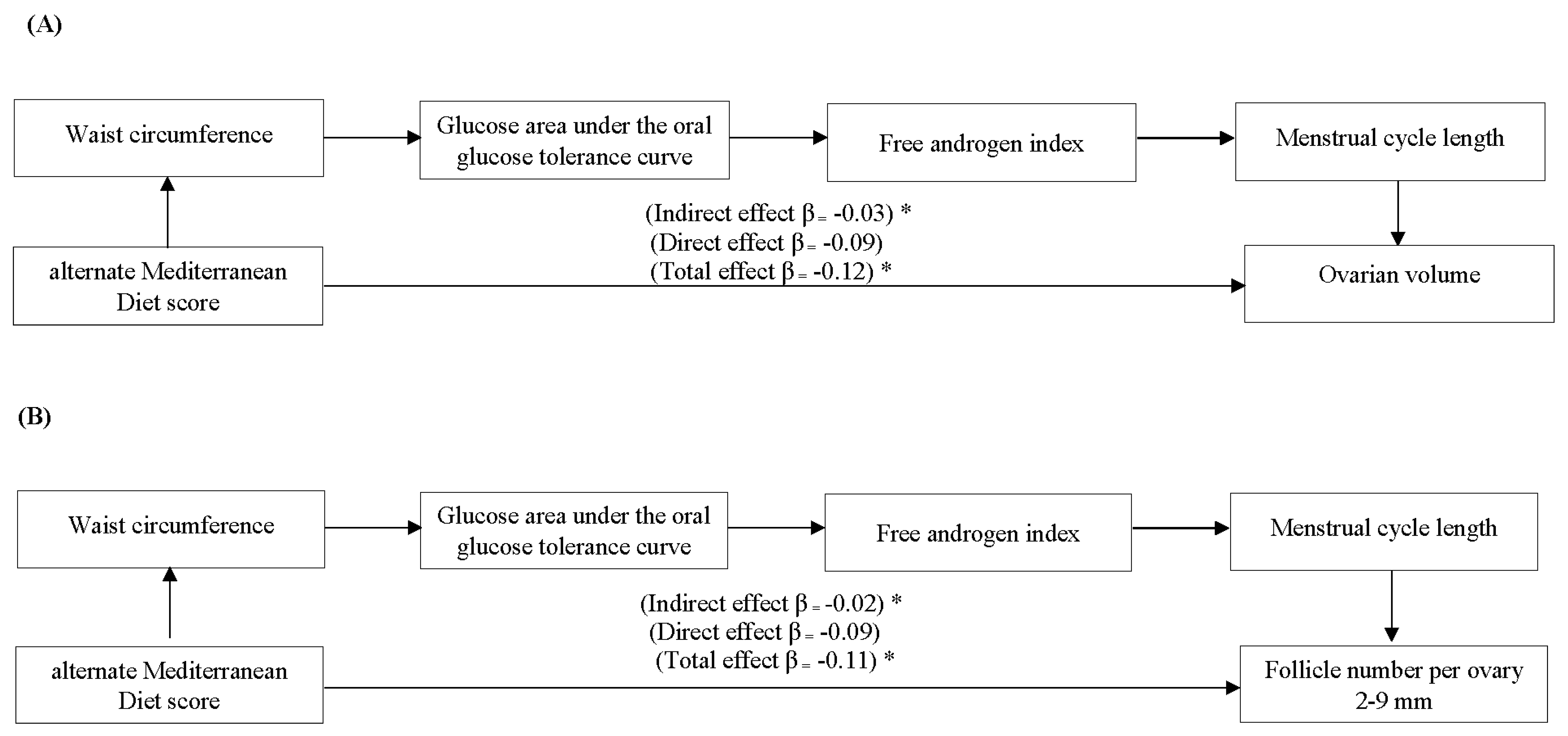
3.4.2. Serial Mediation Analyses Evaluating Associations between Dietary Patterns and Ovarian Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Esmaillzadeh, A.; Azadbakht, L. Major dietary patterns in relation to general obesity and central adiposity among Iranian women. J. Nutr. 2008, 138, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Randall, E.; Marshall, J.; Graham, S.; Brasure, J. Patterns in food use and their associations with nutrient intakes. Am. J. Clin. Nutr. 1990, 52, 739–745. [Google Scholar] [CrossRef]
- Howard, B.V.; Aragaki, A.K.; Tinker, L.F.; Allison, M.; Hingle, M.D.; Johnson, K.C.; MansonJ, E.; Shadyab, A.H.; Shikany, J.M.; Snetselaar, L.G.; et al. A low-fat dietary pattern and diabetes: A secondary analysis from the Women’s Health Initiative Dietary Modification Trial. Diabetes Care 2018, 41, 680–687. [Google Scholar] [CrossRef] [PubMed]
- George, S.M.; Ballard-Barbash, R.; Manson, J.E.; Reedy, J.; Shikany, J.M.; Subar, A.F.; Tinker, L.F.; Vitolins, M.; Neuhouser, M.L. Comparing indices of diet quality with chronic disease mortality risk in postmenopausal women in the Women’s Health Initiative Observational Study: Evidence to inform national dietary guidance. Am. J. Epidemiol. 2014, 180, 616–625. [Google Scholar] [CrossRef]
- Fung, T.T.; Hu, F.B.; McCullough, M.L.; Newby, P.; Willett, W.C.; Holmes, M.D. Diet quality is associated with the risk of estrogen receptor–negative breast cancer in postmenopausal women. J. Nutr. 2006, 136, 466–472. [Google Scholar] [CrossRef]
- Qin, B.; Moorman, P.G.; Kelemen, L.E.; Alberg, A.J.; Barnholtz-Sloan, J.S.; Bondy, M.; Cote, M.L.; Funkhouser, E.; Peters, E.S.; Schwartz, A.G. Dietary quality and ovarian cancer risk in African-American women. Am. J. Epidemiol. 2017, 185, 1281–1289. [Google Scholar] [CrossRef]
- Gaskins, A.J.; Rich-Edwards, J.W.; Hauser, R.; Williams, P.L.; Gillman, M.W.; Penzias, A.; Missmer, S.A.; Chavarro, J.E. Prepregnancy dietary patterns and risk of pregnancy loss. Am. J. Clin. Nutr. 2014, 100, 1166–1172. [Google Scholar] [CrossRef]
- Vujkovic, M.; de Vries, J.H.; Lindemans, J.; Macklon, N.S.; van der Spek, P.J.; Steegers, E.A.P.; Steegers-Theunissen, R.P.M. The preconception Mediterranean dietary pattern in couples undergoing in vitro fertilization/intracytoplasmic sperm injection treatment increases the chance of pregnancy. Fertil. Steril. 2010, 94, 2096–2101. [Google Scholar] [CrossRef]
- Toledo, E.; Lopez-del Burgo, C.; Ruiz-Zambrana, A.; Donazar, M.; Navarro-Blasco, Í.; Martínez-González, M.A.; de Irala, J. Dietary patterns and difficulty conceiving: A nested case–control study. Fertil. Steril. 2011, 96, 1149–1153. [Google Scholar] [CrossRef] [PubMed]
- Grieger, J.A.; Grzeskowiak, L.E.; Bianco-Miotto, T.; Jankovic-Karasoulos, T.; Moran, L.J.; Wilson, R.L.; Leemaqz, S.Y.; Poston, L.; McCowan, L.; Kenny, L.C.; et al. Pre-pregnancy fast food and fruit intake is associated with time to pregnancy. Hum. Reprod. 2018, 33, 1063–1070. [Google Scholar] [CrossRef]
- Moran, L.; Grieger, J.; Mishra, G.; Teede, H. The association of a Mediterranean-style diet pattern with polycystic ovary syndrome status in a community cohort study. Nutrients 2015, 7, 8553–8564. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, T.B.; Osterdal, M.L.; Knudsen, V.K.; Haugen, M.; Meltzer, H.M.; Bakketeig, L.; Olsen, S.F. Association between a Mediterranean-type diet and risk of preterm birth among Danish women: A prospective cohort study. Acta Obstet. Gynecol. Scand. 2008, 87, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Coelho, N.; de, L.; Cunha, D.B.; Esteves, A.P.; Lacerda, E.M.; Theme Filha, M.M. Dietary patterns in pregnancy and birth weight. Rev. Saude Publica 2015, 49, 62. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhao, D.; Mao, X.; Xia, Y.; Baker, P.N.; Zhang, H. Maternal dietary patterns and pregnancy outcome. Nutrients 2016, 8, 351. [Google Scholar] [CrossRef] [PubMed]
- Hodge, A.; Bassett, J. What can we learn from dietary pattern analysis? Public Health Nutr. 2016, 19, 191–194. [Google Scholar] [CrossRef]
- Slattery, M.L.; Boucher, K.M. The senior authors’ response: Factor analysis as a tool for evaluating eating patterns. Am. J. Epidemiol. 1998, 148, 20–21. [Google Scholar] [CrossRef]
- Zamora, D.; Gordon-Larsen, P.; Jacobs, D.R., Jr.; Popkin, B.M. Diet quality and weight gain among black and white young adults: The Coronary Artery Risk Development in Young Adults (CARDIA) Study (1985–2005). Am. J. Clin. Nutr. 2010, 92, 784–793. [Google Scholar] [CrossRef]
- Xiao, R.S.; Moore Simas, T.A.; Pagoto, S.L.; Person, S.D.; Rosal, M.C.; Waring, M.E. Sleep duration and diet quality among women within 5 years of childbirth in the United States: A cross-sectional study. Matern. Child Health J. 2016, 20, 1869–1877. [Google Scholar] [CrossRef]
- Laster, L.E.; Lovelady, C.A.; West, D.G.; Wiltheiss, G.A.; Brouwer, R.J.M.; Ostbye, T. Diet quality of overweight and obese mothers and their preschool children. J. Acad. Nutr. Diet. 2013, 113, 1476–1483. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kazemi, M.; McBreairty, L.E.; Chizen, D.R.; Pierson, R.A.; Chilibeck, P.D.; Zello, G.A. A comparison of a pulse-based diet and the Therapeutic Lifestyle Changes diet in combination with exercise and health counselling on the cardio-metabolic risk profile in women with polycystic ovary syndrome: A randomized controlled trial. Nutrients 2018, 10, 1387. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Kruszon-Moran, D.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Trends in obesity among adults in the United States, 2005 to 2014. J. Am. Med. Assoc. 2016, 315, 2284–2291. [Google Scholar] [CrossRef] [PubMed]
- Franks, S.; Mason, H.; White, D.; Willis, D. Etiology of anovulation in polycystic ovary syndrome. Steroids 1998, 63, 306–307. [Google Scholar] [CrossRef]
- NestlerJ, E. Obesity, insulin, sex steroids and ovulation. Int. J. Obes. 2000, 24, S71–S73. [Google Scholar] [CrossRef]
- Gambineri, A.; Laudisio, D.; Marocco, C.; Radellini, S.; Colao, A.; Savastano, S. On behalf of the Obesity Programs of nutrition, Education Research Assessment, group. Female infertility: Which role for obesity? Int. J. Obes. 2019, 9, 65–72. [Google Scholar] [CrossRef]
- Sohrabi, M.; Roushandeh, A.M.; Alizadeh, Z.; Vahidinia, A.M.M. Effect of a high fat diet on ovary morphology, in vitro development, in vitro fertilisation rate and oocyte quality in mice. Singap. Med. J. 2015, 56, 573–579. [Google Scholar] [CrossRef]
- Hilal, G.; Fatma, T.; Ferruh, Y.; Sabire, G.; Yüksel, A. Effect of high-fat diet on the various morphological parameters of the ovary. Anat. Cell Biol. 2020, 53, 58–67. [Google Scholar] [CrossRef]
- Wang, N.; Luo, L.-L.; Xu, J.-J.; Xu, M.-Y.; Zhang, X.-M.; Zhou, X.-L.; Liu, W.-J.; Fu, Y.-C. Obesity accelerates ovarian follicle development and follicle loss in rats. Metabolism 2014, 63, 94–103. [Google Scholar] [CrossRef]
- Wu, L.L.-Y.; Dunning, K.R.; Yang, X.; Russell, D.L.; Lane, M.; Norman, R.J.; Robker, R.L. High-fat diet causes lipotoxicity responses in cumulus–oocyte complexes and decreased fertilization rates. Endocrinol 2010, 151, 5438–5445. [Google Scholar] [CrossRef]
- Zhuo, Y.; Hua, L.; Feng, B.; Jiang, X.; Li, J.; Jiang, D.; Huang, X.; Zhu, Y.; Li, Z.; Yan, L.; et al. Fibroblast growth factor 21 coordinates adiponectin to mediate the beneficial effects of low-protein diet on primordial follicle reserve. EBioMedicine 2019, 41, 623–635. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; McGee, W.K.; Bishop, C.V.; Park, B.S.; Cameron, J.L.; Zelinski, M.B.; Stouffer, R.L. Exposure of female macaques to Western-style diet with or without chronic T in vivo alters secondary follicle function during encapsulated 3-dimensional culture. Endocrinol 2015, 156, 1133–1142. [Google Scholar] [CrossRef] [PubMed]
- Newell-Fugate, A.E.; Taibl, J.N.; Clark, S.G.; Alloosh, M.; Sturek, M.; Krisher, R.L. Effects of diet-induced obesity on metabolic parameters and reproductive function in female Ossabaw minipigs. Comp. Med. 2014, 64, 44–49. [Google Scholar] [PubMed]
- Moslehi, N.; Mirmiran, P.; Tehrani, F.R.; Azizi, F. Current evidence on associations of nutritional factors with ovarian reserve and timing of menopause: A systematic review. Adv. Nutr. 2017, 8, 597–612. [Google Scholar] [PubMed]
- Franks, S.; McCarthy, M.I.; Hardy, K. Development of polycystic ovary syndrome: Involvement of genetic and environmental factors. Int. J. Androl. 2006, 29, 278–285. [Google Scholar] [CrossRef]
- Franks, S.; Stark, J.; Hardy, K. Follicle dynamics and anovulation in polycystic ovary syndrome. Hum. Reprod. Update 2008, 14, 367–378. [Google Scholar] [CrossRef]
- Diamanti-Kandarakis, E.; Dunaif, A. Insulin resistance and the polycystic ovary syndrome revisited: An update on mechanisms and implications. Endocr. Rev. 2012, 33, 981–1030. [Google Scholar] [CrossRef]
- McCartney, C.R.; Marshall, J.C. Polycystic ovary syndrome. N. Engl. J. Med. 2016, 375, 54–64. [Google Scholar] [CrossRef]
- Escobar-Morreale, H.F.; Luque-Ramírez, M.; San Millán, J.L. The molecular-genetic basis of functional hyperandrogenism and the polycystic ovary syndrome. Endocr. Rev. 2005, 26, 251–282. [Google Scholar] [CrossRef]
- Maciel, G.A.; Baracat, E.C.; Benda, J.A.; Markham, S.M.; Hensinger, K.; Chang, R.J.; Erickson, G.F. Stockpiling of transitional and classic primary follicles in ovaries of women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2004, 89, 5321–5327. [Google Scholar] [CrossRef]
- Lujan, M.E.; Jarrett, B.Y.; Brooks, E.D.; Reines, J.K.; Peppin, A.K.; Muhn, N.; Haider, E.; Pierson, R.A.; Chizen, D.R. Updated ultrasound criteria for polycystic ovary syndrome: Reliable thresholds for elevated follicle population and ovarian volume. Hum. Reprod. 2013, 28, 1361–1368. [Google Scholar] [CrossRef] [PubMed]
- Lujan, M.E.; Brooks, E.D.; Kepley, A.L.; Chizen, D.R.; Pierson, R.A.; Peppin, A.K. Grid analysis improves reliability in follicle counts made by ultrasonography in women with polycystic ovary syndrome. Ultrasound Med. Biol. 2010, 36, 712–718. [Google Scholar] [CrossRef] [PubMed]
- Dewailly, D.; Lujan, M.E.; Carmina, E.; Cedars, M.I.; Laven, J.; Norman, R.J.; Escobar-Morreale, H.F. Definition and significance of polycystic ovarian morphology: A task force report from the Androgen Excess and Polycystic Ovary Syndrome Society. Hum. Reprod. Update 2014, 20, 334–352. [Google Scholar] [CrossRef] [PubMed]
- Christ, J.P.; Willis, A.D.; Brooks, E.D.; Vanden, B.H.; Jarrett, B.Y.; Pierson, R.A.; Chizen, D.R.; Lujan, M.E. Follicle number, not assessments of the ovarian stroma, represents the best ultrasonographic marker of polycystic ovary syndrome. Fertil. Steril. 2014, 101, 280–287.e1. [Google Scholar] [CrossRef] [PubMed]
- Christ, J.P.; Vanden, B.H.; Brooks, E.D.; Pierson, R.A.; Chizen, D.R.; Lujan, M.E. Ultrasound features of polycystic ovaries relate to degree of reproductive and metabolic disturbance in polycystic ovary syndrome. Fertil. Steril. 2015, 103, 787–794. [Google Scholar] [CrossRef]
- Kazemi, M.; Pierson, R.A.; McBreairty, L.E.; Chilibeck, P.D.; Zello, G.A.; Chizen, D.R. A randomized controlled trial of a lifestyle intervention with longitudinal follow up on ovarian dysmorphology in women with polycystic ovary syndrome. Clin. Endocrinol. 2020, 92, 525–535. [Google Scholar] [CrossRef]
- Kazemi, M.; Pierson, R.; Lujan, M.; Chilibeck, P.; McBreairty, L.; Gordon, J.; Serrao, S.; Zello, G.D. Evaluation of type 2 diabetes and cardiovascular disease risk factors in reproductive-age women with polycystic ovary syndrome (PCOS) using the 2014 Androgen Excess and PCOS Society Criteria for the polycystic ovarian morphology (MON-213). JES 2019, 3 (Suppl. 1), MON-213. [Google Scholar] [CrossRef]
- Lujan, M.E.; Kepley, A.L.; Chizen, D.R.; Lehotay, D.C.; Pierson, R.A. Development of morphologically dominant follicles is associated with fewer metabolic disturbances in amenorrheic women with polycystic ovary syndrome: A pilot study. Ultrasound Obstet. Gynecol. 2010, 36, 759–766. [Google Scholar] [CrossRef]
- Scheffer, G.J.; Broekmans, F.J.M.; Looman, C.W.N.; Blankenstein, M.; Fauser, B.C.J.M.; de Jong, F.H.; te Velde, E.R. The number of antral follicles in normal women with proven fertility is the best reflection of reproductive age. Hum. Reprod. 2003, 18, 700–706. [Google Scholar] [CrossRef]
- Pierson, R.A. Chapter 3. Human folliculogenesis revisited: The menstrual cycle visualized by ultrasonography. In The Ovary, 3rd ed.; Leung, P.C.K., Adashi, E.Y., Eds.; Academic Press: Cambridge, MA, USA, 2019; pp. 51–69. [Google Scholar]
- O’Rourke, H.P.; MacKinnon, D.P. Reasons for testing mediation in the absence of an intervention effect: A research imperative in prevention and intervention research. J. Stud. Alcohol. Drugs 2018, 79, 171–181. [Google Scholar] [CrossRef]
- Lockwood, C.M.; DeFrancesco, C.A.; Elliot, D.L.; Beresford, S.A.A.; Toobert, D.J. Mediation analyses: Applications in nutrition research and reading the literature. J. Am. Diet. Assoc. 2010, 110, 753–762. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lin, A.W.; Kazemi, M.; Jarrett, B.Y.; Vanden, B.H.; Hoeger, K.M.; Spandorfer, S.D.; Lujan, M.E. Dietary and physical activity behaviors in women with polycystic ovary syndrome per the new International Evidence-Based Guideline. Nutrients 2019, 11, 2711. [Google Scholar] [CrossRef] [PubMed]
- Ferriman, D.; Gallwey, J.D. Clinical assessment of body hair growth in women. J. Clin. Endocrinol. Metab. 1961, 21, 1440–1447. [Google Scholar] [CrossRef] [PubMed]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J. On behalf of the International PCOS Network. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum. Reprod. 2018, 33, 1602–1618. [Google Scholar] [CrossRef]
- Zawadski, J.K.; Dunaif, A. Diagnostic criteria for polycystic ovary syndrome: Towards a rational approach. In Polycystic Ovary Syndrome; Dunaif, A., Givens, J.R., Haseltine, F., Eds.; Black-well Scientific Publications: Boston, MA, USA, 1992; pp. 377–384. [Google Scholar]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Tai, M.M. A mathematical model for the determination of total area under glucose tolerance and other metabolic curves. Diabetes Care 1994, 17, 152–154. [Google Scholar] [CrossRef]
- Pruessner, J.C.; Kirschbaum, C.; Meinlschmid, G.; Hellhammer, D.H. Two formulas for computation of the area under the curve represent measures of total hormone concentration versus time-dependent change. Psychoneuroendocrinology 2003, 28, 916–931. [Google Scholar] [CrossRef]
- Clark, A.F.; Marcellus, S.; deLory, B.; Bird, C.E. Plasma testosterone free index: A better indicator of plasma androgen activity? Fertil. Steril. 1975, 26, 1001–1005. [Google Scholar] [CrossRef]
- Balen, A.H.; Laven, J.S.E.; Tan, S.L.; Dewailly, D. Ultrasound assessment of the polycystic ovary: International consensus definitions. Hum. Reprod. Update 2003, 9, 505–514. [Google Scholar] [CrossRef]
- VioScreen. VIOCARE® Website. Available online: https://www.viocare.com/vioscreen.html (accessed on 25 December 2018).
- Kristal, A.R.; Kolar, A.S.; Fisher, J.L.; Plascak, J.J.; Stumbo, P.J.R.; Paskett, E.D. Evaluation of web-based, self-administered, graphical food frequency questionnaire. J. Acad. Nutr. Diet. 2014, 114, 613–621. [Google Scholar] [CrossRef]
- Deierlein, A.L.; Bihuniak, J.D.; Nagi, E.; Litvak, J.; Victoria, C.; Braune, T.; Weiss, R.; Parekh, N. Development of a technology-assisted food frequency questionnaire for elementary and middle school children: Findings from a pilot study. Nutrients 2019, 11, 1103. [Google Scholar] [CrossRef] [PubMed]
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the healthy eating index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef] [PubMed]
- Panizza, C.E.; Shvetsov, Y.B.; Harmon, B.E.; Wilkens, L.R.; Le Marchand, L.; Haiman, C.; Reedy, J.; Boushey, C.J. Testing the predictive validity of the Healthy Eating Index-2015 in the multiethnic cohort: Is the score associated with a reduced risk of all-cause and cause-specific mortality? Nutrients 2018, 10, 452. [Google Scholar] [CrossRef]
- Reedy, J.; Mitrou, P.; Krebs-Smith, S.; Wirfält, E.; Flood, A.; Kipnis, V.; Leitzmann, M.; Mouw, T.; Hollenbeck, A.A. Index-based dietary patterns and risk of colorectal cancer: The NIH-AARP Diet and Health Study. Am. J. Epidemiol. 2008, 168, 38–48. [Google Scholar] [CrossRef]
- Chiuve, S.E.; Fung, T.T.; Rimm, E.B.; Hu, F.B.; McCullough, M.L.; Wang, M.; Stampfer, M.J.; Willett, W.C. Alternative dietary indices both strongly predict risk of chronic disease. J. Nutr. 2012, 142, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; Chiuve, S.E.; McCullough, M.L.; Rexrode, K.M.; Logroscino, G.; Hu, F.B. Adherence to a DASH-style diet and risk of coronary heart disease and stroke in women. Arch. Intern. Med. 2008, 168, 713–720. [Google Scholar] [CrossRef] [PubMed]
- 2015–2020 Dietary Guidelines for Americans, 8th ed.; Office of Disease Prevention and Health Promotion Website, Skyhorse Publishing Inc.: Washington, DC, USA, 2015. Available online: http://health.gov/dietaryguidelines/2015 (accessed on 25 January 2019).
- Reedy, J.; Lerman, J.L.; Krebs-Smith, S.M.; Kirkpatrick, S.I.; Pannucci, T.E.; Wilson, M.M.; Subar, A.F.; Kahle, L.L.; Tooze, J.A. Evaluation of the Healthy Eating Index-2015. J. Acad. Nutr. Diet. 2018, 118, 1622–1633. [Google Scholar] [CrossRef]
- Guenther, P.M.; Casavale, K.O.; Reedy, J.; Kirkpatrick, S.I.; Hiza, H.A.B.; Kuczynski, K.J.; Kahle, L.L.; Krebs-Smith, S.M. Update of the Healthy Eating Index: HEI-2010. J. Acad. Nutr. Diet. 2013, 113, 569–580. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Kouris-Blazos, A.; Vassilakou, T.; Gnardellis, C.; Polychronopoulos, E.; Venizelos, M.; Lagiou, P.; Wahlqvist, M.L.; Trichopoulos, D. Diet and survival of elderly Greeks: A link to the past. Am. J. Clin. Nutr. 1995, 61, 1346S–1350S. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Kouris-Blazos, A.; Wahlqvist, M.L.; Gnardellis, C.; Lagiou, P.; Polychronopoulos, E.; Vassilakou, T.L.; Trichopoulos, D. Diet and overall survival in elderly people. BMJ 1995, 311, 1457–1460. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Sacks, F.M.; Svetkey, L.P.; Vollmer, W.M.; Appel, L.J.; Bray, G.A.; Harsha, D.; Obarzanek, E.; Conlin, P.R.; Miller, E.R.; Simons-Morton, D.G. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. N. Engl. J. Med. 2001, 344, 3–10. [Google Scholar] [CrossRef] [PubMed]
- AppelL, J.; Moore, T.J.; Obarzanek, E.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Vogt, T.M.; Cutler, J.A.; Windhauser, M.M. A clinical trial of the effects of dietary patterns on blood pressure. N. Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Zhao, X.; Lynch, J.G.Q., Jr. Reconsidering Baron and Kenny: Myths and truths about mediation analysis. J. Consum. Res. 2010, 37, 197–206. [Google Scholar] [CrossRef]
- Hayes, A.F.; Rockwood, N.J. Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behav. Res. Ther. 2017, 98, 39–57. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Fairchild, A.J.; Fritz, M.S. Mediation analysis. Annu. Rev. Psychol. 2007, 58, 593–614. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; The Guilford Press: New York, NY, USA, 2017. [Google Scholar]
- Jarrett, B.Y.; Lujan, M.E. Impact of hypocaloric dietary intervention on ovulation in obese women with PCOS. Reproduction 2017, 153, R15–R27. [Google Scholar] [CrossRef]
- Kazemi, M.; McBreairty, L.E.; Zello, G.A.; Pierson, R.A.; Gordon, J.J.; Serrao, S.B.; Chilibeck, P.D.; Chizen, D.R. A pulse-based diet and the Therapeutic Lifestyle Changes diet in combination with health counseling and exercise improve health-related quality of life in women with polycystic ovary syndrome: Secondary analysis of a randomized controlled trial. J. Psychosom. Obstet. Gynaecol. 2019, 41, 144–153. [Google Scholar] [CrossRef]
- McBreairty, L.E.; Kazemi, M.; Chilibeck, P.D.; Gordon, J.J.; Chizen, D.R.; Zello, G.A. Effect of a pulse-based diet and aerobic exercise on bone measures and body composition in women with polycystic ovary syndrome: A randomized controlled trial. Bone Rep. 2020, 12, 100248. [Google Scholar] [CrossRef]
- Adams, J.; Franks, S.; Polson, D.W.; Mason, H.D.; Abdulwahid, N.; Tucker, M.; Morris, D.V.; Price, J.; Jacobs, H.S. Multifollicular ovaries: Clinical and endocrine features and response to pulsatile gonadotropin releasing hormone. Lancet 1985, 2, 1375–1379. [Google Scholar] [CrossRef]
- Baerwald, A.R.; Adams, G.P.; Pierson, R.A. Ovarian antral folliculogenesis during the human menstrual cycle: A review. Hum. Reprod. Update 2012, 18, 73–91. [Google Scholar] [CrossRef] [PubMed]
- Webber, L.J.; Stubbs, S.; Stark, J.; Trew, G.; Margara, R.; Hardy, K.S. Formation and early development of follicles in the polycystic ovary. Lancet 2003, 362, 1017–1021. [Google Scholar] [CrossRef]
- Webber, L.J.; Stubbs, S.A.; Stark, J.; Margara, R.A.; Trew, G.H.; Lavery, S.A.; Hardy, K.S. Prolonged survival in culture of preantral follicles from polycystic ovaries. J. Clin. Endocrinol. Metab. 2007, 92, 1975–1978. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, R.L.; Ryan, K.J. Hyperandrogenism, insulin resistance, and acanthosis nigricans syndrome: A common endocrinopathy with distinct pathophysiologic features. Am. J. Obstet. Gynecol. 1983, 147, 90–101. [Google Scholar] [CrossRef]
- Moses, A.C.; Flier, J.S.; Grigorescu, F.; Poretsky, L.; Seibel, M. Distribution and characterization of insulin and insulin-like growth factor I receptors in normal human ovary. J. Clin. Endocrinol. Metab. 1985, 61, 728–734. [Google Scholar]
- Jacobs, S.; Harmon, B.E.; Ollberding, N.J.; Wilkens, L.R.; Monroe, K.R.; Kolonel, L.N.; Le Marchand, L.; Boushey, C.J.G. Among 4 diet quality indexes, only the alternate Mediterranean Diet score is associated with better colorectal cancer survival and only in African American women in the multiethnic cohort. J. Nutr. 2016, 146, 1746–1755. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean Diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef]
- Mirabelli, M.; Chiefari, E.; Arcidiacono, B.; Corigliano, D.M.; Brunetti, F.S.; Maggisano, V.; Russo, D.; Foti, D.P.; Brunetti, A. Mediterranean diet nutrients to turn the tide against insulin resistance and related diseases. Nutrients 2020, 12, 1066. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Roman-Vinas, B.; Sanchez-Villegas, A.; Guasch-Ferre, M.; Corella, D.; La Vecchia, C. Benefits of the Mediterranean diet: Epidemiological and molecular aspects. Mol. Asp. Med. 2019, 67, 1–55. [Google Scholar] [CrossRef]
- Gower, B.A.; Chandler-Laney, P.C.; Ovalle, F.; Goree, L.L.; Azziz, R.; Desmond, R.A.; Granger, W.M.; Goss, A.M.; Bates, G.W. Favourable metabolic effects of a eucaloric lower-carbohydrate diet in women with PCOS. Clin. Endocrinol. 2013, 79, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Douglas, C.C.; Gower, B.A.; Darnell, B.E.; Ovalle, F.; Oster, R.A.; Azziz, R. Role of diet in the treatment of polycystic ovary syndrome. Fertil. Steril. 2006, 85, 679–688. [Google Scholar] [CrossRef] [PubMed]
- Mehrabani, H.H.; Salehpour, S.; Amiri, Z.; Farahani, S.J.; Meyer, B.J.; Tahbaz, F. Beneficial effects of a high-protein, low-glycemic-load hypocaloric diet in overweight and obese women with polycystic ovary syndrome: A randomized controlled intervention study. J. Am. Coll. Nutr. 2012, 31, 117–125. [Google Scholar] [CrossRef] [PubMed]
- MarshK, A.; Steinbeck, K.S.; Atkinson, F.S.; Petocz, P.; Brand-Miller, J.C. Effect of a low glycemic index compared with a conventional healthy diet on polycystic ovary syndrome. Am. J. Clin. Nutr. 2010, 92, 83–92. [Google Scholar] [CrossRef]
- Kazemi, M.; Buddemeyer, S.; Fassett, C.M.; Gans, W.M.; Johnston, K.M.; Lungu, E.; Savelle, R.L.; Tolani, P.N.; Dahl, W.J. Chapter 5. Pulses and prevention and management of chronic disease. In Health Benefits of Pulses; Dahl, W., Ed.; Springer: Cham, Switzerland, 2019; pp. 55–72. [Google Scholar]
- Barrea, L.; Arnone, A.; Annunziata, G.; Muscogiuri, G.; Laudisio, D.; Salzano, C.; Pugliese, G.; Colao, A.; Savastano, S. Adherence to the Mediterranean Diet, dietary patterns and body composition in women with polycystic ovary syndrome (PCOS). Nutrients 2019, 11, 2278. [Google Scholar] [CrossRef]
- Banaszewska, B.; Wrotyńska-Barczyńska, J.; Spaczynski, R.Z.; Pawelczyk, L.; Duleba, A.J. Effects of resveratrol on polycystic ovary syndrome: A double-blind, randomized, placebo-controlled trial. J. Clin. Endocrinol. Metab. 2016, 101, 4322–4328. [Google Scholar] [CrossRef]
- Wong, D.H.; Villanueva, J.A.; Cress, A.B.; Duleba, A.J. Effects of resveratrol on proliferation and apoptosis in rat ovarian theca-interstitial cells. Mol. Hum. Reprod. 2010, 16, 251–259. [Google Scholar] [CrossRef]
- Koh, A.; De Vadder, F.; Kovatcheva-Datchary, P.; Bäckhed, F. From dietary fiber to host physiology: Short-chain fatty acids as key bacterial metabolites. Cell 2016, 165, 1332–1345. [Google Scholar] [CrossRef]
- Pilch, S.M. Center for Food Safety and Applied Nutrition, Federation of American Societies for Experimental Biology, Life Sciences Research Office (contributors). In Physiological Effects and Health Consequences of Dietary Fiber; Life Sciences Research Office, Federation of American Societies for Experimental Biology: Bethesda, Maryland, USA, 1987. [Google Scholar]
- van Bennekum, A.M.; Nguyen, D.V.; Schulthess, G.; Hauser, H.; Phillips, M.C. Mechanisms of cholesterol-lowering effects of dietary insoluble fibres: Relationships with intestinal and hepatic cholesterol parameters. Br. J. Nutr. 2005, 94, 331–337. [Google Scholar] [CrossRef]
- Chibbar, R.N.; Ambigaipalan, P.; Hoover, R. Review: Molecular diversity in pulse seed starch and complex carbohydrates and its role in human nutrition and health. Cereal Chem. 2010, 87, 342–352. [Google Scholar] [CrossRef]
- Ludwig, D.S. The glycemic index: Physiological mechanisms relating to obesity, diabetes, and cardiovascular disease. JAMA 2002, 287, 2414–2423. [Google Scholar] [CrossRef] [PubMed]
- Adlercreutz, H. Lignans and human health. Crit. Rev. Clin. Lab. Sci. 2007, 44, 483–525. [Google Scholar] [CrossRef] [PubMed]
- BioCycle Study, G. Effect of daily fiber intake on reproductive function: The BioCycle Study. Am. J. Clin. Nutr. 2009, 90, 1061–1069. [Google Scholar] [CrossRef]
- Gaskins, A.J.; Rovner, A.J.; Mumford, S.L.; Yeung, E.; Browne, R.W.; Trevisan, M.; Perkins, N.J.; Wactawski-Wende, J.; Schisterman, E.F.; BioCycle Study Group. Adherence to a Mediterranean diet and plasma concentrations of lipid peroxidation in premenopausal women. Am. J. Clin. Nutr. 2010, 92, 1461–1467. [Google Scholar] [CrossRef]
- Cena, H.; Calder, P.C. Defining a healthy diet: Evidence for the role of contemporary dietary patterns in health and disease. Nutrients 2020, 12, 334. [Google Scholar] [CrossRef] [PubMed]
- Wali, J.A.; Jarzebska, N.; Raubenheimer, D.; Simpson, S.J.; Rodionov, R.N.; O’Sullivan, J.F. Cardio-metabolic effects of high-fat diets and their underlying mechanisms-A narrative review. Nutrients 2020, 12, 1505. [Google Scholar] [CrossRef]
- Moszak, M.; Szulińska, M.; Bogdański, P. You are what you eat-The relationship between diet, microbiota, and metabolic disorders-A review. Nutrients 2020, 12, 1096. [Google Scholar] [CrossRef]
- Sturmey, R.; Reis, A.; Leese, H.; McEvoy, T. Role of fatty acids in energy povision during oocyte maturation and early embryo development. Reprod. Domest. Anim. 2009, 44, 50–58. [Google Scholar] [CrossRef]
- Al-Safi, Z.A.; Liu, H.; Carlson, N.E.; Chosich, J.; Harris, M.; Bradford, A.P.; Robledo, C.; Eckel, R.H.; Polotsky, A.J. Omega-3 fatty acid supplementation lowers serum FSH in normal weight but not obese women. J. Clin. Endocrinol. Metab. 2016, 101, 324–333. [Google Scholar] [CrossRef]
- Abdalla, H.; Thum, M.Y. An elevated basal FSH reflects a quantitative rather than qualitative decline of the ovarian reserve. Hum. Reprod. 2004, 19, 893–898. [Google Scholar] [CrossRef]
- Anderson, C.; Mark, P.Y.-M.; Stanczyk, F.Z.; Sandler, D.P.; Nichols, H.B. Dietary factors and serum antimüllerian hormone concentrations in late premenopausal women. Fertil. Steril. 2018, 110, 1145–1153. [Google Scholar] [CrossRef] [PubMed]
- Lerchbaum, E.; Obermayer-Pietsch, B. Vitamin D and fertility: A systematic review. Eur. J. Endocrinol. 2012, 166, 765–778. [Google Scholar] [CrossRef] [PubMed]
- Irani, M.; Merhi, Z. Role of vitamin D in ovarian physiology and its implication in reproduction: A systematic review. Fertil. Steril. 2014, 102, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Anagnostis, P.; Karras, S.; Goulis, D.G. Vitamin D in human reproduction: A narrative review. Int. J. Clin. Pract. 2013, 67, 225–235. [Google Scholar] [CrossRef]
- Abadia, L.; Gaskins, A.J.; Chiu, Y.H.; Williams, P.L.; Keller, M.W.D.; Souter, I.; Hauser, R.; Chavarro, J.E. Environment and Reproductive Health Study Team. Serum 25-hydroxyvitamin D concentrations and treatment outcomes of women undergoing assisted reproduction. Am. J. Clin. Nutr. 2016, 104, 729–735. [Google Scholar]
- Aleyasin, A.; Hosseini, M.A.; Mahdavi, A.; Safdarian, L.; Fallahi, P.; Mohajeri, M.R.; Abbasi, M.; Esfahani, F. Predictive value of the level of vitamin D in follicular fluid on the outcome of assisted reproductive technology. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 159, 132–137. [Google Scholar] [CrossRef]
- Neville, G.; Martyn, F.; Kilbane, M.; O’Riordan, M.; Wingfield, M.; McKenna, M.; McAuliffe, F.M. Vitamin D status and fertility outcomes during winter among couples undergoing in vitro fertilization/intracytoplasmic sperm injection. Int. J. Gynecol. Obstet. 2016, 135, 172–176. [Google Scholar] [CrossRef]
- Souter, I.; Chiu, Y.-H.; Batsis, M.; Afeiche, M.; Williams, P.; Hauser, R.; Chavarro, J. The association of protein intake (amount and type) with ovarian antral follicle counts among infertile women: Results from the EARTH prospective study cohort. BJOG 2017, 124, 1547–1555. [Google Scholar] [CrossRef]
- Braga, D.P.A.F.; Halpern, G.; Setti, A.S.; Figueira, R.C.S.; Iaconelli, A.; Borges, E. The impact of food intake and social habits on embryo quality and the likelihood of blastocyst formation. Reprod. Biomed. Online 2015, 31, 30–38. [Google Scholar] [CrossRef]
- Chavarro, J.E.; Rich-Edwards, J.W.; Rosner, B.A.; Willett, W.C. Protein intake and ovulatory infertility. Am. J. Obstet. Gynecol. 2008, 198, 210-e1. [Google Scholar] [CrossRef]
- Schulze, M.B.; Manson, J.E.; Ludwig, D.S.; Colditz, G.A.; Stampfer, M.J.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages, weight gain, and incidence of type 2 diabetes in young and middle-aged women. JAMA 2004, 292, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Baudrand, R.; Campino, C.; Carvajal, C.; Olivieri, O.; Guidi, G.; Faccini, G.; Vöhringer, P.; Cerda, J.; Owen, G.; Kalergis, A. High sodium intake is associated with increased glucocorticoid production, insulin resistance and metabolic syndrome. Clin. Endocrinol. 2014, 80, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Yi, S.S.; Firestone, M.J.; Beasley, J.M. Independent associations of sodium intake with measures of body size and predictive body fatness. Obesity 2015, 23, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Samimi, M.; Tabassi, Z.; Shakeri, H.; Sabihi, S.-S.; Esmaillzadeh, A. Effects of DASH diet on lipid profiles and biomarkers of oxidative stress in overweight and obese women with polycystic ovary syndrome: A randomized clinical trial. Nutrition 2014, 30, 1287–1293. [Google Scholar] [CrossRef] [PubMed]
- Azadi-Yazdi, M.; Karimi-Zarchi, M.; Salehi-Abargouei, A.; Fallahzadeh, H.; Nadjarzadeh, A. Effects of Dietary Approach to Stop Hypertension diet on androgens, antioxidant status and body composition in overweight and obese women with polycystic ovary syndrome: A randomised controlled trial. J. Hum. Nutr. Diet. 2017, 30, 275–283. [Google Scholar] [CrossRef]
- Orio, F.; Muscogiuri, G.; Palomba, S. Could the Mediterranean diet be effective in women with polycystic ovary syndrome? A proof of concept. Eur. J. Clin. Nutr. 2015, 69, 974. [Google Scholar] [CrossRef]
- Mena, G.P.; Mielke, G.I.; Brown, W.J. The effect of physical activity on reproductive health outcomes in young women: A systematic review and meta-analysis. Hum. Reprod. Update 2019, 25, 542–564. [Google Scholar] [CrossRef]
- Hayes, A.F. PROCESS: A Versatile Computational Tool for Observed Variable Mediation, Moderation, and Conditional Process Modeling. 2012. Available online: http://www.afhayes.com/public/process2012.pdf (accessed on 5 January 2019).
- Thompson, F.E.; Kirkpatrick, S.I.; Subar, A.F.; Reedy, J.; Schap, T.E.; Wilson, M.M.; Krebs-Smith, S.M. The national cancer institute’s dietary assessment primer: A resource for diet research. J. Acad. Nutr. Diet. 2015, 115, 1986–1995. [Google Scholar] [CrossRef]
- McCarney, R.; Warner, J.; Iliffe, S.; van Haselen, R.; Griffin, M.; Fisher, P. The Hawthorne Effect: A randomised, controlled trial. BMC Med. Res. Methodol. 2007, 7, 30. [Google Scholar] [CrossRef]
- Lujan, M.E.; Chizen, D.R.; Peppin, A.K.; Kriegler, S.; Leswick, D.A.; Bloski, T.G.; Pierson, R.A. Improving inter-observer variability in the evaluation of ultrasonographic features of polycystic ovaries. Reprod. Biol. Endocrinol. 2008, 6, 30. [Google Scholar] [CrossRef]
- Mavrelos, D.; Al Chami, A.; Talaulikar, V.; Burt, E.; Webber, L.; Ploubidis, G.; Yasmin, E. Variation in antral follicle counts at different times in the menstrual cycle: Does it matter? Reprod. BioMed. Online 2016, 33, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Scheffer, G.J.; Broekmans, F.J.; Dorland, M.; Habbema, J.D.; Looman, C.W.; te Velde, E.R. Antral follicle counts by transvaginal ultrasonography are related to age in women with proven natural fertility. Fertil. Steril. 1999, 72, 845–851. [Google Scholar] [CrossRef]
- Hansen, K.R.; Morris, J.L.; Thyer, A.C.; Soules, M.R. Reproductive aging and variability in the ovarian antral follicle count: Application in the clinical setting. Fertil. Steril. 2003, 80, 577–583. [Google Scholar] [CrossRef]
- Bancsi, L.F.; Broekmans, F.J.; Looman, C.W.; Habbema, J.D.; te Velde, E.R. Impact of repeated antral follicle counts on the prediction of poor ovarian response in women undergoing in vitro fertilization. Fertil. Steril. 2004, 81, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Elter, K.; Sismanoglu, A.; Durmusoglu, F. Intercycle variabilities of basal antral follicle count and ovarian volume in subfertile women and their relationship to reproductive aging: A prospective study. Gynecol. Endocrinol. 2005, 20, 137–143. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Orfanos, P.; Norat, T.; Bueno-de-Mesquita, B.; Ocke, M.C.; Peeters, P.H.; van der Schouw, Y.T.; Boeing, H.; Hoffmann, K.; Boffetta, P.; et al. Modified Mediterranean diet and survival: EPIC-elderly prospective cohort study. BMJ 2005, 330, 991. [Google Scholar] [CrossRef]
- Du, M.; Liu, S.H.; Mitchell, C.; Fung, T.T. Associations between diet quality scores and risk of postmenopausal estrogen receptor-negative breast cancer: A systematic review. J. Nutr. 2018, 148, 100–108. [Google Scholar] [CrossRef]
- Ricceri, F.; Giraudo, M.T.; Fasanelli, F.; Milanese, D.; Sciannameo, V.; Fiorini, L.; Sacerdote, C. Diet and endometrial cancer: A focus on the role of fruit and vegetable intake, Mediterranean diet and dietary inflammatory index in the endometrial cancer risk. BMC Cancer 2017, 17, 757. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Measures (Measurement Unit) | Mean (SD) or Number (%) |
|---|---|
| Demographics | |
| Age (y) | 27.8 (6.3) |
| Race (n [%]) | |
| African American | 13 (11.7) |
| Asian | 12 (10.8) |
| White | 73 (65.8) |
| Other | 13 (11.7) |
| DM FHx (n [%]) | 63 (56.8) |
| CVD and/or HTN FHx (n [%]) | 72 (64.9) |
| PCOS Dx (n [%]) | 39 (35.1) |
| Dietary characteristics | |
| Total energy intake (kcal/day) | 2237 (1000) |
| Dietary index | |
| HEI-2015 score | 65.5 (13) |
| aHEI-2010 score | 53.7 (13) |
| aMED score | 4 (2) |
| DASH score | 24 (5) |
| Alcohol intake (g/day) | 8.9 (13) |
| Anthropometric characteristics | |
| BMI (kg/m2) | 30.3 (8.1) |
| WC (cm) | 91.9 (19.7) |
| WHR | 0.84 (0.08) |
| Overweight (n [yes %]) | 56 (50.5) |
| Obesity (n [yes %]) | 18 (16.2) |
| Endocrine measures | |
| Fasting insulin (µIU) | 12.3 (10.1) |
| FPG (mg/dL) | 5.1 (0.5) |
| HOMA-IR index (%) | 2.6 (2.4) |
| Insulin AUC (µIU/mL × 120 min) | 8495 (6167) |
| Glucose AUC (mg/dL × 120 min) | 756 (1.7) |
| TT (nmol/L) | 1.7 (0.7) |
| Estradiol (pmol/L) | 202.4 (120.4) |
| Modified hirsutism score | 6 (5) |
| SHBG (nmol/mL) | 49.8 (34.3) |
| FAI (%) | 5 (4) |
| Menstruation history | |
| Menstrual cycle length (d) | 65 (71) |
| Markers of ovarian morphology | |
| OV (mL) | 9.6 (5.0) |
| FNPO 2–9 mm (n) | 34 (23) |
| Dietary Index | HEI-2015 | aHEI-2010 | aMED | DASH |
|---|---|---|---|---|
| HEI-2015 | 1.00 a | 0.70 a | 0.48 a | 0.53 a |
| aHEI-2010 | 1.00 a | 0.63 a | 0.62 a | |
| aMED | 1.00 a | 0.73 a | ||
| DASH | 1.00 a |
| Measures (Unit) | HEI-2015 | aHEI-2010 | aMED | DASH | ||||
|---|---|---|---|---|---|---|---|---|
| Unstandard βDirect | Standard βDirect | Unstandard βDirect | Standard βDirect | Unstandard βDirect | Standard βDirect | Unstandard βDirect | Standard βDirect | |
| OV (mL) | 0.00 | −0.06 | 0.00 | −0.07 | −0.02 | −0.09 | −0.01 | −0.09 |
| FNPO 2–9 mm (n) | 0.00 | −0.02 | 0.00 | 0.03 | −0.01 | −0.04 | 0.00 | 0.05 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kazemi, M.; Jarrett, B.Y.; Vanden Brink, H.; Lin, A.W.; Hoeger, K.M.; Spandorfer, S.D.; Lujan, M.E. Obesity, Insulin Resistance, and Hyperandrogenism Mediate the Link between Poor Diet Quality and Ovarian Dysmorphology in Reproductive-Aged Women. Nutrients 2020, 12, 1953. https://doi.org/10.3390/nu12071953
Kazemi M, Jarrett BY, Vanden Brink H, Lin AW, Hoeger KM, Spandorfer SD, Lujan ME. Obesity, Insulin Resistance, and Hyperandrogenism Mediate the Link between Poor Diet Quality and Ovarian Dysmorphology in Reproductive-Aged Women. Nutrients. 2020; 12(7):1953. https://doi.org/10.3390/nu12071953
Chicago/Turabian StyleKazemi, Maryam, Brittany Y. Jarrett, Heidi Vanden Brink, Annie W. Lin, Kathleen M. Hoeger, Steven D. Spandorfer, and Marla E. Lujan. 2020. "Obesity, Insulin Resistance, and Hyperandrogenism Mediate the Link between Poor Diet Quality and Ovarian Dysmorphology in Reproductive-Aged Women" Nutrients 12, no. 7: 1953. https://doi.org/10.3390/nu12071953
APA StyleKazemi, M., Jarrett, B. Y., Vanden Brink, H., Lin, A. W., Hoeger, K. M., Spandorfer, S. D., & Lujan, M. E. (2020). Obesity, Insulin Resistance, and Hyperandrogenism Mediate the Link between Poor Diet Quality and Ovarian Dysmorphology in Reproductive-Aged Women. Nutrients, 12(7), 1953. https://doi.org/10.3390/nu12071953