Changes in Free-Living Glycemic Profiles after 12 Months of Lifestyle Intervention in Children with Overweight and with Obesity


Abstract
1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Study Participants
2.3. Participant Characteristics
2.4. Glucose Metabolism
2.5. Cardiovascular Risk Parameters
2.6. Statistical Analysis
3. Results
3.1. Participant Characteristics at Baseline and after 12 Months of Intervention
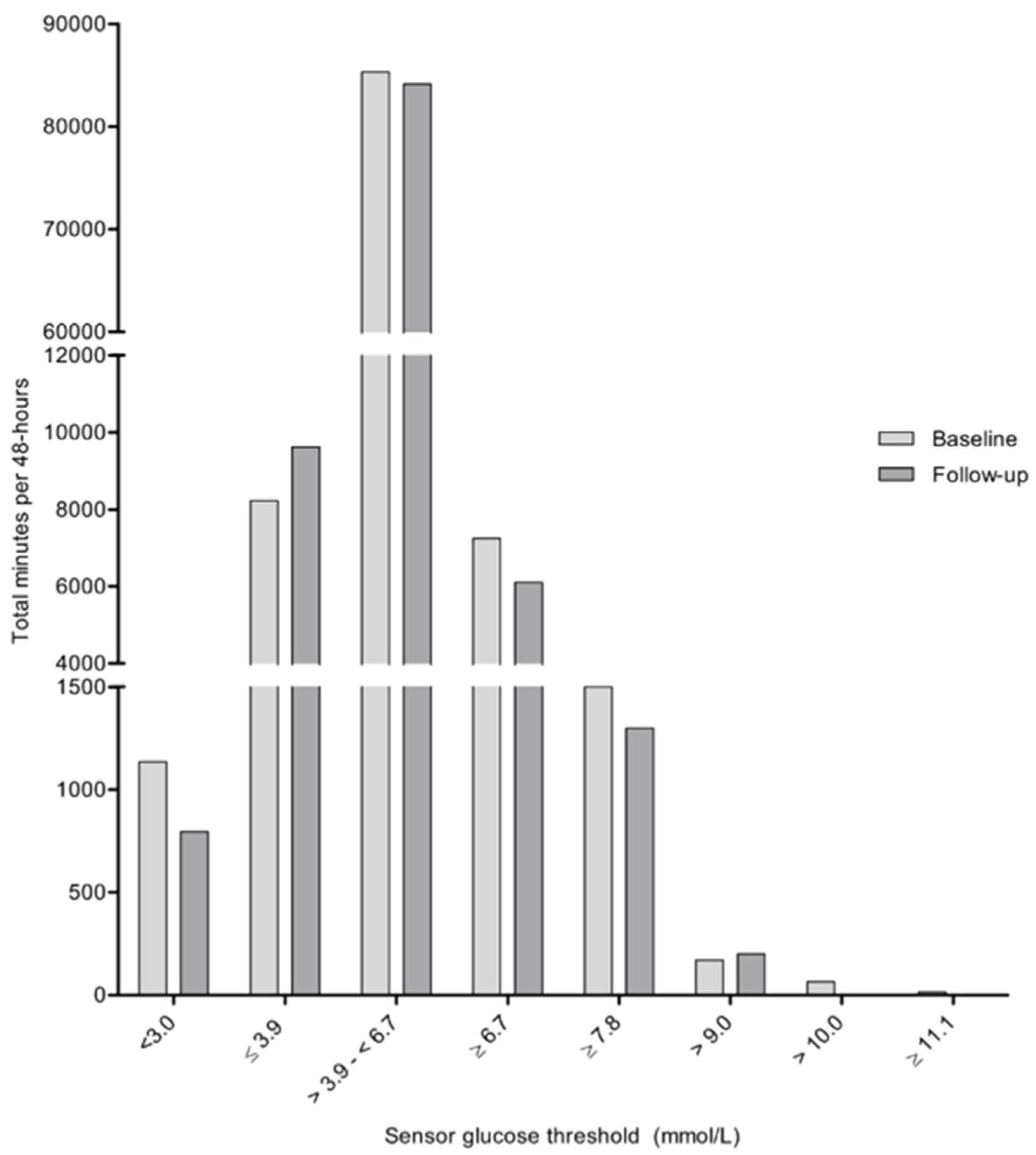
3.2. 48-Hour Glycemic Profile Analysis at Baseline and after 12 Months of Intervention
3.3. Associations between Changes in Glucose Metabolism and CVD Risk after 12 Months of Lifestyle Intervention
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- D’Adamo, E.; Caprio, S. Type 2 diabetes in youth: Epidemiology and pathophysiology. Diabetes Care 2011, 34 (Suppl. 2), S161–S165. [Google Scholar] [CrossRef] [PubMed]
- Freedman, D.S.; Mei, Z.; Srinivasan, S.R.; Berenson, G.S.; Dietz, W.H. Cardiovascular risk factors and excess adiposity among overweight children and adolescents: The Bogalusa Heart Study. J. Pediatr. 2007, 150, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Haffner, S.M.; Stern, M.P.; Hazuda, H.P.; Mitchell, B.D.; Patterson, J.K. Cardiovascular risk factors in confirmed prediabetic individuals. Does the clock for coronary heart disease start ticking before the onset of clinical diabetes? JAMA 1990, 263, 2893–2898. [Google Scholar] [CrossRef]
- Harris, M.I.; Klein, R.; Welborn, T.A.; Knuiman, M.W. Onset of NIDDM occurs at least 4–7 yr before clinical diagnosis. Diabetes Care 1992, 15, 815–819. [Google Scholar] [CrossRef] [PubMed]
- Rijks, J.M.; Plat, J.; Mensink, R.P.; Dorenbos, E.; Buurman, W.A.; Vreugdenhil, A. Children with morbid obesity benefit equally as children with overweight and obesity from an on-going care program. J. Clin. Endocrinol. Metab. 2015, 100, 3572–3580. [Google Scholar] [CrossRef] [PubMed]
- Skinner, A.C.; Perrin, E.M.; Moss, L.A.; Skelton, J.A. Cardiometabolic Risks and Severity of Obesity in Children and Young Adults. N. Engl. J. Med. 2015, 373, 1307–1317. [Google Scholar] [CrossRef] [PubMed]
- Karnebeek, K.; Thapar, S.; Willeboordse, M.; van Schayk, O.C.P.; Vreugdenhil, A.C.E. Comorbidities in Primary vs Secondary School Children with Obesity and Responsiveness to Lifestyle Intervention. J. Clin. Endocrinol. Metab. 2019, 104, 3803–3811. [Google Scholar] [CrossRef] [PubMed]
- Koskinen, J.S.; Kyto, V.; Juonala, M.; Viikari, J.S.A.; Nevalainen, J.; Kahonen, M.; Lehtimäki, T.; Hutri-Kähönen, N.; Laitinen, T.; Tossavainen, P.; et al. Childhood risk factors and carotid atherosclerotic plaque in adulthood: The Cardiovascular Risk in Young Finns Study. Atherosclerosis 2020, 293, 18–25. [Google Scholar] [CrossRef]
- Rijks, J.; Karnebeek, K.; van Dijk, J.W.; Dorenbos, E.; Gerver, W.J.; Stouthart, P.; Plat, J.; Vreugdenhil, A. Glycaemic Profiles of Children with Overweight and Obesity in Free-living Conditions in Association with Cardiometabolic Risk. Sci. Rep. 2016, 6, 31892. [Google Scholar] [CrossRef]
- Chan, C.L.; Pyle, L.; Newnes, L.; Nadeau, K.J.; Zeitler, P.S.; Kelsey, M.M. Continuous glucose monitoring and its relationship to hemoglobin A1c and oral glucose tolerance testing in obese and prediabetic youth. J. Clin. Endocrinol. Metab. 2015, 100, 902–910. [Google Scholar] [CrossRef]
- Razavi Nematollahi, L.; Kitabchi, A.E.; Stentz, F.B.; Wan, J.Y.; Larijani, B.A.; Tehrani, M.M.; Gozashti, M.H.; Omidfar, K.; Taheri, E. Proinflammatory cytokines in response to insulin-induced hypoglycemic stress in healthy subjects. Metabolism 2009, 58, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Adler, G.K.; Bonyhay, I.; Failing, H.; Waring, E.; Dotson, S.; Freeman, R. Antecedent hypoglycemia impairs autonomic cardiovascular function: Implications for rigorous glycemic control. Diabetes 2009, 58, 360–366. [Google Scholar] [CrossRef]
- Ceriello, A.; Esposito, K.; Piconi, L.; Ihnat, M.A.; Thorpe, J.E.; Testa, R.; Boemi, M.; Giugliano, D. Oscillating glucose is more deleterious to endothelial function and oxidative stress than mean glucose in normal and type 2 diabetic patients. Diabetes 2008, 57, 1349–1354. [Google Scholar] [CrossRef] [PubMed]
- Monnier, L.; Mas, E.; Ginet, C.; Michel, F.; Villon, L.; Cristol, J.P.; Colette, C. Activation of oxidative stress by acute glucose fluctuations compared with sustained chronic hyperglycemia in patients with type 2 diabetes. Jama 2006, 295, 1681–1687. [Google Scholar] [CrossRef] [PubMed]
- Mauras, N.; Mazaika, P.; Buckingham, B.; Weinzimer, S.; White, N.H.; Tsalikian, E.; Hershey, T.; Cato, A.; Cheng, P.; Kollman, C.; et al. Longitudinal assessment of neuroanatomical and cognitive differences in young children with type 1 diabetes: Association with hyperglycemia. Diabetes 2015, 64, 1770–1779. [Google Scholar] [CrossRef]
- Tay, J.; Luscombe-Marsh, N.D.; Thompson, C.H.; Noakes, M.; Buckley, J.D.; Wittert, G.A.; Yancy, W.S.; Brinkworth, G.D. A very low-carbohydrate, low-saturated fat diet for type 2 diabetes management: A randomized trial. Diabetes Care 2014, 37, 2909–2918. [Google Scholar] [CrossRef]
- Mikus, C.R.; Oberlin, D.J.; Libla, J.; Boyle, L.J.; Thyfault, J.P. Glycaemic control is improved by 7 days of aerobic exercise training in patients with type 2 diabetes. Diabetologia 2012, 55, 1417–1423. [Google Scholar] [CrossRef]
- Van Dijk, J.W.; Manders, R.J.; Canfora, E.E.; Mechelen, W.V.; Hartgens, F.; Stehouwer, C.D.; Van Loon, L.J. Exercise and 24-h glycemic control: Equal effects for all type 2 diabetes patients? Med. Sci. Sports Exerc. 2013, 45, 628–635. [Google Scholar] [CrossRef]
- Figueira, F.R.; Umpierre, D.; Casali, K.R.; Tetelbom, P.S.; Henn, N.T.; Ribeiro, J.P.; Schaan, B.D. Aerobic and combined exercise sessions reduce glucose variability in type 2 diabetes: Crossover randomized trial. PLoS ONE 2013, 8, e57733. [Google Scholar] [CrossRef]
- Slover, R.H.; Tryggestad, J.B.; DiMeglio, L.A.; Fox, L.A.; Bode, B.W.; Bailey, T.S.; Brazg, R.; Christiansen, M.P.; Sherr, J.L.; Tsalikian, E.; et al. Accuracy of a Fourth-Generation Continuous Glucose Monitoring System in Children and Adolescents with Type 1 Diabetes. Diabetes Technol. Ther. 2018, 20, 576–584. [Google Scholar] [CrossRef]
- Dovc, K.; Cargnelutti, K.; Sturm, A.; Selb, J.; Bratina, N.; Battelino, T. Continuous glucose monitoring use and glucose variability in pre-school children with type 1 diabetes. Diabetes Res. Clin. Pract. 2019, 147, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Patton, S.R.; Noser, A.E.; Youngkin, E.M.; Majidi, S.; Clements, M.A. Early Initiation of Diabetes Devices Relates to Improved Glycemic Control in Children with Recent-Onset Type 1 Diabetes Mellitus. Diabetes Technol. Ther. 2019, 21, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Schonbeck, Y.; Talma, H.; van Dommelen, P.; Bakker, B.; Buitendijk, S.E.; Hirasing, R.A.; van Buuren, S. Increase in prevalence of overweight in Dutch children and adolescents: A comparison of nationwide growth studies in 1980, 1997 and 2009. PLoS ONE 2011, 6, e27608. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatric Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef]
- Fredriks, A.M.; van Buuren, S.; Fekkes, M.; Verloove-Vanhorick, S.P.; Wit, J.M. Are age references for waist circumference, hip circumference and waist-hip ratio in Dutch children useful in clinical practice? Eur. J. Pediatr. 2005, 164, 216–222. [Google Scholar] [CrossRef]
- Etniciteit, Definitie en gegevens. In Nationaal Kompas Volksgezondheid; RIVM: Bilthoven, The Netherlands, 2012.
- American Diabetes, A. 2. Classification and Diagnosis of Diabetes. Diabetes Care 2016, 39 (Suppl. 1), S13–S22. [Google Scholar]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Danne, T.; Nimri, R.; Battelino, T.; Bergenstal, R.M.; Close, K.L.; DeVries, J.H.; Garg, S.; Heinemann, L.; Hirsch, I.; Amiel, S.A.; et al. International Consensus on Use of Continuous Glucose Monitoring. Diabetes Care 2017, 40, 1631–1640. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2018. Diabetes Care 2018, 41 (Suppl. 1), S13–S27. [Google Scholar] [CrossRef]
- McDonnell, C.M.; Donath, S.M.; Vidmar, S.I.; Werther, G.A.; Cameron, F.J. A novel approach to continuous glucose analysis utilizing glycemic variation. Diabetes Technol. Ther. 2005, 7, 253–263. [Google Scholar] [CrossRef]
- Wuhl, E.; Witte, K.; Soergel, M.; Mehls, O.; Schaefer, F. Distribution of 24-h ambulatory blood pressure in children: Normalized reference values and role of body dimensions. J. Hypertens. 2002, 20, 1995–2007. [Google Scholar] [CrossRef] [PubMed]
- Grimm, J.J. Interaction of physical activity and diet: Implications for insulin-glucose dynamics. Public Health Nutr. 1999, 2, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Shah, V.N.; DuBose, S.N.; Li, Z.; Beck, R.W.; Petesrs, A.L.; Weinstock, R.S.; Kruger, D.; Tansey, M.; Sparling, D.; Woerner, S.; et al. Continuous Glucose Monitoring Profiles in Healthy Non-Diabetic Participants: A Multicenter Prospective Study. J. Clin. Endocrinol. Metab. 2019, 104, 4356–4364. [Google Scholar] [CrossRef] [PubMed]
- Nightingale, C.M.; Rudnicka, A.R.; Owen, C.G.; Wells, J.C.K.; Sattar, N.; Cook, D.G.; Whincup, P.H. Influence of Adiposity on Insulin Resistance and Glycemia Markers Among, U.K. Children of South Asian, Black African-Caribbean, and White European Origin. Diabetes Care 2013, 36, 1712–1719. [Google Scholar] [CrossRef] [PubMed]
- Monnier, L.; Lapinski, H.; Colette, C. Contributions of fasting and postprandial plasma glucose increments to the overall diurnal hyperglycemia of type 2 diabetic patients: Variations with increasing levels of HbA(1c). Diabetes Care 2003, 26, 881–885. [Google Scholar] [CrossRef]
- Woerle, H.J.; Neumann, C.; Zschau, S.; Tenner, S.; Irsigler, A.; Schirra, J.; Gerich, J.E.; Göke, B. Impact of fasting and postprandial glycemia on overall glycemic control in type 2 diabetes Importance of postprandial glycemia to achieve target HbA1c levels. Diabetes Res. Clin. Pract. 2007, 77, 280–285. [Google Scholar] [CrossRef]
- Avramoglu, R.K.; Basciano, H.; Adeli, K. Lipid and lipoprotein dysregulation in insulin resistant states. Clin. Chim. Acta 2006, 368, 1–19. [Google Scholar] [CrossRef]
- Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group; Fox, L.A.; Beck, R.W.; Xing, D. Variation of interstitial glucose measurements assessed by continuous glucose monitors in healthy, nondiabetic individuals. Diabetes Care 2010, 33, 1297–1299. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Baseline | After 12 Months of Intervention |
|---|---|---|
| Age, years | 12.5 ± 3.2 | 13.8 ± 3.0 |
| BMI z-score | 3.53 ± 0.66 | 3.46 ± 0.67 |
| Overweight/obesity/morbid obesity, % | 9/42/49 | 15/39/46 * |
| Waist circumference z-score | 6.85 ± 2.43 | 7.33 ± 2.12 * |
| Median sensor glucose, mmol/L | 5.0 (3.2–7.3) | 5.1 (3.6–6.9) |
| Maximum sensor glucose, mmol/L | 7.2 (5.6–11.2) | 7.0 (5.4–9.9) |
| Minimum sensor glucose, mmol/L | 3.4 (2.2–4.4) | 3.4 (2.2–4.9) |
| Sensor glucose area under the curve | 14867 ± 1447 | 14746 ± 1586 |
| CONGA1 | 0.57 (0.39–1.31) | 0.50 (0.30–1.08) * |
| CONGA2 | 0.72 (0.46–1.61) | 0.69 (0.30–1.58) |
| CONGA4 | 0.88 (0.45–2.02) | 0.87 (0.39–1.94) |
| CV, % | 15.7 ± 5.5 | 15.1 ± 4.0 |
| Fasting glucose, mmol/L | 4.0 ± 0.5 | 4.0 ± 0.5 |
| Fasting insulin, mU/L | 18.5 ± 9.2 | 25.6 ± 13.7 * |
| HOMA-IR | 3.31 ± 1.61 | 4.29 ± 2.30 * |
| HbA1c, % | 5.4 ± 0.3 | 5.2 ± 0.4 * |
| Plasma glucose 2 hours after glucose load, mmol/L | 5.5 ± 1.2 | 5.6 ± 1.1 |
| Total cholesterol, mmol/L | 4.8 (3.5–6.6) | 4.5 (3.5–6.9) * |
| LDL-cholesterol, mmol/L | 3.1 (2.0–4.5) | 2.7 (1.7–4.6) * |
| HDL-cholesterol, mmol/L | 1.1 (0.8–1.9) | 1.1 (0.8–1.9) |
| Triglycerides, mmol/L | 1.21 (0.39–4.48) | 1.13 (0.51–3.77) |
| Systolic blood pressure z-score | 0.19 ± 1.26 | 0.02 ± 1.16 |
| Diastolic blood pressure z-score | −0.37 ± 0.88 | −0.66 ± 1.17 |
| Decrease in BMI z-Score after 12 Months of Intervention (n = 20) | Increase in BMI z-Score after 12 Months of Intervention (n = 13) | |||
|---|---|---|---|---|
| Baseline | 12 Months of Intervention | Baseline | 12 Months of Intervention | |
| Age | 11.3 ± 2.6 | 12.7 ± 2.5 | 14.4 ± 3.1 | 15.6 ± 3.0 |
| BMI z-score | 3.54 ± 0.62 | 3.30 ± 0.61 * | 3.50 ± 0.74 | 3.71 ± 0.71 * |
| Waist circumference z-score | 6.3 ± 1.9 | 6.9 ± 1.6 | 7.6 ± 3.4 | 8.2 ±3.1 |
| Fasting glucose, mmol/L | 4.1 ± 0.6 | 4.3 ± 0.4 | 3.9 ± 0.5 | 4.1 ± 0.6 |
| Fasting insulin, mU/L | 18.1 ± 7.0 | 20.7 ± 9.8 | 20.2 ± 12.4 | 27.5 ± 13.3 * |
| HOMA-IR | 3.21 ± 1.40 | 4.00 ± 2.00 | 3.20 ± 1.84 | 4.50 ± 2.48 |
| HbA1c, % | 5.4 ± 0.3 | 5.2 ± 0.4 * | 5.5 ± 0.2 | 5.2 ± 0.4 * |
| Plasma glucose 2 hours after glucose load, mmol/L | 5.6 (3.9–7.5) | 5.6 (4.2–6.7) | 4.8 (2.9–6.3) | 5.2 (4.2–8.5) |
| Total cholesterol, mmol/L | 5.0 ± 0.9 | 4.4 ± 0.6 * | 4.9 ± 0.7 | 5.0 ± 0.9 |
| LDL-cholesterol, mmol/L | 3.2 ± 0.8 | 2.7 ± 0.6 * | 2.9 ± 0.7 | 3.0 ± 0.7 |
| HDL-cholesterol, mmol/L | 1.1 ± 0.2 | 1.2 ± 0.2 | 1.3 ± 0.4 | 1.2 ± 0.3 |
| Triglycerides, mmol/L | 1.23 (0.49–3.11) | 1.02 (0.51–3.69) | 1.20 (0.39–4.48) | 1.28 (0.65–3.77) |
| Systolic blood pressure z-score | 0.23 ± 1.09 | −0.11 ± 1.07 | 0.11 ± 1.63 | 0.21 ± 1.37 |
| Diastolic blood pressure z-score | −0.55 ± 0.65 | −0.89 ± 1.23 | −0.17 ± 1.15 | −0.16 ± 0.95 |
| Decrease in BMI z-Score after 12 Months of Intervention (n = 20) | Increase in BMI z-score after 12 Months of Intervention (n = 13) | |||
|---|---|---|---|---|
| Baseline | After 12 Months of Intervention | Baseline | After 12 Months of Intervention | |
| Median sensor glucose, mmol/L | 4.9 (3.2–7.3) | 4.9 (3.6–5.9) | 5.0 (3.7–6.1) | 5.1 (3.6–6.9) |
| Maximum sensor glucose, mmol/L | 7.0 (6.0–9.5) | 6.9 (5.4–8.7) | 7.5 (5.6–11.2) | 7.3 (5.9–9.9) |
| Minimum sensor glucose, mmol/L | 3.4 (2.2–4.4) | 3.3 (2.6–4.8) | 3.3 (2.2–3.9) | 3.6 (2.2–4.9) |
| Time in level 2 hypoglycemic range (<3.0 mmol/L), minutes | 0 (0–265) | 0 (0–250) | 0 (0–395) | 0 (0–135) |
| Time in level 1 hypoglycemic range (3.0–3.9 mmol/L), minutes | 58 (0–690) | 0 (0–650) | 85 (0–870) | 45 (0–1270) |
| Time in target range (3.9–10.0 mmol/L), minutes | 2823 (2050–2880) | 2710 (2195–2880) | 2795 (1615–2880) | 2835 (1545–2880) |
| Time in secondary target range (3.9–7.8 mmol/L), minutes | 2735 (1945–2880) | 2703 (2195–2880) | 2655 (1615–2880) | 2560 (1545–2880) |
| Time in high-normal range (≥6.7 mmol/L), minutes | 38 (0–895) | 7 (0–123) * | 205 (0–840) | 22 (0–210) |
| Time in high-normal range (≥7.8 mmol/L), minutes | 0 (0–190) | 0 (0–170) | 0 (0–185) | 0 (0–345) |
| Time in level 1 hyperglycemic range (>10.0 mmol/L), minutes | 0 (0–0) | 0 (0–0) | 0 (0–40) | 0 (0–0) |
| Time in level 2 hyperglycemic range (>13.9 mmol/L), minutes | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) |
| Sensor glucose area under the curve | 14729 ± 1214 | 14419 ± 1301 | 15080 ± 1780 | 15249 ± 1891 |
| CV, % | 15.1 ± 5.4 | 14.5 ± 2.7 | 16.7 ± 5.6 | 16.1 ± 5.3 |
| CONGA1 | 0.56 (0.39–1.00) | 0.49 (0.30–1.00) * | 0.65 (0.39–1.31) | 0.60 (0.30–1.08) |
| CONGA2 | 0.70 (0.46–1.26) | 0.63 (0.39–1.16) * | 0.77 (0.46–1.61) | 0.71 (0.30–1.58) |
| CONGA4 | 0.83 (0.45–1.51) | 0.87 (0.48–1.31) | 0.95 (0.66–2.02) | 0.80 (0.39–1.94) |
| Δ Median sensor glucose | Δ Maximum sensor glucose | Δ Minimum sensor glucose | Δ CONGA1 | Δ CONGA2 | Δ CONGA4 | Δ CV | Δ AUC | |
|---|---|---|---|---|---|---|---|---|
| Δ BMI z-score | −0.127 | 0.502 * | −0.356 | 0.601 * | 0.643 * | 0.686 * | 0.620 * | 0.214 |
| Δ Fasting glucose | −0.067 | −0.241 | −0.342 | −0.095 | −0.076 | 0.03 | 0.350 | −0.416 |
| Δ Fasting insulin | 0.150 | −0.183 | −0.05 | −0.084 | 0.082 | 0.11 | 0.000 | 0.075 |
| Δ HOMA-IR | −0.072 | −0.034 | −0.023 | −0.179 | 0.216 | 0.191 | 0.197 | −0.038 |
| Δ HbA1c | 0.340 | 0.153 | −0.175 | 0.340 | 0.319 | 0.239 | 0.032 | 0.229 |
| Δ Glucose 2 h after glucose load | 0.027 | 0.144 | −0.412 | 0.155 | 0.236 | 0.292 | 0.490 | −0.259 |
| Δ Total cholesterol | 0.305 | 0.342 | −0.196 | 0.170 | 0.207 | 0.282 | 0.453 * | 0.162 |
| Δ LDL-cholesterol | 0.472 * | 0.150 | 0.029 | 0.166 | 0.045 | 0.021 | 0.111 | 0.214 |
| Δ HDL-cholesterol | 0.041 | 0.065 | −0.167 | −0.214 | −0.061 | 0.108 | 0.172 | 0.056 |
| Δ Triglycerides | −0.203 | 0.404 | −0.445 * | 0.228 | 0.433 | 0.520 * | 0.457 * | −0.117 |
| Δ Systolic blood pressure z-score | 0.598 * | 0.268 | 0.095 | −0.033 | 0.019 | 0.020 | −0.104 | 0.498 * |
| Δ Diastolic blood pressure z-score | 0.605 * | 0.148 | 0.140 | 0.052 | 0.010 | −0.093 | −0.335 | 0.366 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karnebeek, K.; Rijks, J.M.; Dorenbos, E.; Gerver, W.-J.M.; Plat, J.; Vreugdenhil, A.C.E. Changes in Free-Living Glycemic Profiles after 12 Months of Lifestyle Intervention in Children with Overweight and with Obesity. Nutrients 2020, 12, 1228. https://doi.org/10.3390/nu12051228
Karnebeek K, Rijks JM, Dorenbos E, Gerver W-JM, Plat J, Vreugdenhil ACE. Changes in Free-Living Glycemic Profiles after 12 Months of Lifestyle Intervention in Children with Overweight and with Obesity. Nutrients. 2020; 12(5):1228. https://doi.org/10.3390/nu12051228
Chicago/Turabian StyleKarnebeek, Kylie, Jesse M. Rijks, Elke Dorenbos, Willem-Jan M. Gerver, Jogchum Plat, and Anita C. E. Vreugdenhil. 2020. "Changes in Free-Living Glycemic Profiles after 12 Months of Lifestyle Intervention in Children with Overweight and with Obesity" Nutrients 12, no. 5: 1228. https://doi.org/10.3390/nu12051228
APA StyleKarnebeek, K., Rijks, J. M., Dorenbos, E., Gerver, W.-J. M., Plat, J., & Vreugdenhil, A. C. E. (2020). Changes in Free-Living Glycemic Profiles after 12 Months of Lifestyle Intervention in Children with Overweight and with Obesity. Nutrients, 12(5), 1228. https://doi.org/10.3390/nu12051228