Sodium and Potassium Intakes and Their Ratio in Adults (18–90 y): Findings from the Irish National Adult Nutrition Survey

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. The National Adult Nutrition Survey (NANS) Sample
2.2. Urine Sample Collection, Processing and Analysis
2.3. Food Consumption Data
2.4. Data Analyses
2.4.1. Urinary
2.4.2. Dietary
3. Results
3.1. Urinary Data
3.2. Dietary Data
3.2.1. Dietary Intakes of Sodium and Potassium
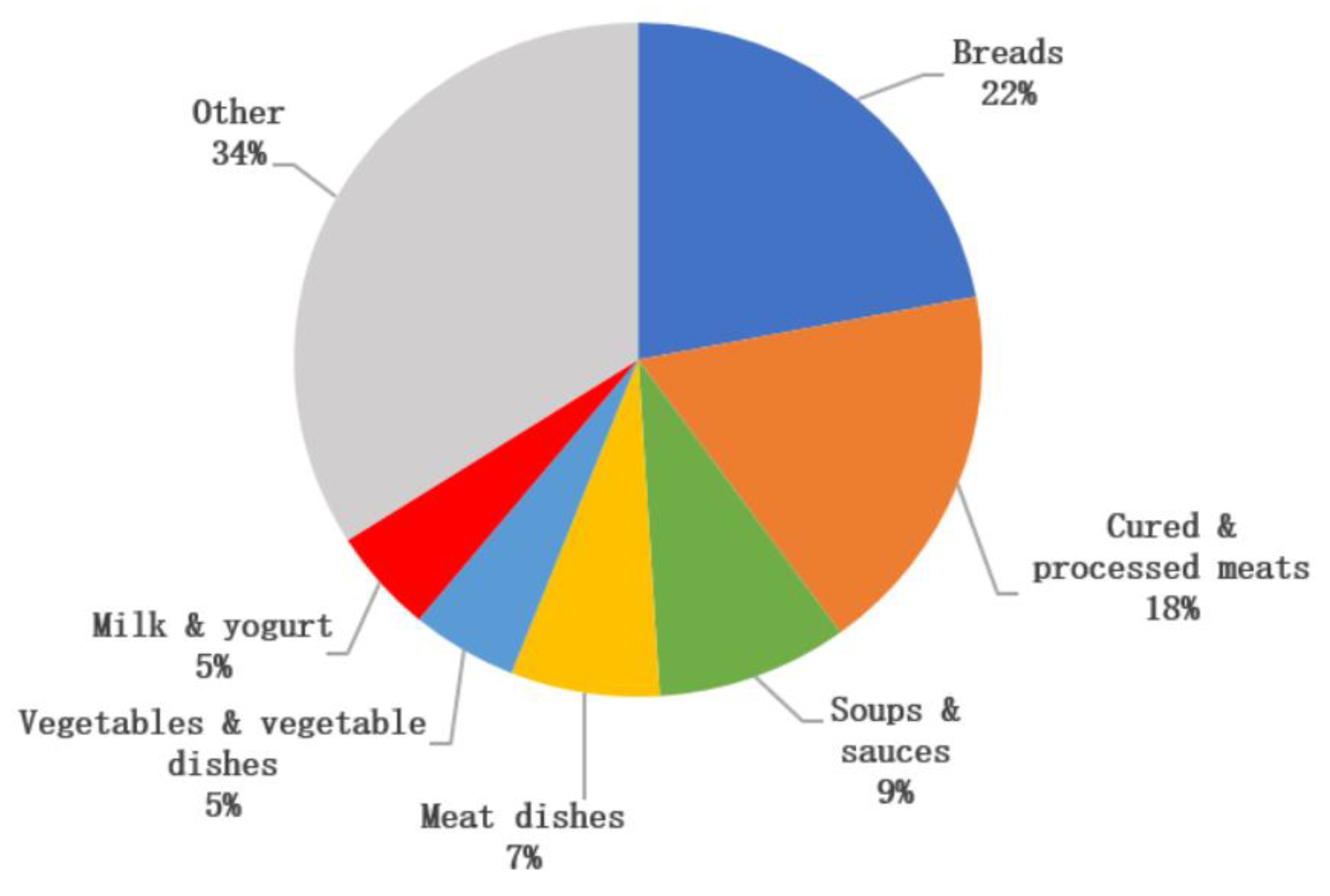
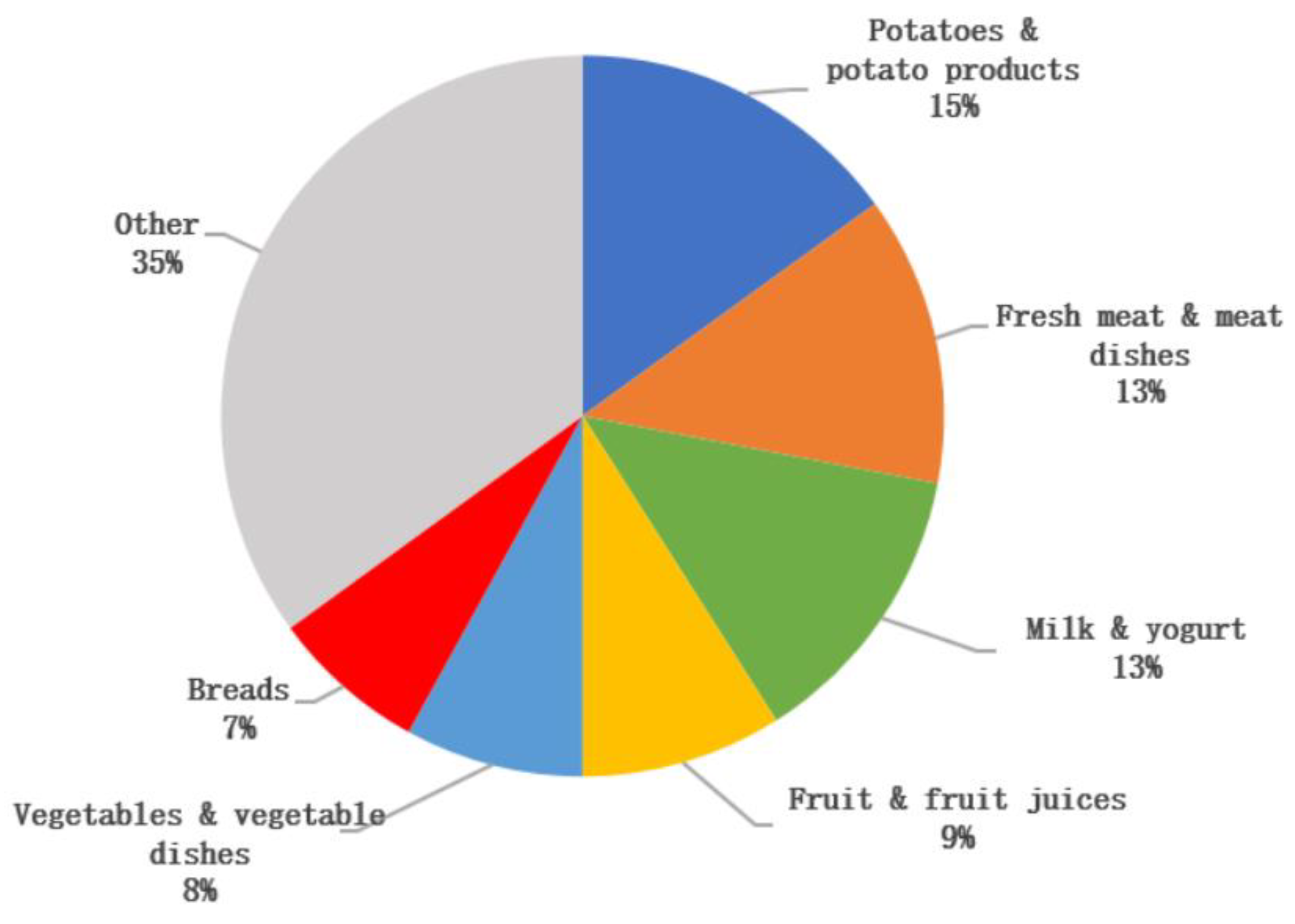
3.2.2. Dietary Sources of Sodium and Potassium Intake
3.2.3. Foods Associated with A Lower Na:K
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Perez, V.; Chang, E.T. Sodium-to-potassium ratio and blood pressure, hypertension, and related factors. Adv. Nutr. 2014, 5, 712–741. [Google Scholar] [CrossRef] [PubMed]
- WHO. Cardiovascular Disease Fact Sheet; World Health Organization (WHO): Geneva, Switzerland, 2017; Available online: https://www.who.int/cardiovascular_diseases/en/ (accessed on 1 September 2018).
- EFSA Panel on Nutrition, Novel Foods and Food Allergens (NDA); Turck, D.; Castenmiller, J.; de Henauw, S.; Hirsch-Ernst, K.I.; Kearney, J.; Knutsen, H.K.; Maciuk, A.; Mangelsdorf, I.; McArdle, H.J.; et al. Scientific Opinion on the dietary reference values for sodium. EFSA J. 2019, 17, e05778. [Google Scholar]
- FSAI. Salt and Health. Review of the Scientific Evidence and Recommendations for Public Policy in Ireland; Food Safety Authority of Ireland: Dublin, Ireland, 2016. [Google Scholar]
- SACN. Salt and Health; The Stationery Office: Norwich, UK, 2003.
- EFSA. Dietary Reference Values for Nutrients Summary Report. EFSA Support. Publ. 2017, 14. [Google Scholar] [CrossRef]
- EFSA. EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies); Turck, D.; Bresson, J.-L.; Burlingame, B.; Dean, T.; Fairweather-Tait, S.; Heinonen, M.; Hirsch-Ernst, K.I.; Mangelsdorf, I.; McArdle, H.; et al. Scientific opinion on dietary reference values for potassium. Efsa J. 2016, 14, 56. [Google Scholar] [CrossRef]
- Tzoulaki, I.; Patel, C.J.; Okamura, T.; Chan, Q.; Brown, I.J.; Miura, K.; Ueshima, H.; Zhao, L.; Van Horn, L.; Daviglus, M.L.; et al. A nutrient-wide association study on blood pressure. Circulation 2012, 126, 2456–2464. [Google Scholar] [CrossRef] [PubMed]
- Stamler, J.; Rose, G.; Stamler, R.; Elliott, P.; Dyer, A.; Marmot, M. INTERSALT study findings. Public health and medical care implications. Hypertension 1989, 14, 570–577. [Google Scholar] [CrossRef] [PubMed]
- WHO. Guideline: Sodium Intake for Adults and Children; World Health Organization (WHO): Geneva, Switzerland, 2012. [Google Scholar]
- WHO. Guideline: Potassium Intake for Adults and Children; World Health Organization (WHO): Geneva, Switzerland, 2012. [Google Scholar]
- Averill, M.M.; Young, R.L.; Wood, A.C.; Kurlak, E.O.; Kramer, H.; Steffen, L.; McClelland, R.L.; Delaney, J.A.; Drewnowski, A. Spot Urine Sodium-to-Potassium Ratio Is a Predictor of Stroke. Stroke 2019, 50, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Donfrancesco, C.; Ippolito, R.; Lo Noce, C.; Palmieri, L.; Iacone, R.; Russo, O.; Vanuzzo, D.; Galletti, F.; Galeone, D.; Giampaoli, S.; et al. Excess dietary sodium and inadequate potassium intake in Italy: Results of the MINISAL study. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 850–856. [Google Scholar] [CrossRef]
- Vasara, E.; Marakis, G.; Breda, J.; Skepastianos, P.; Hassapidou, M.; Kafatos, A.; Rodopaios, N.; Koulouri, A.A.; Cappuccio, F.P. Sodium and Potassium Intake in Healthy Adults in Thessaloniki Greater Metropolitan Area-The Salt Intake in Northern Greece (SING) Study. Nutrients 2017, 9, 417. [Google Scholar] [CrossRef]
- Swanepoel, B.; Schutte, A.E.; Cockeran, M.; Steyn, K.; Wentzel-Viljoen, E. Sodium and potassium intake in South Africa: An evaluation of 24-h urine collections in a white, black, and Indian population. J. Am. Soc. Hypertens. JASH 2016, 10, 829–837. [Google Scholar] [CrossRef]
- McLean, R.; Edmonds, J.; Williams, S.; Mann, J.; Skeaff, S. Balancing Sodium and Potassium: Estimates of Intake in a New Zealand Adult Population Sample. Nutrients 2015, 7, 8930–8938. [Google Scholar] [CrossRef] [PubMed]
- Asakura, K.; Uechi, K.; Sasaki, Y.; Masayasu, S.; Sasaki, S. Estimation of sodium and potassium intakes assessed by two 24 h urine collections in healthy Japanese adults: A nationwide study. Br. J. Nutr. 2014, 112, 1195–1205. [Google Scholar] [CrossRef] [PubMed]
- Yi, S.S.; Curtis, C.J.; Angell, S.Y.; Anderson, C.A.M.; Jung, M.; Kansagra, S.M. Highlighting the ratio of sodium to potassium in population-level dietary assessments: Cross-sectional data from New York City, USA. Public Health Nutr. 2014, 17, 2484–2488. [Google Scholar] [CrossRef] [PubMed]
- Cook, N.R.; Obarzanek, E.; Cutler, J.A.; Buring, J.E.; Rexrode, K.M.; Kumanyika, S.K.; Appel, L.J.; Whelton, P.K. Joint effects of sodium and potassium intake on subsequent cardiovascular disease: The Trials of Hypertension Prevention follow-up study. Arch. Intern. Med. 2009, 169, 32–40. [Google Scholar] [CrossRef]
- Iwahori, T.; Miura, K.; Ueshima, H. Time to Consider Use of the Sodium-to-Potassium Ratio for Practical Sodium Reduction and Potassium Increase. Nutrients 2017, 9, 700. [Google Scholar] [CrossRef]
- Mente, A.; O’Donnell, M.J.; Dagenais, G.; Wielgosz, A.; Lear, S.A.; McQueen, M.J.; Jiang, Y.; Xingyu, W.; Jian, B.; Calik, K.B.; et al. Validation and comparison of three formulae to estimate sodium and potassium excretion from a single morning fasting urine compared to 24-h measures in 11 countries. J. Hypertens. 2014, 32, 1005–1014, discussion 1015. [Google Scholar] [CrossRef]
- Iwahori, T.; Miura, K.; Ueshima, H.; Chan, Q.; Dyer, A.R.; Elliott, P.; Stamler, J. Estimating 24-h urinary sodium/potassium ratio from casual (’spot’) urinary sodium/potassium ratio: The INTERSALT Study. Int. J. Epidemiol. 2017, 46, 1564–1572. [Google Scholar] [CrossRef]
- Huang, L.; Woodward, M.; Stepien, S.; Tian, M.; Yin, X.; Hao, Z.; Li, Z.; Sun, J.; Yu, Y.; Zhou, B.; et al. Spot urine samples compared with 24-h urine samples for estimating changes in urinary sodium and potassium excretion in the China Salt Substitute and Stroke Study. Int. J. Epidemiol. 2018, 47, 1811–1820. [Google Scholar] [CrossRef]
- IUNA. National Adult Nutrition Survey Main Report; Irish Universities Nutrition Alliance: Cork, Ireland, 2011. [Google Scholar]
- Cashman, K.D.; Muldowney, S.; McNulty, B.; Nugent, A.; FitzGerald, A.P.; Kiely, M.; Walton, J.; Gibney, M.J.; Flynn, A. Vitamin D status of Irish adults: Findings from the National Adult Nutrition Survey. Br. J. Nutr. 2013, 109, 1248–1256. [Google Scholar] [CrossRef]
- Central Statistics Office (CSO). Census 2006 Principal Demographic Results; The Stationery Office: Dublin, Ireland, 2007. [Google Scholar]
- Harrington, K.E.; Robson, P.J.; Kiely, M.; Livingstone, M.B.; Lambe, J.; Gibney, M.J. The North/South Ireland Food Consumption Survey: Survey design and methodology. Public Health Nutr 2001, 4, 1037–1042. [Google Scholar] [CrossRef]
- Nelson, M.; Atkinson, M.; Meyer, J. A Photographic Atlas of Food Portion Sizes; Ministry of Agriculture Fisheries and Food: London, UK, 1997.
- Food Standards Agency. Food Portion Sizes, 3rd ed.; The Stationery Office: London, UK, 2002.
- Food Standards Agency. McCance and Widdowson’s The Composition of Foods, 6th ed.; Royal Society of Chemistry: Cambridge, UK, 2002.
- Holland, B.; Unwin, I.; Buss, D. Cereal and Cereal Products, Third Supplement to McCance & Widdowson’s The Composition of Foods, 4th ed.; HMSO: London, UK, 1988.
- Holland, B.; Unwin, I.; Buss, D. Milk Products and Eggs. Fourth Supplement to McCance & Widdowson’s The Composition of Foods, 4th ed.; HMSO: London, UK, 1989.
- Holland, B.; Unwin, I.; Buss, D. Vegetables, Herbs and Spices. Fifth Supplement to McCance & Widdowson’s The Composition of Foods, 4th ed.; HMSO: London, UK, 1991.
- Holland, B.; Unwin, I.; Buss, D. Fruits and Nuts, First Supplement to McCance & Widdowson’s The Composition of Foods, 5th ed.; HMSO: London, UK, 1992.
- Kawasaki, T.; Itoh, K.; Uezono, K.; Sasaki, H. A simple method for estimating 24 h urinary sodium and potassium excretion from second morning voiding urine specimen in adults. Clin. Exp. Pharmacol. Physiol. 1993, 20, 7–14. [Google Scholar] [CrossRef]
- Chan, W.; Brown, J.; Buss, D. Miscellaneous Foods, Fourth Supplement to McCance & Widdowson’s The Composition of Foods, 5th ed.; HMSO: London, UK, 1994.
- Chan, W.; Brown, J.; Lee, S.; Buss, D. Meat, Poultry and Game, Fifth Supplement to McCance & Widdowson’s The Composition of Foods, 5th ed.; HMSO: London, UK, 1995.
- Chan, W.; Brown, J.; Church, S.; Buss, D. Meat Products and Dishes, Sixth Supplement to McCance & Widdowson’s The Composition of Foods, 5th ed.; HMSO: London, UK, 1996.
- Holland, B.; Welch, A.; Buss, D. Vegetable Dishes, Second Supplement to McCance and Widdowson’s The Composition of Foods, 5th ed.; HMSO: London, UK, 1996.
- Black, L.J.; Ireland, J.; Moller, A.; Roe, M.; Walton, J.; Flynn, A.; Finglas, P.M.; Kiely, M. Development of an on-line Irish food composition database for nutrients. J. Food Compos. Anal. 2011, 24, 1017–1023. [Google Scholar] [CrossRef]
- Perry, I.; Browne, G.; Loughrey, M.; Harrington, J.; Lutonski, J.; Fitzgerald, A. Dietray Salt Intake and Related Risk Factors in the Irish Population; A Report for Safefood Ireland; Safefood Ireland: Cork, Ireland, 2010; ISBN 987-1-905767-14-4. [Google Scholar]
- Iwahori, T.; Ueshima, H.; Torii, S.; Saito, Y.; Kondo, K.; Tanaka-Mizuno, S.; Arima, H.; Miura, K. Diurnal variation of urinary sodium-to-potassium ratio in free-living Japanese individuals. Hypertens. Res. 2017, 40, 658–664. [Google Scholar] [CrossRef] [PubMed]
- Tooze, J.A.; Kipnis, V.; Buckman, D.W.; Carroll, R.J.; Freedman, L.S.; Guenther, P.M.; Krebs-Smith, S.M.; Subar, A.F.; Dodd, K.W. A mixed-effects model approach for estimating the distribution of usual intake of nutrients: The NCI method. Stat. Med. 2010, 29, 2857–2868. [Google Scholar] [CrossRef] [PubMed]
- Krebs-Smith, S.M.; Kott, P.S.; Guenther, P.M. Mean proportion and population proportion: Two answers to the same question? J. Am. Diet. Assoc. 1989, 89, 671–676. [Google Scholar]
- Bates, B.; Cox, L.; Maplethorpe, N.; Mazumder, A.; Nicholson, S.; Page, P.; Prentice, A.; Rooney, K.; Ziauddeen, N.; Swan, G. National Diet and Nutrition Survey: Assessment of Dietary Sodium. Adults (19 to 64 Years) in England, 2014; NatCen: London, UK, 2016. [Google Scholar]
- Bates, B.; Cox, L.; Maplethorpe, N.; Mazumder, A.; Nicholson, S.; Page, P.; Prentice, A.; Rooney, K.; Ziauddeen, N.; Swan, G.; et al. National Diet and Nutrition Survey: Assessment of Dietary Sodium. Adults (19–64 years) in Scotland, 2014; Food Standards Scotland: Aberdeen, UK, 2016.
- Bates, B.; Cox, L.; Maplethorpe, N.; Mazumder, A.; Nicholson, S.; Page, P.; Prentice, A.; Rooney, K.; Ziauddeen, N.; Swan, G.; et al. National Diet and Nutrition Survey: Assessment of Dietary Sodium. Adults (19–64 Years) in Northern Ireland, 2015; Food Standards Agency: Belfast, Ireland, 2016.
- Bates, B.; Lennox, A.; Prentice, A.; Bates, C.; Page, P.; Nicholson, S.; Swan, G. National Diet and Nutrition Survey. Results from Years 1, 2, 3 and 4 (combined) of the Rolling Programme (2008/2009–2011/2012); Public Health England: London, UK, 2014.
- O’Donnell, M.; Mente, A.; Rangarajan, S.; McQueen, M.J.; Wang, X.; Liu, L.; Yan, H.; Lee, S.F.; Mony, P.; Devanath, A.; et al. Urinary sodium and potassium excretion, mortality, and cardiovascular events. N. Engl. J. Med. 2014, 371, 612–623. [Google Scholar] [CrossRef]
- Kalogeropoulos, A.P.; Georgiopoulou, V.V.; Murphy, R.A.; Newman, A.B.; Bauer, D.C.; Harris, T.B.; Yang, Z.; Applegate, W.B.; Kritchevsky, S.B. Dietary sodium content, mortality, and risk for cardiovascular events in older adults: The Health, Aging, and Body Composition (Health ABC) Study. JAMA Intern. Med. 2015, 175, 410–419. [Google Scholar] [CrossRef]
- Cook, N.R.; Appel, L.J.; Whelton, P.K. Sodium Intake and All-Cause Mortality Over 20 Years in the Trials of Hypertension Prevention. J. Am. Coll. Cardiol. 2016, 68, 1609–1617. [Google Scholar] [CrossRef]
- Cobb, L.K.; Anderson, C.A.; Elliott, P.; Hu, F.B.; Liu, K.; Neaton, J.D.; Whelton, P.K.; Woodward, M.; Appel, L.J. Methodological issues in cohort studies that relate sodium intake to cardiovascular disease outcomes: A science advisory from the American Heart Association. Circulation 2014, 129, 1173–1186. [Google Scholar] [CrossRef]
- Anderson, C.A.M.; Appel, L.J.; Okuda, N.; Brown, I.J.; Chan, Q.; Zhao, L.; Ueshima, H.; Kesteloot, H.; Miura, K.; Curb, J.D.; et al. Dietary sources of sodium in China, Japan, the United Kingdom, and the United States, women and men aged 40 to 59 years: The INTERMAP study. J. Am. Diet. Assoc. 2010, 110, 736–745. [Google Scholar] [CrossRef]
- RIVM. Dutch National Food Consumption Survey 2007–2010. Part 8-A Sources of micronutrients, Version 2, based on dataset DFC_2010_core_20120822; RIVM: Bilthoven, The Netherlands, 2012. [Google Scholar]
- Hasenegger, V.; Rust, P.; König, J.; Purtscher, A.E.; Erler, J.; Ekmekcioglu, C. Main Sources, Socio-Demographic and Anthropometric Correlates of Salt Intake in Austria. Nutrients 2018, 10, 311. [Google Scholar] [CrossRef] [PubMed]
- FSAI. Salt Reducing in Processed Foods—Salt in Diet Still High. Available online: https://www.fsai.ie/news_centre/press_releases/salt_reduction_programme_031116.html (accessed on 1 May 2019).
- Wyness, L.; Butriss, J.; Stanner, S. Reducing the population’s sodium intake: The UK Food Standards Agency’s Salt Reduction Programme. Public Health Nutr. 2011, 15, 254–261. [Google Scholar] [CrossRef] [PubMed]
- FSAI. Irish Adults have Decreased Daily Salt Intake by more than 1 Gram; FSAI: Dublin, Ireland, 2011. [Google Scholar]
- FSAI. Scientific Recommendations for Healthy Eating Guidelines in Ireland. Food Safety Authority or Ireland, Dublin; FSAI: Dublin, Ireland, 2011. [Google Scholar]
- Okuda, N.; Stamler, J.; Brown, I.J.; Ueshima, H.; Miura, K.; Okayama, A.; Saitoh, S.; Nakagawa, H.; Sakata, K.; Yoshita, K.; et al. Individual efforts to reduce salt intake in China, Japan, UK, USA: What did people achieve? The INTERMAP Population Study. J. Hypertens. 2014, 32, 2385–2392. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Urinary Sodium (mg) | Urinary Salt Equivalents (g) | Urinary Potassium (mg) | Na:K (mmol/mmol) | Urinary Molar Na:K ≤1.0 ** | Urinary Molar Na:K ≤2.0 *** | ||
|---|---|---|---|---|---|---|---|
| Mean | Mean | Mean | Mean | SD | % | % | |
| Men | 4631 | 11.6 | 3894 | 1.90 | 1.49 | 31 | 60 |
| 18–35 years | 4677 | 11.7 | 3775 | 1.99 | 1.57 | 32 | 56 |
| 36–50 years | 4693 | 11.7 | 4306 | 1.71 | 1.36 | 32 | 67 |
| 51–64 years | 4504 | 11.3 | 3888 | 1.82 | 1.39 | 31 | 68 |
| 65+ years | 4550 | 11.4 | 3393 | 2.17 | 1.59 | 25 | 53 |
| Women | 3525 | 8.8 | 2686 | 2.15 | 1.67 | 25 | 57 |
| 18–35 years | 3925 | 9.8 | 2887 | 2.35 | 1.92 | 22 | 52 |
| 36–50 years | 3528 | 8.8 | 2830 | 2.01 | 1.58 | 30 | 61 |
| 51–64 years | 3276 | 8.2 | 2505 | 2.08 | 1.55 | 25 | 58 |
| 65+ years | 2895 | 7.2 | 2139 | 2.05 | 1.28 | 21 | 57 |
| n | Sodium | Salt | Potassium | Dietary Na:K | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| mg/d | mg/10 MJ | g/d | mg/10 MJ | mg/d | mg/10 MJ | (mmol/mmol) | |||||||||
| mean | SD | mean | SD | mean | SD | mean | SD | mean | SD | mean | SD | Mean | SD | ||
| Total population | 1500 | 2501 | 737 | 3025 | 456 | 6.25 | 1.85 | 7.56 | 1.14 | 3055 | 886 | 3761 | 685 | 0.89 | 0.89 |
| 18–35 years | 531 | 2687 | 758 | 3053 | 459 | 6.71 | 1.91 | 7.63 | 1.15 | 3036 | 945 | 3450 | 584 | 0.97 | 0.22 |
| 36–50 years | 437 | 2508 | 733 | 3049 | 452 | 6.27 | 1.85 | 7.63 | 1.13 | 3098 | 873 | 3839 | 650 | 0.88 | 0.20 |
| 51–64 years | 306 | 2363 | 670 | 2926 | 439 | 5.91 | 1.68 | 7.31 | 1.10 | 3138 | 851 | 3971 | 678 | 0.81 | 0.19 |
| 65+ years | 226 | 2236 | 653 | 3045 | 460 | 5.59 | 1.64 | 7.61 | 1.15 | 2904 | 790 | 4054 | 699 | 0.83 | 0.20 |
| Men | 740 | 2877 | 696 | 3022 | 456 | 7.19 | 1.76 | 7.56 | 1.14 | 3417 | 864 | 3621 | 624 | 0.92 | 0.21 |
| 18–35 years | 276 | 3073 | 698 | 2988 | 450 | 7.67 | 1.77 | 7.47 | 1.13 | 3522 | 872 | 3432 | 585 | 0.96 | 0.22 |
| 36–50 years | 205 | 2932 | 671 | 3080 | 454 | 7.33 | 1.70 | 7.71 | 1.14 | 3466 | 853 | 3670 | 608 | 0.92 | 0.21 |
| 51–64 years | 153 | 2671 | 640 | 2925 | 440 | 6.67 | 1.62 | 7.31 | 1.10 | 3402 | 848 | 3768 | 624 | 0.85 | 0.19 |
| 65+ years | 106 | 2562 | 619 | 3137 | 458 | 6.40 | 1.56 | 7.84 | 1.15 | 3070 | 794 | 3803 | 623 | 0.91 | 0.20 |
| Women | 760 | 2134 | 572 | 3027 | 455 | 5.33 | 1.43 | 7.57 | 1.14 | 2703 | 756 | 3897 * | 714 | 0.86 | 0.22 |
| 18–35 years | 255 | 2270 | 579 | 3123 * | 458 | 5.67 | 1.46 | 7.81 | 1.15 | 2510 | 710 | 3470 * | 583 | 0.99 | 0.22 |
| 36–50 years | 232 | 2134 | 561 | 3022 * | 449 | 5.33 | 1.41 | 7.55 | 1.12 | 2773 | 754 | 3988 * | 649 | 0.84 | 0.19 |
| 51–64 years | 153 | 2056 | 548 | 2926 | 437 | 5.14 | 1.37 | 7.32 | 1.09 | 2875 | 767 | 4174 * | 669 | 0.77 | 0.18 |
| 65+ years | 120 | 1948 | 536 | 2965 * | 446 | 4.87 | 1.34 | 7.40 | 1.11 | 2758 | 756 | 4276 * | 688 | 0.76 | 0.18 |
| Low | Medium | High | P Value | ||||
|---|---|---|---|---|---|---|---|
| n = 499 | n = 502 | n = 499 | |||||
| Mean | SD | Mean | SD | Mean | SD | ||
| Dietary Na:K (mmol/mmol) | 1.0 | 0.2 | 1.4 | 0.2 | 1.9 | 0.3 | 0.000 |
| Mean daily intake of sodium (mg) | 1993 | 705 | 2556 | 782 | 2947 | 938 | 0.000 |
| Mean daily intake of potassium (mg) | 3432 | 1163 | 3112 | 887 | 2621 | 816 | 0.000 |
| Food group intakes (g/d) | |||||||
| Grains, rice, pasta and savouries | 60.2 | 75.8 | 59.8 | 68.8 | 59.6 | 69.6 | 0.756 |
| Breads | 89.5 | 54.2 | 118.5 | 59.0 | 138.6 | 65.4 | 0.000 |
| Breakfast cereals | 81.5 | 95.2 | 61.4 | 79.4 | 42.8 | 60.7 | 0.000 |
| Biscuits, cakes and pastries | 28.7 | 34.6 | 31.3 | 35.3 | 28.7 | 35.0 | 0.165 |
| Milk | 244 | 213 | 223 | 188 | 163 | 143 | 0.000 |
| Yogurt | 37.8 | 53.7 | 38.6 | 59.0 | 20.5 | 40.6 | 0.000 |
| Creams, ice-creams and chilled desserts | 22.5 | 38.1 | 22.2 | 36.9 | 17.9 | 32.9 | 0.042 |
| Cheeses | 11.0 | 15.4 | 14 | 17.6 | 15.8 | 19.8 | 0.002 |
| Butter, spreading fats and oils | 10.7 | 11.0 | 14.3 | 13.8 | 20.9 | 21.0 | 0.000 |
| Eggs and egg dishes | 15.3 | 23.2 | 15.9 | 21.9 | 18.7 | 25.9 | 0.069 |
| Potatoes and potato products | 138 | 96.5 | 125 | 78.5 | 98.1 | 75.1 | 0.000 |
| Vegetables and vegetable dishes | 132 | 101 | 112 | 72.0 | 98.5 | 68.8 | 0.000 |
| Fruit | 135 | 135 | 95.9 | 109 | 28.8 | 76.6 | 0.000 |
| Fruit juices | 62.3 | 104 | 52.0 | 84.8 | 34.2 | 68.3 | 0.000 |
| Fish and fish dishes | 33.0 | 44.6 | 29.2 | 39.5 | 24.0 | 37.0 | 0.002 |
| Meat and meat dishes | 166 | 96.1 | 181 | 97.2 | 189 | 103 | 0.001 |
| Cured and processed meat | 38.6 | 39.4 | 57.3 | 51.4 | 80.5 | 61.6 | 0.000 |
| Fresh meat | 68.9 | 59.8 | 57.0 | 48.4 | 47.9 | 45.3 | 0.000 |
| Meat dishes | 58.6 | 77.9 | 66.5 | 79.4 | 61.1 | 77.6 | 0.138 |
| Beverages | 1628 | 936 | 1507 | 823 | 1368 | 787 | 0.098 |
| Alcoholic beverages | 351 | 623 | 322 | 589 | 228 | 423 | 0.021 |
| Tea | 449 | 429 | 470 | 403 | 419 | 386 | 0.056 |
| Coffee | 144 | 236 | 117 | 191 | 111 | 207 | 0.016 |
| Other beverages | 683 | 666 | 598 | 609 | 609 | 621 | 0.086 |
| Sugars, confectionery, jams and savoury snacks | 28.7 | 29.9 | 30.2 | 26.4 | 29.7 | 27.8 | 0.201 |
| Soups and sauces | 56.9 | 75.1 | 56.5 | 64.1 | 56.6 | 65.9 | 0.323 |
| Nuts and seeds, herbs and spices | 4.1 | 12.0 | 2.8 | 8.8 | 1.8 | 5.9 | 0.000 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morrissey, E.; Giltinan, M.; Kehoe, L.; Nugent, A.P.; McNulty, B.A.; Flynn, A.; Walton, J. Sodium and Potassium Intakes and Their Ratio in Adults (18–90 y): Findings from the Irish National Adult Nutrition Survey. Nutrients 2020, 12, 938. https://doi.org/10.3390/nu12040938
Morrissey E, Giltinan M, Kehoe L, Nugent AP, McNulty BA, Flynn A, Walton J. Sodium and Potassium Intakes and Their Ratio in Adults (18–90 y): Findings from the Irish National Adult Nutrition Survey. Nutrients. 2020; 12(4):938. https://doi.org/10.3390/nu12040938
Chicago/Turabian StyleMorrissey, Eoin, Miriam Giltinan, Laura Kehoe, Anne P. Nugent, Breige A. McNulty, Albert Flynn, and Janette Walton. 2020. "Sodium and Potassium Intakes and Their Ratio in Adults (18–90 y): Findings from the Irish National Adult Nutrition Survey" Nutrients 12, no. 4: 938. https://doi.org/10.3390/nu12040938
APA StyleMorrissey, E., Giltinan, M., Kehoe, L., Nugent, A. P., McNulty, B. A., Flynn, A., & Walton, J. (2020). Sodium and Potassium Intakes and Their Ratio in Adults (18–90 y): Findings from the Irish National Adult Nutrition Survey. Nutrients, 12(4), 938. https://doi.org/10.3390/nu12040938