Reversal of Prediabetes in Saudi Adults: Results from an 18 Month Lifestyle Intervention

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
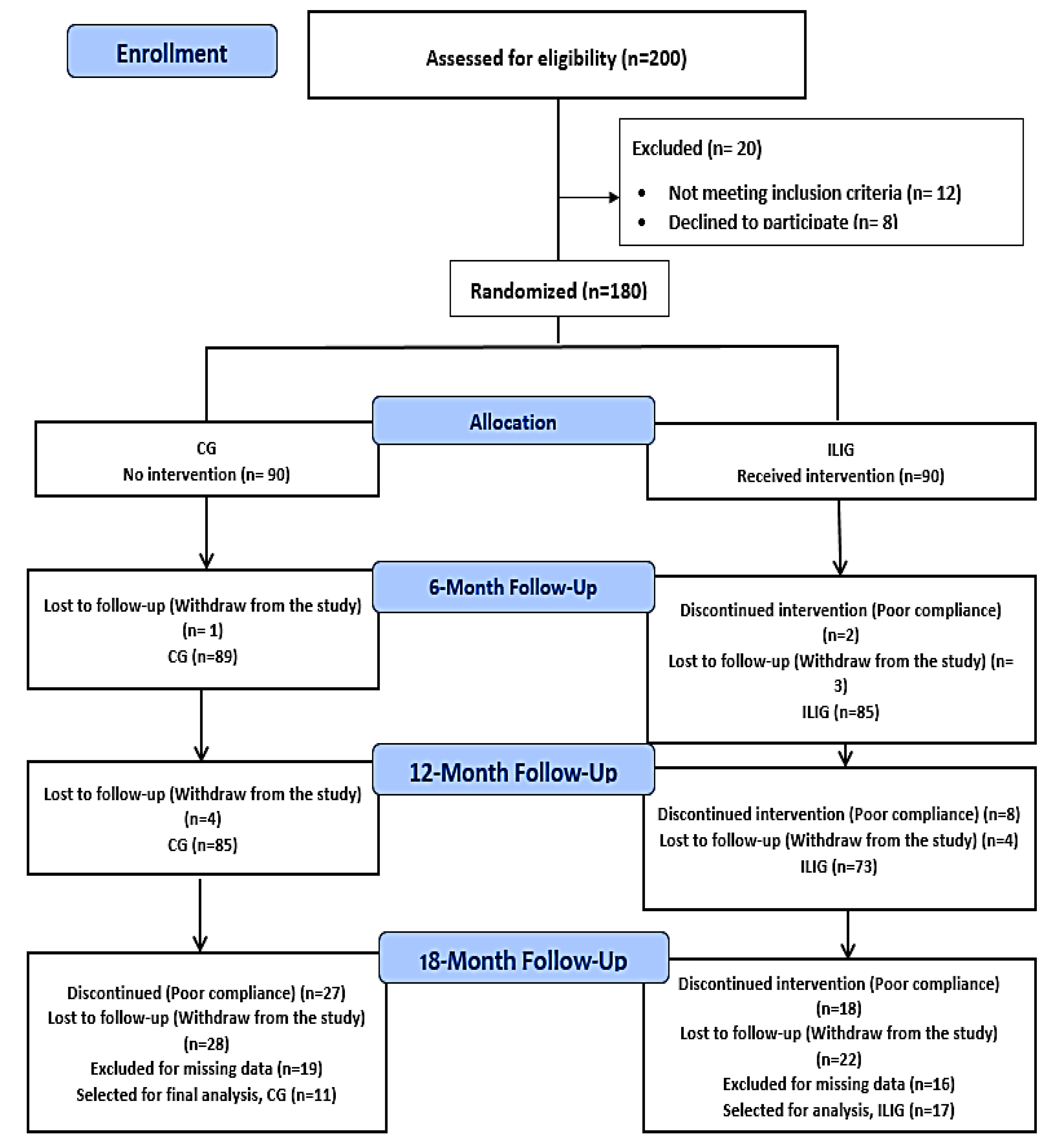
2.1. Participants
2.2. Intervention
2.3. Anthropometric and Biochemical Parameters
2.4. Statistical Analyses
3. Results
3.1. Anthropometric and Biochemical Characteristics Overtime
3.2. Primary Outcome: Reversion to Normoglycemia
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. IDF Diabetes Atlas Committee. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed]
- Tabak, A.G.; Herder, C.; Rathmann, W.; Brunner, E.J.; Kivimaki, M. Prediabetes: A High-Risk State for Diabetes Development. Lancet (Lond. Engl.) 2012, 379, 2279–2290. [Google Scholar] [CrossRef]
- Diabetes Prevention Program Research Group. The Prevalence of Retinopathy in Impaired Glucose Tolerance and Recent-Onset Diabetes in the Diabetes Prevention Program. Diabet. Med. 2007, 24, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Zhao, G.; Li, C. Pre-Diabetes and the Risk for Cardiovascular Disease: A Systematic Review of the Evidence. J. Am. Coll. Cardiol. 2010, 55, 1310–1317. [Google Scholar] [CrossRef]
- World Health Organization. Chapter 1- Chronic diseases: Causes and health impacts. In Preventing Chronic Diseases: A Vital Investment; World Health Organization: Geneva, Switzerland, 2005; pp. 34–58. [Google Scholar]
- Babiker, A.M.I.; Al Jurayyan, N.A.M.; Al Jurayyan, R.N.A.; Al Gadi, I.; Drop, S.L.S. The Clinical Pattern of Diabetes Insipidus in a Large University Hospital in the Middle East. J. Trop. Pediatr. 2015, 61, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Al-Herbish, A.S.; El-Mouzan, M.I.; Al-Salloum, A.A.; Al-Qurachi, M.M.; Al-Omar, A.A. Prevalence of Type 1 Diabetes Mellitus in Saudi Arabian Children and Adolescents. Saudi Med. J. 2008, 29, 1285–1288. [Google Scholar]
- Aljohani, N.J. Metabolic Syndrome: Risk Factors among Adults in Kingdom of Saudi Arabia. J. Fam. Community Med. 2014, 21, 170–175. [Google Scholar] [CrossRef]
- Al-Rubeaan, K.; Abu El-Asrar, A.M.; Youssef, A.M.; Subhani, S.N.; Ahmad, N.A.; Al-Sharqawi, A.H.; Alguwaihes, A.; Alotaibi, M.S.; Al-Ghamdi, A.; Ibrahim, H.M. Diabetic Retinopathy and Its Risk Factors in a Society with a Type 2 Diabetes Epidemic: A Saudi National Diabetes Registry-Based Study. Acta Ophthalmol. 2015, 93, e140–e147. [Google Scholar] [CrossRef]
- Alzaid, A. Diabetes: A Tale of Two Cultures. Br. J. Diabetes Vasc. Dis. 2012, 12, 57–59. [Google Scholar] [CrossRef]
- Alqurashi, K.A.; Aljabri, K.S.; Bokhari, S.A. Prevalence of Diabetes Mellitus in a Saudi Community. Ann. Saudi Med. 2011, 31, 19–23. [Google Scholar] [CrossRef]
- Al-Nozha, M.M.; Al-Maatouq, M.A.; Al-Mazrou, Y.Y.; Al-Harthi, S.S.; Arafah, M.R.; Khalil, M.Z.; Khan, N.B.; Al-Khadra, A.; Al-Marzouki, K.; Nouh, M.S.; et al. Diabetes Mellitus in Saudi Arabia. Saudi Med. J. 2004, 25, 1603–1610. [Google Scholar] [PubMed]
- Li, G.; Zhang, P.; Wang, J.; Gregg, E.W.; Yang, W.; Gong, Q.; Li, H.; Li, H.; Jiang, Y.; An, Y.; et al. The Long-Term Effect of Lifestyle Interventions to Prevent Diabetes in the China Da Qing Diabetes Prevention Study: A 20-Year Follow-up Study. Lancet (Lond. Engl.) 2008, 371, 1783–1789. [Google Scholar] [CrossRef]
- Pan, X.R.; Li, G.W.; Hu, Y.H.; Wang, J.X.; Yang, W.Y.; An, Z.X.; Hu, Z.X.; Lin, J.; Xiao, J.Z.; Cao, H.B.; et al. Effects of Diet and Exercise in Preventing NIDDM in People with Impaired Glucose Tolerance. The Da Qing IGT and Diabetes Study. Diabetes Care 1997, 20, 537–544. [Google Scholar] [CrossRef]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M. Reduction in the Incidence of Type 2 Diabetes with Lifestyle Intervention or Metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef]
- Tuomilehto, J.; Lindstrom, J.; Eriksson, J.G.; Valle, T.T.; Hamalainen, H.; Ilanne-Parikka, P.; Keinanen-Kiukaanniemi, S.; Laakso, M.; Louheranta, A.; Rastas, M.; et al. Prevention of Type 2 Diabetes Mellitus by Changes in Lifestyle among Subjects with Impaired Glucose Tolerance. N. Engl. J. Med. 2001, 344, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Lindstrom, J.; Ilanne-Parikka, P.; Peltonen, M.; Aunola, S.; Eriksson, J.G.; Hemio, K.; Hamalainen, H.; Harkonen, P.; Keinanen-Kiukaanniemi, S.; Laakso, M.; et al. Sustained Reduction in the Incidence of Type 2 Diabetes by Lifestyle Intervention: Follow-up of the Finnish Diabetes Prevention Study. Lancet (Lond. Engl.) 2006, 368, 1673–1679. [Google Scholar] [CrossRef]
- Ramachandran, A.; Snehalatha, C.; Mary, S.; Mukesh, B.; Bhaskar, A.D.; Vijay, V. The Indian Diabetes Prevention Programme Shows That Lifestyle Modification and Metformin Prevent Type 2 Diabetes in Asian Indian Subjects with Impaired Glucose Tolerance (IDPP-1). Diabetologia 2006, 49, 289–297. [Google Scholar] [CrossRef]
- Al-Hamdan, R.; Avery, A.; Salter, A.; Al-Disi, D.; Al-Daghri, N.M.; McCullough, F. Identification of education models to improve health outcomes in Arab women with pre-diabetes. Nutrients 2020, 11, 1113. [Google Scholar] [CrossRef]
- Wani, K.; Alfawaz, H.; Alnaami, A.M.; Sabico, S.; Khattak, M.N.K.; Al-Attas, O.; Alokail, M.S.; Alharbi, M.; Chrousos, G.P.; Kumar, S.; et al. Effects of a 12-month intensive lifestyle monitoring program in predominantly overweight/obese Arab adults with prediabetes. Nutrients 2020, 12, 464. [Google Scholar] [CrossRef]
- American Diabetes Association. Standards of Medical Care in Diabetes. Diabetes Care 2017, 40. Available online: http://care.diabetesjournals.org/content/diacare/suppl/2016/12/15/40.Supplement_1.DC1/DC_40_S1_final.pdf (accessed on 2 May 2019).
- Kosaka, K.; Noda, M.; Kuzuya, T. Prevention of Type 2 Diabetes by Lifestyle Intervention: A Japanese Trial in IGT Males. Diabetes Res. Clin. Pract. 2005, 67, 152–162. [Google Scholar] [CrossRef]
- Moore, S.M.; Hardie, E.A.; Hackworth, N.J.; Critchley, C.R.; Kyrios, M.; Buzwell, S.A.; Crafti, N.A. Can the onset of type 2 diabetes be delayed by a group-based lifestyle intervention? A randomized control trial. Psychol. Health 2011, 26, 485–499. [Google Scholar] [CrossRef]
- Okada, R.; Tsushita, K.; Wakai, K.; Ishizaka, Y.; Kato, K.; Wada, T.; Watanabe, K. Lower Risk of Progression from Prediabetes to Diabetes with Health Checkup with Lifestyle Education: Japan Ningen Dock Study. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 679–687. [Google Scholar] [CrossRef] [PubMed]
- Wing, R.R.; Hamman, R.F.; Bray, G.A.; Delahanty, L.; Edelstein, S.L.; Hill, J.O.; Horton, E.S.; Hoskin, M.A.; Kriska, A.; Lachin, J.; et al. Achieving Weight and Activity Goals among Diabetes Prevention Program Lifestyle Participants. Obes. Res. 2004, 12, 1426–1434. [Google Scholar] [CrossRef] [PubMed]
- Hamman, R.F.; Wing, R.R.; Edelstein, S.L.; Lachin, J.M.; Bray, G.A.; Delahanty, L.; Hoskin, M.; Kriska, A.M.; Mayer-Davis, E.J.; Pi-Sunyer, X.; et al. Effect of Weight Loss with Lifestyle Intervention on Risk of Diabetes. Diabetes Care 2006, 29, 2102–2107. [Google Scholar] [CrossRef] [PubMed]
- Knowler, W.C.; Fowler, S.E.; Hamman, R.F.; Christophi, C.A.; Hoffman, H.J.; Brenneman, A.T.; Brown-Friday, J.O.; Goldberg, R.; Venditti, E.; Nathan, D.M. 10-Year Follow-up of Diabetes Incidence and Weight Loss in the Diabetes Prevention Program Outcomes Study. Lancet (Lond. Engl.) 2009, 374, 1677–1686. [Google Scholar] [CrossRef]
- Perreault, L.; Kahn, S.E.; Christophi, C.A.; Knowler, W.C.; Hamman, R.F. Regression from Pre-Diabetes to Normal Glucose Regulation in the Diabetes Prevention Program. Diabetes Care 2009, 32, 1583–1588. [Google Scholar] [CrossRef]
- Giannopoulou, I.; Ploutz-Snyder, L.L.; Carhart, R.; Weinstock, R.S.; Fernhall, B.; Goulopoulou, S.; Kanaley, J.A. Exercise is Required for Visceral Fat Loss in Postmenopausal Women with Type 2 Diabetes. J. Clin. Endocrinol. Metab. 2005, 90, 1511–1518. [Google Scholar] [CrossRef]
- Chan, J.M.; Rimm, E.B.; Colditz, G.A.; Stampfer, M.J.; Willett, W.C. Obesity, Fat Distribution, and Weight Gain as Risk Factors for Clinical Diabetes in Men. Diabetes Care 1994, 17, 961–969. [Google Scholar] [CrossRef]
- Colditz, G.A.; Willett, W.C.; Rotnitzky, A.; Manson, J.E. Weight Gain as a Risk Factor for Clinical Diabetes Mellitus in Women. Ann. Intern. Med. 1995, 122, 481–486. [Google Scholar] [CrossRef]
- Mann, J.I. Evidence-Based Nutrition Recommendations for the Treatment and Prevention of Type 2 Diabetes and the Metabolic Syndrome. Food Nutr. Bull. 2006, 27, 161–166. [Google Scholar] [CrossRef]
- Conn, V.S.; Hafdahl, A.R.; Mehr, D.R.; LeMaster, J.W.; Brown, S.A.; Nielsen, P.J. Metabolic Effects of Interventions to Increase Exercise in Adults with Type 2 Diabetes. Diabetologia 2007, 50, 913–921. [Google Scholar] [CrossRef] [PubMed]
- Perreault, L.; Pan, Q.; Mather, K.J.; Watson, K.E.; Hamman, R.F.; Kahn, S.E. Effect of Regression from Prediabetes to Normal Glucose Regulation on Long-Term Reduction in Diabetes Risk: Results from the Diabetes Prevention Program Outcomes Study. Lancet (Lond. Engl.) 2012, 379, 2243–2251. [Google Scholar] [CrossRef]
- Sabico, S.; Al-Mashharawi, A.; Al-Daghri, N.M.; Wani, K.; Amer, O.E.; Hussain, D.S.; Ahmed Ansari, M.G.; Masoud, M.S.; Alokail, M.S.; McTernan, P.G. Effects of a 6-month multi-strain probiotics supplementation in endotoxemic, inflammatory and cardiometabolic status of T2DM patients: A randomized, double-blind, placebo-controlled trial. Clin. Nutr. 2019, 38, 1561–1569. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Lifestyle Intervention | CG | ILIG |
|---|---|---|
| Baseline Weight reduction (≥5%) Exercise (150 min/week) Reduce fat intake (<30% of total energy) Increase fiber intake (15 g/1000 kcal) diet | Given as a pamphlet and booklet to all participants as a group | Individually explained to each participant by a registered dietitian |
| Bimonthly lifestyle education sessions every 4 months Dietary counselling Dietary intake record Mode of follow-up On demand support system Blood collection Anthropometrics | No None None As a group No Baseline and every 6 months Baseline and every 6 months | Yes Baseline and every 6 months Baseline and every 6 months Individually Yes Baseline and every 6 months Baseline and every 6 months |
| Parameters | Control | ILIG | p-Values |
|---|---|---|---|
| N | 85 | 73 | |
| Age (years) | 42.3 ± 11.3 | 43.4 ± 7.8 | 0.48 |
| Female/Male | 64/21 | 51/22 | 0.48 |
| BMI (kg/m2) | 32.6 ± 5.8 | 31.3 ± 6.4 | 0.19 |
| Weight (kg) | 81.7 ± 13.9 | 79.6 ± 16.0 | 0.17 |
| Waist (cm) | 95.6 ± 6.8 | 97.9 ± 13.0 | 0.38 |
| WHR | 0.9 ± 0.0 | 0.9 ± 0.1 | 0.60 |
| Systolic BP (mmHg) | 120.0 ± 12.1 | 122.1 ± 15.8 | 0.36 |
| Diastolic BP (mmHg) | 76.4 ± 9.7 | 76.0 ± 11.9 | 0.87 |
| Glucose (mmol/L) | 6.0 ± 0.4 | 6.1 ± 0.4 | 0.18 |
| Insulin (uU/mL) | 15.1 ± 5.0 | 15.9 ± 2.6 | 0.24 |
| HOMA-IR | 4.1 ± 1.4 | 4.3 ± 0.8 | 0.27 |
| Parameters | Control (N = 85) | Intervention (N = 73) | Between Groups | ||||
|---|---|---|---|---|---|---|---|
| Baseline (N = 85) | 6 Months (N = 85) | 12 Months (N = 85) | Baseline (N = 73) | 6 Months (N = 73) | 12 Months (N = 73) | p-Values | |
| Age (years) | 42.3 ± 11.3 | 43.4 ± 7.8 | -- | ||||
| Female/Male | 64/21 | 51/22 | -- | ||||
| BMI (kg/m2) | 32.6 ± 5.8 | 32.8 ± 5.9 | 32.8 ± 5.7 | 31.3 ± 6.4 | 31.0 ± 6.7 | 30.6 ± 6.6 AB | 0.07 |
| Weight (kg) | 81.7 ± 13.9 | 82.3 ± 13.9 | 82.2 ± 13.4 | 79.6 ± 16.0 | 78.7 ± 15.9 | 77.7 ± 16.2 AB | 0.15 |
| Waist (cm) | 95.6 ± 6.8 | 95.7 ± 6.7 | 95.5 ± 6.2 | 97.9 ± 13.0 | 97.7 ± 13.5 | 96.3 ± 13.0 AB | 0.28 |
| WHR | 0.9 ± 0.0 | 0.9 ± 0.1 | 0.9 ± 0.1 | 0.9 ± 0.1 | 0.9 ± 0.1 | 0.9 ± 0.1 | 0.41 |
| Systolic BP (mmHg) | 120.0 ± 12.1 | 118.8 ± 13.4 | 119.2 ± 15.8 | 122.1 ± 15.8 | 120.9 ± 16.8 | 119.5 ± 16.6 | 0.50 |
| Diastolic BP (mmHg) | 76.4 ± 9.7 | 75.4 ± 9.1 | 77.1 ± 13.7 | 76.0 ± 11.9 | 75.1 ± 10.8 | 75.9 ± 12.8 | 050 |
| Glucose (mmol/L) | 6.0 ± 0.4 | 6.1 ± 0.7 | 5.9 ± 0.9 | 6.1 ± 0.4 | 5.7 ± 0.8 A | 5.7 ± 0.8 A | 0.03 |
| Insulin (uU/mL) | 15.1 ± 5.0 | 15.1 ± 6.1 | 15.2 ± 6.0 | 15.9 ± 2.6 | 15.3 ± 2.9 | 15.1 ± 2.5 | 0.67 |
| HOMA-IR | 4.1 ± 1.4 | 4.1 ± 1.6 | 4.0 ± 1.6 | 4.3 ± 0.8 | 3.8 ± 0.8 A | 3.8 ± 0.8 A | 0.66 |
| 6 Months | 12 Months | 18 Months | |||||||
|---|---|---|---|---|---|---|---|---|---|
| CG | ILIG | p-Value | CG | ILIG | p-Value | CG | ILIG | p-Value | |
| N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | ||||
| T2DM | 6 (7.1) | 6 (8.2) | 0.04 | 6 (7.1) | 5 (6.8) | 0.02 | 2 (18.2) | 0 (0.0) | 0.18 |
| Pre-DM | 66 (77.6) | 44 (60.3) | 53 (62.4) | 30 (41.1) | 4 (36.4) | 5 (29.4) | |||
| Normal | 13 (15.3) | 23 (31.5) | 26 (30.6) | 38 (52.1) | 5 (45.5) | 12 (70.6) | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amer, O.E.; Sabico, S.; Alfawaz, H.A.; Aljohani, N.; Hussain, S.D.; Alnaami, A.M.; Wani, K.; Al-Daghri, N.M. Reversal of Prediabetes in Saudi Adults: Results from an 18 Month Lifestyle Intervention. Nutrients 2020, 12, 804. https://doi.org/10.3390/nu12030804
Amer OE, Sabico S, Alfawaz HA, Aljohani N, Hussain SD, Alnaami AM, Wani K, Al-Daghri NM. Reversal of Prediabetes in Saudi Adults: Results from an 18 Month Lifestyle Intervention. Nutrients. 2020; 12(3):804. https://doi.org/10.3390/nu12030804
Chicago/Turabian StyleAmer, Osama E., Shaun Sabico, Hanan A. Alfawaz, Naji Aljohani, Syed Danish Hussain, Abdullah M. Alnaami, Kaiser Wani, and Nasser M. Al-Daghri. 2020. "Reversal of Prediabetes in Saudi Adults: Results from an 18 Month Lifestyle Intervention" Nutrients 12, no. 3: 804. https://doi.org/10.3390/nu12030804
APA StyleAmer, O. E., Sabico, S., Alfawaz, H. A., Aljohani, N., Hussain, S. D., Alnaami, A. M., Wani, K., & Al-Daghri, N. M. (2020). Reversal of Prediabetes in Saudi Adults: Results from an 18 Month Lifestyle Intervention. Nutrients, 12(3), 804. https://doi.org/10.3390/nu12030804