Macronutrients in Parenteral Nutrition: Amino Acids

 ,
, 
 ,
,  ,
,
Abstract
1. Introduction
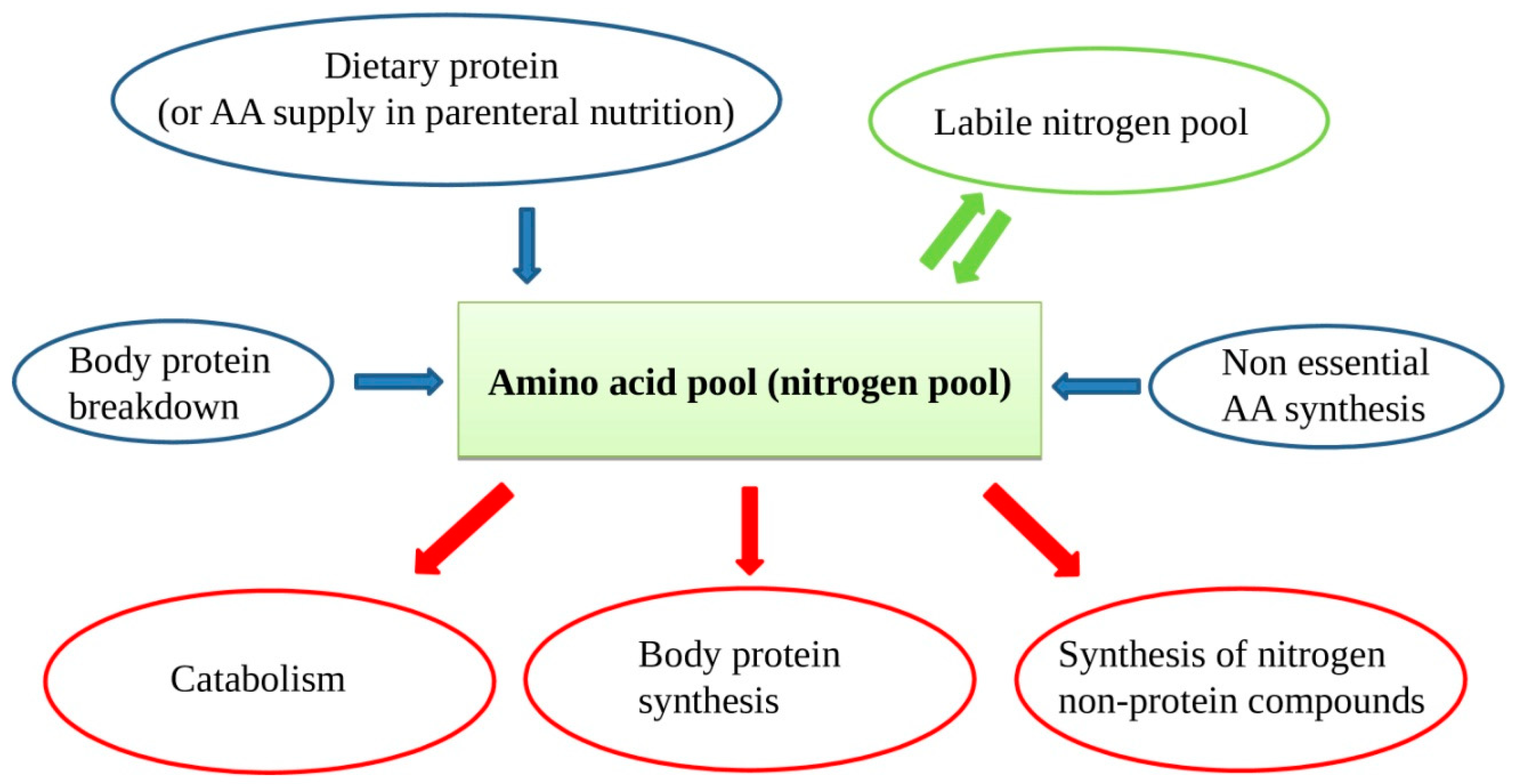
2. Amino Acids: Physiology
3. Amino Acid Solutions for Parenteral Nutrition
4. Disease-Specific AA Mixture
5. Protein Requirement
6. Amino Acid Requirement in Parenteral Nutrition
7. Amino Acid Requirement for Adult Patients without Organ Failure
8. Adult Patients with Cancer
9. Liver Failure
10. Chronic Intestinal Failure
11. Renal Failure
12. Pediatric Patients
13. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Staun, M.; Pironi, L.; Bozzetti, F.; Baxter, J.; Forbes, A.; Joly, F.; Jeppesen, P.; Moreno, J.; Hébuterne, X.; Pertkiewicz, M.; et al. ESPEN Guidelines on Parenteral Nutrition: Home parenteral nutrition (HPN) in adult patients. Clin. Nutr. 2009, 28, 467–479. [Google Scholar] [CrossRef] [PubMed]
- Scanzano, C.; Iacone, R.; Alfonsi, L.; Santarpia, L.; Negro, G.; Pastore, E.; Iervolino, M.; Pagano, M.C.; Galeotalanza, M.R.; Sgambati, D.; et al. Home Artificia Lnutrition in a Specialized Adult Clinical Nutrition Centre: Overview 2011. Nutr. Ther. Metab. 2013, 31, 69–76. [Google Scholar] [CrossRef]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.; et al. ESPEN Guideline: Clinicalnutrition in Surgery. Clin. Nutr. 2017, 36, 623–650. [Google Scholar] [CrossRef]
- Abunnaja, S.; Cuviello, A.; Sanchez, J.A. Enteral and Parenteral Nutrition in the Perioperative Period: State of the Art. Nutrients 2013, 5, 608–623. [Google Scholar] [CrossRef] [PubMed]
- Iresjö, B.M.; Engström, C.; Lundholm, K. Preoperative Overnight Parenteral Nutrition (TPN) Improves Skeletal Muscle Protein Metabolism Indicated by Microarray Algorithm Analyses in a Randomized Trial. Physiol. Rep. 2016, 4, e12789. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.C.; Martindale, R.G.; Kiraly, L.N.; Jones, C.M. Nutrition Optimization Prior to Surgery. Nutr. Clin. Pract. 2014, 29, 10–21. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Zhou, F.X.; Lan, T.; Xu, H.; Yang, X.X.; Xie, C.H.; Dai, J.; Fu, Z.M.; Gao, Y.; Chen, L.L. Optimal Postoperative Nutrition Support for Patients with Gastrointestinal Malignancy: A Systematic Review and Meta-Analysis. Clin. Nutr. 2017, 36, 710–721. [Google Scholar] [CrossRef] [PubMed]
- Burneikis, D.; Stocchi, L.; Steiger, E.; Jezerski, D.; Shawki, S. Parenteral Nutrition Instead of Early Reoperation in the Management of Early Postoperative Small Bowel Obstruction. J. Gastrointest. Surg. 2020, 24, 109–114. [Google Scholar] [CrossRef]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN Guidelines on Nutrition in Cancer Patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef]
- Chao, P.C.; Lin, C.F.; Chuang, H.J. Parenteral Nutrition Combined with Enteral Feeding Improves the Outcome of Cancer Patients. Asia Pac. J. Clin. Nutr. 2017, 26, 1032–1038. [Google Scholar] [CrossRef]
- Orrevall, Y. Parenteral Nutrition in the Elderly Cancer Patient. Nutrition 2015, 31, 610–611. [Google Scholar] [CrossRef] [PubMed]
- Bozzetti, F.; Arends, J.; Lundholm, K.; Micklewright, A.; Zurcher, G.; Muscaritoli, M. ESPEN Guidelines on Parenteral Nutrition: Non-Surgical Oncology. Clin. Nutr. 2009, 28, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Scanzano, C.; Iacone, R.; Alfonsi, L.; Galeotalanza, M.R.; Sgambati, D.; Pastore, E.; D’Isanto, A.; Fierro, F.; Contaldo, F.; Santarpia, L. Composition of Personalized and Standard Nutritional Mixtures in Patients on Home Parenteral Nutrition. Eur. J. Clin. Nutr. 2014, 68, 433–436. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wu, G. Amino Acids: Metabolism, Functions, and Nutrition. Amino Acids. 2009, 37, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Darmaun, D.; Lapillonne, A.; Simeoni, U.; Picaud, J.C.; Rozé, J.C.; Saliba, E.; Bocquet, A.; Chouraqui, J.P.; Dupont, C.; Feillet, F.; et al. Parenteral Nutrition for Preterm Infants: Issues and Strategy. Arch. Pediatr. 2018, 25, 286–294. [Google Scholar] [CrossRef]
- Munro, H.N. Mammalian Protein Metabolism; Munro, H.N., Allison, J.B., Eds.; Academic Press, Inc.: New York, NY, USA, 1964. [Google Scholar]
- Wolfe, R.R. Branched-Chain Amino Acids and Muscle Protein Synthesis in Humans: Myth or Reality? J. Int. Soc. Sports Nutr. 2017, 14, 30. [Google Scholar] [CrossRef]
- Volpi, E.; Kobayashi, H.; Sheffield-Moore, M.; Mittendorfer, B.; Wolfe, R.R. Essential Amino Acids are Primarily Responsible for the Amino Acid Stimulation of Muscle Protein Anabolism in Healthy Elderly adults. Am. J. Clin. Nutr. 2003, 78, 250–258. [Google Scholar] [CrossRef]
- Cohen, S.; Nathan, J.A.; Goldberg, A.L. Muscle Wasting in Disease: Molecular Mechanisms and Promising Therapies. Nat. Rev. Drug Discov. 2015, 14, 58–74. [Google Scholar] [CrossRef]
- Yarandi, S.S.; Zhao, V.M.; Hebbar, G.; Ziegler, T.R. Amino Acid Composition in Parenteral Nutrition: What is the Evidence? Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 75–82. [Google Scholar] [CrossRef]
- Iacone, R.; Scanzano, C.; Santarpia, L.; Alfonsi, L.; Marra, M.; Pagano, M.C.; D’Isanto, A.; Frangipane, I.; Vitalone, A.; D’Angeli, M.; et al. Essential Amino Acid Profile in ParenteralNutritionMixtures: DoesItMeetNeeds? Nutrients 2018, 10, E1937. [Google Scholar] [CrossRef]
- Hoffer, L.J. Parenteral Nutrition: Amino Acids. Nutrients 2017, 9, E257. [Google Scholar] [CrossRef] [PubMed]
- Reeds, P.J.; Burrin, D.G.; Stoll, B.; Jahoor, F.; Wykes, L.; Henry, J.; Frazer, M.E. Enteral Glutamate is the Preferential Source for Mucosal Glutathione Synthesis in Fed Piglets. Am. J. Physiol. 1997, 273, E408e15. [Google Scholar] [CrossRef] [PubMed]
- Kopple, J.D. Phenylalanine and Tyrosine Metabolism in Chronic Kidney Failure. J. Nutr. 2007, 137, 1586S–1590S. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.A.; Ball, R.O.; Moore, A.M.; Filler, R.M.; Pencharz, P.B. The Effect of Graded Intake of glycyl-L-Tyrosine on Phenylalanine and Tyrosine Metabolism in Parenterally Fed Neonates with an Estimation of Tyrosine Requirement. Pediatr. Res. 2001, 49, 111–119. [Google Scholar] [CrossRef]
- Di Buono, M.; Wykes, L.J.; Ball, R.O.; Pencharz, P.B. Dietary Cysteine Reduces the Methionine Requirement in Men. Am. J. Clin. Nutr. 2001, 74, 761–766. [Google Scholar] [CrossRef]
- Plauth, M.; Schuetz, T. Working Group for Developing the Guidelines for Parenteral Nutrition of The German Association for Nutritional Medicine. Hepatology-Guidelines on Parenteral Nutrition, Chapter 16. Ger. Med. Sci. 2009, 7. [Google Scholar] [CrossRef]
- McClave, S.A.; Taylor, B.E.; Martindale, R.G.; Warren, M.M.; Johnson, D.R.; Braunschweig, C.; McCarthy, M.S.; Davanos, E.; Rice, T.W.; Cresci, G.A.; et al. Society of Critical Care Medicine; American Society for Parenteral and Enteral Nutrition. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J. Parenter Enter. Nutr. 2016, 40, 159–211. [Google Scholar] [CrossRef]
- Cano, N.J.; Aparicio, M.; Brunori, G.; Carrero, J.J.; Cianciaruso, B.; Fiaccadori, E.; Lindholm, B.; Teplan, V.; Fouque, D.; Guarnieri, G. ESPEN Guidelines on Parenteral Nutrition: Adult Renal Failure. Clin. Nutr. 2009, 28, 401–414. [Google Scholar] [CrossRef]
- Kaluzny, L.; Szczepanik, M.; Siwinska-Mrozek, Z.; Borkowska-Klos, M.; Cichy, W.; Walkowiak, J. Parenteral Nutrition in Patients with Inborn Errors of Metabolism-a Therapeutic Problem. Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 1579–1582. [Google Scholar]
- van Goudoever, J.B.; Carnielli, V.; Darmaun, D.; Sainz de Pipaon, M. ESPGHAN/ESPEN/ESPR/CSPEN Working Group on Pediatric Parenteral Nutrition. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on Pediatric Parenteral Nutrition: Amino Acids. Clin. Nutr. 2018, 37, 2315–2323. [Google Scholar] [CrossRef]
- Hoffer, L.J. Protein Requirement in Critical Illness. Appl. Physiol. Nutr. Metab. 2016, 41, 573–576. [Google Scholar] [CrossRef] [PubMed]
- Hoffer, L.J.; Bistrian, B.R. Energy Deficit is Clinically Relevant for Critically Ill Patients: No. Intensive Care Med. 2015, 41, 339–341. [Google Scholar] [CrossRef] [PubMed]
- Looijaard, W.G.P.M.; Denneman, N.; Broens, B.; Girbes, A.R.J.; Weijs, P.J.M.; Oudemans-van Straaten, H.M. Achieving Protein Targets without Energy Overfeeding in Critically ill Patients: A Prospective Feasibility Study. Clin. Nutr. 2018. [Google Scholar] [CrossRef] [PubMed]
- VFraipont, J.C.P. Energy Estimation and Measurement in Critically ill Patients. J. Parenter Enter. Nutr. 2013, 37, 705–713. [Google Scholar] [CrossRef] [PubMed]
- Phillips, S.M.; Dickerson, R.N.; Moore, F.A.; Paddon-Jones, D.; Weijs, P.J. Protein Turnover and Metabolism in the Elderly Intensive Care unit Patient. Nutr. Clin. Pract. 2017, 32, 112s–120s. [Google Scholar] [CrossRef] [PubMed]
- Hoffer, L.J. High-Protein Hypocaloric Nutrition for Non-Obese Critically Ill Patients. Nutr. Clin. Pract. 2018, 33, 325–332. [Google Scholar] [CrossRef]
- Iacone, R.; Scanzano, C.; D’Isanto, A.; Vitalone, A.; Frangipane, I.; D’Angeli, M.; Santarpia, L.; Contaldo, F. Prediction of Renal Acid Load in Adult Patients on Parenteral Nutrition. Pharmaceutics 2018, 10, E43. [Google Scholar] [CrossRef]
- Jones, B.J.; Chopra, P.; Groning, J.; Deel-Smith, P. Acid-base Disturbance during Home Parenteral Nutrition—An Observational Cohort Study. e-SPEN Eur. e-J. Clin. Nutr. Metab. 2011, 6, e31–e35. [Google Scholar] [CrossRef][Green Version]
- Kato, K.; Sugiura, S.; Yano, K.; Fukuoka, T.; Itoh, A.; Nagino, M.; Nabeshima, T.; Yamada, K. The Latent Risk of Acidosis in Commercially Available Total Parenteral Nutrition (TPN) Products: A Randomized Clinical Trial in Postoperative Patients. J. Clin. Biochem. Nutr. 2009, 45, 68–73. [Google Scholar] [CrossRef]
- Buchman, A.L.; Moukarzel, A. Metabolic Bone Disease Associated with Total Parenteral Nutrition. Clin. Nutr. 2000, 19, 217–231. [Google Scholar] [CrossRef]
- Hamilton, C.; Seidner, D.L. Metabolic Bone Disease and Parenteral Nutrition. Curr. Gastroenterol. Rep. 2004, 6, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Joint WHO/FAO/UNU Expert Consultation. Protein and Amino Acid Requirements in Human Nutrition; World Health Organ Technical Report Series; WHO: Geneva, Switzerland, 2007; Volume 935, pp. 1–265. [Google Scholar]
- Tessari, P. Nitrogen Balance and Protein Requirements: Definition and Measurements. In Cachexia and Wasting: A Modern Approach; Mantovani, G., Ed.; Springer: Milano, Italy, 2006; pp. 73–79. [Google Scholar]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-Based Recommendations for Optimal Dietary Protein Intake in Older People: A Position Paper from the PROT-Age Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef] [PubMed]
- Millward, D.J. Macronutrient Intakes as Determinants of Dietary Protein and Amino Acid Adequacy. J. Nutr. 2004, 134, 1588S–1596S. [Google Scholar] [CrossRef] [PubMed]
- Millward, D.J. Identifying Recommended Dietary Allowances for Protein and Amino Acids: A Critique of the 2007 WHO/FAO/UNU Report. Br. J. Nutr. 2012, 108, S3–S21. [Google Scholar] [CrossRef]
- Scrimshaw, N.S.; Young, V.R. Adaptation to Low Protein and Energy Intakes. In Human Organization; Spring: Berlin/Heidelberg, Germany, 1989; Volume 48, pp. 20–30. Available online: https://www.jstor.org/stable/44125944 (accessed on 24 January 2020).
- Tomé, D.; Bos, C. Dietary Protein and Nitrogen Utilization. J. Nutr. 2000, 130, 1868S–1873S. [Google Scholar] [CrossRef]
- Young, V.R.; Marchini, J.S. Mechanisms and Nutritional Significance of Metabolic Responses to Altered Intakes of Protein and Amino Acids, with Reference to Nutritional Adaptation in Humans. Am. J. Clin. Nutr. 1990, 51, 270–289. [Google Scholar] [CrossRef]
- Millward, D.J. Metabolic demands for amino acids and the human dietary requirement: Millward and Rivers (1988) revisited. J. Nutr. 1998, 128, 2563S–2576S. [Google Scholar] [CrossRef]
- Millward, D.J. An Adaptive Metabolic Demand Model for Protein and Amino Acid Requirements. Br. J. Nutr. 2003, 90, 249–260. [Google Scholar] [CrossRef]
- Bodwell, C.E.; Schuster, E.M.; Kyle, E.; Brooks, B.; Womack, M.; Steele, P.; Ahrens, R. Obligatory Urinary and Fecal Nitrogen Losses in Young Women, Older Men, and Young Men and the Factorial Estimation of Adult Human Protein Requirements. Am. J. Clin. Nutr. 1979, 32, 2450–2459. [Google Scholar] [CrossRef]
- EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies). Scientific Opinion on Dietary Reference Values for protein. EFSA J. 2012, 10, 2557. Available online: https://efsa.onlinelibrary.wiley.com/doi/epdf/10.2903/j.efsa.2012.2557 (accessed on 24 January 2020). [CrossRef]
- Hoffer, L.J. How much protein do parenteral amino acid mixtures provide? Am. J. Clin. Nutr. 2011, 94, 1396–1398. [Google Scholar] [CrossRef] [PubMed]
- Joint FAO/WHO/UNU Expert Consultation. Energy and protein requirements. World Health Organization Technical Report Series 724. Available online: http://www.fao.org/3/aa040e/AA040E00.htm#TOC (accessed on 24 January 2020).
- Jeejeebhoy, K.N. Protein Nutrition in Clinical Practice. Br. Med. Bull. 1981, 37, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Kreymann, G.; DeLegge, M.H.; Luft, G.; Hise, M.E.; Zaloga, G.P. The Ratio of Energy Expenditure to Nitrogen Loss in Diverse Patient Groups-a Systematic Review. Clin Nutr. 2012, 31, 168–175. [Google Scholar] [CrossRef]
- Teruyoshi, A.; Mari, H.; Moeko, K.; Seiji, H. Non-Protein Calorie: Nitrogen Ratio (NPC/N) as an Indicator of Nitrogen Balance in Clinical Settings. Biomed J. Sci. Tech. Res. 2018, 6, 5013–5018. [Google Scholar] [CrossRef]
- McClave, S.A.; Martindale, R.G.; Vanek, V.W.; McCarthy, M.; Roberts, P.; Taylor, B.; Ochoa, J.B.; Napolitano, L.; Cresci, G. Board of Directors; American College of Critical Care Medicine; Society of Critical Care Medicine. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J. Parenter Enter. Nutr. 2009, 33, 277–316. [Google Scholar] [CrossRef]
- Blackburn, G.L.; Bistrian, B.R.; Maini, B.S.; Schlamm, H.T.; Smith, M.F. Nutritional and Metabolic Assessment of the Hospitalized Patient. JPEN J. Parenter Enter. Nutr. 1977, 1, 11–22. [Google Scholar] [CrossRef]
- Flatt, J.P.; Blackburn, G.L.; Bistrian, B.R. Urinary Urea Excretion and Evaluation of the Nitrogen Balance. JPEN J. Parenter Enter. Nutr. 1992, 16, 191–192. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, R.N. Using Nitrogen Balance in Clinical Practice. Hosp. Pharm. 2005, 40, 1081–1085. [Google Scholar] [CrossRef]
- Dickerson, R.N. Nitrogen Balance and Protein Requirements for Critically Ill Older Patients. Nutrients 2016, 8, 226. [Google Scholar] [CrossRef]
- Dickerson, R.N.; Tidwell, A.C.; Minard, G.; Croce, M.A.; Brown, R.O. Predicting Total Urinary Nitrogen Excretion from Urinary Urea Nitrogen Excretion in Multiple-Trauma Patients Receiving Specialized Nutrition Support. Nutrition 2005, 21, 332–338. [Google Scholar] [CrossRef]
- Derenski, K.; Catlin, J.; Allen, L. Parenteral Nutrition Basics for the Clinician Caring for the Adult Patient. Nutr. Clin. Pract. 2016, 31, 578–595. [Google Scholar] [CrossRef] [PubMed]
- Singer, P.; Blaser, A.R.; Berger, M.M.; Alhazzani, W.; Calder, P.C.; Casaer, M.P.; Hiesmayr, M.; Mayer, K.; Montejo, J.C.; Pichard, C.; et al. ESPEN Guideline on Clinical Nutrition in the Intensive Care Unit. Clin. Nutr. 2019, 38, 48–79. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Baracos, V.; Bertz, H.; Bozzetti, F.; Calder, P.C.; Deutz, N.E.P.; Erickson, N.; Laviano, A.; Lisanti, M.P.; Lobo, D.N.; et al. ESPEN Expert Group Recommendations for Action against Cancer-Related Malnutrition. Clin. Nutr. 2017, 36, 1187–1196. [Google Scholar] [CrossRef] [PubMed]
- Plauth, M.; Bernal, W.; Dasarathy, S.; Merli, M.; Plank, L.D.; Schütz, T.; Bischoff, S.C. ESPEN Guideline on Clinical Nutrition in Liver Disease. Clin. Nutr. 2019, 38, 485–521. [Google Scholar] [CrossRef]
- Pironi, L.; Arends, J.; Bozzetti, F.; Cuerda, C.; Gillanders, L.; Jeppesen, P.B.; Joly, F.; Kelly, D.; Lal, S.; Staun, M.; et al. Home Artificial Nutrition & Chronic Intestinal Failure Special Interest Group of ESPEN. ESPEN Guidelines on Chronic Intestinal Failure in Adults. Clin. Nutr. 2016, 35, 247–307. [Google Scholar] [CrossRef]
- Forbes, A.; Escher, J.; Hébuterne, X.; Kłęk, S.; Krznaric, Z.; Schneider, S.; Shamir, R.; Stardelova, K.; Wierdsma, N.; Wiskin, A.E.; et al. ESPEN Guideline: Clinical Nutrition in Inflammatory Bowel Disease. Clin. Nutr. 2017, 36, 321–347. [Google Scholar] [CrossRef]
- Joosten, K.; Embleton, N.; Yan, W.; Senterre, T.; ESPGHAN/ESPEN/ESPR/CSPEN Working Group on Pediatric Parenteral Nutrition. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition: Energy. Clin. Nutr. 2018, 37, 2309–2314. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Current Commercially Available IV Standard Amino Acid Solutions | |||||||
|---|---|---|---|---|---|---|---|
| Aminoven 10% | Sintamin 10% | Isopuramin 10% | Parentamin 10% | Amixal 10% | Freamine 10% | Travasol 10% | |
| EAA percentage of total AAs | 44.4 | 52.4 | 74.9 | 58.4 | 41.2 | 50.8 | 49.3 |
| Current Commercially Available IV Complete All-in-one Parenteral Mixtures | |||||
|---|---|---|---|---|---|
| Periven Kabiven | Krinuven Smofkabiven Aminomix | Nutriplus Nutrispecial Nutriperi Basalflex Periflex Plusflex Specialflex | Clinimix Oliclinomel | Olimel | |
| EAA percentage of total AAs | 51.2 | 43.3 | 48.6 | 45.7 | 51.1 |
| Nitrogen Losses | % of nitrogen Losses | |
|---|---|---|
| Urine | ~ 36 mg/Kg BW/day | 65% |
| Feces | ~ 12 mg/Kg BW/day | 21% |
| Other pathways * | ~ 8 mg/Kg BW/day | 14% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iacone, R.; Scanzano, C.; Santarpia, L.; Cioffi, I.; Contaldo, F.; Pasanisi, F. Macronutrients in Parenteral Nutrition: Amino Acids. Nutrients 2020, 12, 772. https://doi.org/10.3390/nu12030772
Iacone R, Scanzano C, Santarpia L, Cioffi I, Contaldo F, Pasanisi F. Macronutrients in Parenteral Nutrition: Amino Acids. Nutrients. 2020; 12(3):772. https://doi.org/10.3390/nu12030772
Chicago/Turabian StyleIacone, Roberto, Clelia Scanzano, Lidia Santarpia, Iolanda Cioffi, Franco Contaldo, and Fabrizio Pasanisi. 2020. "Macronutrients in Parenteral Nutrition: Amino Acids" Nutrients 12, no. 3: 772. https://doi.org/10.3390/nu12030772
APA StyleIacone, R., Scanzano, C., Santarpia, L., Cioffi, I., Contaldo, F., & Pasanisi, F. (2020). Macronutrients in Parenteral Nutrition: Amino Acids. Nutrients, 12(3), 772. https://doi.org/10.3390/nu12030772