Dietary Polyphenol Intake is Associated with HDL-Cholesterol and A Better Profile of other Components of the Metabolic Syndrome: A PREDIMED-Plus Sub-Study

 , ,
, ,  , ,
, ,  , ,
, ,  , ,
, ,  , ,
, ,  ,
, 
 ,
,  , , ,
, , ,  , , , , ,
, , , , , 
 ,
,  ,
,  ,
,  ,
,  , , , ,
, , , ,  ,
,  and
and  add
Show full author list
add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Design of the Study
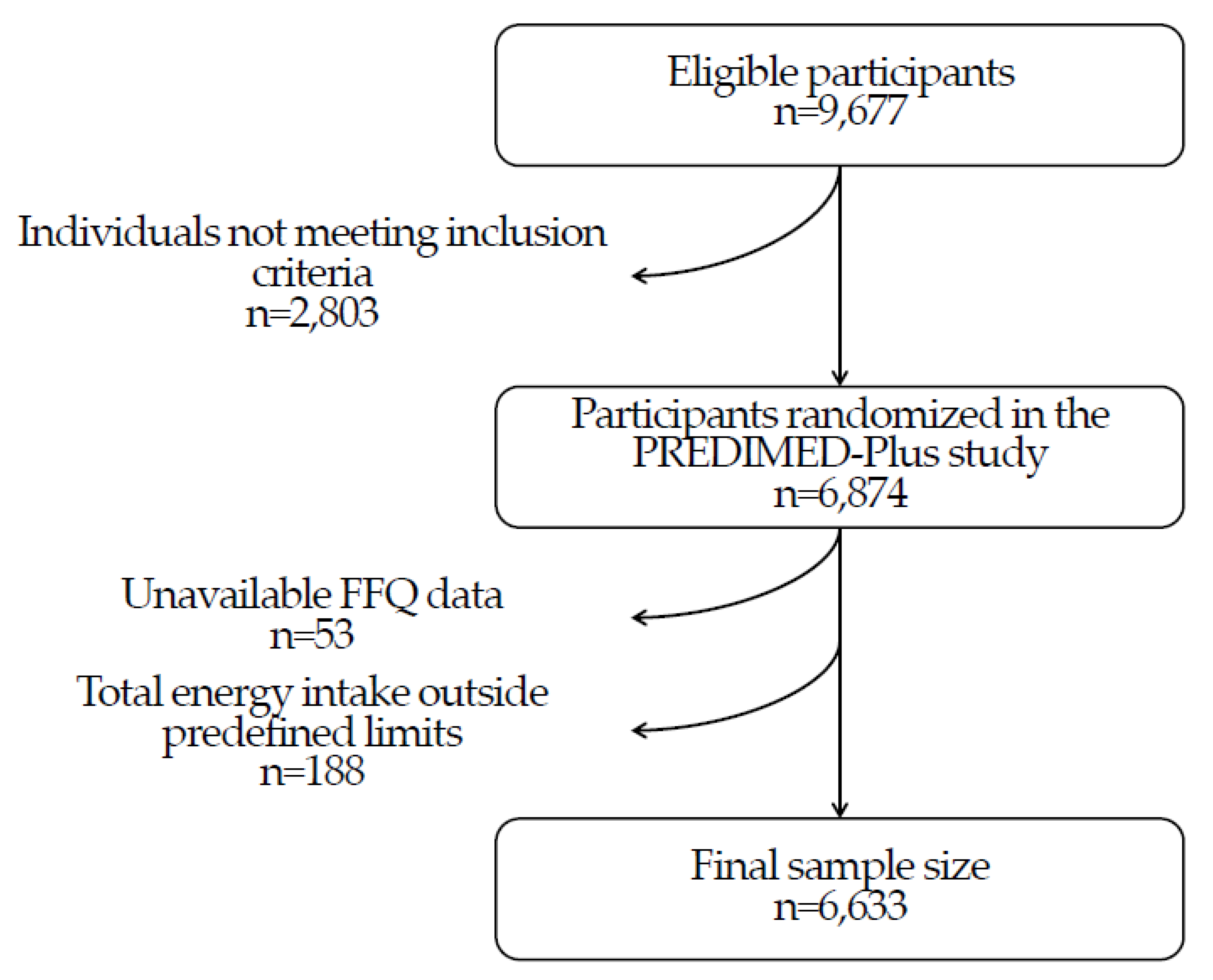
2.2. Participants
2.3. Estimation of Dietary Polyphenol Intake
2.4. Measurements and Outcome Assessment
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Del Rio, D.; Rodriguez-Mateos, A.; Spencer, J.P.; Tognolini, M.; Borges, G.; Crozier, A. Dietary (poly)phenolics in human health: Structures, bioavailability, and evidence of protective effects against chronic diseases. Antioxid. Redox Signal. 2013, 18, 1818–1892. [Google Scholar] [CrossRef] [PubMed]
- Barreca, D.; Gattuso, G.; Bellocco, E.; Calderaro, A.; Trombetta, D.; Smeriglio, A.; Laganà, G.; Daglia, M.; Meneghini, S.; Nabavi, S.M. Flavanones: Citrus phytochemical with health-promoting properties. BioFactors 2017, 43, 495–506. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Zappalà, G.; Bernardini, S.; Giambini, I.; Bes-Rastrollo, M.; Martínez-González, M.A. Adherence to the Mediterranean diet is inversely associated with metabolic syndrome occurrence: A meta-analysis of observational studies. Int. J. Food Sci. Nutr. 2017, 68, 138–148. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef]
- Koloverou, E.; Esposito, K.; Giugliano, D.; Panagiotakos, D. The effect of Mediterranean diet on the development of type 2 diabetes mellitus: A meta-analysis of 10 prospective studies and 136,846 participants. Metabolism 2014, 63, 903–911. [Google Scholar] [CrossRef]
- Grosso, G.; Stepaniak, U.; Micek, A.; Topor-Madry, R.; Stefler, D.; Szafraniec, K.; Bobak, M.; Pajak, A. A Mediterranean-type diet is associated with better metabolic profile in urban Polish adults: Results from the HAPIEE study. Metabolism 2015, 64, 738–746. [Google Scholar] [CrossRef]
- Giglio, R.V.; Patti, A.M.; Cicero, A.F.G.; Lippi, G.; Rizzo, M.; Toth, P.P.; Banach, M. Polyphenols: Potential use in the prevention and treatment of cardiovascular diseases. Curr. Pharm. Des. 2018, 24, 239–258. [Google Scholar] [CrossRef]
- Chiva-Blanch, G.; Badimon, L. Effects of polyphenol intake on metabolic syndrome: Current evidence from human trials. Oxid. Med. Cell. Longev. 2017, 2017, 5812401. [Google Scholar] [CrossRef]
- Patti, A.M.; Al-Rasadi, K.; Giglio, R.V.; Nikolic, D.; Mannina, C.; Castellino, G.; Chianetta, R.; Banach, M.; Cicero, A.F.G.; Lippi, G.; et al. Natural approaches in metabolic syndrome management. Arch. Med. Sci. 2018, 14, 422–441. [Google Scholar] [CrossRef]
- Amiot, M.J.; Riva, C.; Vinet, A. Effects of dietary polyphenols on metabolic syndrome features in humans: A systematic review. Obes. Rev. 2016, 17, 573–586. [Google Scholar] [CrossRef]
- Manach, C.; Scalbert, A.; Morand, C.; Rémésy, C.; Jiménez, L. Polyphenols: Food sources and bioavailability. Am. J. Clin. Nutr. 2004, 79, 727–747. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; Buil-Cosiales, P.; Corella, D.; Bulló, M.; Fitó, M.; Vioque, J.; Romaguera, D.; Martínez, J.A.; Wärnberg, J.; López-Miranda, J.; et al. Cohort profile: Design and methods of the PREDIMED-Plus randomized trial. Int. J. Epidemiol. 2019, 48, 387–388. [Google Scholar] [CrossRef]
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1228S. [Google Scholar] [CrossRef] [PubMed]
- Tresserra-Rimbau, A.; Medina-Remón, A.; Pérez-Jiménez, J.; Martínez-González, M.A.; Covas, M.I.; Corella, D.; Salas-Salvadó, J.; Gómez-Garcia, E.; Lapetra, J.; Arós, F.; et al. Dietary intake and major food sources of polyphenols in a Spanish population at high cardiovascular risk: The PREDIMED study. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Rothwell, J.A.; Pérez-Jiménez, J.; Neveu, V.; Medina-Ramon, A.; M’Hiri, N.; Garcia Lobato, P.; Manach, C.; Knox, K.; Eisner, R.; Wishart, D.; et al. Phenol-Explorer 3.0: A major update of the Phenol-Explorer database to incorporate data on the effects of food processing on polyphenol content. Database 2013. [Google Scholar] [CrossRef]
- Molina, L.; Sarmiento, M.; Peñafiel, J.; Donaire, D.; Garcia-Aymerich, J.; Gomez, M.; Bie, M.; Ruiz, S.; Frances, A.; Schröder, H.; et al. Validation of the regicor short physical activity questionnaire for the adult population. PLoS ONE 2017, 12, e0168148. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; López-Fontana, C.; Varo, J.J.; Sánchez-Villegas, A.; Martinez, J.A. Validation of the Spanish version of the physical activity questionnaire used in the nurses’ health study and the health professionals’ follow-up study. Public Health Nutr. 2005, 8, 920–927. [Google Scholar] [CrossRef]
- Mendonça, R.D.; Carvalho, N.C.; Martin-Moreno, J.M.; Pimenta, A.M.; Lopes, A.C.S.; Gea, A.; Martíne-González, M.A.; Bes-Rastrollo, M. Total polyphenol intake, polyphenol subtypes and incidence of cardiovascular disease: The SUN cohort study. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 69–78. [Google Scholar] [CrossRef]
- Zamora-Ros, E.; Knaze, V.; Rothwell, J.; Hémon, B.; Moskal, A.; Overvad, K.; Tjonneland, A.; Kyro, C.; Fagherazzi, G.; Boutron-Ruault, M.C. Dietary polyphenol intake in Europe: The European Prospective Investigation into Cancer and Nutrition (EPIC) study. Eur. J. Nutr. 2016, 55, 1359–1375. [Google Scholar] [CrossRef]
- Pérez-Jiménez, J.; Fezeu, L.; Touvier, M.; Arnault, N.; Manach, C.; Hercberg, S.; Galan, P.; Scalbert, A. Dietary intake of 337 polyphenols in French adults. Am. J. Clin. Nutr. 2011, 93, 1220–1228. [Google Scholar] [CrossRef]
- Ziauddeen, N.; Rosi, A.; Del Rio, D.; Amoutzopoulos, B.; Nicholson, S.; Page, P.; Scazzina, F.; Brighenti, F.; Ray, S.; Mena, P. Dietary intake of (poly)phenols in children and adults: Cross-sectional analysis of the UK national diet and nutrition survey rolling programme (2008–2014). Eur. J. Nutr. 2019, 58, 3183–3198. [Google Scholar] [CrossRef] [PubMed]
- Pinto, P.; Santos, C.N. Worldwide (poly)phenol intake: Assessment methods and identified gaps. Eur. J. Nutr. 2017, 59, 1393–1408. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Stepaniak, U.; Topor-Madry, R.; Szafraniec, K.; Pajak, A. Estimated dietary intake and major food sources of polyphenols in the Polish arm of the HAPIEE study. Nutrition 2014, 30, 1398–1403. [Google Scholar] [CrossRef] [PubMed]
- Ovaskainen, M.L.; Torronen, R.; Koponen, J.M.; Sinkko, H.; Hellstrom, J.; Reinivuo, H.; Mattila, P. Dietary intake and major food sources of polyphenols in Finnish adults. J. Nutr. 2008, 138, 562–566. [Google Scholar] [CrossRef]
- Vitale, M.; Masulli, M.; Rivellese, A.A.; Bonora, E.; Cappellini, F.; Nicolucci, A.; Squatrito, S.; Antenucci, D.; Barrea, A.; Bianchi, C.; et al. Dietary intake and major food sources of polyphenols in people with type 2 diabetes: The TOSCA.IT study. Eur. J. Nutr. 2018, 57, 679–688. [Google Scholar] [CrossRef]
- Vetrani, C.; Vitale, M.; Bozzetto, L.; Della Pepa, G.; Cocozza, S.; Costabile, G.; Mangione, A.; Cipriano, P.; Annuzzi, G.; Rivellese, A.A. Association between different dietary polyphenol subclases and the improvement in cardiometabolic risk factors: Evidence from a randomized controlled clinical trial. Acta Diabetol. 2018, 55, 149–153. [Google Scholar] [CrossRef]
- Marseglia, L.; Manti, S.; D’Angelo, G.; Nicotera, A.; Parisi, E.; Di Rosa, G.; Gitto, E.; Arrigo, T. Oxidative stress in obesity: A critical component in human diseases. Int. J. Mol. Sci. 2015, 16, 378–400. [Google Scholar] [CrossRef] [PubMed]
- Wisnuwardani, R.W.; De Henauw, S.; Androutsos, O.; Forsner, M.; Gottrand, F.; Huybrechts, I.; Knaze, V.; Le Donne, C.; Marcos, A.; Molnár, D.; et al. Estimated dietary intake of polyphenols in European adolescents: The HELENA study. Eur. J. Nutr. 2019, 58, 2345–2363. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.K.; Dayem, A.A.; Han, J.; Yin, K.; Kim, K.; Saha, S.K.; Yang, G.M.; Choi, H.Y.; Cho, S.G. Molecular mechanisms of the anti-obesity and anti-diabetic properties of flavonoids. Int. J. Mol. Sci. 2016, 17, 569. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Stepanlak, U.; Micek, A.; Stefler, D.; Bobak, M.; Pajak, A. Dietary polyphenols are inversely associated with metabolic syndrome in Polish adults of the HAPIEE study. Eur. J. Nutr. 2017, 56, 1709–1720. [Google Scholar] [CrossRef]
- Ellison, R.C.; Zhang, Y.; Qureshi, M.M.; Knox, S.; Arnett, D.K.; Province, M.A.; Investigators of the NHLBI Family Heart Study. Lifestyle determinants of high-density lipoprotein cholesterol: The national heart, lung, and blood institute family heart study. Am. Heart J. 2004, 147, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Tresserra-Rimbau, A.; Medina-Remón, A.; Lamuela-Raventós, R.M.; Bulló, M.; Salas-Salvadó, J.; Corella, D.; Fitó, M.; Gea, A.; Gómez-Garcia, E.; Lapetra, J.; et al. Moderate red wine consumption is associated with a lower prevalence of the metabolic syndrome in the PREDIMED population. Br. J. Nutr. 2015, 113, S121–S130. [Google Scholar] [CrossRef] [PubMed]
- Wilsgaard, T.; Jacobsen, B.K. Lifestyle factors and incident metabolic syndrome. The Tromso study 1979–2001. Diabetes Res. Clin. Pract. 2007, 78, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Moustaid-Moussa, N.; Chen, L.; Mo, H.; Shastri, A.; Su, R.; Bapat, P.; Kwun, I.; Shen, C.L. Novel insights of dietary polyphenols and obesity. J. Nutr. Biochem. 2014, 25, 1–18. [Google Scholar] [CrossRef]
- Lee, S.H.; Mantzoros, C.; Kim, Y.B. Resveratrol: Is selectivity opening the key to therapeutic effects? Metabolism 2012, 61, 289–290. [Google Scholar] [CrossRef]
- Miranda, A.M.; Steluti, J.; Fisberg, R.M.; Marchioni, D.M. Association between polyphenol intake and hypertension in adults and older adults: A population-based study in Brazil. PLoS ONE 2016, 11, e0165791. [Google Scholar] [CrossRef]
- Grosso, G.; Stepaniak, U.; Micek, A.; Kozela, M.; Stefler, D.; Bobak, M.; Pajak, A. Dietary polyphenol intake and risk of hypertension in the Polish arm of the HAPIEE study. Eur. J. Nutr. 2018, 57, 1535–1544. [Google Scholar] [CrossRef]
- Zamora-Ros, R.; Forouhi, N.G.; Sharp, S.J.; González, C.A.; Buijsse, B.; Guevara, M.; van der Schouw, Y.T.; Amiano, P.; Boeing, H.; Bredsdorff, L.; et al. The association between dietary flavonoid and lignan intakes and incident type 2 diabetes in European populations: The EPIC-InterAct study. Diabetes Care 2013, 36, 3961–3970. [Google Scholar] [CrossRef]
- Tresserra-Rimbau, A.; Guasch-Ferré, M.; Salas-Salvadó, J.; Toledo, E.; Corella, D.; Castañer, O.; Guo, X.; Gómez-Garcia, E.; Lapetra, J.; Arós, F.; et al. Intake of total polyphenols and some clases of polyphenols is inversely associated with diabetes in elderly people at high cardiovascular disease risk. J. Nutr. 2016. [Google Scholar] [CrossRef]
- Tresserra-Rimbau, A.; Castro-Barquero, S.; Vitelli-Storelli, F.; Becerra-Tomas, N.; Vázquez-Ruiz, Z.; Díaz-López, A.; Corella, D.; Castañer, O.; Romaguera, D.; Vioque, J.; et al. Associations between dietary polyphenols and type 2 diabetes in a cross-sectional analysis of the PREDIMED-plus trial: Role of the body mass index and sex. Antioxidants 2019, 8, 537. [Google Scholar] [CrossRef]
- Sun, Q.; Wedick, N.M.; Pan, A.; Townsend, M.K.; Cassidy, A.; Franke, A.A.; Rimm, E.B.; Hu, F.B.; van Dam, R.M. Gut microbiota metabolites of dietary lignans and risk of type 2 diabetes: A prospective investigation in two cohorts of U.S. women. Diabetes Care 2014, 37, 1287–1295. [Google Scholar] [CrossRef]
- Guo, X.; Tresserra-Rimbau, A.; Estruch, R.; Martínez-González, M.A.; Medina-Remón, A.; Castañer, O.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.M. Effects of polyphenol, measured by a biomarker of total polyphenols in urine, on cardiovascular risk factors after a long-term follow-up in the PREDIMED study. Oxid. Med. Cell. Longev. 2016, 2016, 2572606. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.G.; Colletti, A. Polyphenols effect on circulating lipids and lipoproteins: From biochemistry to clinical evidence. Curr. Pharm. Des. 2018, 24, 178–190. [Google Scholar] [CrossRef] [PubMed]
- Medina-Remón, A.; Barrionuevo-González, A.; Zamora-Ros, R.; Andres-Lacueva, C.; Estruch, R.; Martínez-González, M.A.; Diez-Espino, J.; Lamuela-Raventós, R.M. Rapid Folin-Ciocalteu method using microtiter 96-well plate cartridges for solid phase extraction to assess urinary total phenolic compounds, as a biomarker of total polyphenols intake. Anal. Chim. Acta 2009, 634, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.A.; Salas-Salvadó, J.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Q1 (<623, 3 mg/d) | Q2 (623.4–799.4 mg/d) | Q3 (799.5–1019.2 mg/d) | Q4 (>1019.3 mg/d) | p | p for Linear Trend | |
|---|---|---|---|---|---|---|
| n | 1658 | 1658 | 1660 | 1657 | ||
| Age, years | 65.2 ± 4.90 | 64.8 ± 4.87 | 65.0 ± 4.87 | 64.9 ± 4.98 | 0.10 | 0.19 |
| Women, n (%) | 894 (53.9) | 845 (51.0) | 785 (47.3) | 685 (41.3) | <0.001 | <0.001 |
| Family history of CVD 1, n (%) | 659 (39.7) | 698 (42.1) | 662 (39.9) | 678 (40.9) | 0.48 | 0.81 |
| Current smokers, n (%) | 197 (11.9) | 205 (12.4) | 203 (12.2) | 216 (13.0) | 0.78 | 0.36 |
| Former smokers, n (%) | 647 (39.0) | 695 (41.9) | 728 (43.9) | 800 (48.3) | <0.001 | <0.001 |
| BMI, kg/m2 | 32.6 ± 3.46 | 32.6 ± 3.49 | 32.6 ± 3.51 | 32.3 ± 3.31 | 0.03 | 0.02 |
| Waist circumference, cm | 107.0 ± 9.76 | 107.4 ± 9.70 | 107.8 ± 9.75 | 107.8 ± 9.36 | 0.06 | 0.01 |
| Body weight, kg | 85.2 ± 12.8 | 86.2 ± 12.8 | 87.3 ± 13.3 | 87.5 ± 12.8 | <0.001 | <0.001 |
| Glucose, mg/dL | 113.4 ± 28.9 | 113.9 ± 31.0 | 113.9 ± 29.0 | 113.0 ± 27.6 | 0.78 | 0.71 |
| Glycated hemoglobin, % | 6.10 ± 0.88 | 6.22 ± 2.58 | 6.25 ± 3.53 | 6.10 ± 0.88 | 0.15 | 0.85 |
| Total-cholesterol, mg/dL | 196 ± 38.4 | 197 ± 37.7 | 196 ± 37.0 | 198 ± 42.8 | 0.59 | 0.57 |
| HDL-cholesterol, mg/dL | 47.6 ± 11.5 | 48.2 ± 11.7 | 48.7 ± 12.2 | 47.9 ± 11.9 | 0.06 | 0.32 |
| Medications, n (%) | ||||||
| Antihypertensive agents | 1272 (76.7) | 1285 (77.5) | 1294 (77.9) | 1304 (78.7) | 0.48 | 0.46 |
| Colesterol-lowering agents | 862 (52.0) | 846 (51.0) | 858 (51.7) | 842 (50.8) | 0.97 | 0.52 |
| Insulin | 84 (5.07) | 98 (5.91) | 67 (4.04) | 63 (3.80) | 0.01 | 0.01 |
| Metformin | 380 (22.9) | 404 (24.4) | 383 (23.1) | 347 (20.9) | 0.13 | 0.12 |
| Other hypoglycemic drugs | 324 (19.5) | 331 (20.0) | 327 (19.7) | 303 (18.3) | 0.62 | 0.35 |
| Aspirin or antiplatelet drugs | 246 (14.8) | 272 (16.4) | 249 (15.0) | 271 (16.3) | 0.26 | 0.61 |
| NSAIDS | 534 (32.2) | 469 (28.3) | 484 (29.2) | 446 (26.9) | 0.01 | 0.01 |
| Vitamins and minerals | 210 (12.7) | 184 (11.1) | 220 (13.3) | 183 (11.0) | 0.19 | 0.11 |
| Sedative or tranquilliser agents | 417 (25.1) | 416 (25.1) | 389 (23.4) | 392 (23.7) | 0.85 | 0.31 |
| Hormonal treatment (only women) | 42 (2.53) | 41 (2.47) | 33 (1.99) | 38 (2.29) | 0.924 | 0.935 |
| Educational level, n (%) | <0.001 | <0.001 | ||||
| Primary school | 887 (53.6) | 854 (51.5) | 805 (48.5) | 719 (43.4) | ||
| Secondary school | 468 (28.3) | 467 (28.2) | 497 (30.0) | 481 (29.0) | ||
| University and other studies | 301 (18.2) | 337 (20.3) | 356 (21.5) | 456 (27.5) | ||
| Polyphenol Subclasses | Contribution, Mean (mg/d) ± SD, (%) | Polyphenol Contribution as Aglycones, Mean (mg/d) ± SD, (%) | Food Sources (% of Contribution) |
|---|---|---|---|
| Total polyphenols | 846 ± 318 | 620.9 ± 273.5 | |
| Flavonoids | 491 ± 253, (58.0) | 406.3 ± 237.2 (65.44) | |
| 43.5 ± 37.8, (5.14) | 24.7 ± 21.7 (3.98) | Cherries (42.2), red wine (24.1), olives (10.5), strawberries (10.1), grape (9.30), other foods (3.8) |
| 0.009 ± 0.18, (<0.01) | 0.006 ± 0.01 (<0.01) | Beer (100) |
| 1.72 ± 1.59, (0.20) | 0.98 ± 0.91 (0.16) | Apples (93.2), fruit juices from concentrate (6.77) |
| 2.62 ± 4.92, (0.31) | 1.81 ± 3.43 (0.29) | Red wine (97.6), white wine (1.80), rosé wine (0.59) |
| 28.1 ± 22.4, (3.32) | 27.1 ± 20.7 (4.36) | Tea (23.0), red wine (19.2), apples (18.6), chocolate (11.6), peaches (6.0), cocoa powder (3.18), fruit juices from concentrate (2.83), other foods (15.6) |
| 204± 185, (24.1) | 200.7 ± 189.4 (32.32) | Chocolate (42.7), apples (20.4), plums (9.53), red wine (7.09), cocoa powder (5.68), strawberries (4.20), other foods (10.4) |
| 0.70 ± 1.81, (0.08) | 0.57 ± 1.46 (0.09) | Tea (100) |
| 83.2 ± 76.6, (9.83) | 58.1 ± 55.0 (9.35) | Oranges (71.3), natural orange juice (23.0), fruit juices from concentrate (3.22), other foods (2.09) |
| 73.2 ± 47.4, (8.65) | 54.7 ± 32.9 (8.81) | Whole-grain bread (30.0), bread (23.6), oranges (21.6), natural orange juice (8.53), artichoke (3.80), other foods (12.5). |
| 54.0 ± 22.3, (6.40) | 35.6 ± 15.3 (5.73) | Onions (27.8), spinach (26.7), lettuce (11.9), red wine (6.02), olives (5.10), asparagus (4.93), other foods (17.55) |
| 0.002 ± 0.004, (<0.01) | 0.002 ± 0.003 (<0.01) | Beer (100) |
| Phenolic acids | 280 ± 131, (33.1) | 164.2 ± 70.8 (26.44) | |
| 15.5 ± 10.3, (1.83) | 20.5 ± 12.4 (3.30) | Red wine (21.2), olives (19.9), walnuts (18.1), tea (9.46), swiss chard leaves (6.15), white wine (1.34), other foods (23.8) |
| 264 ± 129, (30.9) | 141.6 ± 66.8 (22.80) | Decaffeinated coffee (37.7), coffee (26.1), plums (5.66), potatoes (5.50), olives (4.21), red wine (1.79), other foods (19.0) |
| 0.90 ± 1.04, (0.10) | 1.16 ± 1.40 (0.19) | Olives (87.2), red wine (6.57), beer (3.86), extra virgin olive oil (1.52), white wine (0.65) |
| 0.48 ± 0.65, (0.06) | 0.91 ± 1.23 (0.14) | Olives (100) |
| Stilbenes | 2.13 ± 3.92, (0.25) | 1.78 ± 3.19 (0.29) | Red wine (91.9), white wine (3.94), grapes (1.60), rosé wine (1.21), other foods (0.07) |
| Lignans | 1.53 ± 0.56, (0.18) | 1.33 ± 0.55 (0.21) | Extra virgin olive oil (16.7), seeds (9.84), oranges (9.73), green bean (5.42), pepper (5.32), peaches (4.97), broccoli (4.71), bread (4.48), red wine (4.16), cabbage (2.77), other foods (31.9) |
| Other polyphenols | 70.8 ± 41.5, (8.37) | 45.6 ± 27.8 (7.34) | |
| 0.93 ± 0.87, (0.11) | 0.93 ± 0.87 (0.15) | Decaffeinated coffee (74.1), coffee (16.2), beers (9.77) |
| 13.7 ± 17.8, (1.62) | 13.8 ± 18.5 (2.23) | Whole-grain bread (69.1), whole-grain pastries (14.8), breakfast cereals (8.40), pasta (3.29), other foods (4.41) |
| 0.37 ± 0.38, (0.04) | 0.37 ± 0.39 (0.06) | Celery stalks (98.3), grapefruit juice (1.7) |
| 0.42 ± 0.65, (0.05) | 0.42 ± 0.66 (<0.01) | Red wine (78.9), walnuts (14.5), beer (2.61), white wine (1.95), other foods (2.04) |
| 0.002 ± 0.004, (<0.01) | 0.002 ± 0.003 (<0.01) | Beer (100) |
| 0.10 ± 0.19, (0.01) | 0.09 ±0.18 (<0.01) | Beer (73.6), white wine (26.3), cocoa powder (0.10) |
| 0.13 ± 0.12, (0.01) | 0.11 ± 0.12 (0.01) | Decaffeinated coffee (81.3), coffee (18.7) |
| 0.82 ± 1.12, (0.09) | 0.84 ± 1.14 (0.14) | Walnuts (100) |
| 52.4 ± 37.8, (6.19) | 30.0 ± 21.2 (4.83) | Olives (50.0), extra virgin olive oil (34.8), refined olive oil (5.17), red wine (3.29), other foods (6.74) |
| 1.96 ± 2.30, (0.23) | 0.66 ± 0.54 (0.11) | Orange juice (45.4), pears (18.2), coffee (16.0), other fruit juices (9.98), olives (5.86), other foods (4.56) |
| n | Total Polypenols (mg/d) | p | Flavonoids (mg/d) | p | Phenolic Acids (mg/d) | p | Stilbenes (mg/d) | p | Lignans (mg/d) | p | Other Polyphenols (mg/d) | p | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total population | 6633 | 846 ± 275 1 | 491 ± 229 | 290 ± 127 | 2.13 ± 3.81 | 1.53 ± 0.54 | 70.8 ± 38.5 | ||||||
| Men | 3424 | 830 ± 288 | <0.001 | 469 ± 234 | <0.001 | 285 ± 134 | 0.003 | 3.00 ± 4.74 | <0.001 | 1.53 ± 0.54 | 0.933 | 72.1 ± 42.5 | 0.006 |
| Women | 3209 | 863 ± 259 | 515 ± 220 | 276 ± 118 | 1.21 ± 2.12 | 1.53 ± 0.53 | 69.5 ± 33.7 | ||||||
| Age (years) | |||||||||||||
| <65 | 3530 | 835 ± 275 | 0.002 | 476 ± 230 | <0.001 | 285 ± 128 | 0.014 | 2.15 ± 4.03 | 0.605 | 1.51 ± 0.54 | 0.006 | 70.7 ± 39.2 | 0.967 |
| 65-70 | 2122 | 854 ± 271 | 503 ± 225 | 276 ± 123 | 2.07 ± 3.62 | 1.55 ± 0.52 | 71.0 ± 38.3 | ||||||
| >70 | 981 | 866 ± 281 | 517 ± 228 | 275 ± 127 | 2.21 ± 3.40 | 1.55 ± 0.54 | 70.8 ± 36.4 | ||||||
| BMI (Kg/m2) | |||||||||||||
| <29.9 | 1762 | 847 ± 268 | 0.042 | 501 ± 225 | 0.004 | 272 ± 124 | 0.006 | 2.26 ± 3.85 | <0.001 | 1.52 ± 0.49 | 0.679 | 69.9 ± 36.8 | 0.353 |
| 30-34.9 | 3258 | 852 ± 280 | 493 ± 232 | 284 ± 129 | 2.24 ± 3.90 | 1.53 ± 0.54 | 71.5 ± 39.7 | ||||||
| >35 | 1613 | 831 ± 270 | 475 ± 226 | 282 ± 124 | 1.77 ± 3.57 | 1.54 ± 0.57 | 70.5 ± 37.9 | ||||||
| Physical activity level | |||||||||||||
| Low | 3953 | 833 ± 278 | <0.001 | 480 ± 231 | <0.001 | 280 ± 129 | 0.884 | 1.85 ± 3.48 | <0.001 | 1.51 ± 0.54 | <0.001 | 70.0 ± 38.5 | 0.034 |
| Moderate | 1253 | 861 ± 267 | 503 ± 217 | 282 ± 123 | 2.30 ± 3.79 | 1.55 ± 0.54 | 71.7 ± 36.6 | ||||||
| Active | 1408 | 867 ± 271 | 510 ± 230 | 280 ± 123 | 2.76 ± 4.55 | 1.58 ± 0.53 | 72.8 ± 40.0 | ||||||
| Educational level | |||||||||||||
| Primary school | 3266 | 834 ± 259 | <0.001 | 482 ± 213 | <0.001 | 278 ± 121 | 0.070 | 1.80 ± 3.38 | <0.001 | 1.54 ± 0.55 | 0.093 | 70.9 ± 40.2 | 0.290 |
| Secondary school | 1913 | 840 ± 270 | 487 ± 227 | 279 ± 125 | 2.27 ± 3.98 | 1.51 ± 0.53 | 69.9 ± 38.1 | ||||||
| University | 1450 | 880 ± 311 | 517 ± 260 | 287 ± 139 | 2.70 ± 4.40 | 1.55 ± 0.52 | 72.0 ± 35.0 | ||||||
| Smoking status | |||||||||||||
| Current smokers | 821 | 841 ± 296 | 0.581 | 455 ± 243 | <0.001 | 311 ± 143 | <0.001 | 2.33 ± 4.43 | 0.114 | 1.47±0.53 | <0.001 | 70.5 ± 46.3 | 0.768 |
| Non-smokers | 5812 | 847 ± 272 | 496 ± 226 | 276 ± 123 | 2.10 ± 3.72 | 1.54±0.54 | 70.9 ± 37.3 | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castro-Barquero, S.; Tresserra-Rimbau, A.; Vitelli-Storelli, F.; Doménech, M.; Salas-Salvadó, J.; Martín-Sánchez, V.; Rubín-García, M.; Buil-Cosiales, P.; Corella, D.; Fitó, M.; et al. Dietary Polyphenol Intake is Associated with HDL-Cholesterol and A Better Profile of other Components of the Metabolic Syndrome: A PREDIMED-Plus Sub-Study. Nutrients 2020, 12, 689. https://doi.org/10.3390/nu12030689
Castro-Barquero S, Tresserra-Rimbau A, Vitelli-Storelli F, Doménech M, Salas-Salvadó J, Martín-Sánchez V, Rubín-García M, Buil-Cosiales P, Corella D, Fitó M, et al. Dietary Polyphenol Intake is Associated with HDL-Cholesterol and A Better Profile of other Components of the Metabolic Syndrome: A PREDIMED-Plus Sub-Study. Nutrients. 2020; 12(3):689. https://doi.org/10.3390/nu12030689
Chicago/Turabian StyleCastro-Barquero, Sara, Anna Tresserra-Rimbau, Facundo Vitelli-Storelli, Mónica Doménech, Jordi Salas-Salvadó, Vicente Martín-Sánchez, María Rubín-García, Pilar Buil-Cosiales, Dolores Corella, Montserrat Fitó, and et al. 2020. "Dietary Polyphenol Intake is Associated with HDL-Cholesterol and A Better Profile of other Components of the Metabolic Syndrome: A PREDIMED-Plus Sub-Study" Nutrients 12, no. 3: 689. https://doi.org/10.3390/nu12030689
APA StyleCastro-Barquero, S., Tresserra-Rimbau, A., Vitelli-Storelli, F., Doménech, M., Salas-Salvadó, J., Martín-Sánchez, V., Rubín-García, M., Buil-Cosiales, P., Corella, D., Fitó, M., Romaguera, D., Vioque, J., Alonso-Gómez, Á. M., Wärnberg, J., Martínez, J. A., Serra-Majem, L., Tinahones, F. J., Lapetra, J., Pintó, X., ... Estruch, R. (2020). Dietary Polyphenol Intake is Associated with HDL-Cholesterol and A Better Profile of other Components of the Metabolic Syndrome: A PREDIMED-Plus Sub-Study. Nutrients, 12(3), 689. https://doi.org/10.3390/nu12030689