Effects of a 12-Month Intensive Lifestyle Monitoring Program in Predominantly Overweight/Obese Arab Adults with Prediabetes

 , , ,
, , , 

Abstract
1. Introduction
2. Materials and Methods
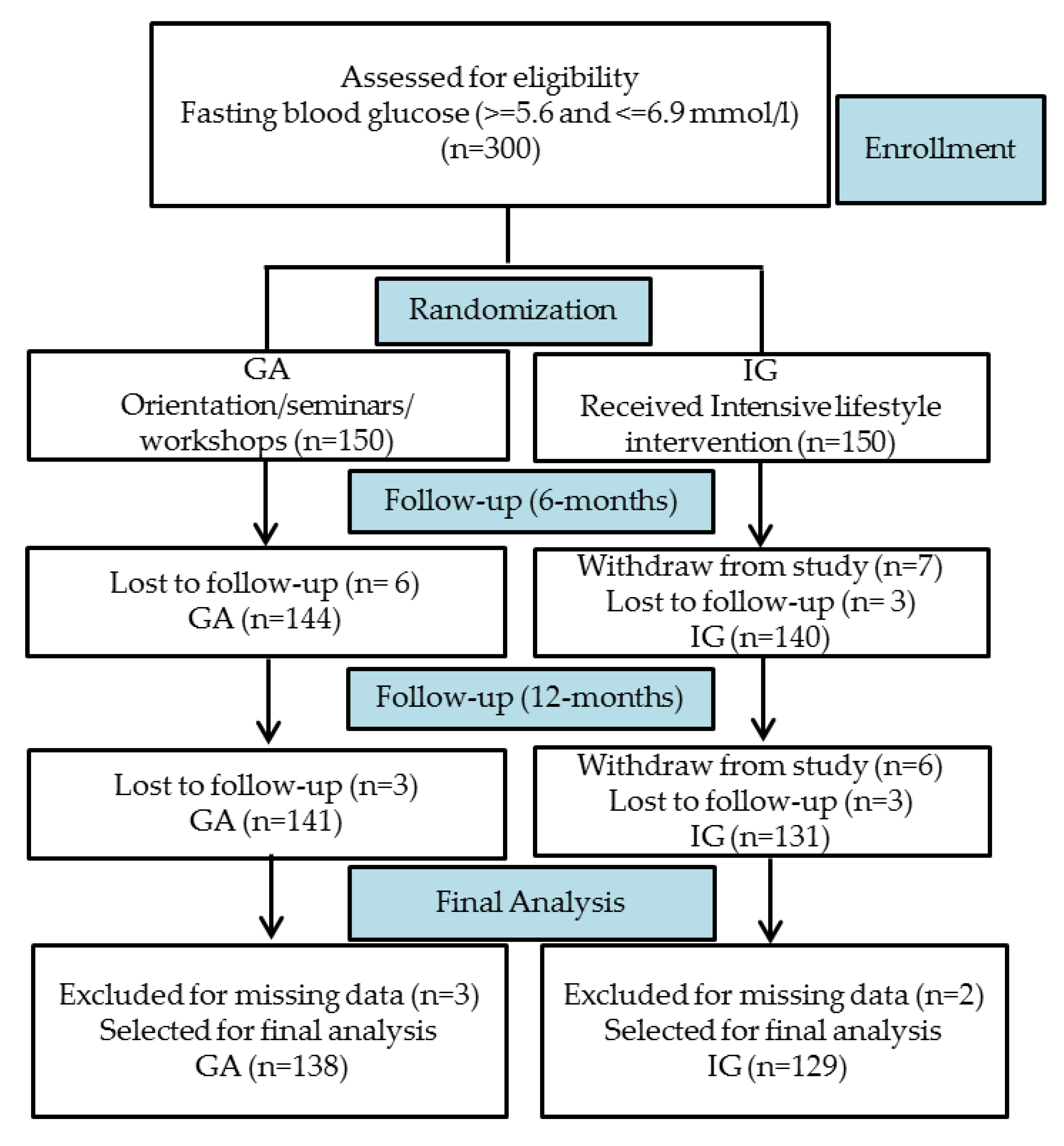
2.1. Study Design and Participants
2.2. Intervention
2.3. Clinical and Biochemical Characteristics
2.4. Statistical Analysis
3. Results
3.1. General Characteristics of the Study Participants at Recruitment
3.2. Clinical Characteristics of the Study Groups’ Over Time
3.3. Percentage Change in Body Weight and Fasting Glucose from Baseline to End of Study
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wild, S.; Roglic, G.; Green, A.; Sicree, R.; King, H. Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care 2004, 27, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Al-Daghri, N.M.; Al-Attas, O.S.; Alokail, M.S.; Alkharfy, K.M.; Yousef, M.; Sabico, S.L.; Chrousos, G.P. Diabetes mellitus type 2 and other chronic non-communicable diseases in the central region, saudi arabia (riyadh cohort 2): A decade of an epidemic. BMC Med. 2011, 9, 76. [Google Scholar] [CrossRef] [PubMed]
- Abuyassin, B.; Laher, I. Diabetes epidemic sweeping the arab world. World J. Diabetes 2016, 7, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Atlas, D.; International Diabetes Federation. IDF Diabetes Atlas, 7th ed.; International Diabetes Federation: Brussels, Belgium, 2015; Available online: https://www.idf.org/e-library/epidemiology-research/diabetes-atlas/13-diabetes-atlas-seventh-edition.html (accessed on 25 November 2019).
- Badran, M.; Laher, I. Type II diabetes mellitus in arabic-speaking countries. Int. J. Endocrinol. 2012, 2012, 902873. [Google Scholar] [CrossRef] [PubMed]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M.; Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [PubMed]
- Tuomilehto, J.; Lindström, J.; Eriksson, J.G.; Valle, T.T.; Hämäläinen, H.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Laakso, M.; Louheranta, A.; Rastas, M. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N. Engl. J. Med. 2001, 344, 1343–1350. [Google Scholar] [CrossRef]
- Pan, X.-R.; Li, G.-W.; Hu, Y.-H.; Wang, J.-X.; Yang, W.-Y.; An, Z.-X.; Hu, Z.-X.; Xiao, J.-Z.; Cao, H.-B.; Liu, P.-A. Effects of diet and exercise in preventing niddm in people with impaired glucose tolerance: The da qing igt and diabetes study. Diabetes Care 1997, 20, 537–544. [Google Scholar] [CrossRef]
- Tabák, A.G.; Herder, C.; Rathmann, W.; Brunner, E.J.; Kivimäki, M. Prediabetes: A high-risk state for diabetes development. Lancet 2012, 379, 2279–2290. [Google Scholar] [CrossRef]
- Low Wang, C.C.; Hess, C.N.; Hiatt, W.R.; Goldfine, A.B. Clinical update: Cardiovascular disease in diabetes mellitus: Atherosclerotic cardiovascular disease and heart failure in type 2 diabetes mellitus–mechanisms, management, and clinical considerations. Circulation 2016, 133, 2459–2502. [Google Scholar] [CrossRef]
- American Diabetes Association. Lifestyle management. Diabetes Care 2017, 40, S33–S43. [Google Scholar] [CrossRef]
- American Diabetes Association. Standards of medical care in diabetes-2019 abridged for primary care providers. Clin. Diabetes 2019, 37, 11–34. [Google Scholar] [CrossRef] [PubMed]
- Starfield, B.; Shi, L.; Macinko, J. Contribution of primary care to health systems and health. Milbank Q. 2005, 83, 457–502. [Google Scholar] [CrossRef] [PubMed]
- Al Alhareth, Y.; Al Alhareth, Y.; Al Dighrir, I. Review of women and society in saudi arabia. Am. J. Educ. Res. 2015, 3, 121–125. [Google Scholar] [CrossRef]
- Ministry of Health, Saudi Arabia. Saudi Health Interview Survey Results. 2013. Available online: http://www.healthdata.org/sites/default/files/files/Projects/KSA/Saudi-Health-Interview-Survey-Results.pdf (accessed on 14 November 2019).
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef]
- Quamar, M.M. Sociology of the veil in saudi arabia: Dress code, individual choices, and questions on women’s empowerment. Dig. Middle East Stud. 2016, 25, 315–337. [Google Scholar] [CrossRef]
- Rubio-Valera, M.; Pons-Vigués, M.; Martínez-Andrés, M.; Moreno-Peral, P.; Berenguera, A.; Fernández, A. Barriers and facilitators for the implementation of primary prevention and health promotion activities in primary care: A synthesis through meta-ethnography. PLoS ONE 2014, 9, e89554. [Google Scholar] [CrossRef]
- Al-Hamdan, R.; Avery, A.; Salter, A.; Al-Disi, D.; Al-Daghri, N.M.; McCullough, F. Identification of education models to improve health outcomes in arab women with pre-diabetes. Nutrients 2019, 11, 1113. [Google Scholar] [CrossRef]
- Al-Bannay, H.R.; Jongbloed, L.E.; Jarus, T.; Alabdulwahab, S.S.; Khoja, T.A.; Dean, E. Outcomes of a type 2 diabetes education program adapted to the cultural contexts of saudi women: A pilot study. Saudi Med. J. 2015, 36, 869. [Google Scholar] [CrossRef]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2014, 37, S81–S90. [Google Scholar] [CrossRef]
- Al-Daghri, N.M.; Alfawaz, H.; Aljohani, N.J.; Al-Saleh, Y.; Wani, K.; Alnaami, A.M.; Alharbi, M.; Kumar, S. A 6-month “self-monitoring” lifestyle modification with increased sunlight exposure modestly improves vitamin d status, lipid profile and glycemic status in overweight and obese saudi adults with varying glycemic levels. Lipids Health Dis. 2014, 13, 87. [Google Scholar] [CrossRef]
- Alfawaz, H.; Wani, K.; Alnaami, A.; Al-Saleh, Y.; Aljohani, N.; Al-Attas, O.; Alokail, M.; Kumar, S.; Al-Daghri, N. Effects of different dietary and lifestyle modification therapies on metabolic syndrome in prediabetic arab patients: A 12-month longitudinal study. Nutrients 2018, 10, 383. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfeler, E.; Lang, A.G.; Buchner, A. Statistical power analyses using G*Power 3: A flexible statistical power analysis program for the social, behavioral and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Lindström, J.; Ilanne-Parikka, P.; Peltonen, M.; Aunola, S.; Eriksson, J.G.; Hemiö, K.; Hämäläinen, H.; Härkönen, P.; Keinänen-Kiukaanniemi, S.; Laakso, M. Sustained reduction in the incidence of type 2 diabetes by lifestyle intervention: Follow-up of the finnish diabetes prevention study. Lancet 2006, 368, 1673–1679. [Google Scholar] [CrossRef]
- Hamman, R.F.; Wing, R.R.; Edelstein, S.L.; Lachin, J.M.; Bray, G.A.; Delahanty, L.; Hoskin, M.; Kriska, A.M.; Mayer-Davis, E.J.; Pi-Sunyer, X. Effect of weight loss with lifestyle intervention on risk of diabetes. Diabetes Care 2006, 29, 2102–2107. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Economic costs of diabetes in the us in 2017. Diabetes Care 2018, 41, 917–928. [Google Scholar] [CrossRef]
- Atlas, D.; International Diabetes Federation. IDF Diabetes Atlas, 8th ed.; International Diabetes Federation: Brussels, Belgium, 2017; Available online: https://www.idf.org/e-library/epidemiology-research/diabetes-atlas/134-idf-diabetes-atlas-8th-edition.html (accessed on 4 February 2020).
- Riddle, M.C.; Herman, W.H. The cost of diabetes care—An elephant in the room. Diabetes Care 2018, 41, 929–932. [Google Scholar] [CrossRef]
- Leitner, D.R.; Frühbeck, G.; Yumuk, V.; Schindler, K.; Micic, D.; Woodward, E.; Toplak, H. Obesity and type 2 diabetes: Two diseases with a need for combined treatment strategies-easo can lead the way. Obes. Facts 2017, 10, 483–492. [Google Scholar] [CrossRef]
- Wells, J.C. The diabesity epidemic in the light of evolution: Insights from the capacity–load model. Diabetologia 2019, 62, 1740–1750. [Google Scholar] [CrossRef]
- Kosaka, K.; Noda, M.; Kuzuya, T. Prevention of type 2 diabetes by lifestyle intervention: A japanese trial in igt males. Diabetes Res. Clin. Pract. 2005, 67, 152–162. [Google Scholar] [CrossRef]
- Group, D.P.P.R. 10-year follow-up of diabetes incidence and weight loss in the diabetes prevention program outcomes study. Lancet 2009, 374, 1677–1686. [Google Scholar]
- Xu, Y.; Wang, L.; He, J.; Bi, Y.; Li, M.; Wang, T.; Wang, L.; Jiang, Y.; Dai, M.; Lu, J. Prevalence and control of diabetes in chinese adults. JAMA 2013, 310, 948–959. [Google Scholar] [CrossRef]
- Penn, L.; White, M.; Oldroyd, J.; Walker, M.; Alberti, K.G.M.; Mathers, J.C. Prevention of type 2 diabetes in adults with impaired glucose tolerance: The european diabetes prevention rct in newcastle upon tyne, UK. BMC Public Health 2009, 9, 342. [Google Scholar] [CrossRef]
- Moore, S.M.; Hardie, E.A.; Hackworth, N.J.; Critchley, C.R.; Kyrios, M.; Buzwell, S.A.; Crafti, N.A. Can the onset of type 2 diabetes be delayed by a group-based lifestyle intervention? A randomised control trial. Psychol. Health 2011, 26, 485–499. [Google Scholar] [CrossRef] [PubMed]
- Magkos, F.; Fraterrigo, G.; Yoshino, J.; Luecking, C.; Kirbach, K.; Kelly, S.C.; De Las Fuentes, L.; He, S.; Okunade, A.L.; Patterson, B.W. Effects of moderate and subsequent progressive weight loss on metabolic function and adipose tissue biology in humans with obesity. Cell Metab. 2016, 23, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Maghsoudi, Z.; Azadbakht, L. How dietary patterns could have a role in prevention, progression, or management of diabetes mellitus? Review on the current evidence. J. Res. Med. Sci. 2012, 17, 694–709. [Google Scholar] [PubMed]
- Alfawaz, H.; Naeef, A.F.; Wani, K.; Khattak, M.N.K.; Sabico, S.; Alnaami, A.M.; Al-Daghri, N.M. Improvements in glycemic, micronutrient, and mineral indices in arab adults with pre-diabetes post-lifestyle modification program. Nutrients 2019, 11, 2775. [Google Scholar] [CrossRef]
- Prevalence of Prediabetes. 2015. Available online: https://www.Cdc.Gov/diabetes/data/statistics-report/prevalence.Html (accessed on 2 December 2019).
- Perreault, L.; Temprosa, M.; Mather, K.J.; Horton, E.; Kitabchi, A.; Larkin, M.; Montez, M.G.; Thayer, D.; Orchard, T.J.; Hamman, R.F. Regression from prediabetes to normal glucose regulation is associated with reduction in cardiovascular risk: Results from the diabetes prevention program outcomes study. Diabetes Care 2014, 37, 2622–2631. [Google Scholar] [CrossRef] [PubMed]
- Perreault, L.; Pan, Q.; Mather, K.J.; Watson, K.E.; Hamman, R.F.; Kahn, S.E.; Group, D.P.P.R. Effect of regression from prediabetes to normal glucose regulation on long-term reduction in diabetes risk: Results from the diabetes prevention program outcomes study. Lancet 2012, 379, 2243–2251. [Google Scholar] [CrossRef]


{kind=link}
| Lifestyle Intervention | GA Group | IG Group |
|---|---|---|
| (A) Diabetes Education | ● Orientation Session at recruitment ● Distribution of pamphlets/booklets at recruitment ● Seminars/workshops every four months | ● Orientation Session at recruitment ● Distribution of pamphlets/booklets at recruitment ● Seminars/workshops every four months |
| ● Health effects of impaired fasting glucose ● Health effects of overweight/obesity ● Risk of developing diabetes | ||
| (B) Education on Healthy diet | ||
| ● Healthy food and lifestyle choices ● Nutritional components of food ● Healthy Eating Plate (HEP) | ||
| (C) Education on benefits of physical activity | ||
| ● Health effects of sedentary behavior ● Concept of wellbeing | ||
| (D) Dietary counseling | ● No | ● Individual consultation with a dietician ● Follow up through phone call/email/short message service |
| ● Assessment of food intake ● Special dietary charts ● Ways to reduce total dietary fat <30% of energy ● Ways to increase fiber consumption to 15 g/1000 Kcal | ||
| (E) Physical activity counseling | ● No | ● Individual consultation with a physical therapist ● Pedometers (081565583, Patterson Medical) supplied ● Recommended at least 5000 steps/day ● Follow up through phone call/email/short message service |
| ● Assessment of physical activity levels ● Special physical activity/exercise/yoga charts ● Concept of calorie burn ● Concept of Metabolic Equivalents (MET) ● Saudi guidelines for management of obesity | ||
| (F) Fasting blood samples and Anthropometrics | ● Baseline, 6M and 12M ● Baseline and every six months | ● Baseline, 6M and 12M ● Baseline and every six months |
| Parameters | GA (n = 150) | IG (n = 150) | p -Value |
|---|---|---|---|
| Age group (years) ^ | |||
| 20-29 | 14 (9.3) | 13 (8.7) | 0.09 |
| 30-39 | 40 (26.7) | 37 (24.7) | |
| 40-49 | 50 (33.3) | 60 (40.0) | |
| 50-73 | 46 (30.7) | 40 (26.6) | |
| Marital Status ^ | |||
| Married | 84 (56.0) | 76 (50.7) | 0.11 |
| Not married | 21 (14.0) | 18 (12.0) | |
| NA | 45 (30.0) | 56 (37.3) | |
| Sex^ | |||
| Male | 42 (28.0) | 50 (33.3) | 0.12 |
| Female | 108 (72.0) | 100 (66.6) | |
| Nutritional status ^ | |||
| Lean | 8 (5.3) | 14 (9.3) | 0.25 |
| Overweight | 40 (26.7) | 46 (30.7) | |
| Obese | 96 (64.0) | 81 (54.0) | |
| NA | 6 (4.0) | 9 (6.0) | |
| Age (years)# | 43.75 ± 10.9 | 43.10 ± 9.4 | 0.61 |
| Weight (kg)# | 81.95 ± 14.3 | 81.26 ± 15.5 | 0.72 |
| BMI (kg/m2)# | 32.92 ± 6.0 | 31.71 ± 6.0 | 0.12 |
| Waist (cm)# | 96.96 ± 8.6 | 96.45 ± 13.4 | 0.74 |
| Hips (cm)# | 110.87 ± 9.1 | 111.85 ± 11.4 | 0.48 |
| Systolic BP (mmHg)# | 120.17 ± 13.5 | 121.54 ± 14.7 | 0.45 |
| Diastolic BP (mmHg)# | 76.46 ± 11.6 | 76.3 ± 11.0 | 0.91 |
| Total Cholesterol (mmol/L)# | 4.85 ± 1 | 5.29 ± 1.3 | 0.001 |
| HDL-Cholesterol (mmol/L)# | 1.08 ± 0.3 | 1.17 ± 0.4 | 0.03 |
| Triglycerides (mmol/L)# | 1.45 (1.1, 2.0) | 1.49 (1.1, 2.0) | 0.84 |
| Glucose (mmol/L)# | 6.17 ± 0.6 | 6.09 ± 0.4 | 0.22 |
| Insulin (μU/mL)$ | 15.83 (12.4, 16.5) | 16.59 (16.4, 16.7) | 0.01 |
| Groups | Intervention Effects (Adjusted Mean Change, p) | |||||
|---|---|---|---|---|---|---|
| Time-point | GA (n = 138) | IG (n = 129) | GA (6M vs. B) | GA (12M vs. B) | IG (6M vs. B) | IG (12M vs. B) |
| Anthropometric characteristics | ||||||
| Weight (kg) # | ||||||
| Baseline | 82.56 ± 13.8 | 80.71 ± 15.7 | 0.47, 0.48 | 0.57, 0.46 | −0.91, 0.06 | −1.96, <0.01 |
| 6-months | 83.09 ± 14.1 | 79.56 ± 15.6 | ||||
| 12-months | 83.27 ± 13.7 | 78.01 ± 15.8 | ||||
| BMI (kg/m2) # | ||||||
| Baseline | 33.13 ± 5.9 | 31.67 ± 6.0 | 0.20, 0.42 | 0.24, 0.44 | −0.31, 0.15 | −0.76, <0.01 |
| 6-months | 33.36 ± 6.1 | 31.24 ± 6.1 | ||||
| 12-months | 33.39 ± 5.9 | 30.57 ± 6.3 | ||||
| Physiological Indices | ||||||
| Systolic Blood Pressure (mmHg) # | ||||||
| Baseline | 120.28 ± 13.5 | 121.23 ± 14.6 | −2.25, 0.36 | −0.84, 1.0 | −2.12, 0.52 | −2.59, 0.08 |
| 6-months | 118.30 ± 14.7 | 119.83 ± 17.9 | ||||
| 12-months | 119.20 ± 15.9 | 118.27 ± 16.9 | ||||
| Diastolic Blood Pressure (mmHg) # | ||||||
| Baseline | 76.70 ± 11.8 | 76.08 ± 10.8 | −0.23, 0.96 | 0.27, 0.72 | −0.43, 0.84 | −1.46, 0.15 |
| 6-months | 76.43 ± 11.9 | 75.57 ± 11.9 | ||||
| 12-months | 77.07 ± 13.5 | 74.53 ± 12.2 | ||||
| Glycemic Indices | ||||||
| Fasting Glucose (mmol/L) # | ||||||
| Baseline | 6.17 ± 0.6 | 6.11 ± 0.4 | 0.07, 1.00 | −0.18, 0.52 | −0.38, <0.01 | −0.47, <0.01 |
| 6-months | 6.16 ± 1.1 | 5.72 ± 1.1 | ||||
| 12-months | 5.92 ± 0.8 | 5.59 ± 0.8 | ||||
| Insulin (μU/mL) $ | ||||||
| Baseline | 15.78 (11.9,16.1) | 16.56 (16.5,16.7) | 0.02, 0.18 | 0.03, 0.45 | 0.04, 0.39 | −0.03, 0.05 |
| 6-months | 15.80 (10.5,15.9) | 16.65 (16.6,16.7) | ||||
| 12-months | 15.83 (11.6,15.9) | 15.99 (15.9,16.1) | ||||
| Lipid Indices | ||||||
| Total Cholesterol (mmol/L) # | ||||||
| Baseline | 4.84 ± 0.9 | 5.25 ± 1.2 | −0.06, 1.00 | −0.23, 0.12 | −0.19, 0.24 | 0.28, 0.17 |
| 6-months | 4.67 ± 1.1 | 5.10 ± 1.1 | ||||
| 12-months | 4.63 ± 1.1 | 4.94 ± 1.0 | ||||
| HDL-Cholesterol (mmol/L) # | ||||||
| Baseline | 1.07 ± 0.3 | 1.17 ± 0.4 | −0.10, 0.06 | −0.13, 0.02 | 0.03, 1.00 | 0.05, 1.00 |
| 6-months | 0.94 ± 0.4 | 1.19 ± 0.4 | ||||
| 12-months | 0.97 ± 0.4 | 1.15 ± 0.4 | ||||
| Triglycerides (mmol/L) $ | ||||||
| Baseline | 1.47 (1.1,2.1) | 1.48 (1.1,2.0) | 0.02, 1.00 | −0.01, 0.64 | −0.04, 0.23 | −0.03, 0.17 |
| 6-months | 1.51 (1.1,2.1) | 1.35 (1.0,1.9) | ||||
| 12-months | 1.43 (1.1,2.0) | 1.40 (1.0,1.9) | ||||
| Category | % Change at End of Study | GA n (%) | IG n (%) | p |
|---|---|---|---|---|
| Weight | ||||
| 1 | >5% reduced | 17 (12.3) | 48 (37.2) | <0.01 |
| 2 | 1–5% reduced | 8 (5.8) | 43 (33.3) | <0.01 |
| 3 | 1–5% increased | 62 (44.9) | 11 (8.5) | <0.01 |
| 4 | >5% increased | 11 (8.0) | 4 (3.1) | 0.08 |
| 5 | <1% increased/<1% reduced | 40 (29.0) | 23 (17.8) | 0.02 |
| Fasting Glucose | ||||
| 1 | >25% reduced | 2 (1.4) | 11 (8.5) | 0.007 |
| 2 | 15.1%–25% reduced | 7 (5.1) | 18 (14.0) | 0.013 |
| 3 | 5.1%–15% reduced | 18 (13.0) | 27 (20.9) | 0.08 |
| 4 | 1%–5% reduced | 26 (18.8) | 17 (13.2) | 0.21 |
| 5 | 1%–5% increased | 19 (13.8) | 6 (4.7) | 0.01 |
| 6 | 5.1%–15% increased | 18 (13.0) | 9 (7.0) | 0.10 |
| 7 | 15.1%–25% increased | 4 (2.9) | 7 (5.4) | 0.29 |
| 8 | >25% increased | 8 (5.8) | 0 (0.0) | 0.005 |
| 9 | Normal FG after 12-months | 30 (21.7) | 60 (46.5) | <0.01 |
| 10 | FG > 7mmol/L after 12-months | 19 (13.8) | 5 (3.9) | 0.005 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wani, K.; Alfawaz, H.; Alnaami, A.M.; Sabico, S.; Khattak, M.N.K.; Al-Attas, O.; Alokail, M.S.; Alharbi, M.; Chrousos, G.; Kumar, S.; et al. Effects of a 12-Month Intensive Lifestyle Monitoring Program in Predominantly Overweight/Obese Arab Adults with Prediabetes. Nutrients 2020, 12, 464. https://doi.org/10.3390/nu12020464
Wani K, Alfawaz H, Alnaami AM, Sabico S, Khattak MNK, Al-Attas O, Alokail MS, Alharbi M, Chrousos G, Kumar S, et al. Effects of a 12-Month Intensive Lifestyle Monitoring Program in Predominantly Overweight/Obese Arab Adults with Prediabetes. Nutrients. 2020; 12(2):464. https://doi.org/10.3390/nu12020464
Chicago/Turabian StyleWani, Kaiser, Hanan Alfawaz, Abdullah M. Alnaami, Shaun Sabico, Malak Nawaz Khan Khattak, Omar Al-Attas, Majed S. Alokail, Mohammed Alharbi, George Chrousos, Sudhesh Kumar, and et al. 2020. "Effects of a 12-Month Intensive Lifestyle Monitoring Program in Predominantly Overweight/Obese Arab Adults with Prediabetes" Nutrients 12, no. 2: 464. https://doi.org/10.3390/nu12020464
APA StyleWani, K., Alfawaz, H., Alnaami, A. M., Sabico, S., Khattak, M. N. K., Al-Attas, O., Alokail, M. S., Alharbi, M., Chrousos, G., Kumar, S., & Al-Daghri, N. M. (2020). Effects of a 12-Month Intensive Lifestyle Monitoring Program in Predominantly Overweight/Obese Arab Adults with Prediabetes. Nutrients, 12(2), 464. https://doi.org/10.3390/nu12020464