Performance Factors Influencing Efficacy and Effectiveness of Iron Fortification Programs of Condiments for Improving Anemia Prevalence and Iron Status in Populations: A Systematic Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection Criteria
2.3. Data Extraction
2.4. Study Quality Assessment
2.5. Data Synthesis
3. Results
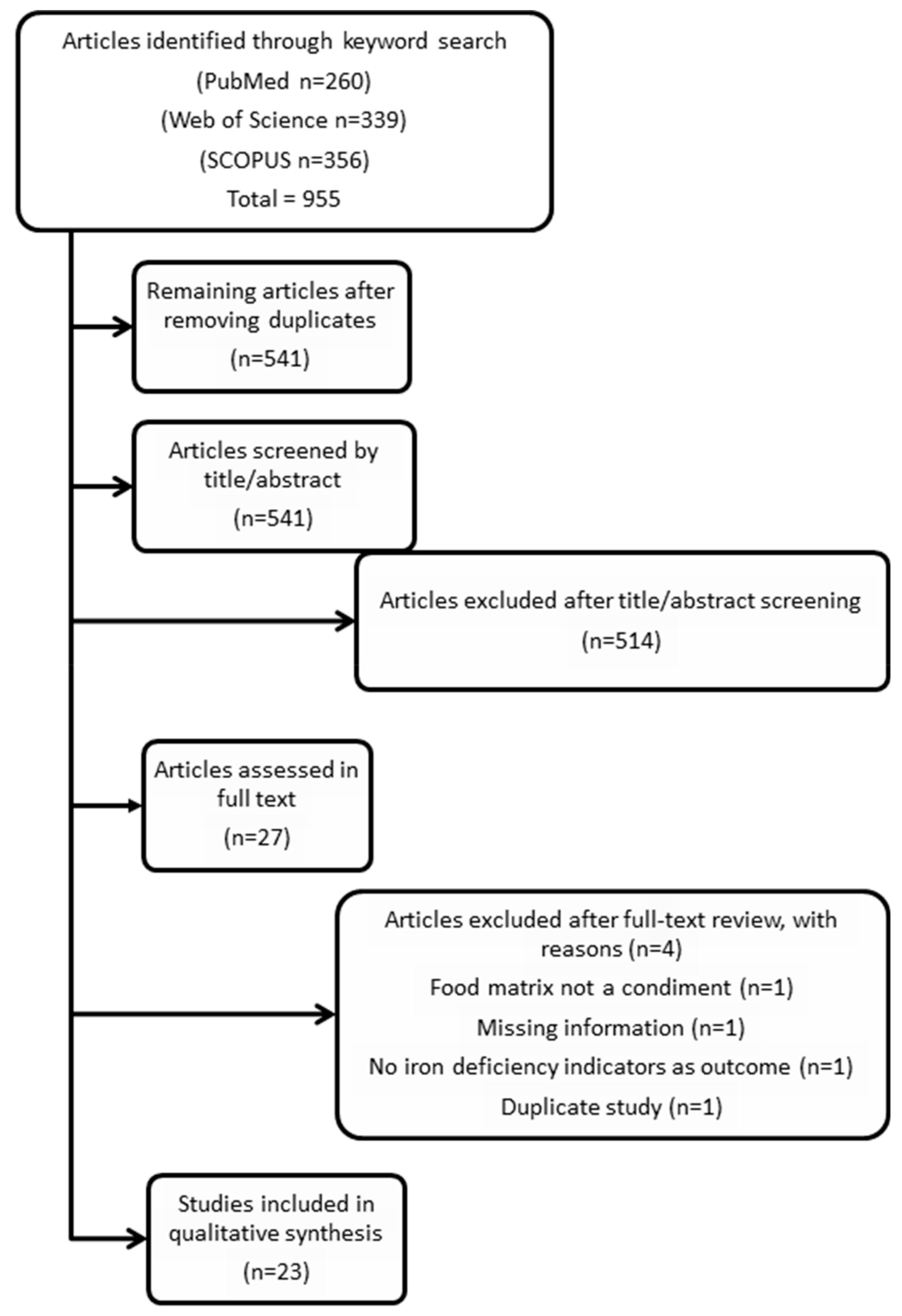
3.1. Study Selection
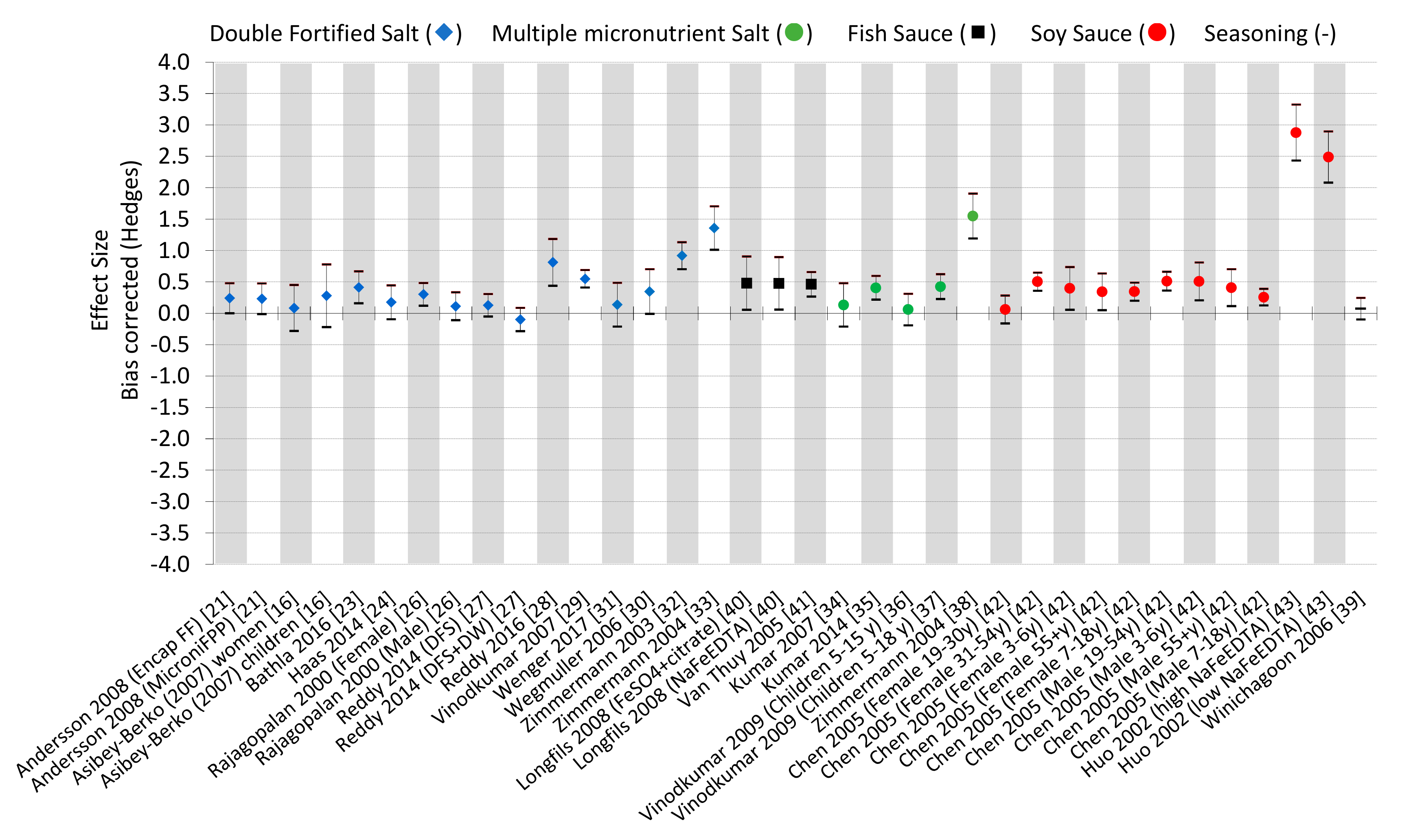
3.2. Data Analysis
3.3. Study Quality Assessment
3.4. Data Synthesis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- McLean, E.; Cogswell, M.; Egli, I.; Wojdyla, D.; De Benoist, B. Worldwide prevalence of anaemia, WHO vitamin and mineral nutrition information system, 1993–2005. Public Health Nutr. 2009, 12, 444–454. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.H. Anemia and iron deficiency: Effects on pregnancy outcome. Am. J. Clin. Nutr. 2000, 71, 1280S–1284S. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Health Observatory Data Repository. WHO: Geneva, Switzerland, 2017. Available online: apps.who.int/gho/data/node.main (accessed on 19 January 2020).
- WHO. WHO Sixty-Fifth World Health Assembly; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Zimmermann, M.B.; Hurrell, R.F. Nutritional iron deficiency. Lancet 2007, 370, 511–520. [Google Scholar] [CrossRef]
- Bank, W. Enriching Lives: Overcoming Vitamin and Mineral Malnutrition in Developing Countries; World Bank: Washington, DC, USA, 1994. [Google Scholar]
- Consensus, C. Copenhagen consensus 2008—Results. Cph. Consens. Cent. 2008. Available online: http://www.luo.ch/win-win/files/001-2_vision_ranking.copenhagen.concensus.pdf (accessed on 6 January 2019).
- De Mejia, E.G.; Aguilera-Gutiérrez, Y.; Martin-Cabrejas, M.A.; Mejia, L.A. Industrial processing of condiments and seasonings and its implications for micronutrient fortification. Ann. N. Y. Acad. Sci. 2015, 1357, 8–28. [Google Scholar] [CrossRef] [PubMed]
- Mejia, L.A.; Bower, A.M. The global regulatory landscape regarding micronutrient fortification of condiments and seasonings. Ann. N. Y. Acad. Sci. 2015, 1357, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Timbo. Celusal Salt. Available online: www.timbo.com.ar/eng/productos_hogar_sales.php (accessed on 19 November 2019).
- Venkatesh Mannar, M.G.; Hurrell, R. Food Fortification in a Globalized World, 1st ed.; Academic Press: London, UK, 2018; p. 414. [Google Scholar]
- Horton, S.; Wesley, A.; Mannar, M.V. Double-fortified salt reduces anemia, benefit: Cost ratio is modestly favorable. Food Policy 2011, 36, 581–587. [Google Scholar] [CrossRef]
- Hess, S.; Tecklenburg, L.; Eichler, K. Micronutrient fortified condiments and noodles to reduce anemia in children and adults—A literature review and meta-analysis. Nutrients 2016, 8, 88. [Google Scholar] [CrossRef]
- Ramírez-Luzuriaga, M.J.; Larson, L.M.; Mannar, V.; Martorell, R. Impact of double-fortified salt with iron and iodine on hemoglobin, anemia, and iron deficiency anemia: A systematic review and meta-analysis. Adv. Nutr. 2018, 9, 207–218. [Google Scholar] [CrossRef]
- Association, A.D. Evidence Analysis Manual: Steps in the ADA Evidence Analysis Process; American Dietetic Association: Chicago, IL, USA, 2008. [Google Scholar]
- Siopis, G.; Chey, T.; Allman-Farinelli, M. A systematic review and meta—Analysis of interventions for weight management using text messaging. J. Hum. Nutr. Diet. 2015, 28, 1–15. [Google Scholar] [CrossRef]
- Centre for Evaluation and Monitoring. D.U. Effect Size Calculator; Centre for Evaluation and Monitoring: Durham, England, 2017. [Google Scholar]
- Ialongo, C. Understanding the effect size and its measures. Biochem. Med. Biochem. Med. 2016, 26, 150–163. [Google Scholar] [CrossRef] [PubMed]
- Ross, S.D.; Fahrbach, K.; Frame, D.; Scheye, R.; Connelly, J.E.; Glaspy, J. The Effect of Anemia Treatment on Selected Health-Related Quality-of-Life Domains: A Systematic Review; Elsevier: Amsterdam, The Netherlands, 2003. [Google Scholar]
- Sullivan, G.M.; Feinn, R. Using effect size—Or why the P value is not enough. J. Grad. Med Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.; Thankachan, P.; Muthayya, S.; Goud, R.B.; Kurpad, A.V.; Hurrell, R.F.; Zimmermann, M.B. Dual fortification of salt with iodine and iron: A randomized, double-blind, controlled trial of micronized ferric pyrophosphate and encapsulated ferrous fumarate in southern India. Am. J. Clin. Nutr. 2008, 88, 1378–1387. [Google Scholar] [PubMed]
- Asibey-Berko, E.; Zlotkin, S.; Yeung, G.; Nti-Nimako, W.; Ahunu, B.; Kyei-Faried, S.; Johnston, J.; Tondeur, M.; Mannar, V. Dual fortification of salt with iron and iodine in women and children in rural Ghana. East Afr. Med. J. 2007, 84, 473–480. [Google Scholar]
- Bathla, S.; Grover, K. Effect of supplementation of double fortified salt in mid day meal programme on the nutritional status of anaemic children. Indian J. Agric. Biochem. 2016, 29, 189–194. [Google Scholar] [CrossRef]
- Haas, J.D.; Rahn, M.; Venkatramanan, S.; Marquis, G.S.; Wenger, M.J.; Murray-Kolb, L.E.; Wesley, A.S.; Reinhart, G.A. Double-fortified salt is efficacious in improving indicators of iron deficiency in female Indian tea pickers. J. Nutr. 2014, 144, 957–964. [Google Scholar] [CrossRef]
- Nair, S.; Bandyopadhyay, S.; Skaria, L. Impact assessment on DFS supplementation Post NHE on nutrient intake of critically anemic pregnant mothers in a tribal set up of Gujarat. Indian J. Community Health 2014, 26, 170–174. [Google Scholar]
- Rajagopalan, S.; Vinodkumar, M. Effects of salt fortified with iron and iodine on the haemoglobin levels and productivity of tea pickers. Food Nutr. Bull. 2000, 21, 323–329. [Google Scholar] [CrossRef]
- Reddy, K.J.; Nair, S. Double fortified salt and deworming—Game changers in the battle against iodine and iron malnutrition in Indian school children. Indian J. Community Health 2014, 26, 175–182. [Google Scholar]
- Reddy, K.J.; Nair, S. Double fortified salt: An effective measure to control micronutrient deficiencies in Indian pregnant women. Int. J. Community Med. Public Health 2017, 3, 679–686. [Google Scholar] [CrossRef]
- Vinodkumar, M.; Rajagopalan, S.; Bhagwat, I.; Singh, S.; Parmar, B.S.; Mishra, O.P.; Upadhyay, S.S.; Bhalia, N.; Deshpande, S.R. A multicenter community study on the efficacy of double-fortified salt. Food Nutr. Bull. 2007, 28, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Wegmüller, R.; Camara, F.; Zimmermann, M.B.; Adou, P.; Hurrell, R.F. Salt dual-fortified with iodine and micronized ground ferric pyrophosphate affects iron status but not hemoglobin in children in Cote d’Ivoire. J. Nutr. 2006, 136, 1814–1820. [Google Scholar] [CrossRef] [PubMed]
- Wenger, M.J.; Murray-Kolb, L.E.; Nevins, J.E.; Venkatramanan, S.; Reinhart, G.A.; Wesley, A.; Haas, J.D. Consumption of a double-fortified salt affects perceptual, attentional, and mnemonic functioning in women in a randomized controlled trial in India. J. Nutr. 2017, 147, 2297–2308. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Zeder, C.; Chaouki, N.; Saad, A.; Torresani, T.; Hurrell, R.F. Dual fortification of salt with iodine and microencapsulated iron: A randomized, double-blind, controlled trial in Moroccan schoolchildren. Am. J. Clin. Nutr. 2003, 77, 425–432. [Google Scholar] [CrossRef]
- Zimmermann, M.B.; Wegmueller, R.; Zeder, C.; Chaouki, N.; Rohner, F.; Saïssi, M.; Torresani, T.; Hurrell, R.F. Dual fortification of salt with iodine and micronized ferric pyrophosphate: A randomized, double-blind, controlled trial. Am. J. Clin. Nutr. 2004, 80, 952–959. [Google Scholar] [CrossRef]
- Kumar, M.V.; Rajagopalan, S. Multiple micronutrient fortification of salt and its effect on cognition in Chennai school children. Asia Pac. J. Clin. Nutr. 2007, 16, 505–511. [Google Scholar]
- Kumar, M.V.; Nirmalan, P.K.; Erhardt, J.G.; Rahmathullah, L.; Rajagopalan, S. An efficacy study on alleviating micronutrient deficiencies through a multiple micronutrient fortified salt in children in South India. Asia Pac. J. Clin. Nutr. 2014, 23, 413–422. [Google Scholar] [CrossRef]
- Vinodkumar, M.; Rajagopalan, S. Multiple micronutrient fortification of salt. Eur. J. Clin. Nutr. 2009, 63, 437. [Google Scholar] [CrossRef]
- Vinodkumar, M.; Erhardt, J.G.; Rajagopalan, S. Impact of a multiple-micronutrient fortified salt on the nutritional status and memory of schoolchildren. Int. J. Vitam. Nutr. Res. 2009, 79, 348–361. [Google Scholar] [CrossRef]
- Zimmermann, M.B.; Wegmueller, R.; Zeder, C.; Chaouki, N.; Biebinger, R.; Hurrell, R.F.; Windhab, E. Triple fortification of salt with microcapsules of iodine, iron, and vitamin A. Am. J. Clin. Nutr. 2004, 80, 1283–1290. [Google Scholar] [CrossRef]
- Winichagoon, P.; McKenzie, J.E.; Chavasit, V.; Pongcharoen, T.; Gowachirapant, S.; Boonpraderm, A.; Manger, M.S.; Bailey, K.B.; Wasantwisut, E.; Gibson, R.S. A multimicronutrient-fortified seasoning powder enhances the hemoglobin, zinc, and iodine status of primary school children in North East Thailand: A randomized controlled trial of efficacy. J. Nutr. 2006, 136, 1617–1623. [Google Scholar] [CrossRef] [PubMed]
- Longfils, P.; Monchy, D.; Weinheimer, H.; Chavasit, V.; Nakanishi, Y.; Schümann, K. A comparative intervention trial on fish sauce fortified with NaFe-EDTA and FeSO4+ citrate in iron deficiency anemic school children in Kampot, Cambodia. Asia Pac. J. Clin. Nutr. 2008, 17, 250–257. [Google Scholar] [PubMed]
- Van Thuy, P.; Berger, J.; Nakanishi, Y.; Khan, N.C.; Lynch, S.; Dixon, P. The use of NaFeEDTA-fortified fish sauce is an effective tool for controlling iron deficiency in women of childbearing age in rural Vietnam. J. Nutr. 2005, 135, 2596–2601. [Google Scholar] [CrossRef]
- Chen, J.; Zhao, X.; Zhang, X.; Yin, S.; Piao, J.; Huo, J.; Yu, B.; Qu, N.; Lu, Q.; Wang, S. Studies on the effectiveness of NaFeEDTA-fortified soy sauce in controlling iron deficiency: A population-based intervention trial. Food Nutr. Bull. 2005, 26, 177–186. [Google Scholar] [CrossRef]
- Huo, J.; Sun, J.; Miao, H.; Yu, B.; Yang, T.; Liu, Z.; Lu, C.; Chen, J.; Zhang, D.; Ma, Y. Therapeutic effects of NaFeEDTA—Fortified soy sauce in anaemic children in China. Asia Pac. J. Clin. Nutr. 2002, 11, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Martorell, R.; de Romaña, D.L. Components of successful staple food fortification programs: Lessons from Latin America. Food Nutr. Bull. 2017, 38, 384–404. [Google Scholar] [CrossRef]
- Green, R.; Mitra, A.D. Megaloblastic anemias: Nutritional and other causes. Med Clin. 2017, 101, 297–317. [Google Scholar]
- Farid, Z.; Bassily, S.; Lehman, J., Jr.; Kent, D.; Haxton, J.; Patwardhan, V.; Hassan, A.; Mahran, A. Iron loss and reabsorption in Ancylostoma duodenale infection and bilharzial colonic polyposis. Trans. R. Soc. Trop. Med. Hyg. 1970, 64, 881–884. [Google Scholar] [CrossRef]
- Girum, T.; Wasie, A. The effect of deworming school children on anemia prevalence: A systematic review and meta-analysis. Open Nurs. J. 2018, 12, 155–161. [Google Scholar] [CrossRef]
- Watanapaisantrakul, R.; Chavasit, V.; Kongkachuichai, R. Fortification of soy sauce using various iron sources: Sensory acceptability and shelf stability. Food Nutr. Bull. 2006, 27, 19–25. [Google Scholar] [CrossRef]
- Huo, J.S.; Yin, J.Y.; Sun, J.; Huang, J.; Lu, Z.X.; Regina, M.P.; Chen, J.S.; Chen, C.M. Effect of NaFeEDTA-fortified soy sauce on anemia prevalence in China: A systematic review and meta-analysis of randomized controlled trials. Biomed. Environ. Sci. 2015, 28, 788–798. [Google Scholar] [CrossRef]
- Mejía, L.A.; Chew, F. Hematological effect of supplementing anemic children with vitamin A alone and in combination with iron. Am. J. Clin. Nutr. 1988, 48, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Bothwell, T.H.; MacPhail, A.P. The potential role of NaFeEDTA as an iron fortificant. Int. J. Vitam. Nutr. Res. 2004, 74, 421–434. [Google Scholar] [CrossRef] [PubMed]
- Karanicolas, P.J.; Farrokhyar, F.; Bhandari, M. Blinding: Who, what, when, why, how? Can. J. Surg. 2010, 53, 345. [Google Scholar] [PubMed]
- Syifaa, A.S.; Jinap, S.; Sanny, M.; Khatib, A. Chemical profiling of different types of soy sauce and the relationship with its sensory attributes. J. Food Qual. 2016, 39, 714–725. [Google Scholar] [CrossRef]
- Shahar, S.; You, Y.X.; Zainuddin, N.S.; Michael, V.; Ambak, R.; Haron, H.; He, F.J.; MacGregor, G.A. Sodium content in sauces—A major contributor of sodium intake in Malaysia: A cross-sectional survey. BMJ Open 2019, 9, e025068. [Google Scholar] [CrossRef] [PubMed]
- The National Academies of Sciences Engineering and Medicine. Dietary Reference Intakes Tables and Application. Available online: http://nationalacademies.org/HMD/Activities/Nutrition/SummaryDRIs/DRI-Tables.aspx (accessed on 3 December 2019).
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Hipgrave, D.B.; Chang, S.; Li, X.; Wu, Y. Salt and sodium intake in China. JAMA 2016, 315, 703–705. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study/Objective/Country/Duration and Experimental Design/Subjects | Condiment/ Fe Source/Concentration | Iron Intervention Outcomes (Hemoglobin, Anemia Prevalence, and Ferritin) | Selected Performance Indicators | ||||
|---|---|---|---|---|---|---|---|
| Education/Behavior Change Component | Parasitic Treatment | Sensory/Acceptability Testing | Monitoring Compliance/Adherence | Other Micronutrients Associated with Anemia | |||
| Andersson et al., 2008 [21] Compare the efficacy of DFS with FePP and EFF India 10 mo RCT 458 rural children (5–15 y) | DFS Micronized ground FePP or encapsulated FF 2 mg Fe/g salt | Hb (+0.6 * and +0.8 * g/dL, FePP and FF) Anemia prevalence (−9.1% * and −10.1% *, FePP and FF) Ferritin (+6.4 * and +4.9 * μg/L, FePP and FF) | At each salt distribution, families were instructed that the new salt should be used for all cooking and food preparation. Health effects were explained to noncompliant families. | Albendazole treatment at 1 mo and 8 mo | Sensory panel (n = 18 women). Adverse color changes in cooked foods using FF. Acceptability testing pre- and post-study with women at a local market (n = 50 women) | Salt container was weighed on four consecutive mornings (n = 80 households pre-study; n = 85 households post-study). Salt intake per person was 11.3 ± 5.1 g/d throughout the 10 mo study period. 17% of households (n = 20) in the FF group stopped using the salt for short periods at some point during the trial. Salt consumption was resumed after beneficial health effects were explained. | Vitamin A supplements (200,000 IU) distributed at 1 mo |
| Asibey-Berko et al., 2007 [22] Test the efficacy of DFS on anemia and iodine deficiency of women and children Ghana 8 mo RCT 300 NP, NL women (15–45 y) and 157 children (1–5 y) | DFS FF 1 mg Fe/g salt | No Hb post-treatment data Anemia prevalence (−21.7% * and +3.3%, children and women) Ferritin NA | NA | NA | 2.7% of the women in the DFS group reported darkening of fried plantains with DFS | Weekly household visits to monitor salt usage, encourage compliance, and check health status (diarrhea, pregnancy, malaria, constipation). No adherence data were available. | NA |
| Bathla et al., 2016 [23] Evaluate DFS effect on nutritional status of anemic children India 90 day pre- and post-test design 120 children with Hb <12 g/dL (7–9 y) | DFS FS 0.85 mg Fe/g salt | Hb (+0.6 * g/dL) Anemia prevalence (−6.6% *) Ferritin NA | NA | NA | NA | Supervision of a researcher during mid-day meal. Adherence NA. | NA |
| Haas et al., 2014 [24] Test the efficacy of DFS in reducing ID in WRA India 7.5–9 mo RCT 212 NP women (18–55 y) | DFS Micro-encapsulated FF 1.1 mg Fe/g salt | Hb (+0.24 * g/dL) Anemia prevalence (+1%) Ferritin (+0.13 * log10 μg/mL) | NA | 200 mg of albendazole at −4 wk and at study midpoint | Stability, organoleptic, and acceptability testing of the DFS showed some discoloration and black specks, but the salt was still considered acceptable for consumption by all of the participants | Salt consumption was monitored at midpoint and endline by weighing salt bags, salt consumed at major meals, and dietary recalls. The salt consumption per person was 12.4 ± 7.9 g in the DFS group and 15.0 ± 13.6 g in the control group. | Folate deficiency (−13% *) Vitamin B12 deficiency (+9% *) |
| Nair et al., 2014 [25] Test efficacy of DFS with nutrition health education on pregnant, anemic mothers India 2 mo RCT 135 pregnant, anemic women | DFS Fe source NA 1 mg Fe/g salt | Hb (−0.15 g/dL) Anemia prevalence NA Ferritin NA | Nutrition Health Education (NHE) specifically pertaining to the use and storage of DFS, iron-rich foods, consequences of deficiency. | NA | NA | Compliance monitoring NA NHE improved adherence to salt consumption by 42%. | NA |
| Rajagopalan et al., 2000 [26] Determine if DFS improved the Hb and productivity of tea pickers India 1 y RCT 793 tea pickers | DFS Fe source NA 1 mg Fe/g salt | Hb (+0.85 * and 1.55 * g/dL, men and women) Anemia prevalence (−22.5% and −15.5%, dewormed and not dewormed) Ferritin NA | Education on DFS nutritional benefits, cooking demonstrations. DFS was introduced for 3 mo prior to the study to allow for behavior change. | Dewormed half the population at baseline | Through cooking demonstrations, they observed that the fortified salt did not change the color, taste, or appearance of the food | Periodic surprise visits to the houses of the workers and collected salt samples from their kitchens for analysis. These checks proved that the population was using only Nutrisalt. | NA |
| Reddy et al., 2014 [27] Assess the impact of DFS on iron and iodine status of schoolchildren India 9 mo longitudinal intervention study 947 schoolchildren (6–15 y) | DFS Source NA Concentration NA | Hb (+0.6 * g/dL and 0.21 * g/dL, deworming and not) Anemia prevalence (−6.3% * and +1.5%, deworming and not) Ferritin NA | All the groups were also provided nutrition and health education regarding the need and importance of iodine and iron nutrition in children. | Albendazole (400 mg) given twice | NA | NA | NA |
| Reddy et al., 2016 [28] Assess the impact of DFS on iron and iodine status of pregnant women India 9 mo RCT 150 pregnant women (<12 weeks gestation) | DFS Ferrous sulfate 1000 ppm at 10 g/day | Hb (+0.42 * g/dL) Anemia prevalence (−10.5%) Ferritin NA | NA | NA | NA | Nutrient intake was recorded using 24 h dietary recall information. | All pregnant women were on iron, folic acid, and calcium supplements during 2nd and 3rd trimester |
| Vinodkumar et al., 2007 [29] Test the stability of DFS during storage and to assess its efficacy in improving the iron and iodine status in communities India 1 y multicenter, single-blind, RCT 829 family members | DFS FS monohydrate chelated with malic acid and sodium hexameta-phosphate 1 mg Fe/g salt | Hb (+1.98 * g/dL) Anemia prevalence NA Ferritin NA | NA | Dewormed at baseline, 6 mo, and 12 mo | No complaints regarding taste. People noted that the amount of salt to be added to food was less, and that food turned slightly sour when kept for more than 6 h. After use for 1 y, 98%–100% of households rated the taste and color of DFS as acceptable. | NA | NA |
| Wegmueller et al., 2006 [30] Test efficacy of DFS Cote d’Ivoire 6 mo, double-blind, efficacy RCT 123 iron-deficient children (5–15 y) | DFS Micronized ground FePP 3 mg Fe/g salt | Hb (0 g/dL) Anemia prevalence (+5%) Ferritin (+15 * μg/L) | In a village meeting at the beginning of the study and at each of the monthly salt distribution, it was emphasized that the salt should be used for all cooking, food preparation, and at the table. | At the baseline screening and again at 4 mo, all children received an oral dose of 400 mg albendazole | Triangle test by 18–21 untrained local adults were not able to detect differences in color, odor, or taste in either traditional staples (rice, cassava, yam, plantain) or sauces (tomato, eggplant, okra, palm nut) | Remaining salt at the end of the month was weighed and the amount of salt consumed per day per person during the period since the last distribution calculated. Calculated per capita salt consumption in the households using DFS was 4.0 +/−2.5 and 6.1 +/−4.0 g/d at 1 and 6 mo. | Median vitamin A intake was at the EAR for children 2–5 y and above the EAR for children 6–15 y, women, and men, due to high consumption of red palm oil and refined palm oil fortified with retinyl palmitate. 7% of children had vitamin A deficiency at baseline |
| Wenger et al., 2017 [31] Assess the extent to which increases in dietary iron consumption are related to improvements in behavioral measures of perceptual, attentional, and mnemonic function India 10 mo RCT 126 NP women (18–55 y) | DFS Micro-encapsulated FF 1.1 mg Fe/g salt | Hb (+0.1 * g/dL) Anemia prevalence (−5% *) Ferritin (+12.5 * μg/L) | NA | 200 mg albendazole was administered to all eligible participants 4 wk before and 4 mo after the initial baseline blood collection | It was considered acceptable by participants in a previous study | NA | Folate deficiency (−22% *) Vitamin B12 (−14.8 * μg/L and +12% * deficiency) |
| Zimmermann et al., 2003 [32] Test DFS efficacy Morocco 9 mo double-blind, randomized trial 377 iodine-deficient children (6–15 y) | DFS FS hydrate encapsulated with partially hydrogenated vegetable oil 1 mg Fe/g salt | Hb (+1.4 * g/dL) Anemia prevalence (−25% *) Ferritin (+20 * μg/L) | At each monthly salt distribution, all salt used for cooking and food preparation was emphasized. | NA | Baseline acceptability interviews indicated nearly unanimous acceptance. At 8 mo, 14% of households rated the color unacceptable in the damp season. 17% reported that the salt changed the color of foods. In a triangle test, there was no significant, detectable difference in color, odor, or taste | NA | NA |
| Zimmermann et al., 2004 [33] Test efficacy of DFS for reducing the prevalence of iodine and iron deficiencies in children Morocco 10 mo double-blind, RCT 158 children (6–15 y) | DFS Micronized FePP 2 mg Fe/g salt | Hb (+1.5 * g/dL) Anemia prevalence (−25% *) Ferritin (+17.6 * μg/L) | NA | NA | Triangle test showed no significant difference in color, odor, or taste between the salts in any of the traditional foods | NA | NA |
| Kumar et al., 2007 [34] Test the efficacy of a multiple micronutrient fortified salt in improving the micronutrient status and health of schoolchildren and its effect on cognition India 1 y RCT 129 children (7–11 y) | Multiple micronutrient fortified salt (microencapsulated vitamin A, B1, B2, B6, B12, folic acid, niacin, calcium pantothenate, and iodine) Chelated FS 1 mg Fe/g salt | Hb (+0.65 * g/dL) Anemia prevalence NA Ferritin NA | NA | 400 mg albendazole at baseline, after 6 mo and 1 y of intervention (end of study) | The fortified salt did not change the color or taste of any food preparation | The continuous use of the fortified salt in all the meals prepared every day was monitored. All the food prepared is consumed. | Salt contained 5 μg folic acid/g salt, 400 μg vitamin B12/kg salt, and 300 IU vitamin A/g salt. Serum vitamin A significantly increased by 4.9 μg/dL |
| Kumar et al., 2014 [35] Establish the efficacy of multi-micronutrient fortified salt in addressing multiple micronutrient deficiencies among children compared to nutrition education and no intervention India 8 mo RCT 528 children (5–15 y) | Multiple micronutrient fortified salt (iron, iodine, vitamin A, vitamin B12, and folic acid) Chelated FS 1 mg Fe/g salt | Hb (+0.5 g/dL) Anemia prevalence (−13.4% *) Ferritin (+10.8 * μg/L) | Prior to the start of the study, a list of locally available foods that are rich in micronutrients and recipes for was communicated. Then, every month a specific topic was chosen, and in-depth education was given on that topic. | Children in all three arms of the study were given a tablet of albendazole (400 mg) at baseline and post-intervention after 8 mo | NA | Health workers visited the homes once a month to collect leftover salt. All homes only used the salt provided by the study in the intervention group, and salt was used to cook the children all three meals and an evening snack, daily. | Salt contained 1 μg folic acid/g salt, 0.1 μg vitamin B12/g salt, and 300 IU vitamin A/g salt. Vitamin A deficiency prevalence reduced by 23.5% |
| Vinodkumar et al., 2009 [36] Develop a salt fortified with multiple micronutrients, test its stability, and assess its efficacy in improving the micronutrient status of schoolchildren India 1 y pre- and post-test design with experimental and control groups 245 children (5–15 y) | Multiple micronutrient fortified salt (microencapsulated vitamins A, B1, B2, B6, B12, folic acid, niacin, calcium pantothenate, and iodine) Chelated FS 1 mg Fe/g salt | Hb (+0.55 * g/dL) Anemia prevalence (−4.3%, significance NA) Ferritin NA | NA | Albendazole 400 mg at baseline, after 6 mo and after 1 y of intervention | NA | Continuous use in daily cooking was monitored. NA adherence | Salt contained 5 μg folic acid/g salt, 0.4 μg vitamin B12/g salt, and 300 IU vitamin A/g salt. There was a 5.6 μg/dL increase in serum vitamin A. |
| Vinodkumar et al., 2009 [37] Test efficacy of multiple micronutrient fortified salt on children India 9 mo RCT 402 children (5–18 y) | Multiple micronutrient fortified salt (vitamins A, B1, B2, B6, B12, folic acid, niacin, iron, iodine, and zinc) Chelated FS 1 mg Fe/g salt | Hb (+0.67 * g/dL) Anemia prevalence (−40% *) Ferritin (-0.12 μg/L) | NA | Albendazole (400 mg) at baseline, 4 mo, and post-trial at 9 mo | The cooking staff confirmed that the fortified salt did not change the color or taste of any food | Weighed salt leftover from the previous month to verify compliance. No food was left on the plates. | Salt contained 10 μg folic acid/g salt, 0.4 mcg vitamin B12/g salt, and 300 IU vitamin A/g salt. There was a significant 4.7 μg/dL increase in serum vitamin A and 10,129 pg/mL increase in serum B12. Serum folic acid significantly decreased by −6.28 ng/mL. |
| Zimmermann et al., 2004 [38] Develop a stable, efficacious salt fortified with iodine, iron, and vitamin A Morocco 10 mo double-blind, RCT 157 children (6–14 y) | Triple fortified salt (iron, vitamin A, iodine) Micronized FePP at 2 mg Fe/g salt | Hb (+1.5 * g/dL) Anemia prevalence (−26% *) Ferritin (+16.0 * μg/L) | NA | NA | Triangle test showed no significant difference in color, odor, or taste (or all three) between the fortified salts in any of the traditional foods. However, 32% noted a color change in one or more foods when the salt was added. This did not affect the overall acceptability | NA | Salt contained 60 μg vitamin A/g salt. Vitamin A deficiency decreased by 8%. |
| Winichagoon et al., 2006 [39] Assess the efficacy of a micronutrient-fortified seasoning powder served with a school lunch on reducing anemia and improving the micronutrient status of children Thailand 31 wk RCT 569 children (5.5–13.4 y) | Seasoning powder (zinc, iron, vitamin A, and iodine) H-reduced elemental iron encapsulated with partially hydrogenated vegetable oil 5 mg Fe/pouch | Hb (+0.31 g/dL) Anemia prevalence NA Ferritin (−11.5 μg/L) | NA | NA | NA | Teachers recorded whether the child ate “all,” “more than half,” “half,” “less than half,” or “none” of the school lunch. Adherence NA | The seasoning packet contained 270 μg of vitamin A. Fortification had no effect on serum retinol. |
| Longfils et al., 2008 [40] To assess the efficacy and safety of fortified fish sauce, added to daily school meals either as NaFeEDTA or as FeSO4+ citrate Cambodia 21 wk double-blinded, placebo controlled RCT 140 iron-deficiency anemic children (6–21 y) | Fish sauce NaFeEDTA or FeSO4+ citrate 1 mg Fe/mL | Hb (+0.29 * g/dL and +0.31 * g/dL, FeSO4+ citrate and NaFeEDTA) Anemia prevalence NA Ferritin (+13.5 * and +17.3 * μg/L) | NA | 500 mg Mebendazole at the beginning, in the middle, and at the end of the study in addition to doses provided by the National Health Program | The taste of the school meals, corresponding to an average Cambodian fare, remained unaffected after the addition of either variety | Field workers fully supervised the ingestion of the meals. Food that was not consumed was re-weighed and recorded. All meals were fully consumed with no left-over. | NA |
| Van Thuy et al., 2005 [41] Evaluate the effectiveness of fortified fish sauce with for improving iron status in WRA Vietnam 18 mo double-blind, intervention with randomization by village 576 WRA | Fish sauce NaFeEDTA 9 mmol Fe/L | Hb (+0.54 * g/dL) Anemia prevalence (−16.2% *) Ferritin (+36.3 * μg/L) | NA | NA | The fortified fish sauce was well accepted by the target population over an 18 mo period | Compliance monitoring NA Mean consumption for all individuals in all villages was 18 mL/(person x d) | <8.0% of the women had vitamin A deficiency. |
| Chen et al., 2005 [42] Study the effectiveness of NaFeEDTA-fortified soy sauce for controlling iron deficiency in a high-risk population China 18 mo RCT 14,000 residents (3+ y) | Soy sauce NaFeEDTA 29.6 mg Fe/100 mL | Hb (M3 − 6 y +0.69 *, M7 − 18 y + 1.0 *, M19 − 54 y + 0.98 *, M55 + y + 0.88 *, W3 − 6 y + 0.75 *, W7-18 y + 1.0 *, W19 − 30 y + 1.2 *, W31-54 y + 1.56 *, W55 + y + 0.72 * g/dL) Anemia prevalence (M3-6 y − 31.9% *, M7-18 y − 36.3% *, M19-54 y -25.6% *, M55 + y − 37.8% *, W3-6 y − 26.1% *, W7 – 18 y − 40.6% *, W19 – 30 y − 44.9% *, W31 – 54 y − 42.8% *, W55 + y − 34.9% *) Ferritin (M7 − 18 y + 1.87 *, M19 − 54 y + 6.79 *, M55 + y + 2.91 *, F7 − 18 y + 1.74 *, F19 − 30 y + 1.34 *, F31 − 54 y + 1.86 *, F55 + y +3.43 * μg/L) | NA | NA | A survey of the organoleptic qualities and acceptance of the fortified/unfortified soy sauce was conducted in 187 households. Both products were considered to be of high quality and no complaints of adverse effects. The two were reported to taste the same | Food frequency questionnaires at baseline, 6, 12, and 18 mo. During the trial period, the mean soy sauce consumption increased from 14.3 to 16.4 mL/person/day in the fortified group and from 14.1 to 15.8 mL/person/day in the control group. | There were no significant differences in plasma retinol levels between the fortified and control groups. There may be a high prevalence of subclinical vitamin A deficiency in these villages. Folate and B12 deficiencies should be considered in future studies. |
| Huo et al., 2002 [43] Study the therapeutic effects of NaFeEDTA-fortified soy sauce on anemic students at two concentration levels China 3 mo RCT 304 iron-deficiency anemic children (11–17 y) | Soy sauce NaFeEDTA Low = 1 mg Fe/mL High = 4 mg Fe/mL | Hb (+2.03 * and +2.39 * g/dL, low and high Fe levels) Anemia prevalence NA Ferritin (+17.19 * and +15.65 * μg/L, low and high Fe levels) | NA | NA | NA | The soup was consumed under complete supervision from the teachers. At the same time, detailed information on the soy sauce consumption of each subject was recorded on a consumption sheet. Adherence NA. | NA |
| Outcome | Children (16 Studies) 1 | Women (Eight Studies) 2 | Whole Population (One Study) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| YES | NO | NA | YES | NO | NA | YES | NO | NA | |
| Increased hemoglobin | 13 | 3 | 0 | 6 | 1 | 1 | 1 | 0 | 0 |
| Decreased anemia | 10 | 2 | 4 | 4 | 3 | 1 | 0 | 0 | 1 |
| Increased Ferritin | 9 | 2 * | 5 | 4 | 0 | 4 | 0 | 0 | 1 |
| Category from Table 2 | Study/Objective/Country/Duration and Experimental Design/Subjects | Condiment/ Fe Source/Concentration | Iron Intervention Outcomes (Hemoglobin, Anemia Prevalence, and Ferritin) | Suggested Possible Causes (Low-Performing Factors) |
|---|---|---|---|---|
| Did not increase hemoglobin significantly (children) | Kumar et al., 2014 [35] Establish the efficacy of multi-micronutrient fortified salt in addressing multiple micronutrient deficiencies among children compared to nutrition education and no intervention. India 8 mo RCT 528 children (5–15 y) | Multiple micronutrient fortified salt (iron, iodine, vitamin A, vitamin B12, and folic acid) Chelated FS 1 mg Fe/g salt | Hb (+0.5 g/dL, NS) Anemia prevalence (−13.4% *) Ferritin (+10.8 * μg/L) | Insignificant hemoglobin increase was not addressed by authors |
| Did not increase hemoglobin significantly (children) Did not decrease anemia significantly (children) | Wegmueller et al., 2006 [30] Test efficacy of DFS Cote d’Ivoire 6 mo, double-blind efficacy trial 123 iron-deficient children (5–15 y) | DFS Micronized ground FePP 3 mg Fe/g salt | No change in Hb (0 g/dL) Anemia prevalence (+5%, NS) Ferritin increased (+15 * μg/L) | High prevalence of malaria (55%) and multiple micronutrient deficiencies (B2 deficiency 66%). Up to 52% of households reported darkening of food |
| Did not increase hemoglobin significantly (children) Did not increase ferritin significantly (children) | Winichagoon et al., 2006 [39] Assess the efficacy of a micronutrient-fortified seasoning powder served with a school lunch on reducing anemia and improving the micronutrient status of children Thailand 31 wk RCT 569 children (5.5–13.4 y) | Seasoning powder (zinc, iron, vitamin A, and iodine) H-reduced elemental iron encapsulated with partially hydrogenated vegetable oil 5 mg Fe/pouch | No significant change in Hb (+0.31 g/dL, NS) Anemia prevalence NA No significant change in Ferritin (−11.5 μg/L, NS) | Insufficient content (5 mg/serving) and form of iron used in the intervention (Reduced elemental Fe) |
| Did not increase hemoglobin significantly (women) | Nair et al., 2014 [25] Test efficacy of DFS with nutrition education on pregnant, anemic mothers India 2 mo RCT 135 pregnant, anemic women | DFS Fe source NA 1 mg Fe/g salt | Hb change before and after intervention: −0.15 g/dL (NS) Anemia prevalence NA Ferritin NA | Not enough Fe intake to meet pregnancy needs during only 2 mo of intervention |
| Did not decrease anemia significantly (children) | Reddy et al., 2014 [27] To assess the impact of DFS on iron and iodine status of schoolchildren. India 9 mo longitudinal intervention study 947 schoolchildren (6–15 y) | DFS Source NA Concentration NA | Hb (+0.6 * g/dL and 0.21 * g/dL, deworming and not) Anemia prevalence (−6.3% * and +1.5%, deworming and not) Ferritin NA | Absence of deworming |
| Did not decrease anemia significantly (women) | Asibey-Berko et al., 2007 [22] Test efficacy of DFS on anemia and iodine deficiency in women and children Ghana 8 mo RCT 300 NP, NL women (15–45 y) and 157 children (1–5 y) | DFS/ FF/ 1 mg Fe/g salt | No Hb post-treatment data Anemia prevalence: Children: −21.7% * Women: +3.3% Ferritin NA | Significant increase of anemia in the control group. Uneven baseline prevalence of anemia. Darker color of DFS. Women reported the darkening of plantains when frying |
| Did not decrease anemia significantly (women) | Haas et al., 2014 [24] Test efficacy of DFS in reducing ID in WRA India 7.5–9 mo RCT 212 NP women (18–55 y) | DFS Micro-encapsulated FF 1.1 mg Fe/g salt | Hb (+0.24 * g/dL) Anemia prevalence (+1%) Ferritin (+0.13 * log10 μg/mL), 34% increase. | High prevalence of folate and B12 deficiencies. High prevalence of elevated MCV (25%) |
| Did not decrease anemia significantly (women) | Reddy et al., 2016 [28] Assess the impact of DFS on iron and iodine status of pregnant women. India 9 mo RCT 150 pregnant women (<12 weeks gestation) | DFS Ferrous sulfate 1000 ppm at 10 g/day | Hb (+0.42 * g/dL) Anemia prevalence (−10.5%) Ferritin NA | Significance of anemia not addressed by authors |
| Did not increase ferritin significantly (children) | Vinodkumar et al., 2009, Int. J Vit Nut Res [37] Test efficacy of multiple micronutrient fortified salt on children India 9 mo RCT 402 children (5–18 y) | Multiple micronutrient fortified salt (vitamins A, B1, B2, B6, B12, folic acid, niacin, iron, iodine, and zinc) Chelated FS 1 mg Fe/g salt | Hb increased (+0.67 * g/dL) Anemia prevalence decreased (−40% *) No change in Ferritin (−0.12 μg/L) NS | Uneven prevalence of anemia and ferritin levels at baseline. Possible adverse interaction with zinc absorption |
| Study/Objective/Country/ Duration and Experimental Design/Subjects | Condiment/Fe source/Concentration | Iron Intervention Outcomes (Hemoglobin, Anemia Prevalence, and Ferritin) | Reported Possible Causes of Success | Quality Assessment Score and Effect Size |
|---|---|---|---|---|
| Andersson 2008 [21] Compare the efficacy of DFS with FePP and EFF India 10 mo RCT 458 rural children (5–15 years) | DFS Micronized ground FePP or encapsulated FF 2 mg Fe/g salt | Hb (+0.6 * and +0.8 * g/dL, FePP and FF) Anemia prevalence (−9.1% * and −10.1% *, FePP and FF) Ferritin (+6.4 * and +4.9 * μg/L, FePP and FF) | Reiteration of health effects and instructions at each salt distribution Parasitic treatment Assessed sensory Compliance monitored Vitamin A supplements | Strong quality assessment 0.24 and 0.23 effect sizes, encapsulated FF and micronized FePP, respectively |
| Wenger 2017 [31] To assess the extent to which increases in dietary iron consumption are related to improvements in behavioral measures of perceptual, attentional, and mnemonic function. India 10 mo RCT 126 NP women (18–55 y) | DFS Micro-encapsulated FF 1.1 mg Fe/g salt | Hb (+0.1 * g/dL) Anemia prevalence (−5% *) Ferritin (+12.5 * μg/L) | Parasitic treatment Assessed sensory Assessed folate and vitamin B12 deficiencies | Strong quality assessment 0.13 effect size |
| Zimmermann 2003 [32] To test DFS efficacy. Morocco 9 mo double-blind, RCT 377 iodine-deficient children (6–15 y) | DFS FS hydrate encapsulated with partially hydrogenated vegetable oil 1 mg Fe/g salt | Hb (+1.4 * g/dL) Anemia prevalence (−25% *) Ferritin (+20 * μg/L) | Assessed acceptability and sensory | Strong quality assessment 0.91 effect size |
| Zimmermann 2004 [33] To test the efficacy of DFS for reducing the prevalence of iodine and iron deficiencies in children. Morocco 10 mo double-blind, RCT 158 children (6–15 y) | DFS Micronized FePP 2 mg Fe/g salt | Hb (+1.5 * g/dL) Anemia prevalence (−25% *) Ferritin (+17.6 * μg/L) | Assessed acceptability and sensory | Strong quality assessment 1.36 effect size |
| Van Thuy 2005 [41] To evaluate the effectiveness of fortified fish sauce with for improving iron status in WRA. Vietnam 18 mo double-blind, intervention with randomization by village 576 WRA | Fish sauce NaFeEDTA 9mmol Fe/L | Hb (+0.54 * g/dL) Anemia prevalence (−16.2% *) Ferritin (+36.3 * μg/L) | Assessed acceptability Assessed adherence Assessed vitamin A deficiency prevalence | Strong quality assessment 0.46 effect size |
| Chen 2005 [42] To study the effectiveness of NaFeEDTA-fortified soy sauce for controlling iron deficiency in a high-risk population. China 18 mo RCT 14,000 residents (3 + y) | Soy sauce NaFeEDTA 29.6 mg Fe/100mL | Hb (M3 − 6 y + 0.69 *, M7 − 18 y + 1.0 *, M19 − 54 y + 0.98 *, M55 + y + 0.88 *, W3-6 y + 0.75 *, W7 − 18 y + 1.0 *, W19 − 30 y + 1.2 *, W31 − 54 y + 1.56 *, W55 + y + 0.72 * g/dL) Anemia prevalence (M3 − 6 y − 31.9% *, M7 − 18 y − 36.3% *, M19 − 54 y − 25.6% *, M55 + y − 37.8% *, W3 − 6 y − 26.1% *, W7 − 18 y − 40.6% *, W19 − 30 y − 44.9% *, W31 − 54 y − 42.8% *, W55 + y − 34.9% *) Ferritin (M7 − 18 y +1.87 *, M19 − 54 y + 6.79 *, M55 + y + 2.91 *, F7 − 18 y + 1.74 *, F19 − 30 y + 1.34 *, F31 − 54 y + 1.86 *, F55 + y + 3.43 * μg/L) | Assessed sensory and acceptability Monitored compliance and adherence Assessed plasma retinol levels | Strong quality assessment F19 − 30 y 0.06, F31 − 54 y 0.50, F3 − 6 y 0.40, F55 + y 0.34, F7 − 18 y 0.34, M19 − 54 y 0.51, M3 − 6 y 0.51, M55 + y 0.41, M7 − 18 y 0.26 |
| Kumar 2014 [35] To establish the efficacy of multi-micronutrient fortified salt in addressing multiple micronutrient deficiencies among children compared to nutrition education and no intervention. India 8 mo RCT 528 children (5–15 y) | Multiple micronutrient fortified salt (iron, iodine, vitamin A, vitamin B12, and folic acid) Chelated FS 1 mg Fe/g salt | Hb (+0.5 g/dL) Anemia prevalence (−13.4% *) Ferritin (+10.8 * μg/L) | Education component Parasitic treatment Monitored compliance and adherence Vitamin A deficiency prevalence reduced | Strong quality assessment 0.40 effect size |
| Zimmermann 2004 [38] To develop a stable, efficacious salt fortified with iodine, iron, and vitamin A. Morocco 10 mo double-blind, RCT 157 children (6-14 y) | Triple fortified salt (iron, vitamin A, iodine) Micronized FePP at 2 mg Fe/g salt | Hb (+1.5 * g/dL) Anemia prevalence (−26% *) Ferritin (+16.0 * μg/L) | Assessed sensory and acceptability Vitamin A deficiency prevalence reduced | Strong quality assessment 1.55 effect size |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waller, A.W.; Andrade, J.E.; Mejia, L.A. Performance Factors Influencing Efficacy and Effectiveness of Iron Fortification Programs of Condiments for Improving Anemia Prevalence and Iron Status in Populations: A Systematic Review. Nutrients 2020, 12, 275. https://doi.org/10.3390/nu12020275
Waller AW, Andrade JE, Mejia LA. Performance Factors Influencing Efficacy and Effectiveness of Iron Fortification Programs of Condiments for Improving Anemia Prevalence and Iron Status in Populations: A Systematic Review. Nutrients. 2020; 12(2):275. https://doi.org/10.3390/nu12020275
Chicago/Turabian StyleWaller, Anna W., Juan E. Andrade, and Luis A. Mejia. 2020. "Performance Factors Influencing Efficacy and Effectiveness of Iron Fortification Programs of Condiments for Improving Anemia Prevalence and Iron Status in Populations: A Systematic Review" Nutrients 12, no. 2: 275. https://doi.org/10.3390/nu12020275
APA StyleWaller, A. W., Andrade, J. E., & Mejia, L. A. (2020). Performance Factors Influencing Efficacy and Effectiveness of Iron Fortification Programs of Condiments for Improving Anemia Prevalence and Iron Status in Populations: A Systematic Review. Nutrients, 12(2), 275. https://doi.org/10.3390/nu12020275