Plasma Branched-Chain and Aromatic Amino Acids in Relation to Hypertension

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Issues
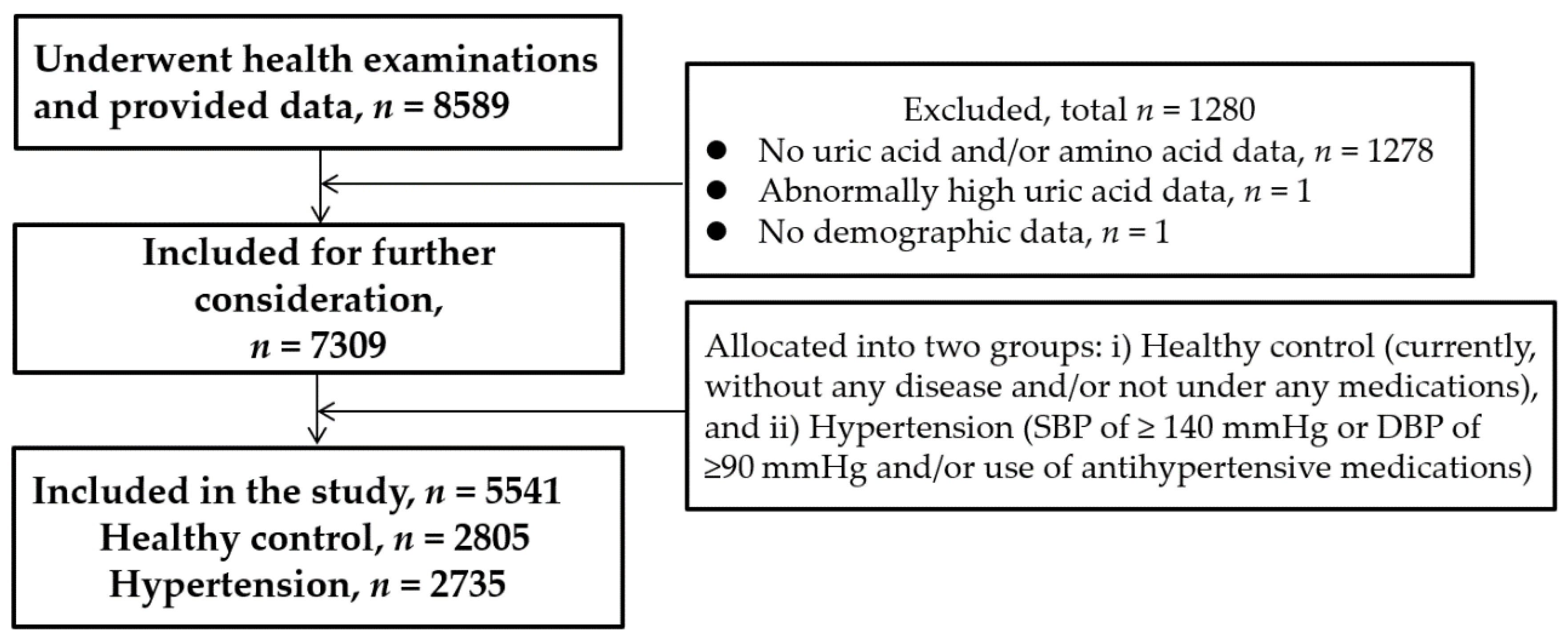
2.2. Study Population
2.3. Blood Sample Collection
2.4. Measurements of Clinical and Laboratory Variables
2.5. Statistical Analyses
3. Results
3.1. Demographic and Clinical Characteristics of Study Subjects
3.2. Differences in the Concentrations of BCAAs and AAAs between Healthy and Hypertensive Subjects
3.3. Correlation between BCAAs and AAAs
3.4. Association of BCAAs and AAAs with Hypertension
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; Amann, M.; Anderson, H.R.; Andrews, K.G.; Aryee, M.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [Green Version]
- Mills, K.T.; Bundy, J.D.; Kelly, T.N.; Reed, J.E.; Kearney, P.M.; Reynolds, K.; Chen, J.; He, J. Global Disparities of Hypertension Prevalence and Control: A Systematic Analysis of Population-Based Studies from 90 Countries. Circulation 2016, 134, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Buford, T.W. Hypertension and Aging. Ageing Res. Rev. 2016, 26, 96–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roth, E.; Druml, W. Plasma amino acid imbalance: Dangerous in chronic diseases? Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; Fauman, E.; Erte, I.; Perry, J.R.; Kastenmüller, G.; Shin, S.Y.; Petersen, A.K.; Hyde, C.; Psatha, M.; Ward, K.J.; et al. Biomarkers for type 2 diabetes and impaired fasting glucose using a nontargeted metabolomics approach. Diabetes 2013, 62, 4270–4276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yatabe, J.; Yatabe, M.S.; Ishibashi, K.; Nozawa, Y.; Sanada, H. Early detection of colon cancer by amino acid profiling using AminoIndex Technology: A case report. Diagn. Pathol. 2013, 8, 203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, C.N.; Tain, Y.L. Amino Acids and Developmental Origins of Hypertension. Nutrients 2020, 12, 1763. [Google Scholar] [CrossRef]
- Poggiogalle, E.; Fontana, M.; Giusti, A.M.; Pinto, A.; Iannucci, G.; Lenzi, A.; Donini, L.M. Amino Acids and Hypertension in Adults. Nutrients 2019, 11, 1459. [Google Scholar] [CrossRef] [Green Version]
- Flores-Guerrero, J.L.; Groothof, D.; Connelly, M.A.; Otvos, J.D.; Bakker, S.; Dullaart, R. Concentration of Branched-Chain Amino Acids Is a Strong Risk Marker for Incident Hypertension. Hypertension 2019, 74, 1428–1435. [Google Scholar] [CrossRef]
- Hu, W.; Sun, L.; Gong, Y.; Zhou, Y.; Yang, P.; Ye, Z.; Fu, J.; Huang, A.; Fu, Z.; Yu, W.; et al. Relationship between Branched-Chain Amino Acids, Metabolic Syndrome, and Cardiovascular Risk Profile in a Chinese Population: A Cross-Sectional Study. Int. J. Endocrinol. 2016, 8173905. [Google Scholar] [CrossRef] [Green Version]
- Perng, W.; Rifas-Shiman, S.L.; Hivert, M.F.; Chavarro, J.E.; Oken, E. Branched Chain Amino Acids, Androgen Hormones, and Metabolic Risk Across Early Adolescence: A Prospective Study in Project Viva. Obesity 2018, 26, 916–926. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Dong, J.; Zhao, H.; Li, H.; Guo, H.; Wang, S.; Zhang, C.; Wang, S.; Wang, M.; Yu, S.; et al. Association of branched-chain amino acids with carotid intima-media thickness and coronary artery disease risk factors. PLoS ONE 2014, 9, e99598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahbub, M.H.; Yamaguchi, N.; Takahashi, H.; Hase, R.; Ishimaru, Y.; Sunagawa, H.; Amano, H.; Kobayashi-Miura, M.; Kanda, H.; Fujita, Y.; et al. Association of plasma free amino acids with hyperuricemia in relation to diabetes mellitus, dyslipidemia, hypertension and metabolic syndrome. Sci. Rep. 2017, 7, 17616. [Google Scholar] [CrossRef] [PubMed]
- Mahbub, M.H.; Yamaguchi, N.; Takahashi, H.; Hase, R.; Yamamoto, H.; Kikuchi, S.; Tanabe, T. Relationship of reduced glomerular filtration rate with alterations in plasma free amino acids and uric acid evaluated in healthy control and hypertensive subjects. Sci. Rep. 2019, 9, 10252. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J. Hyperten. 2018, 36, 1953–2041. [Google Scholar] [CrossRef] [Green Version]
- Muntner, P.; Shimbo, D.; Carey, R.M.; Charleston, J.B.; Gaillard, T.; Misra, S.; Myers, M.G.; Ogedegbe, G.; Schwartz, J.E.; Townsend, R.R.; et al. Measurement of Blood Pressure in Humans: A Scientific Statement From the American Heart Association. Hypertension 2019, 73, e35–e66. [Google Scholar] [CrossRef]
- Shimbo, K.; Oonuki, T.; Yahashi, A.; Hirayama, K.; Miyano, H. Precolumn derivatization reagents for high-speed analysis of amines and amino acids in biological fluid using liquid chromatography/electrospray ionization tandem mass spectrometry. Rapid Commun. Mass Spectrom. 2009, 23, 1483–1492. [Google Scholar] [CrossRef]
- Shimbo, K.; Yahashi, A.; Hirayama, K.; Nakazawa, M.; Miyano, H. Multifunctional and Highly Sensitive Precolumn Reagents for Amino Acids in Liquid Chromatography/Tandem Mass Spectrometry. Anal. Chem 2009, 81, 5172–5179. [Google Scholar] [CrossRef]
- Faresjö, T.; Faresjö, A. To match or not to match in epidemiological studies—Same outcome but less power. Int. J. Environ. Res. Public Health 2010, 7, 325–332. [Google Scholar] [CrossRef] [Green Version]
- Yamakado, M.; Nagao, K.; Imaizumi, A.; Tani, M.; Toda, A.; Tanaka, T.; Jinzu, H.; Miyano, H.; Yamamoto, H.; Daimon, T.; et al. Plasma Free Amino Acid Profiles Predict Four-Year Risk of Developing Diabetes, Metabolic Syndrome, Dyslipidemia, and Hypertension in Japanese Population. Sci. Rep. 2015, 5, 11918. [Google Scholar] [CrossRef]
- Hundal, H.S.; Taylor, P.M. Amino acid transceptors: Gate keepers of nutrient exchange and regulators of nutrient signaling. Am. J. Physiol. Endocrinol. Metab. 2009, 296, E603–E613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lynch, C.J.; Adams, S.H. Branched-chain amino acids in metabolic signalling and insulin resistance. Nat. Rev. Endocrinol. 2014, 10, 723–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, G. Amino acids: Metabolism, functions, and nutrition. Amino Acids 2009, 37, 1–17. [Google Scholar] [CrossRef]
- Gelber, R.P.; Gaziano, J.M.; Manson, J.E.; Buring, J.E.; Sesso, H.D. A prospective study of body mass index and the risk of developing hypertension in men. Am. J. Hypertens. 2007, 20, 370–377. [Google Scholar] [CrossRef] [Green Version]
- Lindholm, L. Hypertension and ageing. Clin. Exp. Hypertens. A 1990, 12, 745–759. [Google Scholar] [CrossRef]
- Mazzali, M.; Kanbay, M.; Segal, M.S.; Shafiu, M.; Jalal, D.; Feig, D.I.; Johnson, R.J. Uric acid and hypertension: Cause or effect. Curr. Rheumatol. Rep. 2010, 12, 108–117. [Google Scholar] [CrossRef]
- Martin, M.; Deussen, A. Effects of natural peptides from food proteins on angiotensin converting enzyme activity and hypertension. Crit. Rev. Food Sci. Nutr. 2019, 59, 1264–1283. [Google Scholar] [CrossRef]
- Siomkajło, M.; Rybka, J.; Mierzchała-Pasierb, M.; Gamian, A.; Stankiewicz-Olczyk, J.; Bolanowski, M.; Daroszewski, J. Specific plasma amino acid disturbances associated with metabolic syndrome. Endocrine 2017, 58, 553–562. [Google Scholar] [CrossRef]
- Zhang, Z.Y.; Monleon, D.; Verhamme, P.; Staessen, J.A. Branched-Chain Amino Acids as Critical Switches in Health and Disease. Hypertension 2018, 72, 1012–1022. [Google Scholar] [CrossRef]
- Yang, Y.; Wu, Z.; Meininger, C.J.; Wu, G. L-Leucine and NO-mediated cardiovascular function. Amino Acids 2015, 47, 435–447. [Google Scholar] [CrossRef]
- Yudkoff, M. Interactions in the Metabolism of Glutamate and the Branched-Chain Amino Acids and Ketoacids in the CNS. Neurochem. Res. 2017, 42, 10–18. [Google Scholar] [CrossRef] [Green Version]
- Holmes, E.; Loo, R.L.; Stamler, J.; Bictash, M.; Yap, I.K.; Chan, Q.; Ebbels, T.; De Iorio, M.; Brown, I.J.; Veselkov, K.A.; et al. Human metabolic phenotype diversity and its association with diet and blood pressure. Nature 2008, 453, 396–400. [Google Scholar] [CrossRef]
- Lu, J.; Xie, G.; Jia, W.; Jia, W. Insulin resistance and the metabolism of branched-chain amino acids. Front. Med. 2013, 7, 53–59. [Google Scholar] [CrossRef]
- Saad, M.F.; Rewers, M.; Selby, J.; Howard, G.; Jinagouda, S.; Fahmi, S.; Zaccaro, D.; Bergman, R.N.; Savage, P.J.; Haffner, S.M. Insulin resistance and hypertension: The Insulin Resistance Atherosclerosis study. Hypertension 2004, 43, 1324–1331. [Google Scholar] [CrossRef] [Green Version]
- Soleimani, M. Insulin resistance and hypertension: New insights. Kidney Int. 2015, 87, 497–499. [Google Scholar] [CrossRef] [Green Version]
- Fernstrom, J.D. Branched-chain amino acids and brain function. J. Nutr. 2005, 135, 1539S–1546S. [Google Scholar] [CrossRef]
- Shah, S.H.; Crosslin, D.R.; Haynes, C.S.; Nelson, S.; Turer, C.B.; Stevens, R.D.; Muehlbauer, M.J.; Wenner, B.R.; Bain, J.R.; Laferrère, B.; et al. Branched-chain amino acid levels are associated with improvement in insulin resistance with weight loss. Diabetologia 2012, 55, 321–330. [Google Scholar] [CrossRef] [Green Version]
- Tang, J.P.; Xu, Z.Q.; Douglas, F.L.; Rakhit, A.; Melethil, S. Increased blood-brain barrier permeability of amino acids in chronic hypertension. Life Sci. 1993, 53, PL417–PL420. [Google Scholar] [CrossRef]
- Watts, S.W.; Morrison, S.F.; Davis, R.P.; Barman, S.M. Serotonin and blood pressure regulation. Pharm. Rev. 2012, 64, 359–388. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | Healthy | Hypertension | p-Value | ||
|---|---|---|---|---|---|
| (n = 2805) | (n = 2736) | ||||
| Median or n | IQR or % | Median or n | IQR or % | ||
| Age (years) | 43 | 25 | 64 | 18 | <0.001 |
| Sex | <0.001 | ||||
| Male | 1192 | 42.5 | 1473 | 53.8 | |
| Female | 1613 | 57.5 | 1263 | 46.2 | |
| BMI (kg/m2) | 21.3 | 3.7 | 23.6 | 4.2 | <0.001 |
| SBP (mmHg) | 118 | 15 | 140 | 17 | <0.001 |
| DBP (mmHg) | 73 | 13 | 86 | 15 | <0.001 |
| FPG (mg/dL) | 91 | 10 | 98 | 14 | <0.001 |
| UA (mg/dL) | 4.6 | 1.9 | 5.3 | 2 | <0.001 |
| Amino Acids | Healthy | Hypertension | p-Value | ||
|---|---|---|---|---|---|
| (n = 2805) | (n = 2736) | ||||
| Median | IQR | Median | IQR | ||
| Ile | 51.5 | 16.0 | 57.4 | 18.7 | <0.001 |
| Leu | 102.6 | 29.3 | 112.7 | 33.3 | <0.001 |
| Val | 190.8 | 51.0 | 211.8 | 54.8 | <0.001 |
| Phe | 53.7 | 10.2 | 58.9 | 10.8 | <0.001 |
| Tyr | 57.2 | 14.8 | 65.4 | 17.0 | <0.001 |
| Trp | 51.2 | 11.9 | 53.7 | 12.0 | <0.001 |
| Healthy: AAAs | Hypertension: AAAs | |||||
|---|---|---|---|---|---|---|
| BCAAs | Phe | Tyr | Trp | Phe | Tyr | Trp |
| Ile | 0.48 * | 0.42 * | 0.52 * | 0.48 * | 0.45 * | 0.49 * |
| Leu | 0.58 * | 0.47 * | 0.56 * | 0.53 * | 0.46 * | 0.53 * |
| Val | 0.52 * | 0.45 * | 0.55 * | 0.47 * | 0.44 * | 0.49 * |
| Amino Acids | Quartile Categories | Model 1 a | Model 2 b | Model 3 c | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | ||||||||
| Lower | Upper | p-Value | (Trend) d | Lower | Upper | p-Value | (Trend) d | Lower | Upper | p-Value | (Trend) d | |||||
| Ile | 1 | Ref | – | – | – | Ref | – | – | – | Ref | – | – | – | |||
| 2 | 1.10 | 0.93 | 1.30 | 0.257 | <0.001 | 1.01 | 0.82 | 1.23 | 0.952 | <0.001 | 1.11 | 0.62 | 2.02 | 0.721 | <0.05 | |
| 3 | 1.46 | 1.25 | 1.71 | <0.001 | 1.21 | 1.00 | 1.48 | 0.056 | 1.63 | 0.93 | 2.87 | 0.091 | ||||
| 4 | 2.43 | 2.08 | 2.82 | <0.001 | 1.65 | 1.36 | 1.99 | <0.001 | 2.30 | 1.31 | 4.04 | <0.005 | ||||
| Leu | 1 | Ref | – | – | – | Ref | – | – | – | Ref | – | – | – | |||
| 2 | 1.19 | 1.01 | 1.40 | 0.041 | <0.001 | 1.03 | 0.84 | 1.26 | 0.799 | <0.001 | 1.78 | 0.97 | 3.24 | 0.063 | <0.05 | |
| 3 | 1.34 | 1.14 | 1.57 | <0.001 | 1.14 | 0.93 | 1.39 | 0.213 | 1.48 | 0.83 | 2.62 | 0.185 | ||||
| 4 | 2.47 | 2.13 | 2.88 | <0.001 | 1.49 | 1.23 | 1.81 | <0.001 | 2.41 | 1.35 | 4.33 | <0.005 | ||||
| Val | 1 | Ref | – | – | – | Ref | – | – | – | Ref | – | – | – | |||
| 2 | 1.19 | 1.00 | 1.40 | 0.050 | <0.001 | 1.02 | 0.83 | 1.25 | 0.886 | <0.001 | 1.22 | 0.68 | 2.20 | 0.508 | <0.05 | |
| 3 | 1.47 | 1.25 | 1.73 | <0.001 | 1.11 | 0.90 | 1.36 | 0.327 | 1.50 | 0.82 | 2.74 | 0.185 | ||||
| 4 | 2.83 | 2.43 | 3.30 | <0.001 | 1.53 | 1.26 | 1.86 | <0.001 | 2.19 | 1.25 | 3.85 | <0.01 | ||||
| Phe | 1 | Ref | – | – | – | Ref | – | – | – | Ref | – | – | – | |||
| 2 | 1.55 | 1.30 | 1.85 | <0.001 | <0.001 | 0.89 | 0.72 | 1.11 | 0.310 | 0.355 | 1.34 | 0.72 | 2.49 | 0.359 | 0.654 | |
| 3 | 2.26 | 1.90 | 2.67 | <0.001 | 0.89 | 0.72 | 1.10 | 0.264 | 1.49 | 0.79 | 2.78 | 0.217 | ||||
| 4 | 4.23 | 3.59 | 4.98 | <0.001 | 1.01 | 0.82 | 1.24 | 0.966 | 1.40 | 0.75 | 2.63 | 0.291 | ||||
| Tyr | 1 | Ref | – | – | – | Ref | – | – | – | Ref | – | – | – | |||
| 2 | 1.62 | 1.35 | 1.95 | <0.001 | <0.001 | 0.99 | 0.79 | 1.24 | 0.896 | 0.026 | 1.12 | 0.56 | 2.27 | 0.747 | 0.601 | |
| 3 | 2.60 | 2.18 | 3.10 | <0.001 | 1.11 | 0.89 | 1.37 | 0.365 | 1.48 | 0.79 | 2.79 | 0.223 | ||||
| 4 | 5.22 | 4.41 | 6.18 | <0.001 | 1.27 | 1.03 | 1.57 | 0.025 | 1.37 | 0.72 | 2.62 | 0.336 | ||||
| Trp | 1 | Ref | – | – | – | Ref | – | – | – | Ref | – | – | – | |||
| 2 | 0.95 | 0.81 | 1.11 | 0.493 | <0.001 | 0.96 | 0.79 | 1.16 | 0.652 | 0.153 | 1.63 | 0.91 | 2.93 | 0.102 | 0.053 | |
| 3 | 1.15 | 0.98 | 1.33 | 0.081 | 1.10 | 0.91 | 1.33 | 0.321 | 2.10 | 1.20 | 3.70 | <0.01 | ||||
| 4 | 1.45 | 1.25 | 1.68 | <0.001 | 1.16 | 0.97 | 1.40 | 0.111 | 1.94 | 1.10 | 3.40 | <0.05 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahbub, M.H.; Yamaguchi, N.; Hase, R.; Takahashi, H.; Ishimaru, Y.; Watanabe, R.; Saito, H.; Shimokawa, J.; Yamamoto, H.; Kikuchi, S.; et al. Plasma Branched-Chain and Aromatic Amino Acids in Relation to Hypertension. Nutrients 2020, 12, 3791. https://doi.org/10.3390/nu12123791
Mahbub MH, Yamaguchi N, Hase R, Takahashi H, Ishimaru Y, Watanabe R, Saito H, Shimokawa J, Yamamoto H, Kikuchi S, et al. Plasma Branched-Chain and Aromatic Amino Acids in Relation to Hypertension. Nutrients. 2020; 12(12):3791. https://doi.org/10.3390/nu12123791
Chicago/Turabian StyleMahbub, M. H., Natsu Yamaguchi, Ryosuke Hase, Hidekazu Takahashi, Yasutaka Ishimaru, Rie Watanabe, Hiroyuki Saito, Junki Shimokawa, Hiroshi Yamamoto, Shinya Kikuchi, and et al. 2020. "Plasma Branched-Chain and Aromatic Amino Acids in Relation to Hypertension" Nutrients 12, no. 12: 3791. https://doi.org/10.3390/nu12123791
APA StyleMahbub, M. H., Yamaguchi, N., Hase, R., Takahashi, H., Ishimaru, Y., Watanabe, R., Saito, H., Shimokawa, J., Yamamoto, H., Kikuchi, S., & Tanabe, T. (2020). Plasma Branched-Chain and Aromatic Amino Acids in Relation to Hypertension. Nutrients, 12(12), 3791. https://doi.org/10.3390/nu12123791