1. Introduction
Poor diet, which leads to heart disease, certain types of cancer, and type 2 diabetes, is the leading risk factor for premature morbidity and chronic disability in the United States [
1,
2]. The health care cost of treating these chronic diseases is in excess of USD 50 billion annually [
3]. Thus, strategies to promote healthier eating are imperative.
A critical, but under-appreciated, component of a healthy diet is dietary fiber [
4]. Dietary fiber is an important nutrient that can aid in weight management, lower blood cholesterol, control blood sugar, maintain regularity, and increase lifespan [
5]. Yet currently only 5% of Americans consume the recommended daily intake of fiber (14 g/1000 kcal) [
6,
7]. Adult women are recommended to consume 25 g of fiber per day [
5], but on average consume only 15.5 g dietary fiber/day [
8]. Men are recommended to consume 38 g of fiber per day [
5], but only consume an average of 18.4 g dietary fiber/day [
8].
One way to improve dietary fiber intake is through initiatives implemented in a grocery store or supermarket environment that influence consumers to select higher-fiber products. Many food retailers in the United States and other countries already have resources in the retail environment that can facilitate healthier eating by providing nutrition information that can help consumers identify healthy food products. These resources include nutrition labeling on packaged food products, shelf labeling programs that identify the healthiness of food products (e.g., Guiding Stars in the US; Nutri-score in Europe), health and wellness information on store websites, access to educational grocery tours and registered dietitians, and in-store samples [
9].
While these strategies provide the tools to make health judgments among food products, evidence of the effectiveness of these programs suggests that alternative strategies may need to be implemented to effectively promote the purchase of healthier foods. Research that has studied the provision of nutrition information in food retail settings, such as the nutrition facts label or calorie labeling on restaurant menus, finds little to no effect on average in the general population [
10,
11,
12]. Due to the profusion of product options available [
13], consumers may limit their attention to a subset of products [
14], which may not include the healthiest options, before they begin to consider available nutrition information when making a product choice.
Many existing environmental interventions have been described as point-of-decision prompts (PDPs). PDPs are materials that are available to consumers when they are making a purchasing decision that can influence their choice and include nutrition education programs or point-of-purchase information (i.e., nutrition fact panels and shelf labels) [
15,
16,
17]. More recently, literature has begun to develop around health-focused PDPs that are strategically located to influence the consumer by making health attributes salient before the narrowing of food choices within a category has begun [
18]. This literature builds on research on PDPs in the context of promoting physical activity [
19,
20,
21]. The use of strategically placed, simple messaging in the realm of food purchases is a recent approach to promoting healthier food choices. The existing research in this area has found that health-focused point-of-decision messages improved the healthiness of consumer grocery purchases [
18,
22,
23]. A strategy that increases consumer motivation to buy healthy foods at the start of the food decision process may therefore improve the nutritional quality of food choices by influencing the set of products and the nutrition information the shopper considers. Consumers may be more likely to consider health in their shopping choices if they are presented with a health-focused PDP before they begin to determine which products they will consider within a category.
Although previous PDP studies have improved consumer food choice simply by reminding consumers about health and the importance of eating healthy foods [
23], a PDP could be designed to target important but under-consumed nutrients. Previous research on the effect of PDPs [
18,
22] and health primes [
23] on food choices in food retail settings have examined messages promoting the consumption of a broad category of food, such as “healthy foods” or “fruits and vegetables.” It is important to understand if a PDP can be used to target a specific under-consumed nutrient while also improving the general healthiness of product choices.
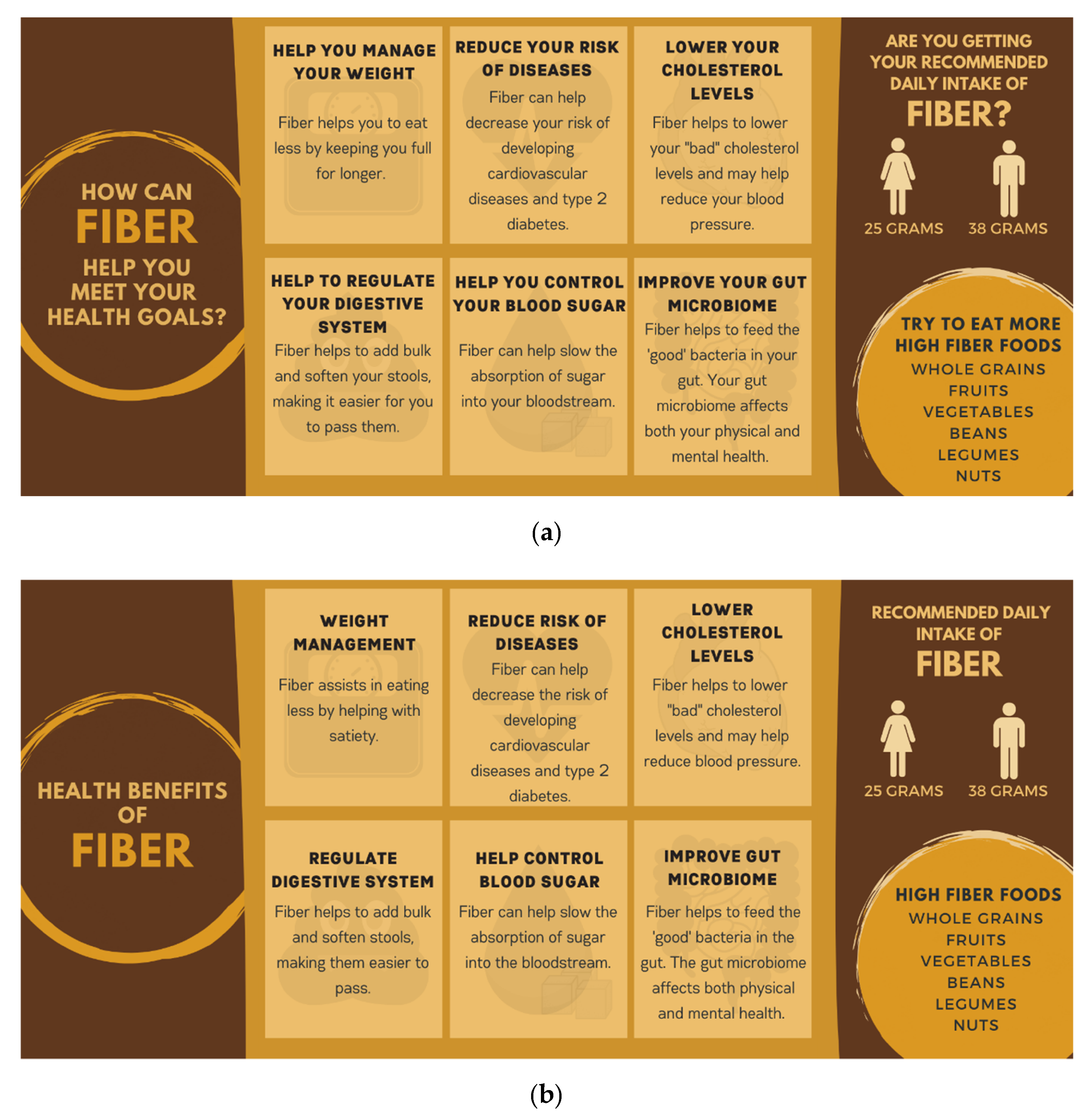
PDPs targeting key nutrients could provide simple educational messages to consumers as part of the prompt. For dietary fiber, in particular, many people are unaware of many of the health benefits of fiber [
24]. While the majority of Americans realize that fiber helps with digestion (85%) and weight management (72%), far fewer realize that fiber also helps with heart health (52%) and blood sugar control (43%) [
24]. Even fewer Americans likely realize that fiber improves the gut microbiota since this is a new benefit that members of the scientific and health communities are still working to fully document [
25]. Consumers may be more motivated to increase their fiber consumption if they understand its health benefits [
26].
In addition to the need to further study the use of PDPs in a grocery store environment, there is also a need to study its use in the online grocery shopping environment. Online grocery shopping is growing in popularity [
27], but research on the feasibility of online nutrition promotion initiatives is limited [
28]. In one poll, fewer consumers indicated looking at nutrition information when shopping for groceries online compared to a physical store [
29], suggesting that health promotion interventions may be more critical in the online environment than in physical retail outlets. A health-focused PDP could be easily implemented in an e-commerce food shopping setting to influence consumers to make healthier food selections.
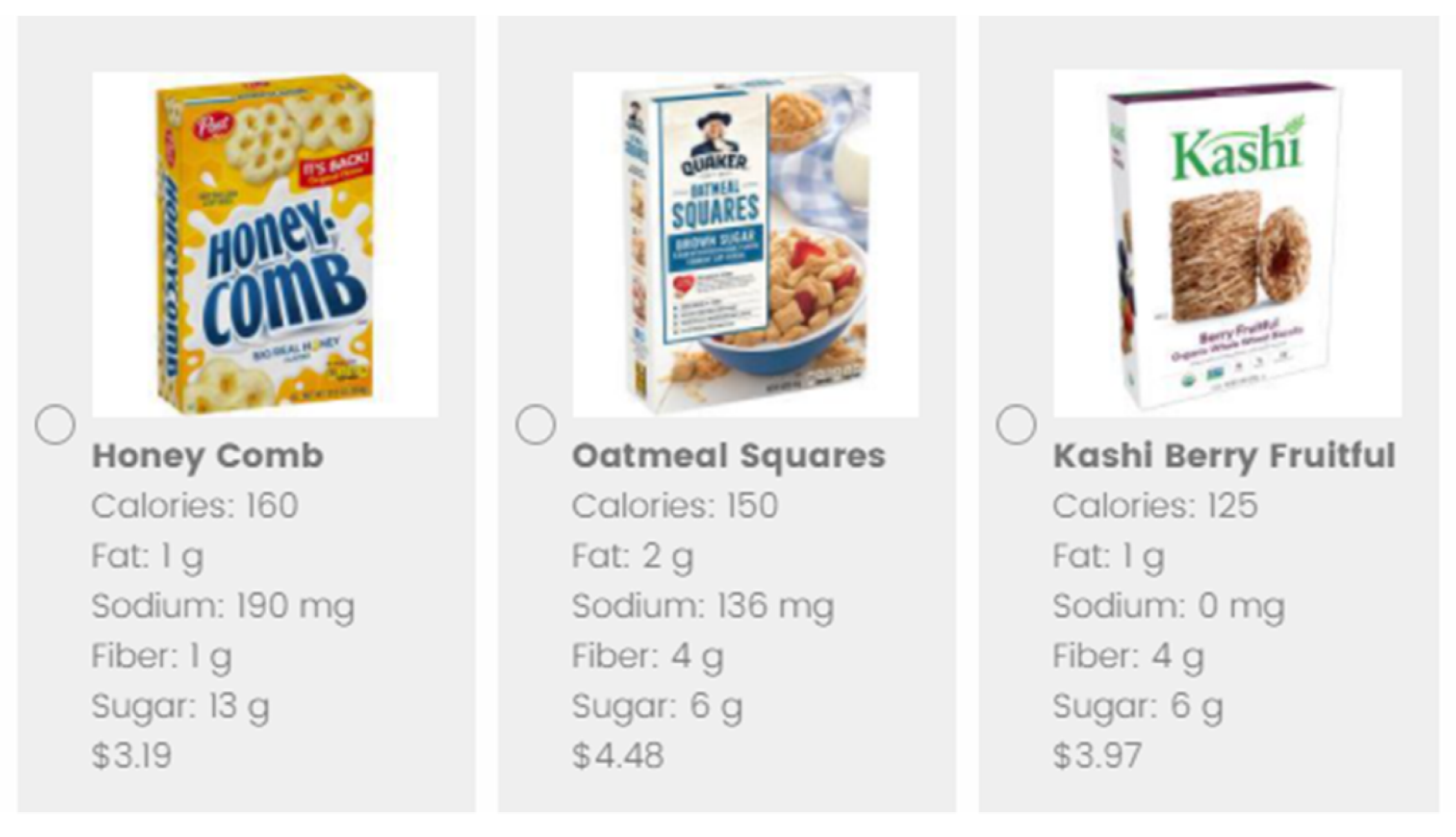
In this research, we simulate an online shopping experience to examine the effect of a PDP about the health benefits of fiber consumption on fiber content and an overall measure of healthfulness in three grain-based product categories that have significant variation in fiber levels. Our experimental design examined the influence of two slight variants of a core PDP message, compared with a no-PDP condition. The two PDPs contained the same content, but one used personal pronouns (e.g., you, your) in an effort to evoke a more personal connection to the message, while the other did not use pronouns (
Figure 1). This was done because the World Health Organization reports creating a personal relevance to an issue can help make health promotion more effective [
30]. We found no significant differences in outcomes in response to the two PDPs; therefore, in this paper, we have pooled the data from the two PDP conditions (termed pooled-PDP (P-PDP)) and compare choices in the presence of a PDP with choices made in the no-PDP condition. We hypothesized that participants who were presented with the dietary fiber PDP at the start of the food choice process would choose products with greater fiber content—and healthier products overall—than participants who were not presented with the PDP.
4. Discussion
Our research corroborates earlier findings that PDPs increase the nutritional quality of food choices [
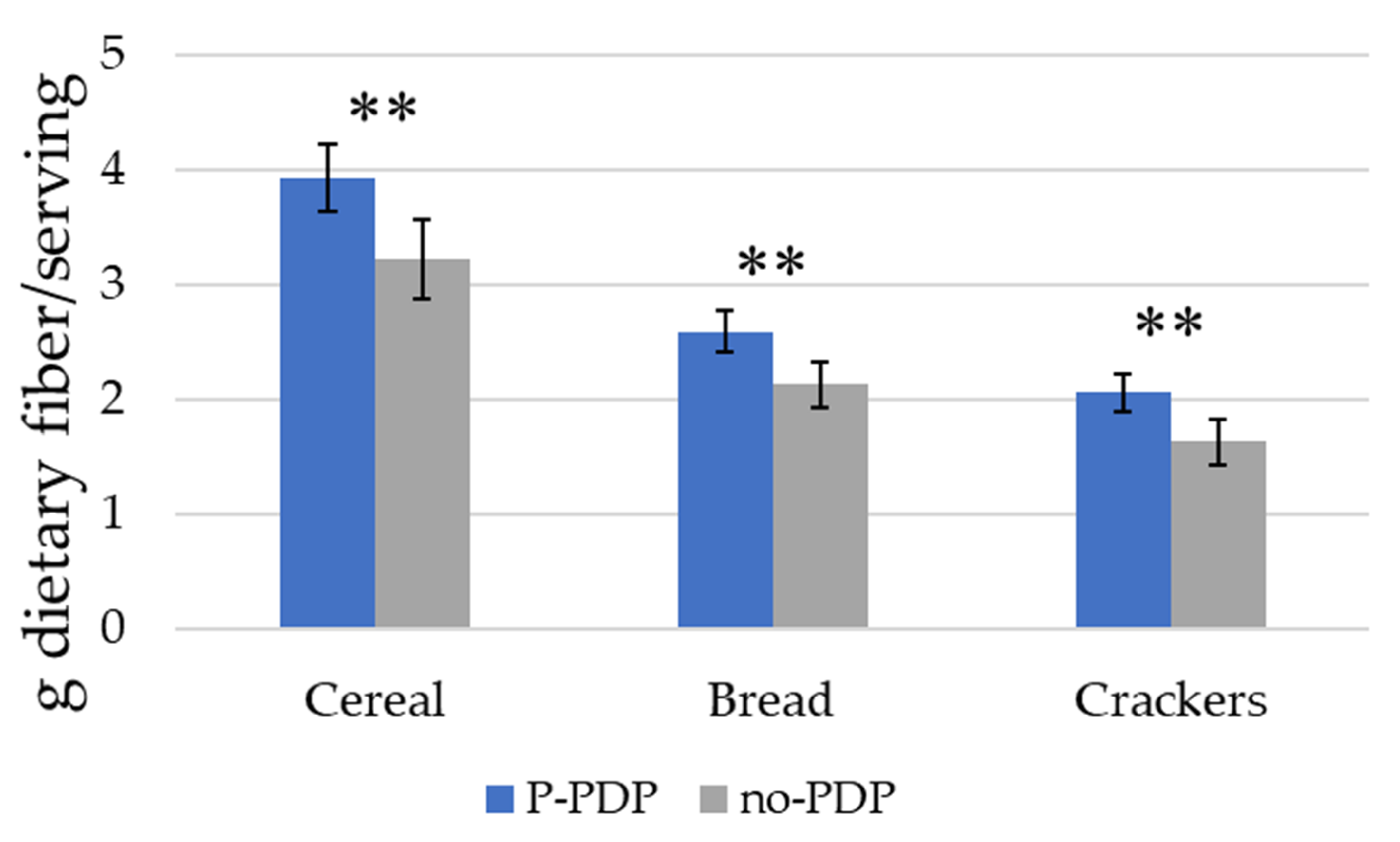
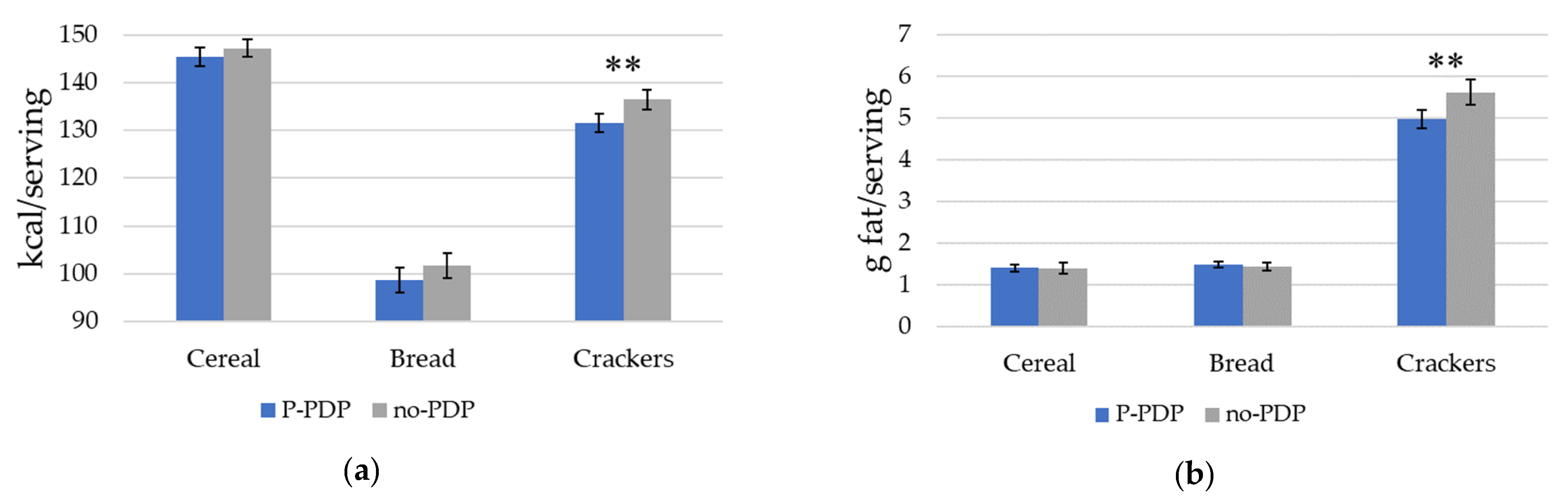
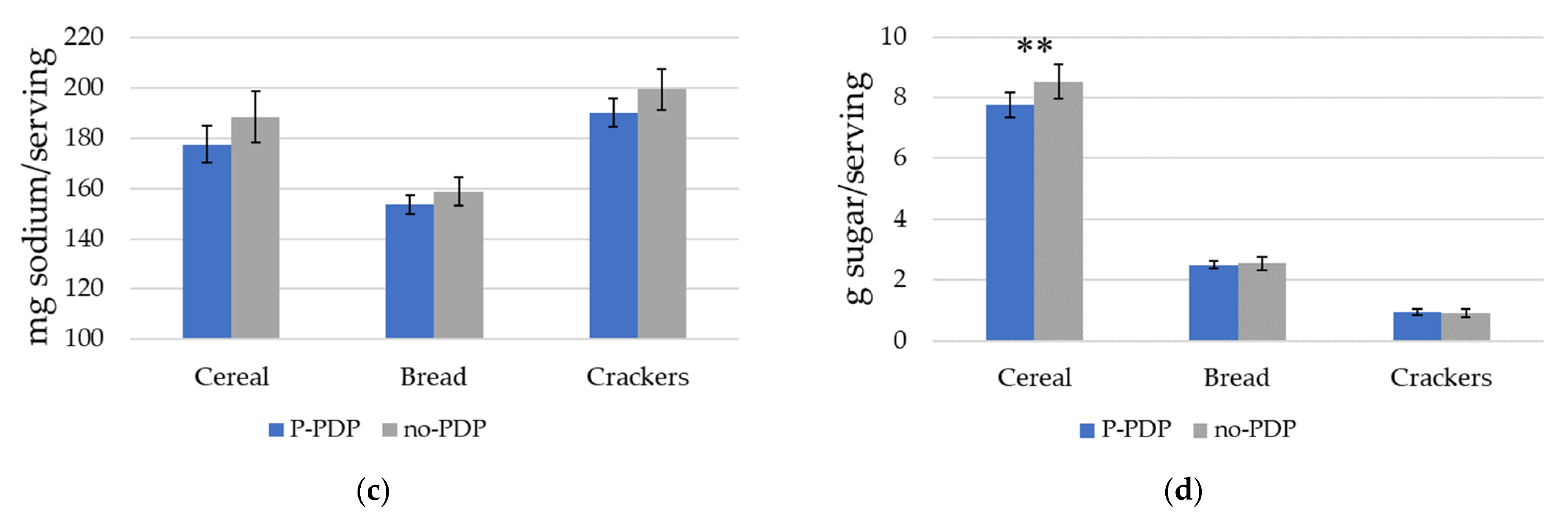
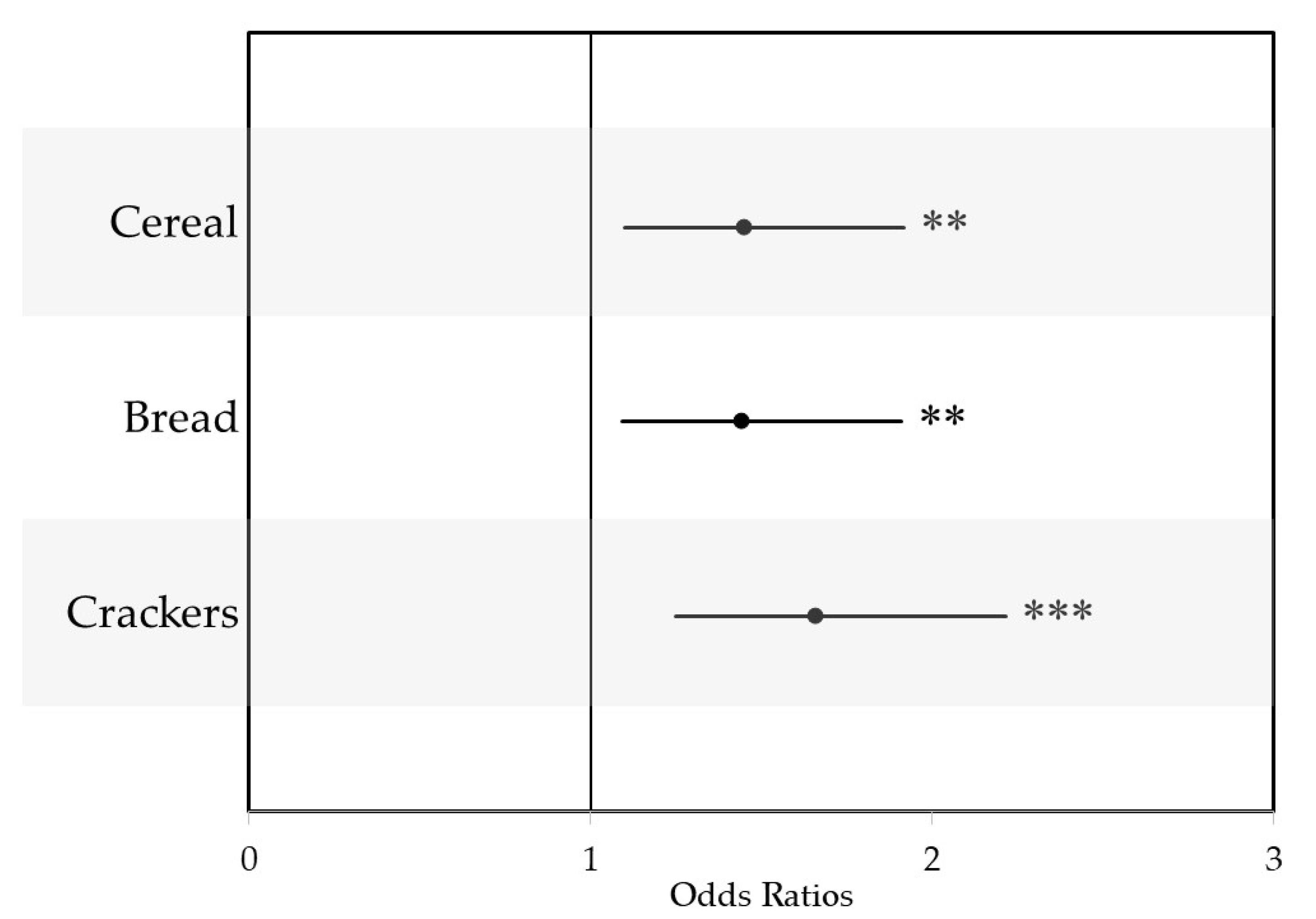
18], but we additionally find that a PDP highlighting the benefits of dietary fiber-an under-consumed nutrient—improves the healthiness of cereal, bread, and cracker choices in a grocery store environment by increasing the amount of dietary fiber/serving in products chosen by participants in the prompt condition. In all three product categories, participants in the P-PDP condition chose products that contained higher fiber density, but were also more likely to select products with higher Guiding Star ratings, suggesting that, in addition to successfully targeting fiber content, the prompt increased the overall nutritional quality of choices compared to choices made by participants in the no-PDP condition. Our correlation analysis suggests that the higher nutritional quality is due both to higher dietary fiber, which contributes to nutritional quality, but also to correlations between fiber and other nutritional attributes that improve the overall nutritional profile of the foods.
The PDP led to fiber increases of 0.43–0.71 g dietary fiber/serving in each of the three product categories, resulting in a total difference of approximately 1.5 g of dietary fiber/serving across the three food categories. Given that the average fiber intake in the US is 16.2 g/day [
8], consumption of one serving of products from each of these categories per day would lead to a 10% increase in total fiber consumption. Currently, the majority of consumer grain-based fiber consumption comes from the high consumption of low fiber foods, so successfully encouraging consumers to choose products with higher fiber content could yield marked increases in consumption of dietary fiber. Participants in the P-PDP condition also selected generally healthier products, as represented by the Guiding Star rating of the products chosen.
Inattentiveness to long-term goals, such as health during decision-making, has been documented in extensive literature on executive function [
34,
35]. Low executive function is associated with the inability to successfully ignore short-term temptations—such as taste—over long-term rewards that have less of an immediate benefit—such as health [
34]. PDPs may work better than nutrition information at reminding consumers of goals for their long-term health. Laboratory studies that simultaneously capture behavioral and neurocognitive data provide evidence on how PDPs may remind one of their long-term health goals. People experience different neural activations when prompted to think about health before making food choices compared to when they are prompted to think of taste or not prompted at all [
18]. The neural activation of health-primed individuals resembled dieters who successfully exerted self-control during food choice in an earlier study [
36]. Behaviorally, health-primed individuals placed greater value on health attributes and, as a result, were more likely to choose a healthy item [
37]. PDPs may be able to help consumers incorporate their long-term goals to balance short-term rewards by recruiting neural systems that are necessary for self-control. Future research should investigate mechanisms by which the PDP affects decision making.
It is important to remind consumers of long-term health goals at the start of their food decision process. With so many product choices within a category, consumers may not consider nutrition information available for products until they have already narrowed their choices down to a subset of choices [
14]. Once consumers begin to compare their subset of choices, they may get distracted from the nutrition information by the visuals of the packages [
38]. Health-focused PDPs may disrupt both of these processes, leading consumers to consider a broader array of products and reminding them to consider nutrition information. Reminding consumers at the start of their food choice process may better encourage shoppers to consider nutrition in their product selection.
Simulating the shopping experience online directly relates our findings to online grocery shopping experiences. Our research is particularly relevant for the growing segment of the population purchasing groceries online or through an app. An increasing number of consumers have begun to do their grocery shopping online. As of 2019, over 36% of Americans reported that they purchased groceries online [
27], and more people have reported using online grocery shopping during the COVID-19 pandemic [
39]. Before the epidemic, the Food Marketing Institute and Nielsen predicted that nearly three-fourths of consumers would purchase groceries online by 2024 [
40]. With the transition from brick-and-mortar to e-commerce grocery shopping, policymakers, researchers, and public health professionals must understand how to encourage healthier food choices in an online grocery shopping platform. The findings in our study support presenting a health PDP on the computer screen before consumers begin to fill their online grocery cart. However, we view our results as being relevant beyond the online shopping environment. Previous research on PDPs and primes was conducted in retail food stores [
6,
9], and many consumers continue to predominantly purchase food in-store. While previous PDPs have been physically displayed in-store [
6], the rise of “smart” devices that are always with consumers, such as phones and watches, present additional—and customizable—opportunities to prompt consumers when they are in the retail food outlet.
An interesting note about our findings is that the data were collected during the midst of the COVID-19 pandemic. The COVID-19 pandemic has led to increased stress in individuals and an economic downturn. During this time, a third of Americans reported experiencing a high level of psychological distress [
41] and purchases of less healthy foods increased [
42]. Historically, people consume more unhealthy foods when under these types of pressures [
42]. Despite consumers likely feeling stressed, our study still found that the PDP encouraged healthier choices. Our PDP might have been more influential if the data had not been collected during the COVID-19 pandemic. In future work, it may be interesting to collect data using this survey design once the COVID-19 pandemic has passed. This would allow us to examine changes in the effect of the PDP when consumers experience higher than average levels of stress.
A limitation of this study is that product choices were hypothetical. By making hypothetical choices, participants may not have invested as much effort in considering product options or reading product nutrition information. We attempted to address this potential bias by prompting participants to make choices as though they would be actually buying the products, and facing the same budget constraints they do in real life, which has been found to reduce hypothetical bias [
32]. While we do not report these data in the paper, analyses show that participants responded to prices in our experiment and were less likely to select higher priced items, suggesting that we were able to mitigate biases related to hypothetical choices.
In conclusion, our data show that participants who were presented a PDP about the health benefits of fiber made healthier product choices within the cereal, bread, and cracker categories by selecting products with higher fiber. This study adds to the burgeoning literature about the use of health PDPs to promote healthy food choices.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





