Iodine Status and Thyroid Function in a Group of Seaweed Consumers in Norway

 , , ,
, , ,  ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
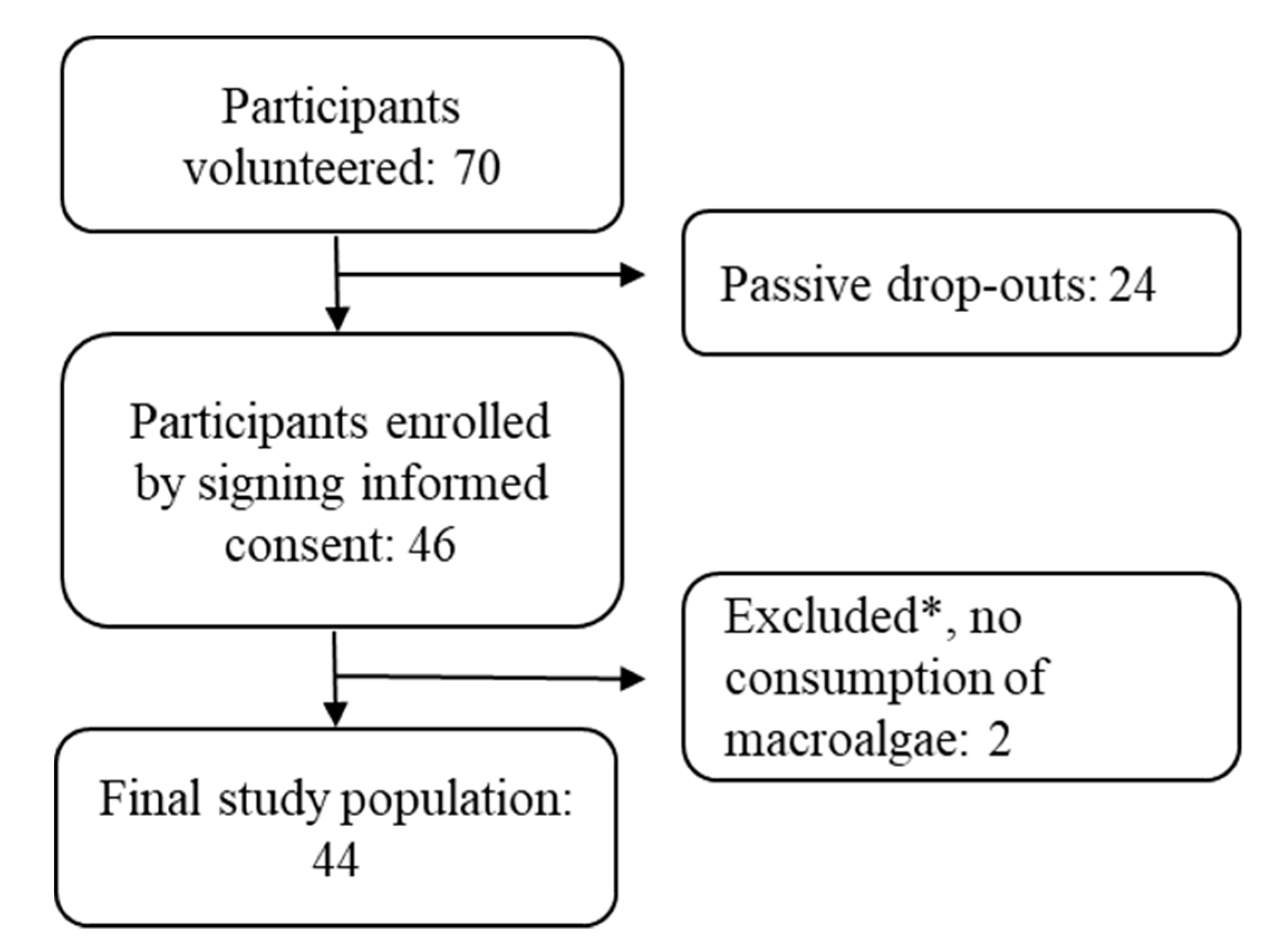
2.1. Recruitment of Study Group
2.2. Sample
2.3. Urinary Iodine Concentration
2.4. Thyroid Hormones in Blood Samples
2.5. Assessment of Iodine from Food and Dietary Supplements, Excluding Macroalgae
2.6. Assessment of Macroalgae Consumption
2.7. Assessment of Iodine from Macroalgae
2.8. Statistical Methods
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zimmermann, M.B. Iodine deficiency. Endocr. Rev. 2009, 30, 376–408. [Google Scholar] [CrossRef]
- Haldimann, M.; Alt, A.; Blanc, A.; Blondeau, K. Iodine content of food groups. J. Food Compos. Anal. 2005, 18, 461–471. [Google Scholar] [CrossRef]
- Rasmussen, L.B.; Andersen, A.; Ovesen, L.; Laurberg, P. Iodine intake and food choice. In Comprehensive Handbook of Iodine: Nutritional, Biochemical, Pathological and Therapeutic Aspects; Elsevier: Berkeley, CA, USA, 2009; pp. 333–338. [Google Scholar]
- European Food Safety Authority. Opinion of the scientific panel on additives and products or substances used in animal feed (feedap) on the use of iodine in feedingstuffs. EFSA J. 2005, 3, 168. [Google Scholar] [CrossRef]
- Teas, J.; Pino, S.; Critchley, A.; Braverman, L.E. Variability of iodine content in common commercially available edible seaweeds. Thyroid 2004, 14, 836–841. [Google Scholar] [CrossRef] [PubMed]
- Mæhre, H.K.; Malde, M.K.; Eilertsen, K.-E.; Elvevoll, E.O. Characterization of protein, lipid and mineral contents in common norwegian seaweeds and evaluation of their potential as food and feed. J. Sci. Food Agric. 2014, 94, 3281–3290. [Google Scholar] [CrossRef]
- Zava, T.T.; Zava, D.T. Assessment of japanese iodine intake based on seaweed consumption in japan: A literature-based analysis. Thyroid Res. 2011, 4, 14. [Google Scholar] [CrossRef]
- Teas, J.; Braverman, L.E.; Kurzer, M.S.; Pino, S.; Hurley, T.G.; Hebert, J.R. Seaweed and soy: Companion foods in asian cuisine and their effects on thyroid function in american women. J. Med. Food 2007, 10, 90–100. [Google Scholar] [CrossRef]
- Rhee, S.S.; Braverman, L.E.; Pino, S.; He, X.; Pearce, E.N. High iodine content of korean seaweed soup: A health risk for lactating women and their infants? Thyroid 2011, 21, 927–928. [Google Scholar] [CrossRef] [PubMed]
- Bangmei, X.; Abbott, I.A. Edible seaweeds of china and their place in the chinese diet. Econ. Bot. 1987, 41, 341–353. [Google Scholar] [CrossRef]
- McHugh, D.J. A Guide to the Seaweed Industry. Fao Fisheries Technical Paper 441; FAO: Rome, Italy, 2003. [Google Scholar]
- Bouga, M.; Combet, E. Emergence of seaweed and seaweed-containing foods in the uk: Focus on labeling, iodine content, toxicity and nutrition. Foods 2015, 4, 240–253. [Google Scholar] [CrossRef]
- MacArtain, P.; Gill, C.I.R.; Brooks, M.; Campbell, R.; Rowland, I.R. Nutritional value of edible seaweeds. Nutr. Rev. 2007, 65, 535–543. [Google Scholar] [CrossRef] [PubMed]
- FAO. The Global Status of Seaweed Production, Trade and Utilization. Globefish Research Programme; FAO: Rome, Italy, 2018. [Google Scholar]
- Holdt, S.L.; Kraan, S. Bioactive compounds in seaweed: Functional food applications and legislation. J. Appl. Phycol. 2011, 23, 543–597. [Google Scholar] [CrossRef]
- Teas, J.; Baldeón, M.E.; Chiriboga, D.E.; Davis, J.R.; Sarriés, A.J.; Braverman, L.E. Could dietary seaweed reverse the metabolic syndrome? Asia Pac. J. Clin. Nutr. 2009, 18, 145. [Google Scholar] [PubMed]
- Brown, E.M.; Allsopp, P.J.; Magee, P.J.; Gill, C.I.; Nitecki, S.; Strain, C.R.; McSorley, E.M. Seaweed and human health. Nutr. Rev. 2014, 72, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Laurberg, P.; Pedersen, I.; Carlé, A.; Andersen, S.; Knudsen, N.; Ovesen, L.; Rasmussen, L.B. The u-shaped curve of iodine intake and thyroid disorders. In Comprehensive Handbook on Iodine: Nutritional, Endocrine and Pathological Aspects; Elsevier: Amsterdam, The Netherlands, 2009; pp. 449–455. [Google Scholar]
- Burgi, H. Iodine excess. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 107–115. [Google Scholar] [CrossRef]
- Leung, A.M. The effects of iodine excess. In Iodine Deficiency Disorders and Their Elimination; Pearce, E.N., Ed.; Springer International Publishing: Berlin/Heidelberg, Germany, 2017; pp. 75–89. [Google Scholar]
- Wolff, J.; Chaikoff, I. Plasma inorganic iodide as a homeostatic regulator of thyroid function. J. Biol. Chem. 1948, 174, 555–564. [Google Scholar]
- Miyai, K.; Tokushige, T.; Kondo, M. Suppression of thyroid function during ingestion of seaweed "kombu" (laminaria japonoca) in normal japanese adults. Endocr. J. 2008, 55, 1103–1108. [Google Scholar] [CrossRef]
- Konno, N.; Makita, H.; Yuri, K.; Iizuka, N.; Kawasaki, K. Association between dietary iodine intake and prevalence of subclinical hypothyroidism in the coastal regions of japan. J. Clin. Endocrinol. Metab. 1994, 78, 393–397. [Google Scholar]
- National Food Institute; Technical University of Denmark; Sá Monteiro, M.; Sloth, J.; Holdt, S.; Hansen, M. Analysis and risk assessment of seaweed. EFSA J. 2019, 17, e170915. [Google Scholar]
- Henjum, S.; Brantsæter, A.L.; Holvik, K.; Lillegaard, I.T.L.; Mangschou, B.; Parr, C.L.; Starrfelt, J.; Stea, T.H.; Lene; Andersen, F.; et al. Benefit and Risk Assessment of Iodization of Household Salt and Salt Used in Bread and Bakery Products; Opinion of the Panel on Nutrition, Dietetic Products, Novel Food and Allergy of the Norwegian Scientific Committee for Food and Environment (VKM): Oslo, Norway, 2020. [Google Scholar]
- Cohen, N.; Arieli, T. Field research in conflict environments: Methodological challenges and snowball sampling. J. Peace Res. 2011, 48, 423–435. [Google Scholar] [CrossRef]
- Combet, E.; Ma, Z.F.; Cousins, F.; Thompson, B.; Lean, M.E.J. Low-level seaweed supplementation improves iodine status in iodine-insufficient women. Br. J. Nutr. 2014, 112, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Institute of Marine Research. Nmkl Prosedyre nr. 5. Beregning av Måleusikkerhet i Kjemiske Analyser; Institute of Marine Research (IMR): Bergen, Norway, 2004. [Google Scholar]
- IOM. Reference Intakes for Vitamin a, Vitamin k, Arsenic, boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium and Zinc: A Report of the Panel on Micronutrients, Subcommittees on Upper Reference Levels of Nutrients and Interpretation and Uses of Dietary Reference Intakes, and the Standing Committee on the Scientific Evaluation of Dietary Reference Intakes; Institute of Medicine: Washington, DC, USA, 2001. [Google Scholar]
- Carlsen, M.; Andersen, L.; Dahl, L.; Norberg, N.; Hjartåker, A. New Iodine Food Composition Database and Updated Calculations of Iodine Intake among Norwegians. Nutrients 2018, 10, 930. [Google Scholar] [CrossRef]
- Dalane, J.Ø.; Bergvatn, T.A.M.; Kielland, E.; Carlsen, M.H. Mål, Vekt og Porsjonsstørrelser for Matvarer [Weights, Measures, and Portion Sizes for Foods] (in Norwegian); Norwegian Food Safety Authority, University of Oslo, Norwegian Directorate of Health: Oslo, Norway, 2015. [Google Scholar]
- Norwegian Food Safety Authority; The Norwegian Directorate of Health; University of Oslo. The Norwegian Food Composition Table (01.01.2020); The Norwegian Food Safety Authority: Oslo, Norway, 2020.
- Nerhus, I.; Wik Markhus, M.; Nilsen, B.Ø.J.; Maage, A.; Ødegård, E.; Kolden Midtbø, L.; Frantzen, S.; Kögel, T.; Eide Graff, I.; Lie, Ø.; et al. Iodine Content of Six Fish Species, Norwegian Dairy Products and Hen’s Egg; Food & Nutrition Research: Lund, Sweeden, 2018; Volume 62. [Google Scholar]
- Henjum, S.; Aakre, I.; Lilleengen, A.; Garnweidner-Holme, L.; Borthne, S.; Pajalic, Z.; Blix, E.; Gjengedal, E.; Brantsæter, A. Suboptimal iodine status among pregnant women in the oslo area, norway. Nutrients 2018, 10, 280. [Google Scholar] [CrossRef] [PubMed]
- WHO. Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination. A Guide for Programme Managers; World Health Organisation, International Council for Control of Iodine Deficiency Disorders, United Nations Children’s Fund: Geneva, Switzerland, 2007. [Google Scholar]
- SCF. Opinion of the Scientific Committee on Food on the Tolerable Upper Intake Level of Iodine; Scientific Committee on Food: Brussels, Belgium, 2002. [Google Scholar]
- Nitschke, U.; Stengel, D.B. A new HPLC method for the detection of iodine applied to natural samples of edible seaweeds and commercial seaweed food products. Food Chem. 2015, 172, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Aquaron, R.; Delange, F.; Marchal, P.; Lognoné, V.; Ninane, L. Bioavailability of seaweed iodine in human beings. Cell. Mol. Biol. 2002, 48, 563–569. [Google Scholar]
- Andersen, S.; Noahsen, P.; Rex, K.F.; Florian-Sørensen, H.C.; Mulvad, G. Iodine in edible seaweed, its absorption, dietary use, and relation to iodine nutrition in arctic people. J. Med. Food 2019, 22, 421–426. [Google Scholar] [CrossRef]
- Åsvold, B.O.; Vatten, L.J.; Midthjell, K.; Bjøro, T. Serum tsh within the reference range as a predictor of future hypothyroidism and hyperthyroidism: 11-year follow-up of the hunt study in norway. J. Clin. Endocrinol. Metab. 2012, 97, 93–99. [Google Scholar] [CrossRef]
- Hollowell, J.G.; Staehling, N.W.; Flanders, W.D.; Hannon, W.H.; Gunter, E.W.; Spencer, C.A.; Braverman, L.E. Serum tsh, t4, and thyroid antibodies in the united states population (1988 to 1994): National health and nutrition examination survey (nhanes iii). J. Clin. Endocrinol. Metab. 2002, 87, 489–499. [Google Scholar] [CrossRef]
- Di Matola, T.; Zeppa, P.; Gasperi, M.; Vitale, M. Thyroid dysfunction following a kelp-containing marketed diet. BMJ Case Rep. 2014, 2014, bcr2014206330. [Google Scholar] [CrossRef]
- Gherbon, A.; Frandes, M.; Lungeanu, D.; Nicula, M.; Timar, R. Transient hyperthyroidism following the ingestion of complementary medications containing kelp seaweed: A case-report. Medicine 2019, 98, e17058. [Google Scholar] [CrossRef]
- Eliason, B.C. Transient hyperthyroidism in a patient taking dietary supplements containing kelp. J. Am. Board Fam. Pract. 1998, 11, 478–480. [Google Scholar] [CrossRef] [PubMed]
- Müssig, K.; Thamer, C.; Bares, R.; Lipp, H.-P.; Häring, H.-U.; Gallwitz, B. Iodine-induced thyrotoxicosis after ingestion of kelp-containing tea. J. Gen. Intern. Med. 2006, 21, C11–C14. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, S.; Mikeda, T.; Okada, T.; Nakamura, K.; Kotani, T.; Hishinuma, A. Transient hypothyroidism or persistent hyperthyrotropinemia in neonates born to mothers with excessive iodine intake. Thyroid 2004, 14, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Emder, P.J.; Jack, M.M. Iodine-induced neonatal hypothyroidism secondary to maternal seaweed consumption: A common practice in some asian cultures to promote breast milk supply. J. Paediatr. Child Health 2011, 47, 750–752. [Google Scholar] [CrossRef] [PubMed]
- Clark, M.; Clifford, D.; Bassett, M.; Bertram; Burge, M.; Mark, R. Effects of kelp supplementation on thyroid function in euthyroid subjects. Endocr. Pract. 2003, 9, 363–369. [Google Scholar] [CrossRef]
- Aakre, I.; Bjøro, T.; Norheim, I.; Strand, T.A.; Barikmo, I.; Henjum, S. Excessive iodine intake and thyroid dysfunction among lactating saharawi women. J. Trace Elem. Med. Biol 2015, 31, 279–284. [Google Scholar] [CrossRef]
- Aakre, I.; Bjøro, T.; Norheim, I.; Strand, T.A.; Barikmo, I.; Henjum, S. Development of thyroid dysfunction among women with excessive iodine intake–a 3-year follow-up. J. Trace Elem. Med. Biol. 2015, 31, 61–66. [Google Scholar] [CrossRef]
- Aakre, I.; Strand, T.A.; Bjøro, T.; Norheim, I.; Barikmo, I.; Ares, S.; Alcorta, M.D.; Henjum, S. Thyroid function among breastfed children with chronically excessive iodine intakes. Nutrients 2016, 8, 398. [Google Scholar] [CrossRef]
- Katagiri, R.; Yuan, X.; Kobayashi, S.; Sasaki, S. Effect of excess iodine intake on thyroid diseases in different populations: A systematic review and meta-analyses including observational studies. PLoS ONE 2017, 12, e0173722. [Google Scholar] [CrossRef]
- Jansen, T.A.; Korevaar, T.I.M.; Mulder, T.A.; White, T.; Muetzel, R.L.; Peeters, R.P.; Tiemeier, H. Maternal thyroid function during pregnancy and child brain morphology: A time window-specific analysis of a prospective cohort. Lancet Diabetes Endocrinol. 2019, 7, 629–637. [Google Scholar] [CrossRef]
- Pearce, E.N.; Lazarus, J.H.; Moreno-Reyes, R.; Zimmermann, M.B. Consequences of iodine deficiency and excess in pregnant women: An overview of current knowns and unknowns. Am. J. Clin. Nutr. 2016, 104, 918S–923S. [Google Scholar] [CrossRef]
- Chen, S.; Zhou, X.; Zhu, H.; Yang, H.; Gong, F.; Wang, L.; Zhang, M.; Jiang, Y.; Yan, C.; Li, J.; et al. Preconception tsh and pregnancy outcomes: A population-based cohort study in 184,611 women. Clin. Endocrinol. (Oxf.) 2017, 86, 816–824. [Google Scholar] [CrossRef]
- Leung, A.M.; Braverman, L.E. Iodine-induced thyroid dysfunction. Curr. Opin. Endocrinol. Diabetes Obes. 2012, 19, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Roleda, M.Y.; Skjermo, J.; Marfaing, H.; Jónsdóttir, R.; Rebours, C.; Gietl, A.; Stengel, D.B.; Nitschke, U. Iodine content in bulk biomass of wild-harvested and cultivated edible seaweeds: Inherent variations determine species-specific daily allowable consumption. Food Chem. 2018, 254, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Cherry, P.; O’Hara, C.; Magee, P.J.; McSorley, E.M.; Allsopp, P.J. Risks and benefits of consuming edible seaweeds. Nutr. Rev. 2019, 77, 307–329. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics d | UIC b µg/L | p-Value c | |
|---|---|---|---|
| Age, mean | 46.1 ± 12.4 | ||
| Male | 16 [36.4] | 1400 (428–2119) | 1.00 |
| Female | 27 [61.4] | 825 (250–5200) | |
| BMI, kg/m2 | 25.4 ± 5.4 | ||
| Country of birth | 0.01 | ||
| Norway | 33 [75] | 620 (226–2550) | |
| Other | 11 [25] | 2225 (1550–5700) | |
| Education level | |||
| ≤High school | 10 [23.3] | 935 (403–1725) | 0.081 |
| ≤4 years university/college | 10 [23.3] | 402 (183–1676) | |
| >4 years university/college | 23 [53.5] | 2225 (655–5700) | |
| Smoking habits | |||
| No | 27 [61.4] | 1250 (620–2950) | 0.366 e |
| Daily/Occasionally | 4 [9.1] | 2200 (496–11213) | |
| Former smoker | 12 [27.3] | 215 (135–1763) | |
| Smokeless tobacco (Snus) | |||
| Daily | 1 [2.3] | ||
| Self-reported thyroid disease | |||
| Hypothyroidism | 3 [6.8] | ||
| Number of children | 1.3 ± 1.5 | ||
| Planned pregnancy, next two years | 1 [2.3] | ||
| Vegetarian practice | 7 [15.9] | 165 (85–1800) | 0.045 f |
| Vegetarian | 1 [2.3] | ||
| Vegan | 2 [4.5] | ||
| Pesco-vegetarian | 2 [4.5] | ||
| Pesco-vegetarian, excluding milk | 2 [4.5] | ||
| Use of iodine containing supplement | 5 [11.4] |
| UIC, µg/L | Median | p25 | p75 | Mean ± SD | Min, Max | P f |
|---|---|---|---|---|---|---|
| 1st urine sample b | 1080 | 300 | 2150 | 1840 ± 2360 | 70, 12,000 | 0.171 |
| 2nd urine sample c | 1050 | 340 | 3450 | 2500 ± 3450 | 70, 16,000 | |
| Mean 1st and 2nd urine sample | 1200 | 370 | 2850 | 2170 ± 2770 | 80, 14,000 | |
| Iodine intake, µg/day | ||||||
| I-24H from food and non-algae supplements | 110 | 70 | 970 | 390 ± 440 | 30, 1140 | |
| FFQ from food and non-algae supplements | 260 | 150 | 380 | 340 ± 490 | 30, 3300 | |
| Daily iodine intake estimated from UIC d | 2430 g | 500 | 4630 | 3750 ± 4770 | 120, 25,660 | |
| Estimated iodine intake from seaweed only e, µg/day | ||||||
| 24 h intake (I-24H) | 2160 | 280 | 4270 | 3450 ± 4720 | 0, 25,520 | |
| Habitual intake (FFQ) | 2200 | 280 | 4060 | 3420 ± 4750 | 0, 25,530 |
| Macroalgae Type | Macroalgae Consumption the Day of Urine Sample | UIC, µg/L |
|---|---|---|
| n [%] | Median (p25–p75) | |
| Sugar kelp | 10 [23] | 2900 (1170–6587) |
| Mix a | 12 [27] | 1350 (629–4613) |
| Badderlocks, winged kelp | 9 [21] | 1650 (565–1800) |
| Rockweed, egg wrack | 4 [9] | 335 (123–596) |
| Oarweed | 1 [2] | - |
| Wakame | 1 [2] | - |
| Dulse | 1 [2] | - |
| Laver | 1 [2] | - |
| Unspecified | 5 [11] | 250 (144–1305) |
| Thyroid Hormones and TPOAb | Median | p25 | p75 | Mean ± SD | Min, Max | Reference |
|---|---|---|---|---|---|---|
| Serum TSH (mIU/L) a | 1.8 | 1.4 | 2.6 | 2.0 ± 0.9 | 0.6, 4.2 | 0.2–4.0 |
| Serum fT4 (pmol/L) | 16.0 | 14.5 | 17.2 | 15.9 ± 1.9 | 12.5, 20.1 | 11.0–23.0 |
| Serum fT3 (pmol/L) | 5.0 | 4.6 | 5.4 | 5.0 ± 0.5 | 4.3, 5.9 | 3.5–6.5 |
| TPOAb (kU/L) | n [%] | Min, Max | ||||
| <34 | 13 [68] | <34,784 | ||||
| ≥34–100 | 4 [21] | <100 | ||||
| >100 | 2 [11] | |||||
| Wholefood Macroalgae (n = 41) | Food Containing Macroalgae (n = 35) | Supplement Containing Macroalgae (n = 5) | All Product Categories (n = 44) | UIC, µg/L | |
|---|---|---|---|---|---|
| Frequency of seaweed consumption a | n [%] b | n [%] b | n [%] b | n [%] b,c | Median (p25–p75) |
| Daily | 10 [23] | 5 [11] | 2 [5] | 13 [30] | 655 (253–2013) |
| 4–6 times/week | 8 [18] | 5 [11] | 0 | 10 [23] | 2550 (564–6625) |
| 1–3 times/week | 16 [36] | 7 [16] | 1 [2] | 15 [34] | 1115 (203–2850) |
| Monthly | 4 [9] | 16 [36] | 2 [5] | 6 [14] | 1525 (893–3438) |
| Other | 3 [7] | 2 [5] | 0 | 0 | - |
| Procurement frequencies | n [%] d | n [%] d | n [%] d | ||
| Personally harvested | 17 [42] | 7 [20] | 0 | - | - |
| Common food store (chain) | 1 [2] | 10 [29] | 1 [20] | - | - |
| Common food store (not chain) | 2 [5] | 1 [3] | 1 [20] | - | - |
| Online store | 4 [10] | 0 | 1 [20] | - | - |
| Health food store | 2 [5] | 0 | 0 | - | - |
| Restaurant | 0 | 2 [6] | 0 | - | - |
| Unspecified store | 8 [20] | 5 [14] | 0 | - | - |
| Product declaration of iodine e | |||||
| Yes | 9 [22] | 5 [14] | 2 [40] | - | - |
| No | 21 [51] | 25 [71] | 2 [40] | - | - |
| Category | English | Latin | Habitual Consumption a |
|---|---|---|---|
| n [%] b | |||
| Brown algae | Sugar kelp | Saccharina latissima | 17 [39] |
| Badderlocks, winged kelp | Alaria esculenta | 16 [36] | |
| Bladderwrack | Fucus vesiculosus | 5 [11] | |
| Sea spaghetti | Himanthalia elongata | 5 [11] | |
| Wakame | Undaria pinnatifida | 4 [9] | |
| Horned wrack | Fucus serratus | 4 [9] | |
| Oarweed | Laminaria digitata | 4 [9] | |
| Japanese kelp | Laminaria japonica/Saccharina japonica | 2 [5] | |
| Rockweed, egg wrack | Ascophyllum nodosum | 2 [5] | |
| Green algae | Sea lettuce | Ulva lactuca | 4 [9] |
| Gut weed, mermaids’ hair | Enteromorpha intestinalis | 1 [2] | |
| Red algae | Dulse | Palmaria palmata | 15 [34] |
| Laver | Porphyra purpurea | 8 [18] | |
| Wrack siphon weed | Polysiphonia (vertebrata) lanosa | 1 [2] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aakre, I.; Tveito Evensen, L.; Kjellevold, M.; Dahl, L.; Henjum, S.; Alexander, J.; Madsen, L.; Markhus, M.W. Iodine Status and Thyroid Function in a Group of Seaweed Consumers in Norway. Nutrients 2020, 12, 3483. https://doi.org/10.3390/nu12113483
Aakre I, Tveito Evensen L, Kjellevold M, Dahl L, Henjum S, Alexander J, Madsen L, Markhus MW. Iodine Status and Thyroid Function in a Group of Seaweed Consumers in Norway. Nutrients. 2020; 12(11):3483. https://doi.org/10.3390/nu12113483
Chicago/Turabian StyleAakre, Inger, Lidunn Tveito Evensen, Marian Kjellevold, Lisbeth Dahl, Sigrun Henjum, Jan Alexander, Lise Madsen, and Maria Wik Markhus. 2020. "Iodine Status and Thyroid Function in a Group of Seaweed Consumers in Norway" Nutrients 12, no. 11: 3483. https://doi.org/10.3390/nu12113483
APA StyleAakre, I., Tveito Evensen, L., Kjellevold, M., Dahl, L., Henjum, S., Alexander, J., Madsen, L., & Markhus, M. W. (2020). Iodine Status and Thyroid Function in a Group of Seaweed Consumers in Norway. Nutrients, 12(11), 3483. https://doi.org/10.3390/nu12113483