Association of Yogurt Consumption with Nutrient Intakes, Nutrient Adequacy, and Diet Quality in American Children and Adults


Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Estimation of Energy and Nutrients Intakes
2.3. Estimation of Diet Quality and Intake of Food Groups
2.4. Estimation of Anthropometric Measures
2.5. Statistical Analysis
3. Results
3.1. Yogurt Intake
3.2. Comparison Between Yogurt Consumers vs. Non-Consumers on Energy and Nutrient Intakes
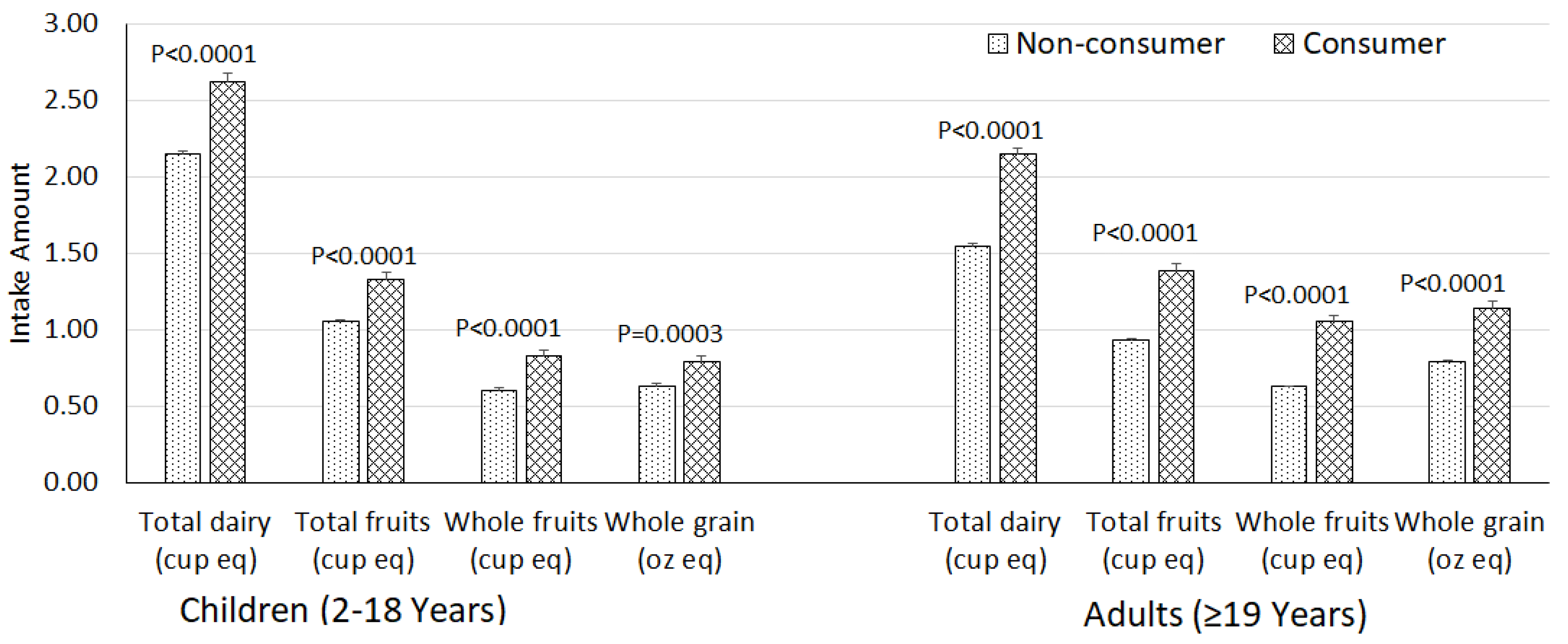
3.3. Link Between Yogurt Intake and Diet Quality
3.4. Association Between Yogurt Intake and Anthropometric Measures
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Hutkins, R.W. Microbiology and Technology of Fermented Foods, 2nd ed.; Wiley: Hoboken, NJ, USA, 2018. [Google Scholar]
- FDA. Yogurt. 21 CFR 131.200, Code of Federal Regulations; US Department of Health and Human Services: Washington, DC, USA, 2013.
- USDA-ERS. Dairy Data. Available online: https://www.ers.usda.gov/data-products/dairy-data.aspx (accessed on 17 August 2020).
- Nielsen, S.J.; Ogden, C. Trends in yogurt consumption, US adults, 1999–2012. FASEB J. 2015, 29, 587.17. [Google Scholar]
- USDA Food Data Central Database. Available online: https://fdc.nal.usda.gov/ (accessed on 20 March 2020).
- Kok, C.R.; Hutkins, R. Yogurt and other fermented foods as sources of health-promoting bacteria. Nutr. Rev. 2018, 76, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Savaiano, D.A.; Hutkins, R.W. Yogurt, cultured fermented milk, and health: A systematic review. Nutr. Rev. 2020. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, M.A.; Panahi, S.; Daniel, N.; Tremblay, A.; Marette, A. Yogurt and cardiometabolic diseases: A critical review of potential mechanisms. Adv. Nutr. 2017, 8, 812–829. [Google Scholar] [CrossRef] [PubMed]
- Astrup, A. Yogurt and dairy product consumption to prevent cardiometabolic diseases: Epidemiologic and experimental studies. Am. J. Clin. Nutr. 2014, 99, 1235S–1242S. [Google Scholar] [CrossRef]
- Gijsbers, L.; Ding, E.L.; Malik, V.S.; de Goede, J.; Geleijnse, J.M.; Soedamah-Muthu, S.S. Consumption of dairy foods and diabetes incidence: A dose-response meta-analysis of observational studies. Am. J. Clin. Nutr. 2016, 103, 1111–1124. [Google Scholar] [CrossRef]
- Chen, M.; Sun, Q.; Giovannucci, E.; Mozaffarian, D.; Manson, J.E.; Willett, W.C.; Hu, F.B. Dairy consumption and risk of type 2 diabetes: 3 cohorts of US adults and an updated meta-analysis. BMC Med. 2014, 12, 215. [Google Scholar] [CrossRef]
- Wu, L.; Sun, D. Consumption of yogurt and the incident risk of cardiovascular disease: A meta-analysis of nine cohort studies. Nutrients 2017, 9, 315. [Google Scholar] [CrossRef] [PubMed]
- PREDIMED Investigators. Consumption of yogurt, low-fat milk, and other low-fat dairy products is associated with lower risk of metabolic syndrome incidence in an elderly Mediterranean population. J. Nutr. 2015, 145, 2308–2316. [Google Scholar] [CrossRef]
- Farvid, M.S.; Malekshah, A.F.; Pourshams, A.; Poustchi, H.; Sepanlou, S.G.; Sharafkhah, M.; Khoshnia, M.; Farvid, M.; Abnet, C.C.; Kamangar, F.; et al. Dairy food intake and all-cause, cardiovascular disease, and cancer mortality: The Golestan cohort study. Am. J. Epidemiol. 2017, 185, 697–711. [Google Scholar] [CrossRef]
- Buendia, J.R.; Li, Y.; Hu, F.B.; Cabral, H.J.; Bradlee, M.L.; Quatromoni, P.A.; Singer, M.R.; Curhan, G.C.; Moore, L.L. Long-Term yogurt consumption and risk of incident hypertension in adults. J. Hypertens. 2018, 36, 1671–1679. [Google Scholar] [CrossRef]
- Wang, H.; Fox, C.S.; Troy, L.M.; Mckeown, N.M.; Jacques, P.F. Longitudinal association of dairy consumption with the changes in blood pressure and the risk of incident hypertension: The Framingham Heart Study. Br. J. Nutr. 2015, 114, 1887–1899. [Google Scholar] [CrossRef]
- Trichia, E.; Luben, R.; Khaw, K.T.; Wareham, N.J.; Imamura, F.; Forouhi, N.G. The associations of longitudinal changes in consumption of total and types of dairy products and markers of metabolic risk and adiposity: Findings from the European Investigation into Cancer and Nutrition (EPIC)-Norfolk study, United Kingdom. Am. J. Clin. Nutr. 2020, 111, 1018–1026. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Hao, T.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Changes in diet and lifestyle and long-term weight gain in women and men. New Eng. J. Med. 2011, 364, 2392–2404. [Google Scholar] [CrossRef]
- Eales, J.; Lenoir-Wijnkoop, I.; King, S.; Wood, H.; Kok, F.J.; Shamir, R.; Prentice, A.; Edwards, M.; Glanville, J.; Atkinson, R.L. Is consuming yoghurt associated with weight management outcomes? Results from a systematic review. Int. J. Obes. 2016, 40, 731–746. [Google Scholar] [CrossRef]
- Wang, H.; Troy, L.M.; Rogers, G.T.; Fox, C.S.; McKeown, N.M.; Meigs, J.B.; Jacques, P.F. Longitudinal association between dairy consumption and changes of body weight and waist circumference: The Framingham Heart Study. Int. J. Obes. 2014, 38, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Hobbs, D.A.; Givens, D.I.; Lovegrove, J.A. Yogurt consumption is associated with higher nutrient intake, diet quality and favourable metabolic profile in children: A cross-sectional analysis using data from years 1–4 of the National diet and Nutrition Survey, UK. Eur. J. Nutr. 2019, 58, 409–422. [Google Scholar] [CrossRef]
- Vatanparast, H.; Islam, N.; Patil, R.P.; Shamloo, A.; Keshavarz, P.; Smith, J.; Whiting, S. Consumption of yogurt in Canada and its contribution to nutrient intake and diet quality among Canadians. Nutrients 2019, 11, 1203. [Google Scholar] [CrossRef]
- Wang, H.; Livingston, K.A.; Fox, C.S.; Meigs, J.B.; Jacques, P.F. Yogurt consumption is associated with better diet quality and metabolic profile in American men and women. Nutr. Res. 2013, 33, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Wang, H.; Hollis, J.H.; Jacques, P.F. The associations between yogurt consumption, diet quality, and metabolic profiles in children in the USA. Eur. J. Nutr. 2015, 54, 543–550. [Google Scholar] [CrossRef]
- Keast, D.R.; Hill Gallant, K.M.; Albertson, A.M.; Gugger, C.K.; Holschuh, N.M. Associations between yogurt, dairy, calcium, and vitamin D intake and obesity among U.S. children aged 8-18 years: NHANES, 2005–2008. Nutrients 2015, 7, 1577–1593. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC); National Center for Health Statistics. National Health and Nutrition Examination Survey. Hyattsville, M.D.: National Center for Health Statistics. Available online: https://www.cdc.gov/nchs/nhanes/index.htm (accessed on 25 March 2020).
- National Center for Health Statistics. Available online: http://www.cdc.gov/nchs/nhanes/ (accessed on 16 September 2020).
- Raper, N.; Perloff, B.; Ingwersen, L.; Steinfeldt, L.; Anand, J. An overview of USDA’s dietary intake data system. J. Food Comp. Anal. 2004, 17, 545–555. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture, Agricultural Research Service. 2018; USDA Food and Nutrient Database for Dietary Studies. Food Surveys Research Group Home Page. Available online: http://www.ars.usda.gov/nea/bhnrc/fsrg (accessed on 25 March 2020).
- U.S. Department of Health and Human Services; U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans, 8th ed.; December 2015. Available online: http://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 7 July 2020).
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture, Agricultural Research Service. USDA Food Patterns Equivalent Database. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/fped-overview/ (accessed on 25 March 2020).
- USDA. Choose My Plate. Available online: https://www.choosemyplate.gov (accessed on 25 March 2020).
- Kuczmarski, R.J.; Ogden, C.L.; Guo, S.S.; Grummer-Strawn, L.M.; Flegal, K.M.; Mei, Z.; Wei, R.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. 2000 CDC Growth Charts for the United States: Methods and Development; Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics: Rockville, MD, USA, 2002; Volume 11, pp. 1–190.
- Expert Panel on the Identification, Evaluation, and Treatment of Overweight in Adults. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: Executive Summary; National Institutes of Health, National Heart, Lung, and Blood Institute: Bethesda, MD, USA, 1998; Volume 68, pp. 899–917. [CrossRef]
- Tooze, J.A.; Kipnis, V.; Buckman, D.W.; Carroll, R.J.; Freedman, L.S.; Guenther, P.M.; Krebs-Smith, S.M.; Subar, A.F.; Dodd, K.W. A mixed-effects model approach for estimating the distribution of usual intake of nutrients: The NCI method. Stat. Med. 2010, 29, 2857–2868. [Google Scholar] [CrossRef]
- Dietary Guidelines Advisory Committee. Scientific Report of the 2015 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Health and Human Services and the Secretary of Agriculture; U.S. Department of Agriculture, Agricultural Research Service: Washington, DC, USA. Available online: https://www.dietaryguidelines.gov/sites/default/files/2019-05/Scientific-Report-of-the-2015-Dietary-Guidelines-Advisory-Committee.pdf (accessed on 7 July 2020).
- Muehlhoff, E.; Bennett, A.; Mcmahon, D. Milk and Dairy Products in Human Nutrition; Food and Agriculture Organization of the United Nations: Rome, Italy, 2013.
- Pfeuffer, M.; Watzl, B. Nutrition and health aspects of milk and dairy products and their ingredients. Ernahr. Umsch. 2018, 65, 22–33.e14–e17. [Google Scholar] [CrossRef]
- O’Neil, C.E.; Nicklas, T.A.; Fulgoni, V.L., III. Food sources of energy and nutrients of public health concern and nutrients to limit with a focus on milk and other dairy foods in children 2 to 18 years of age: National health and nutrition examination survey, 2011–2014. Nutrients 2018, 10, 1050. [Google Scholar] [CrossRef]
- O’Neil, C.E.; Keast, D.R.; Fulgoni, V.L.; Nicklas, T.A. Food sources of energy and nutrients among adults in the US: NHANES 2003–2006. Nutrients 2012, 4, 2097–2120. [Google Scholar] [CrossRef]
- Hiza, H.A.; Casavale, K.O.; Guenther, P.M.; Davis, C.A. Diet quality of Americans differs by age, sex, race/ethnicity, income, and education level. J. Acad. Nutr. Diet. 2013, 113, 297–306. [Google Scholar] [CrossRef]
- Reedy, J.; Krebs-Smith, S.M.; Bosire, C. Evaluating the food environment: Application of the Healthy Eating Index-2005. Am. J. Prev. Med. 2010, 38, 465–471. [Google Scholar] [CrossRef]
- USDA-CNPP. Nutrition Insight 41. Diet Quality of Older Americans in 1994-96 and 2001-02 as Measured by the Healthy Eating Index-2005; USDA/CNPP: Alexandria, VA, USA, 2008.
- Fulgoni, V.L.; Keast, D.R.; Drewnowski, A. Development and validation of the nutrient-rich foods index: A tool to measure nutritional quality of foods. J. Nutr. 2009, 139, 1549–1554. [Google Scholar] [CrossRef]
- Nicklas, T.A.; O’Neil, C.E.; Fulgoni, V.L. Diet quality is inversely related to cardiovascular risk factors in adults. J. Nutr. 2012, 142, 2112–2118. [Google Scholar] [CrossRef]
- Chiuve, S.E.; Fung, T.T.; Rimm, E.B.; Hu, F.B.; McCullough, M.L.; Wang, M.; Stampfer, M.J.; Willett, W.C. Alternative dietary indices both strongly predict risk of chronic disease. J. Nutr. 2012, 142, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Reedy, J.; Mitrou, P.N.; Krebs-Smith, S.M.; Wirfalt, E.; Flood, A.; Kipnis, V.; Leitzmann, M.; Mouw, T.; Hollenbeck, A.; Schatzkin, A.; et al. Index-based dietary patterns and risk of colorectal cancer: The NIH-AARP diet and health study. Am. J. Epidemiol. 2008, 168, 38–48. [Google Scholar] [CrossRef]
- O’Neil, C.E.; Nicklas, T.A.; Rampersaud, G.C.; Fulgoni, V.L. One hundred percent orange juice consumption is associated with better diet quality, improved nutrient adequacy, and no increased risk for overweight/obesity in children. Nutr. Res. 2011, 31, 673–682. [Google Scholar] [CrossRef]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. Expert consensus document. The international scientific association for probiotics and prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef]
- Marco, M.L.; Heeney, D.; Binda, S.; Cifelli, C.J.; Cotter, P.D.; Foligne, B.; Ganzle, M.; Kort, R.; Pasin, G.; Pihlanto, A.; et al. Health benefits of fermented foods: Microbiota and beyond. Curr. Opin. Biotechnol. 2017, 44, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 2014, 311, 806–814. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services, Office of the Surgeon General. The Surgeon General’s Vision for a Healthy and Fit Nation; U.S. Department of Health and Human Services, Office of the Surgeon General: Rockville, MD, USA, 2010.
- Finkelstein, E.A.; Trogdon, J.G.; Cohen, J.W.; Dietz, W. Annual medical spending attributable to obesity: Payer-and service-specific estimates. Health. Aff. 2009, 28, w822–w831. [Google Scholar] [CrossRef]
- Olsen, N.J.; Heitmann, B.L. Intake of calorically sweetened beverages and obesity. Obes. Rev. 2009, 10, 68–75. [Google Scholar] [CrossRef]
- Malik, V.S.; Schulze, M.B.; Hu, F.B. Intake of sugar-sweetened beverages and weight gain: A systematic review. Am. J. Clin. Nutr. 2006, 84, 274–288. [Google Scholar] [CrossRef]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Despres, J.P.; Hu, F.B. Sugar-sweetened beverages, obesity, type 2 diabetes mellitus, and cardiovascular disease risk. Circulation 2010, 121, 1356–1364. [Google Scholar] [CrossRef]
- Dietary Guidelines Advisory Committee. Scientific Report of the 2020 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Agriculture and the Secretary of Health and Human Services; U.S. Department of Agriculture, Agricultural Research Service: Washington, DC, USA. Available online: https://www.dietaryguidelines.gov/2020-advisory-committee-report (accessed on 16 September 2020).


{kind=link}
| Variable | Children (2–18 Years) | Adults (≥19 Years) | ||
|---|---|---|---|---|
| All sources | Yogurt only | All sources | Yogurt only | |
| Energy (kcal) | 1860 ± 25 | 144 ± 3 | 2114 ± 25 | 160 ± 2 |
| Carbohydrate (g) | 257 ± 3 | 24.6 ± 0.6 | 267 ± 4 | 25.7 ± 0.5 |
| Dietary fiber (g) | 13.5 ± 0.2 | 0.08 ± 0.01 | 19.8 ± 0.3 | 0.24 ± 0.02 |
| Total sugars (g) | 137 ± 2 | 23.2 ± 0.6 | 126 ± 2 | 22.0 ± 0.5 |
| Added sugars (tsp eq) | 17.6 ± 0.4 | 3.15 ± 0.09 | 16.3 ± 0.4 | 2.65 ± 0.09 |
| Protein (g) | 67.9 ± 1.2 | 7.07 ± 0.16 | 87.4 ± 1.2 | 9.59 ± 0.20 |
| Total fat (g) | 65.0 ± 1.3 | 2.15 ± 0.07 | 76.3 ± 1.2 | 2.25 ± 0.07 |
| Cholesterol (mg) | 198 ± 8 | 8.0 ± 0.2 | 249 ± 6 | 9.28 ± 0.22 |
| Calcium (mg) | 1227 ± 22 | 227 ± 5 | 1228 ± 17 | 267 ± 4 |
| Iron (mg) | 13.3 ± 0.3 | 0.12 ± 0.003 | 15.6 ± 0.3 | 0.16 ± 0.004 |
| Magnesium (mg) | 246 ± 3 | 22.4 ± 0.5 | 351 ± 5 | 26.9 ± 0.4 |
| Potassium (mg) | 2383 ± 35 | 294 ± 6 | 3133 ± 38 | 350 ± 5 |
| Sodium (mg) | 2719 ± 45 | 87.5 ± 1.8 | 3373 ± 47 | 103 ± 2 |
| Vitamin A, RAE (µg) | 639 ± 16 | 29.5 ± 2.0 | 749 ± 17 | 48.7 ± 2.2 |
| Thiamin (mg) | 1.47 ± 0.02 | 0.06 ± 0.001 | 1.69 ± 0.03 | 0.07 ± 0.001 |
| Folate, DFE (µg) | 521 ± 13 | 14.7 ± 0.4 | 600 ± 12 | 18.7 ± 0.4 |
| Vitamin B6 (mg) | 1.61 ± 0.03 | 0.06 ± 0.001 | 2.20 ± 0.05 | 0.08 ± 0.001 |
| Vitamin B12 (µg) | 5.12 ± 0.12 | 0.73 ± 0.01 | 5.88 ± 0.21 | 0.92 ± 0.01 |
| Vitamin C (mg) | 84.6 ± 3.0 | 1.45 ± 0.09 | 102 ± 3 | 2.43 ± 0.14 |
| Vitamin D (µg) | 6.57 ± 0.18 | 0.69 ± 0.03 | 5.41 ± 0.17 | 0.84 ± 0.03 |
| Variables | Children (2–18 Years) | Adults (≥19 Years) | ||||
|---|---|---|---|---|---|---|
| Non-Consumers (n = 22,355) | Consumers (n = 1557) | p Value for Difference | Non-Consumers (n = 34,711) | Consumers (n = 2024) | p Value for Difference | |
| Energy (kcal) | 1947 ± 9 | 1985 ± 26 | 0.1454 | 2142 ± 7 | 2247 ± 24 | <0.0001 |
| Carbohydrate (g) | 262 ± 1 | 268 ± 1 | 0.0001 | 254 ± 1 | 266 ± 2 | <0.0001 |
| Dietary fiber (g) | 13.3 ± 0.1 | 13.9 ± 0.2 | 0.0019 | 16.4 ± 0.1 | 19.0 ± 0.3 | <0.0001 |
| Total sugars (g) | 129 ± 1 | 141 ± 2 | <0.0001 | 115 ± 1 | 126 ± 1 | <0.0001 |
| Added sugars (tsp eq) | 19.6 ± 0.1 | 19.3 ± 0.3 | 0.3875 | 18.0 ± 0.1 | 16.8 ± 0.3 | 0.0003 |
| Protein (g) | 68.8 ± 0.2 | 72.2 ± 0.7 | <0.0001 | 81.4 ± 0.2 | 87.1 ± 0.9 | <0.0001 |
| Total fat (g) | 73.1 ± 0.2 | 69.3 ± 0.6 | <0.0001 | 81.5 ± 0.2 | 74.6 ± 0.7 | <0.0001 |
| Cholesterol (mg) | 221 ± 2 | 214 ± 7 | 0.3622 | 288 ± 2 | 252 ± 6 | <0.0001 |
| Calcium (mg) | 1001 ± 6 | 1215 ± 17 | <0.0001 | 913 ± 4 | 1190 ± 13 | <0.0001 |
| Iron (mg) | 14.3 ± 0.1 | 14.0 ± 0.2 | 0.2915 | 15.1 ± 0.1 | 15.2 ± 0.2 | 0.4588 |
| Magnesium (mg) | 230 ± 1 | 253 ± 2 | <0.0001 | 293 ± 1 | 343 ± 3 | <0.0001 |
| Potassium (mg) | 2184 ± 10 | 2427 ± 26 | <0.0001 | 2666 ± 9 | 3074 ± 28 | <0.0001 |
| Sodium (mg) | 3113 ± 12 | 2937 ± 30 | <0.0001 | 3561 ± 9 | 3338 ± 30 | <0.0001 |
| Vitamin A, RAE (µg) | 586 ± 5 | 623 ± 15 | 0.0202 | 626 ± 8 | 698 ± 14 | <0.0001 |
| Thiamin (mg) | 1.55 ± 0.01 | 1.53 ± 0.02 | 0.3809 | 1.62 ± 0.01 | 1.65 ± 0.02 | 0.1538 |
| Folate, DFE (µg) | 522 ± 4 | 541 ± 12 | 0.1368 | 531 ± 3 | 583 ± 10 | <0.0001 |
| Vitamin B6 (mg) | 1.70 ± 0.01 | 1.71 ± 0.03 | 0.8478 | 2.02 ± 0.01 | 2.20 ± 0.04 | <0.0001 |
| Vitamin B12 (µg) | 4.93 ± 0.04 | 5.28 ± 0.10 | 0.0004 | 5.20 ± 0.05 | 5.90 ± 0.21 | 0.0016 |
| Vitamin C (mg) | 79.1 ± 1.0 | 85.4 ± 2.8 | 0.0271 | 83.7 ± 0.9 | 99.8 ± 3.1 | <0.0001 |
| Vitamin D (µg) | 5.77 ± 0.05 | 6.21 ± 0.17 | 0.0092 | 4.60 ± 0.05 | 5.23 ± 0.16 | 0.0003 |
| Variables | Children (2–18 Years) | Adults (≥19 Years) | ||||
|---|---|---|---|---|---|---|
| Non-Consumers (n = 24,322) | Consumers (n = 1676) | p Value for Difference | Non-Consumers (n = 37,598) | Consumers (n = 2200) | p Value for Difference | |
| % population below Estimated Average Requirement (EAR) | ||||||
| Calcium (mg) | 48.6 ± 0.7 | 15.4 ± 1.9 | <0.0001 | 48.3 ± 0.6 | 20.7 ± 1.7 | <0.0001 |
| Iron (mg) | 2.18 ± 0.13 | 1.57 ± 0.47 | 0.0770 | 5.01 ± 0.12 | 5.51 ± 0.61 | 0.3147 |
| Magnesium (mg) | 37.0 ± 0.6 | 14.2 ± 1.0 | <0.0001 | 58.0 ± 0.7 | 32.6 ± 1.5 | <0.0001 |
| Vitamin A, RAE (µg) | 26.2 ± 0.9 | 7.58 ± 1.60 | <0.0001 | 48.1 ± 0.8 | 29.5 ± 2.1 | 0.0004 |
| Thiamin (mg) | 1.34 ± 0.20 | 0.56 ± 0.27 | 0.0045 | 7.04 ± 0.41 | 5.47 ± 1.20 | 0.3987 |
| Folate, DFE (µg) | 3.82 ± 0.43 | 0.82 ± 0.52 | <0.0001 | 12.3 ± 0.5 | 9.34 ± 1.57 | 0.3099 |
| Vitamin B6 (mg) | 2.18 ± 0.32 | 1.25 ± 0.51 | 0.1048 | 12.9 ± 0.6 | 10.9 ± 1.4 | 0.4282 |
| Vitamin B12 (µg) | 0.86 ± 0.15 | 0.11 ± 0.08 | <0.0001 | 4.35 ± 0.33 | 0.76 ± 0.40 | <0.0001 |
| Vitamin C (mg) | 19.2 ± 0.9 | 9.39 ± 1.87 | 0.0240 | 45.1 ± 0.8 | 34.8 ± 1.8 | 0.0138 |
| Vitamin D (µg) | 91.1 ± 0.5 | 86.4 ± 2.0 | 0.3103 | 95.4 ± 0.3 | 93.2 ± 1.5 | 0.3487 |
| % population above Adequate Intake (AI) | ||||||
| Dietary fiber (g) | 0.62 ± 0.08 | 2.03 ± 0.71 | 0.0158 | 5.81 ± 0.29 | 16.8 ± 1.2 | <0.0001 |
| Potassium (mg) | 33.2 ± 0.8 | 53.1 ± 2.0 | <0.0001 | 31.3 ± 0.6 | 57.3 ± 1.6 | <0.0001 |
| Sodium (mg) | 99.9 ± 0.03 | 99.9 ± 0.1 | 0.1421 | 99.2 ± 0.1 | 99.2 ± 0.4 | 0.9242 |
| Children (2–18 Years) | Adults (≥19 Years) | |||||||
|---|---|---|---|---|---|---|---|---|
| Non-Consumers (n = 22,335) | Consumers (n = 1557) | β | p Value for Difference | Non-Consumers (n = 34,711) | Consumers (n = 2024) | β | p Value for Difference | |
| HEI-2015 total score | 46.6 ± 0.2 | 51.4 ± 0.5 | 4.8 ± 0.5 | <0.0001 | 50.2 ± 0.1 | 57.8 ± 0.4 | 7.6 ± 0.4 | <0.0001 |
| Component 1 (total vegetables) | 2.16 ± 0.02 | 2.05 ± 0.05 | −0.12 ± 0.06 | 0.0419 | 3.11 ± 0.01 | 3.10 ± 0.04 | −0.01 ± 0.04 | 0.7977 |
| Component 2 (greens and beans) | 0.83 ± 0.02 | 1.02 ± 0.07 | 0.19 ± 0.07 | 0.0082 | 1.46 ± 0.02 | 1.79 ± 0.06 | 0.33 ± 0.06 | <0.0001 |
| Component 3 (total fruit) | 2.45 ± 0.03 | 2.99 ± 0.08 | 0.54 ± 0.08 | <0.0001 | 2.06 ± 0.02 | 2.88 ± 0.06 | 0.82 ± 0.06 | <0.0001 |
| Component 4 (whole fruit) | 2.12 ± 0.03 | 2.85 ± 0.08 | 0.73 ± 0.08 | <0.0001 | 2.01 ± 0.02 | 3.05 ± 0.06 | 1.04 ± 0.06 | <0.0001 |
| Component 5 (whole grains) | 2.14 ± 0.04 | 2.55 ± 0.14 | 0.41 ± 0.14 | 0.0043 | 2.38 ± 0.03 | 3.29 ± 0.11 | 0.91 ± 0.11 | <0.0001 |
| Component 6 (dairy) | 6.89 ± 0.04 | 8.09 ± 0.10 | 1.20 ± 0.10 | <0.0001 | 4.95 ± 0.03 | 6.93 ± 0.07 | 1.98 ± 0.07 | <0.0001 |
| Component 7 (total protein foods) | 3.55 ± 0.02 | 3.40 ± 0.06 | −0.15 ± 0.06 | 0.0137 | 4.20 ± 0.01 | 4.20 ± 0.04 | −0.00 ± 0.04 | 0.9635 |
| Component 8 (seafood and plant protein) | 1.53 ± 0.02 | 1.86 ± 0.10 | 0.33 ± 0.10 | 0.0009 | 2.25 ± 0.02 | 2.74 ± 0.07 | 0.49 ± 0.11 | <0.0001 |
| Component 9 (fatty acid ratio) | 3.82 ± 0.04 | 3.51 ± 0.15 | −0.31 ± 0.15 | 0.0442 | 5.02 ± 0.03 | 4.70 ± 0.11 | −0.32 ± 0.11 | 0.0053 |
| Component 10 (sodium) | 4.91 ± 0.04 | 5.69 ± 0.13 | 0.78 ± 0.13 | <0.0001 | 4.16 ± 0.03 | 4.91 ± 0.10 | 0.75 ± 0.11 | <0.0001 |
| Component 11 (refined grain) | 5.20 ± 0.04 | 5.96 ± 0.13 | 0.76 ± 0.13 | <0.0001 | 6.15 ± 0.03 | 7.03 ± 0.10 | 0.88 ± 0.10 | <0.0001 |
| Component 12 (saturated fat) | 5.49 ± 0.04 | 5.92 ± 0.15 | 0.43 ± 0.16 | 0.0084 | 5.97 ± 0.03 | 6.46 ± 0.10 | 0.49 ± 0.10 | <0.0001 |
| Component 13 (added sugar) | 5.52 ± 0.04 | 5.51 ± 0.11 | −0.01 ± 0.11 | 0.9766 | 6.51 ± 0.04 | 6.78 ± 0.09 | 0.27 ± 0.09 | 0.0036 |
| Variables | Non-Consumer | Consumer | p Value for Difference | ||
|---|---|---|---|---|---|
| n | LSM ± SEM | n | LSM ± SEM | ||
| Children (2–18 years) | |||||
| BMI z-Score | 21,949 | 0.49 ± 0.02 | 1520 | 0.43 ± 0.04 | 0.2140 |
| Weight (kg) | 22,100 | 43.0 ± 0.2 | 1536 | 42.2 ± 0.4 | 0.0311 |
| Waist Circumference (cm) | 21,615 | 68.9 ±0.2 | 1456 | 68.1 ± 0.4 | 0.0635 |
| Adults (≥19 years) | |||||
| BMI (kg/m2) | 34,133 | 28.8 ± 0.1 | 1995 | 27.9 ± 0.2 | <0.0001 |
| Weight (kg) | 34,274 | 82.4 ± 0.2 | 1998 | 80.3 ± 0.6 | 0.0004 |
| Waist Circumference (cm) | 33,416 | 98.8 ± 0.2 | 1947 | 96.5 ± 0.5 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cifelli, C.J.; Agarwal, S.; Fulgoni, V.L., III. Association of Yogurt Consumption with Nutrient Intakes, Nutrient Adequacy, and Diet Quality in American Children and Adults. Nutrients 2020, 12, 3435. https://doi.org/10.3390/nu12113435
Cifelli CJ, Agarwal S, Fulgoni VL III. Association of Yogurt Consumption with Nutrient Intakes, Nutrient Adequacy, and Diet Quality in American Children and Adults. Nutrients. 2020; 12(11):3435. https://doi.org/10.3390/nu12113435
Chicago/Turabian StyleCifelli, Christopher J., Sanjiv Agarwal, and Victor L. Fulgoni, III. 2020. "Association of Yogurt Consumption with Nutrient Intakes, Nutrient Adequacy, and Diet Quality in American Children and Adults" Nutrients 12, no. 11: 3435. https://doi.org/10.3390/nu12113435
APA StyleCifelli, C. J., Agarwal, S., & Fulgoni, V. L., III. (2020). Association of Yogurt Consumption with Nutrient Intakes, Nutrient Adequacy, and Diet Quality in American Children and Adults. Nutrients, 12(11), 3435. https://doi.org/10.3390/nu12113435