Dietary Patterns, Their Nutrients, and Associations with Socio-Demographic and Lifestyle Factors in Older New Zealand Adults

 ,
,  , , , ,
, , , ,
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Socio-Demographic and Lifestyle Data
2.3. Dietary Assessment
2.4. Construction of the Dietary Patterns
2.5. Statistical Analysis
3. Results
3.1. Participants
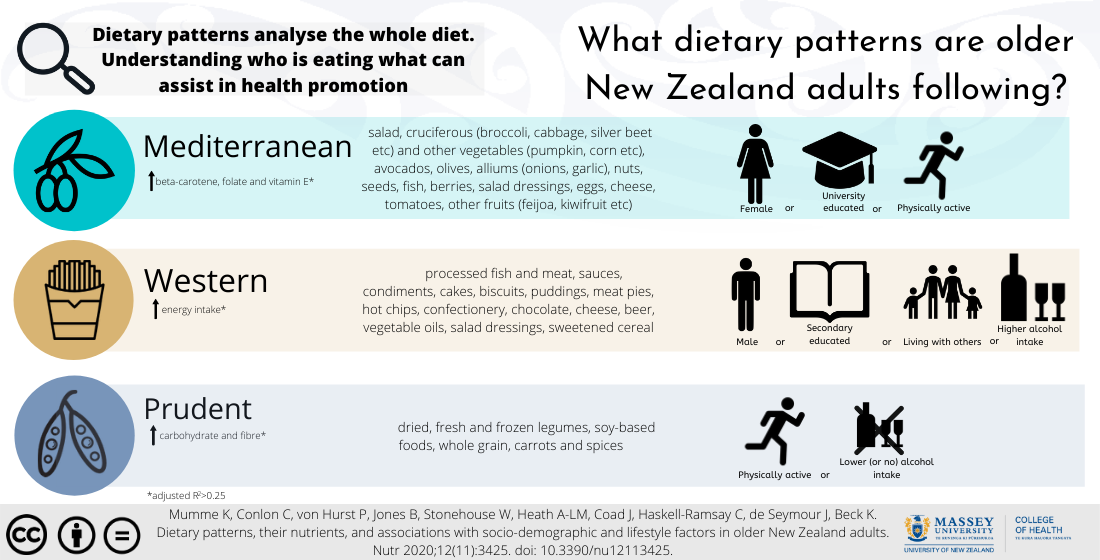
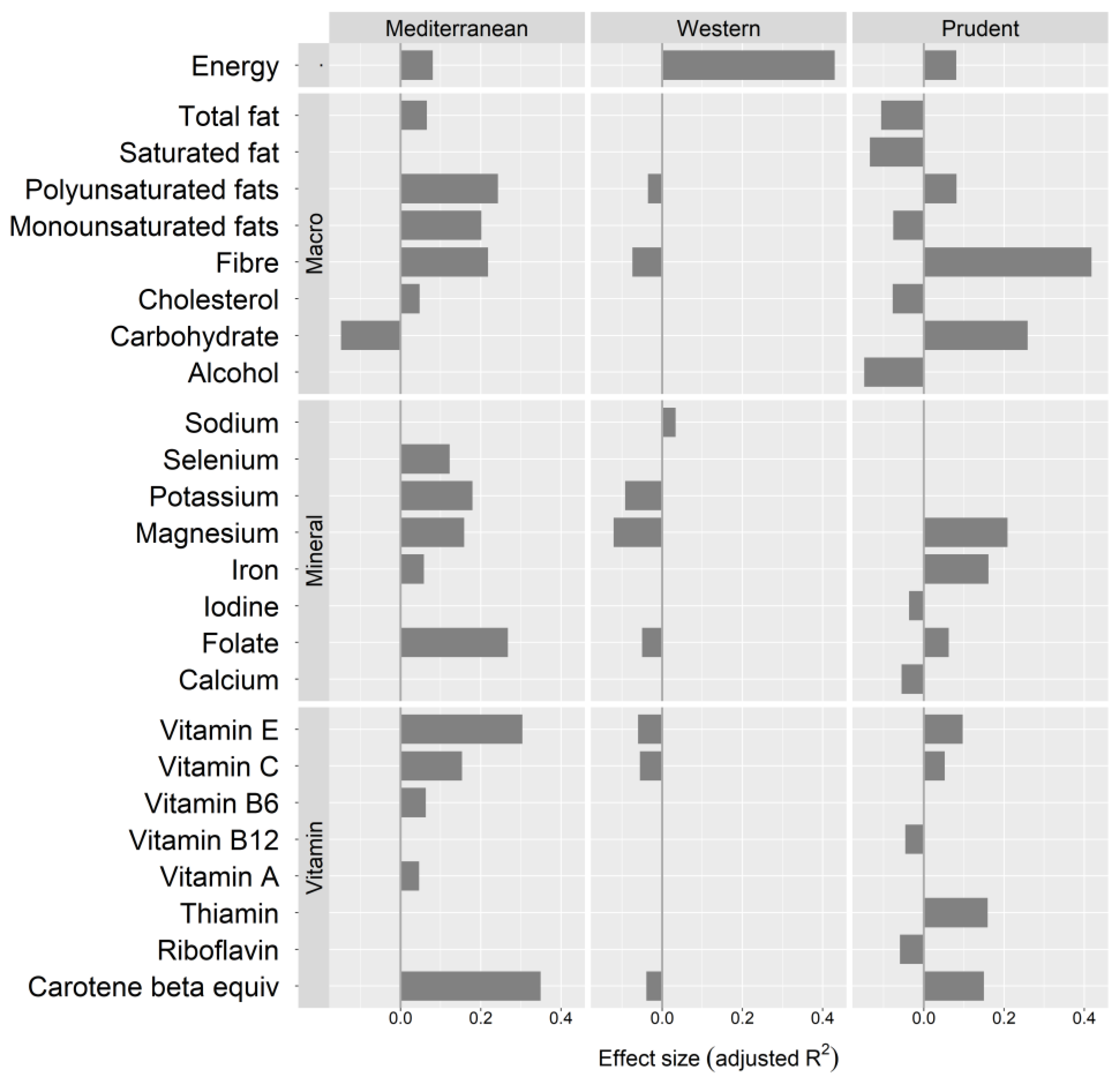
3.2. Dietary Patterns
3.3. Dietary Patterns and Socio-Demographic and Lifestyle Factors
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Sustainable Healthy Diets; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar] [CrossRef]
- World Health Organisation (WHO). World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Newby, P.K.; Tucker, K.L. Empirically derived eating patterns using factor or cluster analysis: A review. Nutr. Rev. 2004, 62, 177–203. [Google Scholar] [CrossRef] [PubMed]
- Fabiani, R.; Naldini, G.; Chiavarini, M. Dietary Patterns in Relation to Low Bone Mineral Density and Fracture Risk: A Systematic Review and Meta-Analysis. Adv. Nutr. 2019, 10, 219–236. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Maguire, B.; Brodaty, H.; O’Leary, F. Dietary Patterns and Cognitive Health in Older Adults: A Systematic Review. J. Alzheimer Dis. 2019, 67, 583–619. [Google Scholar] [CrossRef]
- Bloom, I.; Shand, C.; Cooper, C.; Robinson, S.; Baird, J. Diet Quality and Sarcopenia in Older Adults: A Systematic Review. Nutrients 2018, 10, 308. [Google Scholar] [CrossRef]
- Kennedy, E.T.; Ohls, J.; Carlson, S.; Fleming, K. The Healthy Eating Index: Design and applications. J. Am. Diet. Assoc. 1995, 95, 1103–1108. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Bamia, C.; Orfanos, P.; Ferrari, P.; Overvad, K.; Hundborg, H.H.; Tjønneland, A.; Olsen, A.; Kesse, E.; Boutron-Ruault, M.-C.; Clavel-Chapelon, F.; et al. Dietary patterns among older Europeans: The EPIC-Elderly study. Br. J. Nutr. 2005, 94, 100–113. [Google Scholar] [CrossRef]
- Andreeva, V.; Allès, B.; Feron, G.; Gonzalez, R.; Sulmont-Rossé, C.; Galan, P.; Hercberg, S.; Méjean, C. Sex-Specific Sociodemographic Correlates of Dietary Patterns in a Large Sample of French Elderly Individuals. Nutrients 2016, 8, 484. [Google Scholar] [CrossRef]
- Allès, B.; Samieri, C.; Lorrain, S.; Jutand, M.-A.; Carmichael, P.-H.; Shatenstein, B.; Gaudreau, P.; Payette, H.; Laurin, D.; Barberger-Gateau, P. Nutrient Patterns and Their Food Sources in Older Persons from France and Quebec: Dietary and Lifestyle Characteristics. Nutrients 2016, 8, 225. [Google Scholar] [CrossRef]
- Pryer, J.; Cook, A.; Shetty, P. Identification of groups who report similar patterns of diet among a representative national sample of British adults aged 65 years of age or more. Public Health Nutr. 2001, 4, 787–795. [Google Scholar] [CrossRef]
- Kell, K.P.; Judd, S.E.; Pearson, K.E.; Shikany, J.M.; Fernandez, J.R. Associations between socio-economic status and dietary patterns in US black and white adults. Br. J. Nutr. 2015, 113, 1792–1799. [Google Scholar] [CrossRef]
- Park, S.-Y.; Murphy, S.P.; Wilkens, L.R.; Yamamoto, J.F.; Sharma, S.; Hankin, J.H.; Henderson, B.E.; Kolonel, L.N. Dietary Patterns Using the Food Guide Pyramid Groups Are Associated with Sociodemographic and Lifestyle Factors: The Multiethnic Cohort Study. J. Nutr. 2005, 135, 843–849. [Google Scholar] [CrossRef]
- Cai, H.; Zheng, W.; Xiang, Y.-B.; Xu, W.; Yang, G.; Li, H.; Shu, X.O. Dietary patterns and their correlates among middle-aged and elderly Chinese men: A report from the Shanghai Men’s Health Study. Br. J. Nutr. 2007, 98, 1006–1013. [Google Scholar] [CrossRef]
- Markussen, M.S.; Veierød, M.B.; Kristiansen, A.L.; Ursin, G.; Andersen, L.F. Dietary patterns of women aged 50–69 years and associations with nutrient intake, sociodemographic factors and key risk factors for non-communicable diseases. Public Health Nutr. 2016, 19, 2024–2032. [Google Scholar] [CrossRef]
- Thorpe, M.G.; Milte, C.M.; Crawford, D.; McNaughton, S.A. A comparison of the dietary patterns derived by principal component analysis and cluster analysis in older Australians. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Bishop, N.J.; E Zuniga, K.; Ramirez, C.M. Latent profile analysis of dietary intake in a community-dwelling sample of older Americans. Public Health Nutr. 2019, 23, 243–253. [Google Scholar] [CrossRef]
- Beck, K.L.; Jones, B.; Ullah, I.; McNaughton, S.A.; Haslett, S.J.; Stonehouse, W. Associations between dietary patterns, socio-demographic factors and anthropometric measurements in adult New Zealanders: An analysis of data from the 2008/09 New Zealand Adult Nutrition Survey. Eur. J. Nutr. 2018, 57, 1421–1433. [Google Scholar] [CrossRef]
- National Health and Medical Research Council, Australian Government Department of Health and Ageing, New Zealand Ministry of Health. Nutrient reference values for Australia and New Zealand Executive Summary; National Health and Medical Research Council: Canberra, Australia, 2006; p. 28. Available online: https://www.nhmrc.gov.au/about-us/publications/nutrient-reference-values-australia-and-new-zealand-including-recommended-dietary-intakes (accessed on 7 November 2020).
- Mumme, K.D.; von Hurst, P.R.; Conlon, C.A.; Jones, B.; Haskell-Ramsay, C.F.; Stonehouse, W.; Heath, A.-L.M.; Coad, J.; Beck, K.L. Study protocol: Associations between dietary patterns, cognitive function and metabolic syndrome in older adults—A cross-sectional study. BMC Public Health 2019, 19, 535. [Google Scholar] [CrossRef]
- Mumme, K.; Conlon, C.; von Hurst, P.R.; Jones, B.; de Seymour, J.; Heath, A.L.; Stonehouse, W.; Coad, J.; Haskell-Ramsay, C.; Beck, K.L. Relative validity and reproducibility of a food frequency questionnaire for assessing dietary patterns and food group intake in older New Zealand adults: The REACH study. J. Acad. Nutr. Diet. under review.
- Exeter, D.J.; Zhao, J.; Crengle, S.; Lee, A.; Browne, M. The New Zealand Indices of Multiple Deprivation (IMD): A new suite of indicators for social and health research in Aotearoa, New Zealand. PLoS ONE 2017, 12, e0181260. [Google Scholar] [CrossRef]
- Parnell, W.R.; Reid, J.; Wilson, N.C.; McKenzie, J.; Russell, D.G. Food security: Is New Zealand a land of plenty? N. Z. Med. J. 2001, 114, 141–145. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; E Bauman, A.; Booth, M.L.; E Ainsworth, B.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Yu, A.D. Determining the Relative Validity and Reproducibility of a Food Frequency Questionnaire (FFQ) to Assess Nutrient Intake in Older Adults Living in New Zealand. Master’s Thesis, Massey University, Albany, New Zealand, 2019. [Google Scholar]
- The New Zealand Institute for Plant & Food Research Limited, Ministry of Health. New Zealand Food Composition Database 2017, New Zealand FOODfiles 2016 Version 01. Available online: https://www.foodcomposition.co.nz/foodfiles (accessed on 7 November 2020).
- Wijnhoven, H.A.H.; Elstgeest, L.E.M.; de Vet, H.C.W.; Nicolaou, M.; Snijder, M.B.; Visser, M. Development and validation of a short food questionnaire to screen for low protein intake in community-dwelling older adults: The Protein Screener 55+(Pro55+). PLoS ONE 2018, 13, e0196406. [Google Scholar] [CrossRef]
- Willett, W. Implications of Total Energy Intake for Epidemiologic Analyses. In Nutritional Epidemiology; Oxford University Press (OUP): New York, NY, USA, 2012; pp. 260–286. [Google Scholar]
- Newby, P.; Muller, D.; Hallfrisch, J.; Andres, R.; Tucker, K.L. Food patterns measured by factor analysis and anthropometric changes in adults. Am. J. Clin. Nutr. 2004, 80, 504–513. [Google Scholar] [CrossRef]
- The R Development Core Team. R: A Language and Environment for Statistical Computing Version 3.6.1; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: https://www.R-project.org/ (accessed on 7 November 2020).
- Psych: Procedures for Psychological, Psychometric, and Personality Research, Version 1.9.12. 2019; University, Evanston. Available online: https://CRAN.R-project.org/package=psych (accessed on 10 September 2019).
- Johnson, B.; Stevens, J.J. Exploratory and Confirmatory Factor Analysis of the School Level Environment Questionnaire (SLEQ). Learn. Environ. Res. 2001, 4, 325–344. [Google Scholar] [CrossRef]
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the Tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Fox, J.; Sanford, W. An R Companion to Applied Regression. Available online: https://socialsciences.mcmaster.ca/jfox/Books/Companion/ (accessed on 28 October 2020).
- Balemi, A.; Chandra, D.; Curran, J.; Deppa, B.; Forster, M.; McArdle, B.; Stevenson, B.; Wild, C. s20x: Functions for University of Auckland Course STATS 201/208 Data Analysis. R Package Version 3.1-29. Available online: https://CRAN.R-project.org/package=s20x (accessed on 28 October 2020).
- Baker, A.H.; Wardle, J. Sex differences in fruit and vegetable intake in older adults. Appetite 2003, 40, 269–275. [Google Scholar] [CrossRef]
- Mc Morrow, L.; Ludbrook, A.; MacDiarmid, J.; Olajide, D. Perceived barriers towards healthy eating and their association with fruit and vegetable consumption. J. Public Health 2016, 39, 330–338. [Google Scholar] [CrossRef]
- University of Otago and Ministry of Health. A Focus on Nutrition: Key Findings of the 2008/09 New Zealand Adult Nutrition Survey. Wellington: Minisity of Health. Available online: https://www.health.govt.nz/publication/focus-nutrition-key-findings-2008-09-nz-adult-nutrition-survey (accessed on 2 September 2011).
- Parmenter, K.; Waller, J.; Wardle, J. Demographic variation in nutrition knowledge in England. Health Educ. Res. 2000, 15, 163–174. [Google Scholar] [CrossRef]
- Whitelock, E.; Ensaff, H. On Your Own: Older Adults’ Food Choice and Dietary Habits. Nutrients 2018, 10, 413. [Google Scholar] [CrossRef]
- Parsons, T.J.; Papachristou, E.; Atkins, J.L.; Papacosta, O.; Ash, S.; Lennon, L.T.; Whincup, P.H.; Ramsay, S.E.; Wannamethee, S.G. Healthier diet quality and dietary patterns are associated with lower risk of mobility limitation in older men. Eur. J. Nutr. 2019, 58, 2335–2343. [Google Scholar] [CrossRef]
- Besora-Moreno, M.; Llauradó, E.; Tarro, L.; Solà, R. Social and Economic Factors and Malnutrition or the Risk of Malnutrition in the Elderly: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2020, 12, 737. [Google Scholar] [CrossRef] [PubMed]
- Granic, A.; Davies, K.; Adamson, A.J.; Kirkwood, T.; Hill, T.R.; Siervo, M.; Mathers, J.; Jagger, C. Dietary Patterns and Socioeconomic Status in the Very Old: The Newcastle 85+ Study. PLoS ONE 2015, 10, e0139713. [Google Scholar] [CrossRef]
- Hoenink, J.C.; Beulens, J.W.J.; Harbers, M.C.; Boer, J.M.A.; Dijkstra, S.C.; Nicolaou, M.; Van Der Schouw, Y.T.; Sluijs, I.; Verschuren, W.M.M.; Waterlander, W.; et al. To what extent do dietary costs explain socio-economic differences in dietary behavior? Nutr. J. 2020, 19, 1–12. [Google Scholar] [CrossRef]
- Wardle, J.F.C.; Parmenter, K.; Waller, J. Nutrition knowledge and food intake. Appetite 2000, 34, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Villegas, A.; Delgado-Rodriguez, M.; Martinez-Gonzalez, M.A.; De Irala, J. Gender, age, socio-demographic and lifestyle factors associated with major dietary patterns in the Spanish Project SUN (Seguimiento Universidad de Navarra). Eur. J. Clin. Nutr. 2003, 57, 285–292. [Google Scholar] [CrossRef]
- Meader, N.; King, K.; Moe-Byrne, T.; Wright, K.; Graham, H.; Petticrew, M.; Power, C.; White, M.; Sowden, A.J. A systematic review on the clustering and co-occurrence of multiple risk behaviours. BMC Public Health 2016, 16, 1–9. [Google Scholar] [CrossRef]
- Host, A.; McMahon, A.-T.; Walton, K.; Charlton, K. ‘While we can, we will’: Exploring food choice and dietary behaviour amongst independent older Australians. Nutr. Diet. 2016, 73, 463–473. [Google Scholar] [CrossRef]
- Wham, C.A.; Bowden, J.A. Eating for health: Perspectives of older men who live alone. Nutr. Diet. 2011, 68, 221–226. [Google Scholar] [CrossRef]
- Lim, S.-X.; Cox, V.; Rodrigues, N.; Colega, M.; Barton, S.; Conlon, C.; Wall, C.; Cutfield, W.; Chan, S.-Y.; Godfrey, K.; et al. Preconception Dietary Patterns and Their Sociodemographic and Lifestyle Correlates in a Multi-Country Cohort: The NiPPeR Study. Curr. Dev. Nutr. 2020, 4, 1437. [Google Scholar] [CrossRef]
- Thompson, J.M.D.; Wall, C.; Becroft, D.M.O.; Robinson, E.; Wild, C.J.; Mitchell, E.A. Maternal dietary patterns in pregnancy and the association with small-for-gestational-age infants. Br. J. Nutr. 2010, 103, 1665–1673. [Google Scholar] [CrossRef]
- Wall, C.R.; Gammon, C.S.; Bandara, D.K.; Grant, C.C.; Carr, P.E.A.; Morton, S.M.B. Dietary Patterns in Pregnancy in New Zealand—Influence of Maternal Socio-Demographic, Health and Lifestyle Factors. Nutrients 2016, 8, 300. [Google Scholar] [CrossRef]
- Wall, C.R.; Thompson, J.M.; Robinson, E.; Mitchell, E.A. Dietary patterns of children at 3.5 and 7 years of age: A New Zealand birth cohort study. Acta Paediatr. 2012, 102, 137–142. [Google Scholar] [CrossRef]
- Noble, N.; Paul, C.L.; Turon, H.; Oldmeadow, C. Which modifiable health risk behaviours are related? A systematic review of the clustering of Smoking, Nutrition, Alcohol and Physical activity (‘SNAP’) health risk factors. Prev. Med. 2015, 81, 16–41. [Google Scholar] [CrossRef]
- Prendergast, K.; Mackay, L.; Schofield, G.M. The Clustering of Lifestyle Behaviours in New Zealand and their Relationship with Optimal Wellbeing. Int. J. Behav. Med. 2016, 23, 571–579. [Google Scholar] [CrossRef]
- Esmaili, H.; Yusof, R.M.; Abu Saad, H.; Ghaemian, A.; Zad, N.D. Association of Dietary Patterns with Sociodemographic and Health-related Factors among Coronary Artery Disease (CAD) Patients. Ecol. Food Nutr. 2014, 54, 4–19. [Google Scholar] [CrossRef]
- Krieger, J.-P.; Pestoni, G.; Cabaset, S.; Brombach, C.; Sych, J.; Schader, C.; Faeh, D.; Rohrmann, S. Dietary Patterns and Their Sociodemographic and Lifestyle Determinants in Switzerland: Results from the National Nutrition Survey menuCH. Nutrients 2018, 11, 62. [Google Scholar] [CrossRef]
- Whichelow, M.J.; Prevost, A.T. Dietary patterns and their associations with demographic, lifestyle and health variables in a random sample of British adults. Br. J. Nutr. 1996, 76, 17–30. [Google Scholar] [CrossRef]
- Lennernäs, M.; Fjellström, C.; Becker, W.; Giachetti, I.; Schmitt, A.; De Winter, A.R.; Kearney, M. Influences on food choice perceived to be important by nationally-representative samples of adults in the European Union. Eur. J. Clin. Nutr. 1997, 51, S8. [Google Scholar] [PubMed]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef]
- Hu, F.B.; Rimm, E.; A Smith-Warner, S.; Feskanich, D.; Stampfer, M.J.; Ascherio, A.; Sampson, L.; Willett, W.C. Reproducibility and validity of dietary patterns assessed with a food-frequency questionnaire. Am. J. Clin. Nutr. 1999, 69, 243–249. [Google Scholar] [CrossRef] [PubMed]
- McNaughton, S.A.; Mishra, G.D.; Bramwell, G.; Paul, A.A.; Wadsworth, M.E.J. Comparability of dietary patterns assessed by multiple dietary assessment methods: Results from the 1946 British Birth Cohort. Eur. J. Clin. Nutr. 2004, 59, 341–352. [Google Scholar] [CrossRef]
- Allès, B.; Samieri, C.; Jutand, M.-A.; Carmichael, P.-H.; Shatenstein, B.; Gaudreau, P.; Ferland, G.; Barberger-Gateau, P.; Laurin, D. Nutrient Patterns, Cognitive Function, and Decline in Older Persons: Results from the Three-City and NuAge Studies. Nutrients 2019, 11, 1808. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Food Groups (n = 57) | Food Items |
|---|---|
| Beer | ‘Beer, lager, cider (all varieties)’ |
| Other alcohol | ‘Port, sherry, liquors’, ‘ready to drink alcoholic beverages’, ‘spirits e.g., gin, brandy, whiskey, vodka’, ‘white wine’ |
| Red wine | ‘Red wine’ |
| Bran cereal | ‘Bran-based cereals, muesli, porridges—e.g., rolled oats, oat bran, oatmeal, All Bran, Sultana bran’ |
| Refined grains | ‘White bread and rolls, including sliced and specialty breads such as foccacia, panini, pita, naan, chapatti, ciabatta, Turkish, English muffin, crumpets, pizza bases, wraps, tortillas, burrito, roti, rewena bread’, ‘white pasta, noodles e.g., spaghetti, canned spaghetti, vermicelli, egg noodles, rice noodles, instant noodles’, ‘white rice’ |
| Snacks | ‘Crackers e.g., crisp bread, water crackers, rice cakes, cream crackers, Cruskits, Mealmates, vitawheat’, ‘muesli or cereal bar (all varieties)’ |
| Sweetened cereals | ‘Other breakfast cereals e.g., Special K, Light and tasty’, ‘sweetened cereals e.g., Nutrigrain, Fruit Loops, Honey Puffs, Frosties, Milo cereal, CocoPops’, ‘Weetbix, cornflakes or rice bubbles’ |
| Whole grains | ‘Brown rice’, ‘couscous, polenta, congee, Bulgur wheat, quinoa e.g., tabbouleh’, ‘whole grain or multi grain bread and rolls including sliced and specialty breads, whole meal or wheat meal bread and rolls including sliced and specialty breads’, ‘whole meal pasta, noodles’ |
| Cheese | ‘Cheese e.g., Cheddar, Colby, Edam, Tasty, blue vein, camembert, parmesan, gouda, feta, mozzarella, brie, processed’, ‘cottage cheese, ricotta cheese’ |
| Creamy dairy | ‘Cream, sour cream, cream cheese, cheese spreads’ |
| Milk | ‘Cow’s milk, including milk as a drink, milk added to drinks (e.g., milky coffees), milk added to cereal’ |
| Other milks (non-dairy) | ‘Soy milk, coconut milk, rice milk, almond milk’ |
| Sweetened dairy products | ‘Ice cream’, ‘milk-based puddings e.g., rice pudding, custard, semolina, instant puddings, dairy food’, ‘smoothies, milk shakes (made from milk, yoghurt, ice cream), milk shakes, flavoured milk’ |
| Yoghurt | ‘Yoghurt’ |
| Dried legumes | ‘Beans (canned or dried) e.g., black beans, butter beans, haricot beans, kidney beans, cannellini beans, refried beans, baked beans, chilli beans’, ‘peas and lentils e.g., chickpeas, hummus, falafels, split peas, cow peas, dahl’ |
| Eggs | ‘Eggs—boiled, poached, raw’, ‘eggs—fried, scrambled, egg-based dishes including quiche, soufflés, frittatas, omelettes’ |
| Nuts, seeds | ‘Nut butters or spreads e.g., peanut butter, almond butter, pesto’, ‘nuts e.g., peanuts, mixed nuts, macadamias, pecan, hazelnuts, brazil nuts, walnuts, cashews, pistachios, almonds’, ‘seeds e.g., pumpkin seeds, sunflower seeds, pinenuts, sesame seeds, tahini’ |
| Soy-based foods | ‘Tofu, soybeans, tempeh, vegetarian sausages/meat, vegetarian burger patty, textured vegetable protein’ |
| Oily fish | ‘Albacore tuna, salmon, sardines, herring, kahawai, swordfish, carp, dogfish, gemfish, alfonsino, rudderfish, anchovies’, ‘mackerel, snapper, oreo, barracouta, trevally, dory, trout, eel’ |
| Processed fish | ‘Crumbed fish e.g., patties, cakes, fingers, nuggets’, ‘fish fried in batter (from fish & chips shop)’ |
| White fish, shellfish | ‘Green mussels, squid’, ‘shellfish e.g., cockles, kina, oysters, paua, scallops, shrimp/prawn, pipi, roe’, ‘tuna (canned), hoki, gurnard, hake, kingfish, cod, tarakihi, groper, flounder’ |
| Apples, pears | ‘Apples, pears, nashi pears’ |
| Avocados, olives | ‘Avocado’, ‘olives’ |
| Bananas | ‘Banana’ |
| Berries | ‘Strawberries, blackberries, cherries, blueberries, boysenberries, loganberries, cranberries, gooseberries, raspberries (fresh, frozen, canned)’ |
| Citrus fruit | ‘Citrus fruits e.g., orange, tangelo, tangerine, mandarin, grapefruit, lemon, lime’ |
| Dried fruit | ‘Dried fruit e.g., sultanas, raisins, currants, figs, apricots, prunes, dates’ |
| Other fruit | ‘All other fruit e.g., feijoa, persimmon, tamarillo, kiwifruit, grapes, mango, melon, watermelon, pawpaw, papaya, pineapple, rhubarb’ |
| Stone fruit | ‘Stone fruit e.g., apricots, nectarines, peaches, plums, lychees’ |
| Poultry | ‘Chicken, turkey or duck e.g., roast, steak, fried, steamed, BBQ, casserole, stew, stir fry, curry, mince dishes, frozen dinners’ |
| Processed meat | ‘Corn beef (canned), boil up, pork bones, lamb flaps, povi masima’, ‘ham, bacon, luncheon sausage, salami, pastrami, other processed meat’, ‘sausages, frankfurters, cheerios, hot dogs’ |
| Red meat | ‘Beef, lamb, hogget, mutton, pork, veal e.g., roast, steak, fried, chops, schnitzel, silverside, casserole, stew, stir fry, curry, BBQ, hamburger meat, mince dishes, frozen dinners’, ‘liver, kidney, other offal (including pate)’ |
| Butter, coconut | ‘Butter, ghee’, ‘coconut cream’, ‘coconut oil’ |
| Cakes, biscuits and puddings | ‘Biscuits, chocolate or cream filled’, ‘biscuits, plain’, ‘cakes, slices, pastries’, ‘non-milk based puddings e.g., pavlova, sweet pastries, fruit pies, trifle’, ‘pancakes, waffles, sweet buns, scones, sweet muffins, fruit bread, croissants, doughnuts, brioche’ |
| Chocolate | ‘Chocolate (all other varieties)’ |
| Confectionery | ‘Jam, marmalade, honey, syrups, sweet spreads or preserves’, ‘sugar (all varieties) added to food/drinks’, ‘sweets, lollies’ |
| Salad dressings | ‘Creamy dressings e.g., mayonnaise, tartar, thousand island, ranch dressing’, ‘light dressings e.g., French and Italian dressing, balsamic vinegar’ |
| Meat pies, chips | ‘Hot potato chips, French fries, wedges’, ‘meat pies, sausage rolls’, ‘potato crisps’ |
| Sauces, condiments | ‘Pickles, chutney, mustard’, ‘tomato sauce, barbeque sauce, sweet chilli sauce’, ‘white sauce, cheese sauce, gravies’ |
| Soup | ‘Soup, homemade or canned’ |
| Spices | ‘Spices e.g., turmeric, ginger, cinnamon’ |
| Vegetable oils | ‘Margarine’, ‘vegetable oils’ |
| Yeast spreads | ‘Marmite, vegemite’ |
| Diet drinks | ‘Diet soft/fizzy drinks e.g., Sprite Zero, Diet Coke, Coke Zero’, ‘low calorie cordials’ |
| Juices | ‘Fruit and vegetable juices (all varieties)’ |
| Sugary drinks | ‘Cordials including syrups, powders e.g., Raro’, ‘energy drinks e.g., Red Bull, V’, ‘hot chocolate, drinking chocolate, Cocoa, Ovaltine, Nesquik, Milo’, ‘soft/fizzy drinks e.g., Sprite, Coke’, ‘sports drinks e.g., Powerade’ |
| Tea, coffee | ‘Coffee (all varieties)’, ‘herbal tea, fruit tea’, ‘tea’ |
| Water | ‘Water including tap, bottled or sparkling water’ |
| Alliums | ‘Onions, leeks, garlic’ |
| Carrots | ‘Carrots’ |
| Cruciferous vegetables | ‘Broccoli, cauliflower, Brussel sprouts, cabbage (all varieties)’ |
| Fresh, frozen legumes | ‘Green beans, broad beans, runner beans’, ‘peas, green’ |
| Leafy cruciferous vegetables | ‘Green leafy vegetables e.g., spinach, silver beet, swiss chard, watercress, puha, whitloof, chicory, kale, chard, collards, chinese kale, bok choy, taro leaves (palusami)’ |
| Other vegetables | ‘All other vegetables e.g., corn, pumpkin, mushrooms, capsicum, peppers, courgette, zucchini, gherkins, marrow, squash, asparagus, radish, eggplant, artichoke’ |
| Root vegetables | ‘Kumara, taro, green banana, cassava e.g., boiled, mashed, baked, roasted’, ‘other root vegetables e.g., yams, parsnip, swedes, beetroot, turnips’, ‘potato e.g., boiled, mashed, baked, jacket, instant, roasted’ |
| Salad vegetables | ‘Salad vegetables e.g., lettuce, cucumber, celery, sprouts’ |
| Tomatoes | ‘Tomatoes (all varieties)’ |
| Characteristic | Total (n = 367) Mean ± SD, Median (25, 75) or n (%) | Male (n = 132) Mean ± SD, Median (25, 75) or n (%) | Female (n = 235) Mean ± SD, Median (25, 75) or n (%) |
|---|---|---|---|
| Age (years) ‡,** | 69.7 ± 2.6 | 70.1 ± 2.4 | 69.4 ± 2.6 |
| Highest level of education ‡,*** | |||
| Secondary a,‡ | 83 (23) | 18 (14) | 65 (28) |
| Post-secondary | 148 (40) | 49 (37) | 99 (42) |
| University ‡ | 136 (37) | 65 (49) | 71 (30) |
| Employed (paid or volunteer) | 179 (49) | 55 (42) | 124 (53) |
| Ethnicity | |||
| Asian | 11 (3) | 5 (4) | 6 (3) |
| Māori/Pacific | 10 (3) | 5 (4) | 5 (2) |
| NZ European and other | 346 (94) | 122 (92) | 224 (95) |
| Index of Multiple Deprivation score b | 3831 ± 2,766 | 3943 ± 2,939 | 3768 ± 2668 |
| Dietary pattern score | |||
| ‘Mediterranean’ ‡,*** | 0.00 ± 1.00 | −0.22 ± 1.07 | 0.13 ± 0.94 |
| ‘Western’ ‡,** | 0.00 ± 1.00 | 0.45 ± 1.10 | −0.25 ± 0.84 |
| ‘prudent’ | 0.00 ± 1.00 | −0.03 ± 1.20 | 0.02 ± 0.87 |
| Living situation ‡,*** | |||
| alone | 107 (29) | 18 (14) | 89 (38) |
| with others | 260 (71) | 114 (86) | 146 (62) |
| Physical activity (MET minutes/week) c | 3097 (1680, 5118) | 3086 (1774, 5464) | 3107 (1663, 5037) |
| Smoker | |||
| Yes (current or past) | 78 (21) | 29 (22) | 49 (21) |
| No | 289 (79) | 103 (78) | 186 (79) |
| Daily energy intake (kJ) ‡,** | 7578 ± 2129 | 8044 ± 2275 | 7315 ± 2000 |
| Daily alcohol beverage intake (energy adjusted g/day) ‡,*** | 62 (18, 120) | 100 (33, 212) | 50 (12, 88) |
| Food security | |||
| Secure | 352 (96) | 129 (98) | 223 (95) |
| Moderately secure | 13 (4) | 2 (2) | 11 (5) |
| Insecure | 2 (1) | 1 (1) | 1 (0) |
| Food Groups (n = 57) a,b,c | Mediterranean | Prudent | Western |
|---|---|---|---|
| Salad vegetables | 0.64 | ||
| Leafy cruciferous vegetables | 0.57 | 0.23 | |
| Other vegetables | 0.56 | ||
| Avocados, olives | 0.51 | ||
| Alliums | 0.47 | 0.15 | |
| Nuts, seeds | 0.45 | 0.26 | |
| White fish, shellfish | 0.45 | ||
| Oily fish | 0.42 | ||
| Berries | 0.41 | ||
| Water | 0.40 | 0.18 | −0.16 |
| Salad dressings | 0.39 | −0.18 | 0.35 |
| Cruciferous vegetables | 0.39 | 0.24 | |
| Eggs | 0.34 | ||
| Cheese | 0.33 | −0.18 | 0.34 |
| Tomatoes | 0.33 | ||
| All other fruit | 0.32 | 0.22 | |
| Dried legumes | 0.15 | 0.68 | |
| Soy-based foods | 0.65 | ||
| Fresh, frozen legumes | 0.54 | 0.20 | |
| Whole grains | 0.51 | 0.24 | |
| Carrots | 0.28 | 0.48 | |
| Spices | 0.23 | 0.30 | |
| Processed meats | −0.29 | 0.59 | |
| Sauces, condiments | 0.23 | 0.52 | |
| Cakes, biscuits and puddings | −0.26 | 0.51 | |
| Meat pies, chips | −0.28 | 0.47 | |
| Processed fish | 0.41 | ||
| Confectionery | −0.22 | 0.39 | |
| Vegetable oils | 0.36 | ||
| Beer | −0.21 | 0.35 | |
| Chocolate | 0.35 | ||
| Sweetened cereal | −0.19 | 0.30 | |
| Stone fruit | 0.29 | 0.18 | |
| Apples, pears | 0.26 | 0.28 | |
| Dried fruit | 0.23 | 0.25 | |
| Butter, coconut | 0.23 | −0.20 | |
| Yoghurt | 0.19 | 0.16 | |
| Root vegetables | 0.17 | 0.29 | 0.24 |
| Red wine | 0.15 | −0.27 | 0.16 |
| Refined grains | 0.29 | 0.21 | |
| Other milks (non-dairy) | 0.28 | ||
| Poultry | 0.21 | 0.15 | |
| Citrus fruit | 0.21 | ||
| Bran cereal | 0.20 | ||
| Bananas | 0.17 | ||
| Tea, coffee | −0.21 | 0.21 | |
| Other alcohol | −0.21 | ||
| Red meat | 0.29 | ||
| Diet drinks | 0.28 | ||
| Sugary drinks | 0.25 | ||
| Milk | 0.25 | ||
| Snacks | 0.24 | ||
| Sweetened dairy products | 0.20 | ||
| Yeast spreads | |||
| Creamy dairy | |||
| Juices | |||
| Soup | |||
| score range | −2.32 to 4.26 | −1.93 to 3.83 | −2.49 to 8.31 |
| variance explained | 7.20 | 5.30 | 5.60 |
| Eigenvalue | 4.12 | 3.04 | 3.18 |
| Mediterranean Pattern | |||
| Coefficient | Estimate | Standard Error | p-Value |
| Intercept | −0.37 | 0.14 | 0.007 |
| Sex male | −0.42 | 0.11 | 0.001 |
| Physical activity medium | 0.21 | 0.12 | 0.097 |
| Physical activity high | 0.42 | 0.12 | < 0.001 |
| Education post-secondary | 0.39 | 0.13 | 0.004 |
| Education university | 0.44 | 0.14 | 0.002 |
| Reference group (Intercept) is female, low physical activity, and secondary education Adjusted R2 = 0.07, p-value < 0.001 | |||
| Western Pattern | |||
| Coefficient | Estimate | Standard Error | p-Value |
| Intercept | −0.37 | 0.12 | 0.003 |
| Sex male | 1.22 | 0.25 | < 0.001 |
| Education post-secondary | 0.13 | 0.15 | 0.371 |
| Education university | 0.33 | 0.16 | 0.035 |
| Living alone | −0.30 | 0.11 | 0.006 |
| Alcohol intake | 0.00 | 0.00 | 0.005 |
| Male: Education post-secondary | −0.86 | 0.29 | 0.003 |
| Male: Education university | −0.83 | 0.29 | 0.004 |
| Reference group (Intercept) is female, secondary education, living with others, and lower alcohol intake Adjusted R2 = 0.16, p-value < 0.001 | |||
| Prudent Pattern | |||
| Coefficient | Estimate | Standard Error | p-Value |
| Intercept | 0.13 | 0.09 | 0.155 |
| Physical activity medium | 0.09 | 0.12 | 0.425 |
| Physical activity high | 0.37 | 0.12 | 0.002 |
| Alcohol intake | −0.00 | 0.00 | < 0.001 |
| Reference group (Intercept) is low physical activity and high alcohol intake Adjusted R2 = 0.15, p-value < 0.001 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mumme, K.; Conlon, C.; von Hurst, P.; Jones, B.; Stonehouse, W.; Heath, A.-L.M.; Coad, J.; Haskell-Ramsay, C.; de Seymour, J.; Beck, K. Dietary Patterns, Their Nutrients, and Associations with Socio-Demographic and Lifestyle Factors in Older New Zealand Adults. Nutrients 2020, 12, 3425. https://doi.org/10.3390/nu12113425
Mumme K, Conlon C, von Hurst P, Jones B, Stonehouse W, Heath A-LM, Coad J, Haskell-Ramsay C, de Seymour J, Beck K. Dietary Patterns, Their Nutrients, and Associations with Socio-Demographic and Lifestyle Factors in Older New Zealand Adults. Nutrients. 2020; 12(11):3425. https://doi.org/10.3390/nu12113425
Chicago/Turabian StyleMumme, Karen, Cathryn Conlon, Pamela von Hurst, Beatrix Jones, Welma Stonehouse, Anne-Louise M. Heath, Jane Coad, Crystal Haskell-Ramsay, Jamie de Seymour, and Kathryn Beck. 2020. "Dietary Patterns, Their Nutrients, and Associations with Socio-Demographic and Lifestyle Factors in Older New Zealand Adults" Nutrients 12, no. 11: 3425. https://doi.org/10.3390/nu12113425
APA StyleMumme, K., Conlon, C., von Hurst, P., Jones, B., Stonehouse, W., Heath, A.-L. M., Coad, J., Haskell-Ramsay, C., de Seymour, J., & Beck, K. (2020). Dietary Patterns, Their Nutrients, and Associations with Socio-Demographic and Lifestyle Factors in Older New Zealand Adults. Nutrients, 12(11), 3425. https://doi.org/10.3390/nu12113425