Dietary Protein Intake Patterns and Inadequate Protein Intake in Older Adults from Four Countries

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Data Acquisition
2.2. Protein Intake Variables
2.3. Inadequate Protein Intake
2.4. Statistics
3. Results
3.1. Demographic Data
3.2. Protein Intake
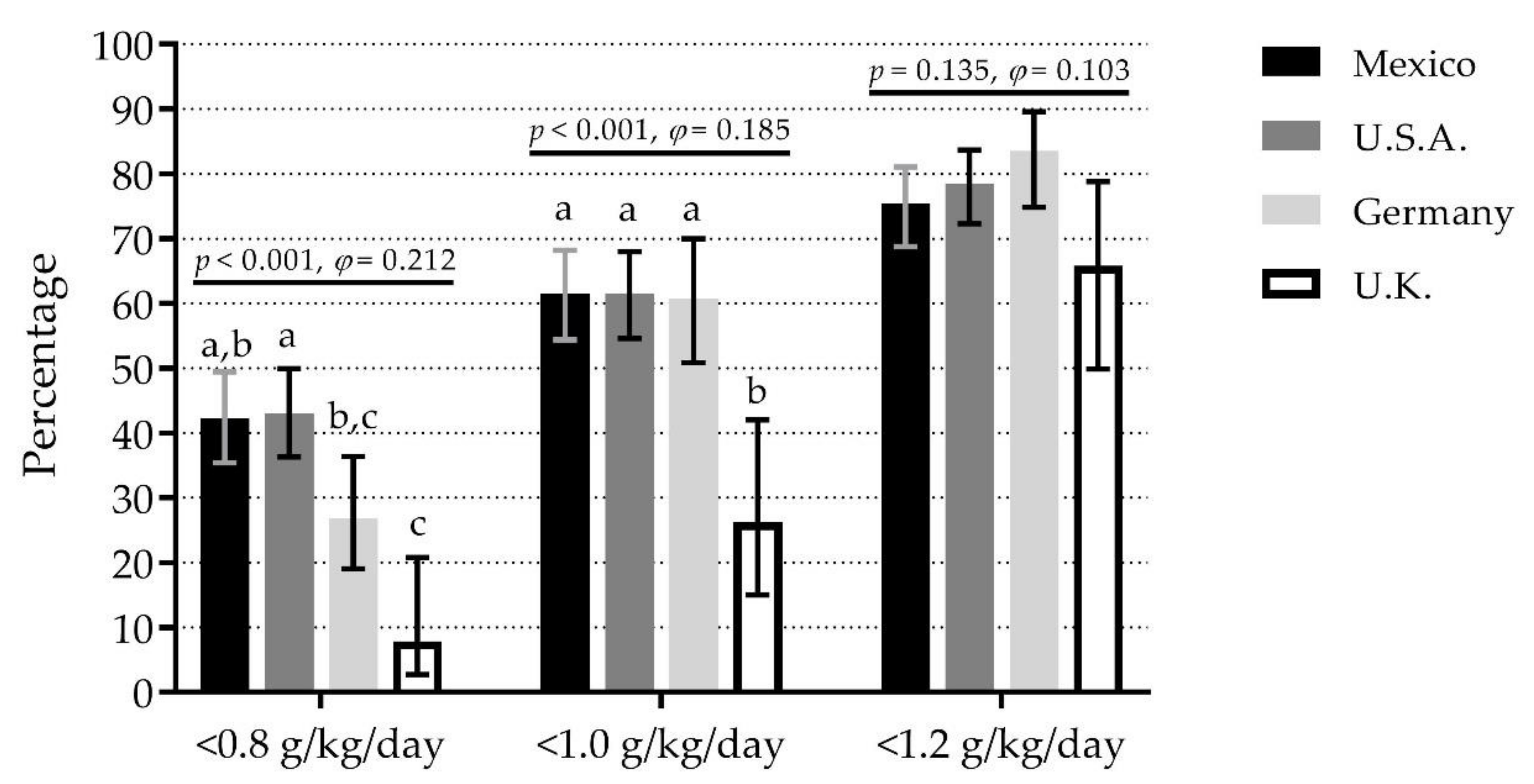
3.3. Inadequate Protein Intake per Day
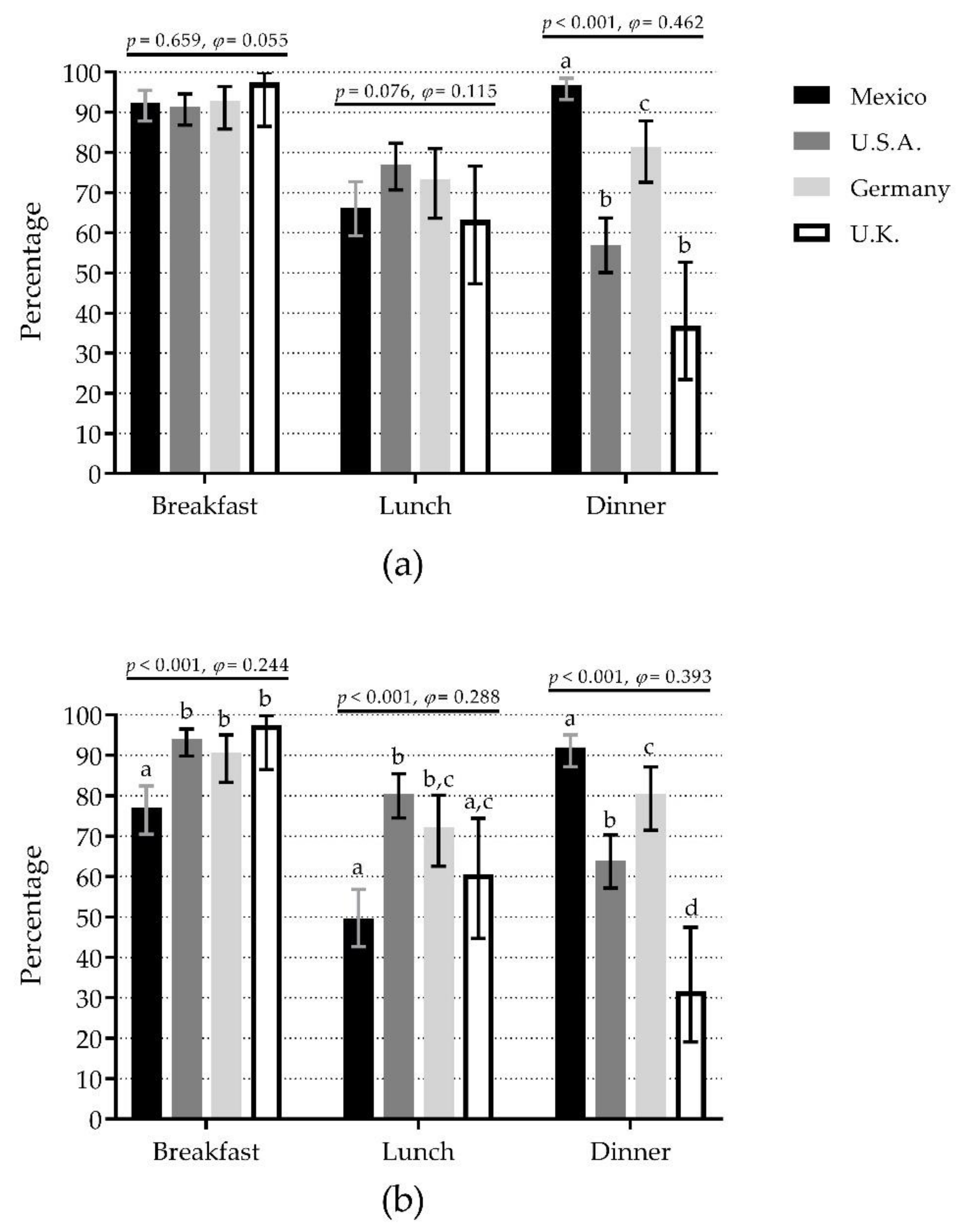
3.4. Inadequate Protein Intake per Meal
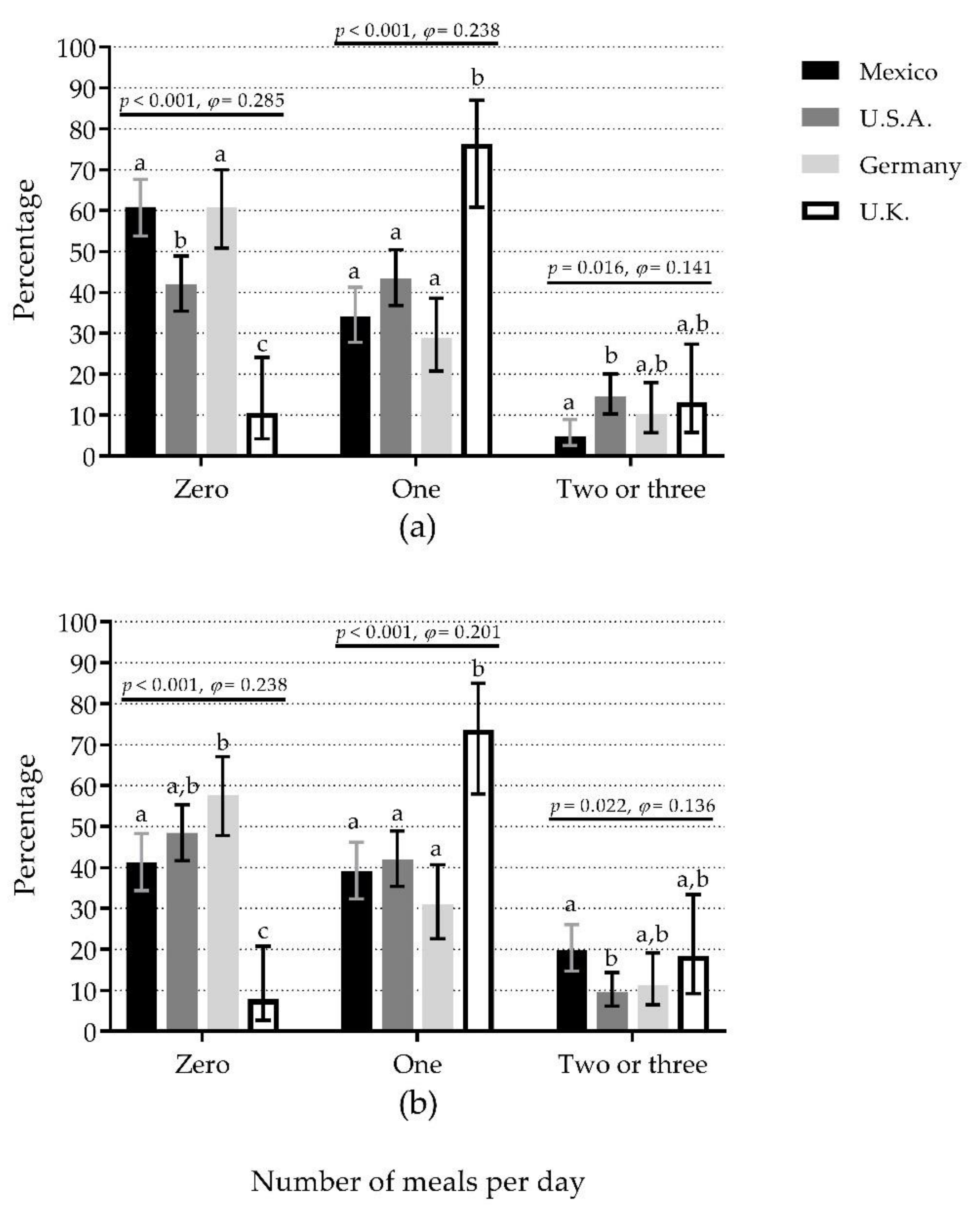
3.5. Number of Meals per Day with Adequate Protein Content
3.6. IPI Combined Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jafarinasabian, P.; Inglis, J.E.; Reilly, W.; Kelly, O.J.; Ilich, J.Z. Aging Human Body: Changes in Bone, Muscle and Body Fat with Consequent Changes in Nutrient Intake. J. Endocrinol. 2017, 234, R37–R51. [Google Scholar] [CrossRef] [PubMed]
- Fulop, T.; Larbi, A.; Khalil, A.; Cohen, A.A.; Witkowski, J.M. Are We Ill Because We Age? Front. Physiol. 2019, 10, 1508. [Google Scholar] [CrossRef] [PubMed]
- Seals, D.R.; Justice, J.N.; Larocca, T.J. Physiological Geroscience: Targeting Function to Increase Healthspan and Achieve Optimal Longevity. J. Physiol. 2016, 594, 2001–2024. [Google Scholar] [CrossRef]
- Martone, A.M.; Marzetti, E.; Calvani, R.; Picca, A.; Tosato, M.; Santoro, L.; Di Giorgio, A.; Nesci, A.; Sisto, A.; Santoliquido, A.; et al. Exercise and Protein Intake: A Synergistic Approach against Sarcopenia. BioMed Res. Int. 2017, 2017, 2672435. [Google Scholar] [CrossRef]
- Robinson, S.M.; Reginster, J.Y.; Rizzoli, R.; Shaw, S.C.; Kanis, J.A.; Bautmans, I.; Bischoff-Ferrari, H.; Bruyère, O.; Cesari, M.; Dawson-Hughes, B.; et al. Does Nutrition Play a Role in the Prevention and Management of Sarcopenia? Clin. Nutr. 2018, 37, 1121–1132. [Google Scholar] [CrossRef] [PubMed]
- Tieland, M.; Trouwborst, I.; Clark, B.C. Skeletal Muscle Performance and Ageing. J. Cachexia. Sarcopenia Muscle 2018, 9, 3–19. [Google Scholar] [CrossRef]
- Landi, F.; Calvani, R.; Tosato, M.; Martone, A.M.; Ortolani, E.; Savera, G.; D’Angelo, E.; Sisto, A.; Marzetti, E. Protein Intake and Muscle Health in Old Age: From Biological Plausibility to Clinical Evidence. Nutrients 2016, 8, 295. [Google Scholar] [CrossRef]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-Based Recommendations for Optimal Dietary Protein Intake in Older People: A Position Paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Coelho-Júnior, H.; Milano-Teixeira, L.; Rodrigues, B.; Bacurau, R.; Marzetti, E.; Uchida, M. Relative Protein Intake and Physical Function in Older Adults: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2018, 10, 1330. [Google Scholar] [CrossRef]
- Mendonça, N.; Granic, A.; Hill, T.R.; Siervo, M.; Mathers, J.C.; Kingston, A.; Jagger, C. Protein Intake and Disability Trajectories in Very Old Adults: The Newcastle 85+ Study. J. Am. Geriatr. Soc. 2019, 67, 50–56. [Google Scholar] [CrossRef]
- Murphy, C.H.; Oikawa, S.Y.; Phillips, S.M. Dietary Protein to Maintain Muscle Mass in Aging: A Case for per-Meal Protein Recommendations. J. Frailty Aging 2016, 5, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Hudson, J.L.; Bergia, R.E.I.; Campbell, W.W. Protein Distribution and Muscle-Related Outcomes: Does the Evidence Support the Concept? Nutrients 2020, 12, 1441. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.Y.; Schutzler, S.; Schrader, A.M.; Spencer, H.J.; Azhar, G.; Wolfe, R.R.; Ferrando, A.A. Protein Intake Distribution Pattern Does Not Affect Anabolic Response, Lean Body Mass, Muscle Strength or Function over 8 Weeks in Older Adults: A Randomized-Controlled Trial. Clin. Nutr. 2018, 37, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Gingrich, A.; Spiegel, A.; Kob, R.; Schoene, D.; Skurk, T.; Hauner, H.; Siebe, C.C.; Volkert, D.; Kiesswetter, E. Amount, Distribution, and Quality of Protein Intake Are Not Associated with Muscle Mass, Strength, and Power in Healthy Older Adults without Functional Limitations—An Enable Study. Nutrients 2017, 9, 1358. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Loprinzi, P.D.; Murphy, C.H.; Phillips, S.M. Per Meal Dose and Frequency of Protein Consumption Is Associated with Lean Mass and Muscle Performance. Clin. Nutr. 2016, 35, 1506–1511. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.R.; Churchward-Venne, T.A.; Witard, O.; Breen, L.; Burd, N.A.; Tipton, K.D.; Phillips, S.M. Protein Ingestion to Stimulate Myofibrillar Protein Synthesis Requires Greater Relative Protein Intakes in Healthy Older versus Younger Men. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 57–62. [Google Scholar] [CrossRef]
- Buckner, S.L.; Loenneke, J.P.; Loprinzi, P.D. Protein Timing during the Day and Its Relevance for Muscle Strength and Lean Mass. Clin. Physiol. Funct. Imaging 2017, 38, 332–337. [Google Scholar] [CrossRef]
- Gaytán-González, A.; Ocampo-Alfaro, M.D.J.; Arroniz-Rivera, M.; Torres-Naranjo, F.; González-Mendoza, R.G.; Gil-Barreiro, M.; López-Taylor, J.R. Inadequate Protein Intake at Specific Meals Is Associated with Higher Risk of Impaired Functionality in Middle to Older Aged Mexican Adults. J. Aging Res. 2019, 2019, 6597617. [Google Scholar] [CrossRef]
- Otsuka, R.; Kato, Y.; Tange, C.; Nishita, Y.; Tomida, M.; Imai, T.; Ando, F.; Shimokata, H.; Arai, H. Protein Intake per Day and at Each Daily Meal and Skeletal Muscle Mass Declines among Older Community Dwellers in Japan. Public Health Nutr. 2019, 23, 1090–1097. [Google Scholar] [CrossRef]
- Gaytán-González, A.; Ocampo-Alfaro, M.D.J.; Torres-Naranjo, F.; Arroniz-Rivera, M.; González-Mendoza, R.G.; Gil-Barreiro, M.; López-Taylor, J.R. The Consumption of Two or Three Meals per Day with Adequate Protein Content Is Associated with Lower Risk of Physical Disability in Mexican Adults Aged 60 Years and Older. Geriatrics 2020, 5, 1. [Google Scholar] [CrossRef]
- Hayashi, A.P.; de Capitani, M.D.; Dias, S.F.; de Souza Gonçalves, L.; Fernandes, A.L.; Jambassi-Filho, J.C.; de Santana, D.A.; Lixandrão, M.; dos Santos Pereira, R.T.; Riani, L.; et al. Number of High-Protein Containing Meals Correlates with Muscle Mass in Pre-Frail and Frail Elderly. Eur. J. Clin. Nutr. 2020, 74, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Tieland, M.; den Berg, K.J.B.-V.; van Loon, L.J.C.; de Groot, L.C.P.G.M. Dietary Protein Intake in Dutch Elderly People: A Focus on Protein Sources. Nutrients 2015, 7, 9697–9706. [Google Scholar] [CrossRef]
- Rousset, S.; Mirand, P.P.; Brandolini, M.; Martin, J.-F.; Boirie, Y. Daily Protein Intakes and Eating Patterns in Young and Elderly French. Br. J. Nutr. 2003, 90, 1107–1115. [Google Scholar] [CrossRef]
- Cardon-Thomas, D.K.; Riviere, T.; Tieges, Z.; Greig, C.A. Dietary Protein in Older Adults: Adequate Daily Intake but Potential for Improved Distribution. Nutrients 2017, 9, 184. [Google Scholar] [CrossRef] [PubMed]
- Berner, L.A.; Becker, G.; Wise, M.; Doi, J. Characterization of Dietary Protein among Older Adults in the United States: Amount, Animal Sources, and Meal Patterns. J. Acad. Nutr. Diet. 2013, 113, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Bollwein, J.; Diekmann, R.; Kaiser, M.J.; Bauer, J.M.; Uter, W.; Sieber, C.C.; Volkert, D. Distribution but Not Amount of Protein Intake Is Associated with Frailty: A Cross-Sectional Investigation in the Region of Nürnberg. Nutr. J. 2013, 12, 109. [Google Scholar] [CrossRef] [PubMed]
- Ten Haaf, D.S.M.; Van Dongen, E.J.I.; Nuijten, M.A.H.; Eijsvogels, T.M.H.; De Groot, L.C.P.G.M.; Hopman, M.T.E. Protein Intake and Distribution in Relation to Physical Functioning and Quality of Life in Community-Dwelling Elderly People: Acknowledging the Role of Physical Activity. Nutrients 2018, 10, 506. [Google Scholar] [CrossRef]
- Huseinovic, E.; Winkvist, A.; Slimani, N.; Park, M.K.; Freisling, H.; Boeing, H.; Buckland, G.; Schwingshackl, L.; Weiderpass, E.; Rostgaard-Hansen, A.L.; et al. Meal Patterns across Ten European Countries-Results from the European Prospective Investigation into Cancer and Nutrition (EPIC) Calibration Study. Public Health Nutr. 2016, 19, 2769–2780. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey (NHANES) 2015–2016. Available online: https://wwwn.cdc.gov/nchs/nhanes/ContinuousNhanes/Default.aspx?BeginYear=2015 (accessed on 2 April 2019).
- Volker, M.A. Reporting Effect Size Estimates in School Psychology Research. Psychol. Sch. 2006, 43, 653–672. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawerence Erlbaum Associates: New York, NY, USA, 1988. [Google Scholar]
- Sullivan, G.M.; Feinn, R. Using Effect Size-or Why the p Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef]
- Isanejad, M.; Mursu, J.; Sirola, J.; Kröger, H.; Rikkonen, T.; Tuppurainen, M.; Erkkilä, A.T. Dietary Protein Intake Is Associated with Better Physical Function and Muscle Strength among Elderly Women. Br. J. Nutr. 2016, 115, 1281–1291. [Google Scholar] [CrossRef] [PubMed]
- Rahi, B.; Colombet, Z.; Gonzalez-Colaço, H.M.; Dartigues, J.F.; Boirie, Y.; Letenneur, L.; Feart, C. Higher Protein but Not Energy Intake Is Associated with a Lower Prevalence of Frailty among Community-Dwelling Older Adults in the French Three-City Cohort. J. Am. Med. Dir. Assoc. 2016, 17, 672.e7–672.e11. [Google Scholar] [CrossRef] [PubMed]
- Coelho-Júnior, H.J.; Rodrigues, B.; Uchida, M.; Marzetti, E. Low Protein Intake Is Associated with Frailty in Older Adults: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2018, 10, 1334. [Google Scholar] [CrossRef] [PubMed]
- Leech, R.M.; Worsley, A.; Timperio, A.; McNaughton, S.A. Understanding Meal Patterns: Definitions, Methodology and Impact on Nutrient Intake and Diet Quality. Nutr. Res. Rev. 2015, 28, 1–21. [Google Scholar] [CrossRef]
- Yasuda, J.; Asako, M.; Arimitsu, T.; Fujita, S. Skipping Breakfast Is Associated with Lower Fat-Free Mass in Healthy Young Subjects: A Cross-Sectional Study. Nutr. Res. 2018, 60, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.M.H.; So, W.K.W.; Choi, K.C.; Cheung, R.; Chan, H.Y.L.; Sit, J.W.H.; Ho, B.; Li, F.; Lee, T.Y.; Chair, S.Y. Malnutrition Risks and Their Associated Factors among Home-Living Older Chinese Adults in Hong Kong: Hidden Problems in an Affluent Chinese Community. BMC Geriatr. 2019, 19, 138. [Google Scholar] [CrossRef] [PubMed]
- Deutz, N.E.P.; Ashurst, I.; Ballesteros, M.D.; Bear, D.E.; Cruz-Jentoft, A.J.; Genton, L.; Landi, F.; Laviano, A.; Norman, K.; Prado, C.M. The Underappreciated Role of Low Muscle Mass in the Management of Malnutrition. J. Am. Med. Dir. Assoc. 2019, 20, 22–27. [Google Scholar] [CrossRef]
- Ballon, A.; Neuenschwander, M.; Schlesinger, S. Breakfast Skipping Is Associated with Increased Risk of Type 2 Diabetes among Adults: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. J. Nutr. 2019, 149, 106–113. [Google Scholar] [CrossRef]
- Hutchison, A.T.; Heilbronn, L.K. Metabolic Impacts of Altering Meal Frequency and Timing-Does When We Eat Matter? Biochimie 2016, 124, 187–197. [Google Scholar] [CrossRef]
- Ten Haaf, D.S.M.; de Regt, M.F.; Visser, M.; Witteman, B.J.M.; de Vries, J.H.M.; Eijsvogels, T.M.H.; Hopman, M.T.E. Insufficient Protein Intake Is Highly Prevalent among Physically Active Elderly. J. Nutr. Health Aging 2018, 22, 1112–1114. [Google Scholar] [CrossRef]
- Smeuninx, B.; Greig, C.A.; Breen, L. Amount, Source and Pattern of Dietary Protein Intake across the Adult Lifespan: A Cross-Sectional Study. Front. Nutr. 2020, 7, 25. [Google Scholar] [CrossRef]
- Ruiz Valenzuela, R.E.; Ponce, J.A.; Morales-Figueroa, G.G.; Muro, K.A.; Carreón, V.R.; Alemán-Mateo, H. Insufficient Amounts and Inadequate Distribution of Dietary Protein Intake in Apparently Healthy Older Adults in a Developing Country: Implications for Dietary Strategies to Prevent Sarcopenia. Clin. Interv. Aging 2013, 8, 1143–1148. [Google Scholar] [CrossRef]
- Tessier, A.J.; Chevalier, S. An Update on Protein, Leucine, Omega-3 Fatty Acids, and Vitamin D in the Prevention and Treatment of Sarcopenia and Functional Decline. Nutrients 2018, 10, 1099. [Google Scholar] [CrossRef]
- Van Til, A.J.; Naumann, E.; Cox-Claessens, I.J.H.M.; Kremer, S.; Boelsma, E.; van der Schueren, M.A.E. Effects of the Daily Consumption of Protein Enriched Bread and Protein Enriched Drinking Yoghurt on the Total Protein Intake in Elderly in a Rehabilitation Centre: A Single Blind Randomised Controlled Trial. J. Nutr. Health Aging 2015, 19, 525–530. [Google Scholar] [CrossRef]
- Host, A.; McMahon, A.T.; Walton, K.; Charlton, K. Factors Influencing Food Choice for Independently Living Older People—A Systematic Literature Review. J. Nutr. Gerontol. Geriatr. 2016, 35, 67–94. [Google Scholar] [CrossRef]
- Pennings, B.; Groen, B.B.L.; van Dijk, J.-W.; de Lange, A.; Kiskini, A.; Kuklinski, M.; Senden, J.M.G.; van Loon, L.J.C. Minced Beef Is More Rapidly Digested and Absorbed than Beef Steak, Resulting in Greater Postprandial Protein Retention in Older Men. Am. J. Clin. Nutr. 2013, 98, 121–128. [Google Scholar] [CrossRef]
- Beasley, J.M.; Wertheim, B.C.; LaCroix, A.Z.; Prentice, R.L.; Neuhouser, M.L.; Tinker, L.F.; Kritchevsky, S.; Shikany, J.M.; Eaton, C.; Chen, Z.; et al. Biomarker-Calibrated Protein Intake and Physical Function in the Women’s Health Initiative. J. Am. Geriatr. Soc. 2013, 61, 1863–1871. [Google Scholar] [CrossRef]
- Houston, D.K.; Tooze, J.A.; Garcia, K.; Visser, M.; Rubin, S.; Harris, T.B.; Newman, A.B.; Kritchevsky, S.B. Protein Intake and Mobility Limitation in Community-Dwelling Older Adults: The Health ABC Study. J. Am. Geriatr. Soc. 2017, 65, 1705–1711. [Google Scholar] [CrossRef]
- Hengeveld, L.M.; Boer, J.M.A.; Gaudreau, P.; Heymans, M.W.; Jagger, C.; Mendonça, N.; Ocké, M.C.; Presse, N.; Sette, S.; Simonsick, E.M.; et al. Prevalence of Protein Intake below Recommended in Community-dwelling Older Adults: A Meta-analysis across Cohorts from the PROMISS Consortium. J. Cachexia. Sarcopenia Muscle 2020. [Google Scholar] [CrossRef]
- Berrazaga, I.; Micard, V.; Gueugneau, M.; Walrand, S. The Role of the Anabolic Properties of Plant-versus Animal-Based Protein Sources in Supporting Muscle Mass Maintenance: A Critical Review. Nutrients 2019, 11, 1825. [Google Scholar] [CrossRef]
- Hengeveld, L.M.; Pelgröm, A.D.A.; Visser, M.; Boer, J.M.A.; Haveman-Nies, A.; Wijnhoven, H.A.H. Comparison of Protein Intake per Eating Occasion, Food Sources of Protein and General Characteristics between Community-Dwelling Older Adults with a Low and High Protein Intake. Clin. Nutr. ESPEN 2019, 29, 165–174. [Google Scholar] [CrossRef]
- Gingrich, A.; Spiegel, A.; Gradl, J.E.; Skurk, T.; Hauner, H.; Sieber, C.C.; Volkert, D.; Kiesswetter, E. Daily and Per-Meal Animal and Plant Protein Intake in Relation to Muscle Mass in Healthy Older Adults without Functional Limitations: An Enable Study. Aging Clin. Exp. Res. 2019, 31, 1271–1281. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Livingstone, M.B.E.; Sasaki, S. Meal-Specific Dietary Patterns and Their Contribution to Overall Dietary Patterns in the Japanese Context: Findings from the 2012 National Health and Nutrition Survey, Japan. Nutrition 2019, 59, 108–115. [Google Scholar] [CrossRef]
- Biró, G.; Hulshof, K.F.A.M.; Ovesen, L.; Amorim Cruz, J.A. Selection of Methodology to Assess Food Intake. Eur. J. Clin. Nutr. 2002, 56 (Suppl. 2), S25–S32. [Google Scholar] [CrossRef]
- Burrows, T.L.; Ho, Y.Y.; Rollo, M.E.; Collins, C.E. Validity of Dietary Assessment Methods When Compared to the Method of Doubly Labeled Water: A Systematic Review in Adults. Front. Endocrinol. 2019, 10, 850. [Google Scholar] [CrossRef]
- Ma, Y.; Olendzki, B.C.; Pagoto, S.L.; Hurley, T.G.; Magner, R.P.; Ockene, I.S.; Schneider, K.L.; Merriam, P.A.; Hébert, J.R. Number of 24-Hour Diet Recalls Needed to Estimate Energy Intake. Ann. Epidemiol. 2009, 19, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Basiotis, P.P.; Welsh, S.O.; Cronin, F.J.; Kelsay, J.L.; Mertz, W. Number of Days of Food Intake Records Required to Estimate Individual and Group Nutrient Intakes with Defined Confidence. J. Nutr. 1987, 117, 1638–1641. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author (Year) | City and Country | Year of Recruitment | Sample Size | Representativity | Setting | Recruitment | Food Assessment Tool |
|---|---|---|---|---|---|---|---|
| (W/M) | |||||||
| Gaytán-González (2020) [20] | Zapopan, Mexico | 2017 | 187 | Local | Community-dwelling | Users of a tertiary care hospital | One 24-h dietary recall |
| (140/47) | |||||||
| NHANES, 2015–2016 [29] | United States of America | 2015–2016 | 200 | National ‡ | Community-dwelling | Random selection from the national census | Two nonconsecutive 24-h dietary recall |
| (100/100) | |||||||
| Gingrich (2017) [14] | Nürnberg, Germany | 2016–2017 | 97 | Local | Community-dwelling | Citizen registry | 7-day food record |
| (48/49) | |||||||
| Cardon-Thomas (2018) [24] | Birmingham, United Kingdom | 2014 | 38 | Local | Community-dwelling | Volunteer databases | 3-day food diary |
| (26/12) |
| Mexico | U.S.A. | Germany | United Kingdom | p-Value | Effect Size | ||
|---|---|---|---|---|---|---|---|
| n | 187 | 200 | 97 | 38 | |||
| Women (%) | 74.9 a | 50.0 b | 49.5 b | 68.4 a,b | <0.001 | 0.244 | S |
| Age (year) | 79 ± 8 a | 71 ± 7 b | 78 ± 3 a | 78 ± 5 a | <0.001 | 0.226 | L |
| Body mass (kg) | 63.2 ± 13.1 a | 83.8 ± 19.6 b | 74.1 ± 14.0 c | 68.0 ± 12.0 a,c | <0.001 | 0.238 | L |
| Height (cm) | 153.6 ± 9.1 a | 166.6 ± 10.3 b | 166.1 ± 9.2 b | - † | <0.001 | 0.297 | L |
| BMI (kg/m2) | 26.9 ± 5.7 a | 30.1 ± 6.0 b | 26.8 ± 4.0 a | - † | <0.001 | 0.074 | M |
| Absolute protein intake (g) | |||||||
| Day | 57 ± 20 a | 74 ± 28 b | 70 ± 19 b | 76 ± 12 b | <0.001 | 0.111 | M |
| Breakfast | 17 ± 8 a | 16 ± 10 a,b | 16 ± 9 a,b | 14 ± 6 b | 0.023 | 0.006 | T |
| Lunch | 25 ± 12 | 23 ± 14 | 24 ± 10 | 29 ± 14 | 0.098 | 0.009 | T |
| Dinner | 13 ± 8 a | 30 ± 17 b | 22 ± 11 c | 33 ± 12 b | <0.001 | 0.275 | L |
| Relative protein intake (g/kg) | |||||||
| Day | 0.93 ± 0.37 a | 0.92 ± 0.38 a | 0.97 ± 0.28 a | 1.14 ± 0.25 b | <0.001 | 0.019 | S |
| Breakfast | 0.29 ± 0.16 a | 0.20 ± 0.13 b | 0.23 ± 0.12 b | 0.21 ± 0.10 b | <0.001 | 0.077 | M |
| Lunch | 0.41 ± 0.22 a | 0.28 ± 0.19 b | 0.33 ± 0.14 c | 0.43 ± 0.23 a,c | <0.001 | 0.082 | M |
| Dinner | 0.21 ± 0.14 a | 0.37 ± 0.22 b | 0.30 ± 0.14 c | 0.50 ± 0.19 d | <0.001 | 0.196 | L |
| Daily contribution (%) | |||||||
| Breakfast | 32 ± 14 a | 22 ± 13 b,c | 23 ± 10 b | 19 ± 8 c | <0.001 | 0.126 | M |
| Lunch | 43 ± 15 a | 31 ± 16 b | 35 ± 12 b | 38 ± 16 a,b | <0.001 | 0.114 | M |
| Dinner | 23 ± 12 a | 40 ± 16 b | 31 ± 11 c | 44 ± 15 b | <0.001 | 0.268 | L |
| PDCV | 0.55 ± 0.26 a | 0.59 ± 0.28 a | 0.43 ± 0.24 b | 0.60 ± 0.18 a | <0.001 | 0.044 | S |
| n | (%) | (95% CI) | |
|---|---|---|---|
| IPID-0.8 | 194 | (37.2) | (33.1–41.4) |
| IPID-1.0 | 307 | (58.8) | (54.5–63.0) |
| IPID-1.2 | 404 | (77.4) | (73.6–80.8) |
| IPIM-30 | |||
| Breakfast | 483 | (92.5) | (89.9–94.5) |
| Lunch | 373 | (71.5) | (67.4–75.2) |
| Dinner | 388 | (74.3) | (70.4–77.9) |
| IPIM-0.4 | |||
| Breakfast | 457 | (87.5) | (84.4–90.1) |
| Lunch | 347 | (66.5) | (62.3–70.4) |
| Dinner | 390 | (74.7) | (70.8–78.3) |
| Number of meals with ≥30 g/meal | |||
| Zero | 261 | (50.0) | (45.7–54.3) |
| One | 208 | (39.8) | (35.7–44.1) |
| Two or three | 53 | (10.2) | (7.8–13.0) |
| Number of meals with ≥0.4 g/kg/meal | |||
| Zero | 233 | (44.6) | (40.4–48.9) |
| One | 215 | (41.2) | (37.0–45.5) |
| Two or three | 74 | (14.2) | (11.4–17.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaytán-González, A.; Ocampo-Alfaro, M.d.J.; Torres-Naranjo, F.; González-Mendoza, R.G.; Gil-Barreiro, M.; Arroniz-Rivera, M.; López-Taylor, J.R. Dietary Protein Intake Patterns and Inadequate Protein Intake in Older Adults from Four Countries. Nutrients 2020, 12, 3156. https://doi.org/10.3390/nu12103156
Gaytán-González A, Ocampo-Alfaro MdJ, Torres-Naranjo F, González-Mendoza RG, Gil-Barreiro M, Arroniz-Rivera M, López-Taylor JR. Dietary Protein Intake Patterns and Inadequate Protein Intake in Older Adults from Four Countries. Nutrients. 2020; 12(10):3156. https://doi.org/10.3390/nu12103156
Chicago/Turabian StyleGaytán-González, Alejandro, María de Jesús Ocampo-Alfaro, Francisco Torres-Naranjo, Roberto Gabriel González-Mendoza, Martha Gil-Barreiro, Maritza Arroniz-Rivera, and Juan R. López-Taylor. 2020. "Dietary Protein Intake Patterns and Inadequate Protein Intake in Older Adults from Four Countries" Nutrients 12, no. 10: 3156. https://doi.org/10.3390/nu12103156
APA StyleGaytán-González, A., Ocampo-Alfaro, M. d. J., Torres-Naranjo, F., González-Mendoza, R. G., Gil-Barreiro, M., Arroniz-Rivera, M., & López-Taylor, J. R. (2020). Dietary Protein Intake Patterns and Inadequate Protein Intake in Older Adults from Four Countries. Nutrients, 12(10), 3156. https://doi.org/10.3390/nu12103156